
Abstract
Purpose:
Around three quarters of individuals undergoing chemotherapy self-report multiple symptoms. There is clinical trial evidence of effectiveness for acupuncture for commonly experienced symptoms, and emerging evidence for reflexology, but little is known about the effects of these therapies on multiple symptoms when implemented in a real world setting during active chemotherapy treatment.
Methods:
This was a cohort study of participants receiving reflexology and/or acupuncture while attending chemotherapy. Participants received a 20 minute reflexology treatment or a 20 minute acupuncture treatment or a combination of both. Patient reported outcome measures were administered before and after the treatment using the Edmonton Symptom Assessment Scale (ESAS).
Results:
During the study period, 330 unique patients received a total of 809 acupuncture and/or reflexology treatments. Participants had, on average, 5.3 symptoms each which they reported as moderate to severe (≥4/10) using the ESAS at baseline. Following treatment, participants reported 3.2 symptoms as moderate to severe. The symptom change for all participant encounters receiving any therapy was statistically significant for all symptoms, and clinically significant (a reduction of more than 1) for all symptoms except financial distress, appetite, and memory. Clinically significant levels of global distress (<3) were reduced in 72% of all participants receiving either therapy. No adverse events were recorded.
Conclusions:
The results indicate that acupuncture and reflexology administered alongside chemotherapy may reduce patient reported symptom burden and patient global symptom related distress. Future research would include an active control group, and consider confounding factors such as chemotherapy stage and medication.
Introduction
Chemotherapy side effects impact quality of life, psychological wellbeing and may impact on capacity to tolerate a full dose of treatment. Around three quarters of individuals undergoing chemotherapy self-report multiple symptoms the most frequent being fatigue, anxiety, nausea, and bowel disturbances. 1 Complementary therapies are increasingly being incorporated into supportive cancer care within a hosptial setting to assist patients in managing these symptoms.
Acupuncture is used globally for cancer symptoms and side effects. It is offered across all National Institutes of Health cancer centers, and incorporated in ASCO endorsed guidelines.2,3 Randomized controlled trials (RCT) have demonstrated benefit for anxiety, depression, insomnia, vasomotor symptoms, and other symptoms experienced by patients undergoing chemotherapy. 3 Acupuncture has been shown to be safe, and may provide an option for patients.
Reflexology is a non-invasive, localized touch therapy that is an easily administered therapeutic treatment well suited to the setting of a chemotherapy day unit. Studies have shown benefit for anxiety, sleep, pain, and quality of life.4-6 Together, acupuncture and reflexology may also assist in managing chemotherapy induced peripheral neuropathy.
Symptoms experienced by patients undergoing chemotherapy often appear in clusters. 7 While there is evidence of the beneficial effects of acupuncture for individual symptom control in clinical trial settings, and emerging evidence for reflexology, little is known about the effects of reflexology and acupuncture and the treatment of multiple symptoms when implemented in a real world setting during chemotherapy treatment.
The aim of this cohort study was to observe the effects of acupuncture and/or reflexology on the multiple self-reported symptoms of patients undergoing chemotherapy.
Methods
This was a prospective, observational cohort study of participants who utilized reflexology and/or acupuncture services while attending chemotherapy at the Chris O’Brien Lifehouse during the period of 2017 to 2020. The study received ethics approval from the Sydney Local Area Health District Ethics Committee in May 2019 (HREC/18/RPAH/519).
This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement. 8
Participants
Patients receiving chemotherapy for solid tumors in the hospital day therapy unit were offered acupuncture or reflexology therapy. Participants could self-refer or be referred by healthcare professionals within the hospital. Treatments were provided free of charge to the patient, funded by a philanthropic grant to the hospital. Patients were excluded if they had profound neutropenia, thrombocytopenia (platelets <50), selected skin conditions or risk of bruising due to their coagulation status.
Setting
The Chris O’Brien Lifehouse in Australia, operates as a non-for-profit cancer hospital and services over 15 000 patients per year, and has a dedicated integrative oncology service. 9 The Day Therapy unit has over 45 chemotherapy chairs with 20 000 appointments annually. The acupuncture and reflexology service is available twice a week, over a 90 minutes period in the chemotherapy suite with either an acupuncturist or a reflexologist, or at times both of these. Participants were treated in either their chair while having their infusion or in a multi-chair room within the day therapy unit.
Intervention
Participants had a short initial consultation and received a 20 minute reflexology treatment or a 20 minute acupuncture treatment or, if requested and available, a combination of both.
For both acupuncture and reflexology, patient reported outcomes were evaluated and contraindications considered to determine an appropriate treatment plan.
For the acupuncture, the treatment plan also included considerations of traditional Chinese medicine diagnostic tools of tongue and pulse. Acupoints were tailored to the presentation of the individual and selected based on traditional Chinese medicine, patient reported outcome measures, and the expertise of the traditional Chinese medicine trained acupuncturists. Points were needled with manual stimulation only until de qi sensation was attained. Needles were typically retained for 20 minutes. Acupuncture points were restricted to those that could be safely administered while the patient was seated in a reclining position. Where participants were undergoing an infusion through their arm that limb was typically not included in the acupuncture points selected. Acupuncture needles were single use sterile Balance Spring Handle (IKS type, sizes 25/30/40 mm × 0.20 mm and 13 mm × 0.20 mm).
For the reflexology treatment, the feet were massaged with cream and pressed in a systematic way to address areas of imbalance in the body in accordance with the internationally accepted Ingham protocol. 10 In the Ingham protocol the therapists uses their hands only to massage reflex points on the patient’s feet that correspond to a specific internal organ within the body.
Therapists had a minimum of 5 years’ experience working with cancer patients, and were credentialed to work within the hospital setting. Participants could choose to have additional treatments, if available at the time of their next chemotherapy infusion.
Outcome Measure
Patient reported outcome measures were administered before and after the treatment using the Edmonton Symptom Assessment Scale (ESAS). 11 The ESAS-R includes 9 symptoms rated on a visual analog scale (VAS) from 0 to 10. We used the ESAS-R with the addition of the following items relevant to patients with cancer: sleep, spiritual pain, financial distress, hot flashes, numbness, dry mouth, and memory. This modified ESAS has been used in previous studies in the cancer population. 12 Participants completed the initial ESAS prior to treatment and were asked to select a value that related to how they felt in the last 24 hours. Immediately after treatment, they were asked to report on how they felt “right now.” The ESAS-R has 3 subscales: the physical distress score (PHS), a composite of 6 symptoms—pain, fatigue, nausea, drowsiness, appetite, and shortness of breath (0-60); the psychological stress score (PSS), a sum of depression and anxiety (0-20); and the global distress score (GDS) a sum of the PHS, PSS and well-being (0-90). 13 The higher the score, the more distress.
The ESAS was administered by a research assistant not providing treatment to minimize administration bias. The research assistant was not blinded to the intervention patients received. Basic demographic data, and primary cancer diagnosis were extracted from the electronic medical record. Participants were asked if they had ever used acupuncture or reflexology before. While this was a prospective cohort study, the intervention was part of usual care; as such we did not seek to record additional socio-demographic characteristics. At the start of the treatment, participants were asked to advise therapists if they experienced any discomfort at any time during the treatment. Any adverse events were recorded in the electronic medical record.
Statistical Analysis
Statistical analysis was conducted using the statistical software R version 4.0.2. 14 Descriptive statistics were used to analyze demographic information. For the ESAS symptom scores and composite scores, where one encounter per patient (the last treatment) was analyzed, paired t-tests for the change from baseline were used. Where all patient encounters were analyzed, generalized estimation equation methods were used to compute means, standard deviations, and tests for changes from baseline, in order to correct for more than one treatment (ie, repeat treatments). Complete case analysis was performed, (ie, where a patient symptom response was missing, that data item was omitted from the analysis).
Change of ESAS scores greater than 1 are considered clinically significant. For the physical, emotional, and total symptom distress subscales, clinically significant reductions are as follows: PHS ≥ 2, PSS ≥ 2, and GDS ≥ 3. 13 Degree of symptom burden was classified by 0 as “no burden,” 1 to 3 “mild,” 4 to 6 “moderate,” and 7 to 10 “severe” burden. Moderate and severe burden scores on the ESAS represent need for further support or investigation.15,16 Statistical significance was set at 5% and high statistical significance at 1%.
A separate analysis of the mean was calculated for the different therapy groups (acupuncture, reflexology, combined). Paired t-tests were used to determine the changes in mean score.
Results
During the study period, 330 unique participants with a cancer diagnosis received acupuncture and/or reflexology treatments while undergoing chemotherapy. Participants were mainly female (79%) with breast cancer (31%), and a median age of 56 (Table 1). Of the 330 participants, 58 (20%) had used acupuncture before, 54 (19%) had used reflexology, and 95 (33%) had used both therapies before.
Demographics and Baseline Presenting Symptoms. 1

1 Missing data: due to a changeover in electronic medical record systems within the hospital not all demographics were able to be extracted.
2 If a participant scored the ESAS symptom ≥1 this was recorded as symptomatic. Where a symptom was scored as “0” this not recorded as symptomatic. The “N” refers to the total number of responses received for each symptom.
3N refers to the number of participants. Missing data for individual symptoms occurred where participants did not record a response.
Baseline presenting symptoms: The most prevalent presenting symptoms (ESAS ≥ 1) for patients were poor sleep (85%), fatigue (85%) and decreased sense of well-being (95%) (Table 1). Presenting symptoms were similar across acupuncture, reflexology, and acupuncture/reflexology therapies.
Number of treatments per participant: For 330 participants, there were 809 treatments provided, with participants receiving an average of 2.45 (range 1-28) treatments each, with a median of 1. Methods for addressing data collected across several treatments is described in the Statistical Analysis section.
Symptom severity: Moderate to severe (≥4) symptoms at baseline were reported for fatigue (51%), poor sleep (51%), and poor well-being (49%) (Figure 1; Supplemental Table S1). After treatment, those reporting moderate to severe symptoms reduced in fatigue (23%), poor sleep (31%), and poor wellbeing (22%).
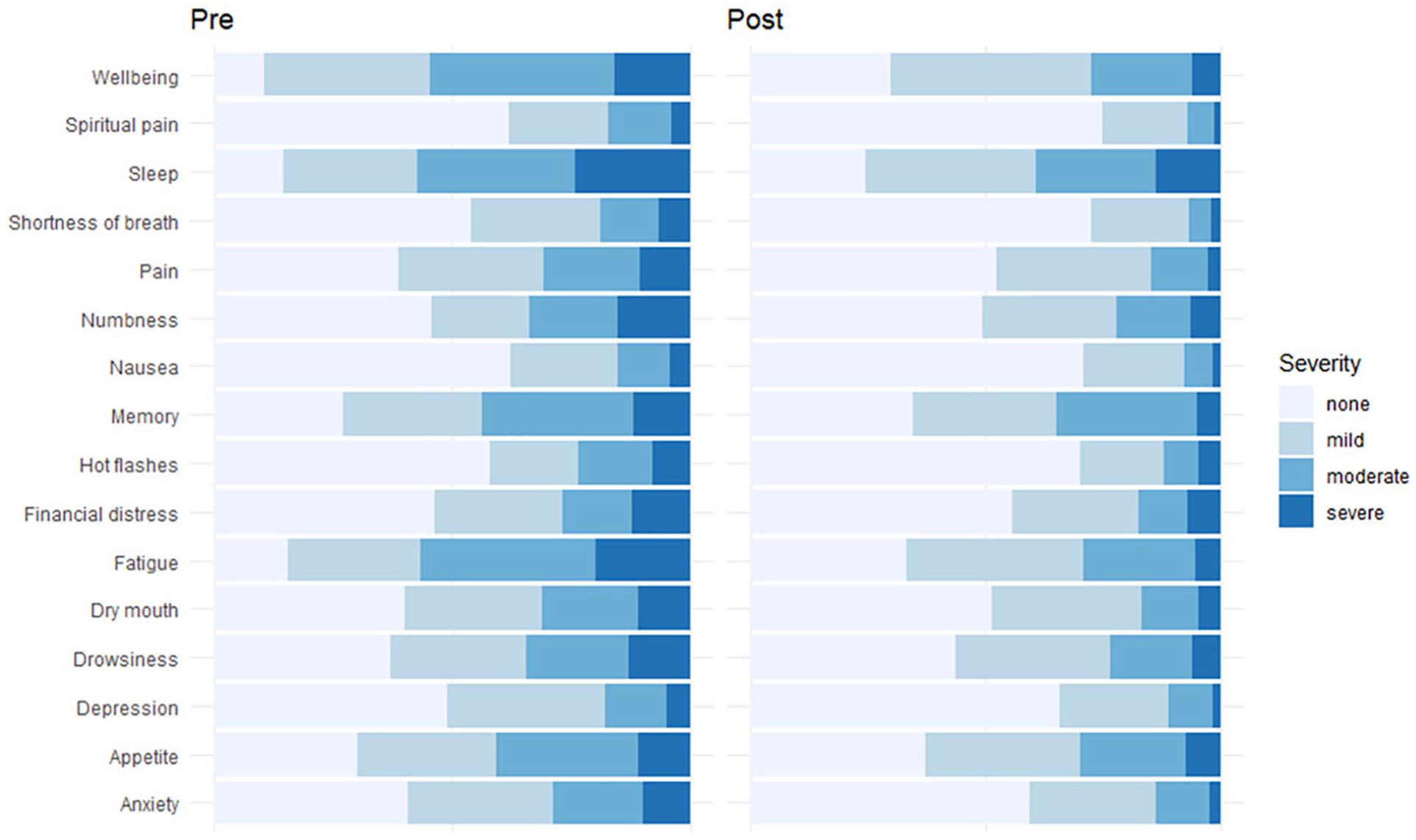
Change in symptom severity. 1
Number of symptoms: Participants had, on average, 5.3 moderate to severe (≥4/10) symptoms before treatment (Figure 1; Supplemental Table S1). Following treatment, participants reported 3.2 symptoms as moderate to severe.
Symptom change in all encounters: The symptom change for all participant encounters receiving any therapy was statistically significant for all symptoms, and clinically significant (a reduction of more than 1) for all symptoms except financial distress, appetite, and memory (Table 2).
Symptom Change in all Participant Encounters. 1

1 All mean changes from baseline were highly significant (P < .001) with the exception of appetite in the acupuncture group which was significant (P = .036) and financial distress (P = .074).
Clinically significant changes were noted in overall global (GDS), physical symptom distress (PHS), and psychological stress score (PSS). For the ESAS sub-scales, there were clinically and statistically significant mean changes for the global distress score (−8.01), the physical (−5.15), and the emotional distress score (−2.44).
Acupuncture group: Statistically significant and clinically significant changes were experienced for all symptoms with the exception of financial distress. There was a clinically and statistically significant mean change (P < .001) on all global distress (−7.31), physical distress (−4.87), and psychological symptom scores (−2.15).
Reflexology group: Statistically significant changes were found for all reported symptoms, and these changes were clinically significant with the exception of financial distress and appetite. There was a clinically and statistically significant change on all global distress (−7.83), physical distress (−4.89), and psychological (−2.41) symptom scores.
Combined acupuncture and reflexology: Combined treatment resulted in statistically and clinically significant changes for all symptoms with the exception of financial distress and memory. There was a clinically and statistically significant change on all global distress (−8.36), physical distress (−5.68), and psychological symptom scores (−2.3). There was no significant difference in mean changes between groups (acupuncture alone, reflexology alone, both therapies).
Clinical Response Rates for Participants. 1 .

1 Clinical response rate: a 1-point decrease or more on ESAS individual symptoms; 2-point decrease or more on the ESAS PSS; 3-point decrease or more on the ESAS PHS and GDS.
Global distress scores reduced by 3 points in 72% of all patients receiving any therapy or combination of therapy.
No adverse events were reported.
Discussion
This is one of the first observational studies to examine the effects of acupuncture and reflexology on patient reported symptom burden while undergoing chemotherapy in a routine care setting. Overall, patients receiving either or both therapies were likely to experience a clinically significant change in all symptoms except appetite, financial distress and memory. Clinically significant reductions in global distress (a reduction of more than 3 points) was reported in 72% of all participants using any therapy, with a mean reduction of 8 on the 90-point scale. There was no statistically significant difference between the responses to the therapies participants were given. A more rigorous study design may elucidate comparative effectiveness and guide cost considerations on therapy preferences for provision in other integrative oncology settings. Acupuncture can be provided to more than one individual at the same time, while reflexology is fixed which may have cost implications. In our study, therapists were reimbursed at the same hourly rate but this may differ in other jurisdictions.
The most prevalent symptoms in our study for those presenting for acupuncture were sleep disturbance, fatigue, and reduced appetite, and are consistent with frequently reported symptoms in other studies of cancer patients using acupuncture in a hospital setting.17,18
To date most studies directed at reducing the symptom burden of patients undergoing chemotherapy have focused on self-help, nurse-led intervention, psychoeducation, and cognitive behavioral therapies with mixed results.19-21 Other non-pharmacological approaches specifically for symptom clusters in patients undergoing chemotherapy have included self-acupressure, and guided imagery. 22
Our study indicates that the use of reflexology for reducing the symptom burden of patients during chemotherapy may provide benefit. This is consistent with other studies, however, evidence limitations include small sample size and quasi-experimental designs. 6
Several studies have investigated acupuncture and reflexology specifically for a single symptom such as nausea and/or vomiting but few on the use of either acupuncture or reflexology for the reduction of several symptoms during chemotherapy.23-26 Reflexology and acupuncture may be an option for patient to address multiple symptoms or symptom clusters with the flexibility to address changes over the course of treatment. 27
Limitations
This study has several limitations. This study was undertaken at a single cancer center and may not be generalizable to other settings. Without a control group it is difficult to predict the non-specific effects of the attention, touch, or simply being in a quiet, reclining environment for 20 minutes. This study did not control patient interaction with other staff, patients or friends during intervention and more accurately reflects real world practice.
We did not control for supportive care medications and this may have impacted on self-report symptoms. Participants were free to choose if they were interested in the intervention, and which intervention they preferred, as such selection bias cannot be ruled out.
Although the service was initially offered only for 90 minutes 1 day a week, we expanded to 2 days and these days remained fixed. The reflexology service was available more frequently than the acupuncture.
Future research would include an active control group, factor in statistical measures for selection bias and consider confounding factors such as chemotherapy stage and medication. Research may also consider quality of life following chemotherapy, impact on dose delays, dose reductions, and reduced relative dose intensity (RDI) rates, and medication rates.
Conclusion
Acupuncture and reflexology can safely be administered alongside chemotherapy in the chemotherapy chair/suite to produce a clinically significant reduction in patient global symptom distress, physical and psychological distress and reported symptom burden. This cohort study provides a real-world example of the complex quality of life symptoms experienced by people undergoing chemotherapy and how therapies such as acupuncture and reflexology have the potential to mitigate these. The results of the current study support the importance of advancing the investigation of acupuncture and reflexology for the management of not only individual symptoms, but symptom clusters that occur within the context of cancer treatments.
Supplemental Material
sj-docx-1-ict-10.1177_15347354221123055 – Supplemental material for Acupuncture and Reflexology for Patients Undergoing Chemotherapy: A Cohort Study
Supplemental material, sj-docx-1-ict-10.1177_15347354221123055 for Acupuncture and Reflexology for Patients Undergoing Chemotherapy: A Cohort Study by Suzanne J. Grant, Gretel Spiegel, Amanda Brand, Ki Kyung Kwon, Gillian Heller, Victoria Choi, Emma K. Wong, Lindley Randle and Judith Lacey in Integrative Cancer Therapies
Footnotes
Authors’ contributions
SG and GS conceived the study. SG, GS, JL and LR designed the study. SG, GS, VC, EW, KK and AB contributed to the data, data collection and cleaning. GH and SG performed the analysis. All members contributed to writing the final paper.
Availability of data and material
Deidentified data set
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This research was supported by a donation from the McNiven family and Mostyn family. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Code availability
Not applicable
Consent to participate
Consent to participate as per Ethics approval.
Consent for publication
Not applicable
Ethics approval
The study received ethics approval from the Sydney Local Area Health District Ethics Committee in May 2019 (HREC/18/RPAH/519).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.