
Abstract
Keywords
Introduction
Breast cancer is the most frequent form of female cancer worldwide, with a steadily rising incidence over the past decades. 1 Most patients are diagnosed with primary, resectable breast cancer, and a relevant part is treated with systemic therapies to decrease the risk for relapse and improve breast cancer–related survival. Systemic therapies, such as chemotherapy and endocrine therapy, cause considerable side effects and decline in functional status and health-related quality of life (HR-QoL).2,3
Throughout chemotherapy treatment, most breast cancer patients report multiple burdensome physical and psychological symptoms, related to the disease itself and to respective treatments. Symptom burden is defined as the subjective, quantifiable prevalence, frequency, and severity of symptoms, placing a physiological burden on patients and producing multiple negative, physical, and emotional patient responses. 4 The burdensomeness of symptoms can be assessed with various questionnaires, for example, the Memorial Symptom Assessment Scale (MSAS), where the patient grades the self-perceived severity of the respective symptoms. Such burdensome symptoms can be described individually, as well as be grouped into clusters. Symptom clusters can be defined as 2 or more concurrent symptoms that are related to each other, for example, by etiology or affected domain.5,6 This clustering as well as reporting the burden of symptoms has a larger impact on clinical outcomes and HR-QoL than individual symptoms.7-14 Grouping self-reported symptoms into clusters adds to our understanding of the coherence of individual symptoms and can help identify shared pathophysiological factors. Moreover, it enables estimation of their burdensomeness and assessment of the combined effect of certain symptoms on HR-QoL. This information helps clinicians design effective interventions targeting the most burdensome symptoms and identify factors promoting self-support measures.
A number of studies have described burdensome symptoms and/or symptom clusters in patients with early-stage breast cancer. To our knowledge, only 2 longitudinal studies reported on changes in both symptom clusters and burdensome symptoms during and after adjuvant systemic treatment, assessed by self-reported symptoms from the MSAS.15,16 Both studies revealed clusters of burdensome symptoms involved in emotional, gastrointestinal, and physical symptomatology and showed dynamics in the composition of symptoms within the clusters over time. In addition, core symptoms within these clusters contributed the most to the burdensomeness experienced by patients. Core symptoms were based on the symptoms within a cluster with the highest internal correlations. 13
The prospective, randomized controlled OptiTrain study that included breast cancer patients receiving adjuvant chemotherapy showed beneficial effects of 16 weeks of both resistance and high-intensity interval training (RT-HIIT) and moderate-intensity aerobic and high-intensity interval training (AT-HIIT) on total symptoms and symptom burden as measured by the MSAS, while detrimental effects were found for the usual care (UC) group. 17 To date, the effects of a physical exercise intervention during chemotherapy on clusters of burdensome symptoms are not known. Moreover, it is not known which domains and core burdensome symptoms within those clusters are most affected by physical exercise.
In the current analysis, we aim to describe longitudinal changes in symptom clusters in the RT-HIIT, AT-HIIT, and UC groups in the OptiTrain cohort. We will also assess the effect of RT-HIIT and AT-HIIT on core burdensome symptoms within these symptom clusters.
Patients and Methods
This study is a secondary analysis of data collected as part of the longitudinal prospective, randomized controlled OptiTrain breast cancer trial.
Participants
Recruitment to the study took place at the Karolinska University Hospital (Solna, Sweden) from March 2013 to July 2016. Inclusion criteria were women aged between 18 and 70 years, diagnosed with I to IIIa stage breast cancer, and scheduled to receive adjuvant chemotherapy consisting of anthracyclines, taxanes, or a combination of both. Exclusion criteria included cardiac disease (assessed by routine electrocardiogram and a questionnaire), major psychiatric disorders, or other concurrent malignant diseases. The participants were randomly allocated to either (1) RT-HIIIT, (2) AT-HIIT, or (3) a control group receiving UC prior to baseline testing. The intervention groups (RT-HIIT and AT-HIIT) commenced the exercise training 3 days after the second chemotherapy session and ended the intervention 3 weeks following the last chemotherapy session. Details of the randomization and blinding process have been published previously. 18 The OptiTrain study (NCT02522260) was approved by the Regional Ethical Review Board in Stockholm (Dnr 2012/1347-31/1, 2012/1347-31/2, 2013/632-32, 2014/408 32). 17 All participants gave written informed consent prior to enrollment.
Outcome Measures
Study assessments took place at baseline (1 week prior to participants’ second chemotherapy session), at 16 weeks (postintervention), and 12-month post-baseline (follow-up). Neither participants nor testers were blinded to study group allocation.
Memorial Symptom Assessment Scale
Patients completed the 32-item MSAS at home.19,20 The scale includes occurrence, frequency, severity, and distress associated with each symptom using 4- and 5-point rating scales. Symptom burden was calculated as the average of frequency, severity, and distress of each symptom. Higher scores indicated higher symptom burden.
Intervention
The OptiTrain exercise protocol has been described previously.17,18 Briefly, both exercise groups trained twice per week for 16 weeks, and each session was approximately 60 minutes in duration. The exercise sessions were conducted at the exercise clinic at the Karolinska University Hospital and supervised by an exercise physiologist or oncology nurse. The RT-HIIT group performed high-load resistance exercises targeting the major muscle groups consisting of 2 to 3 sets of 8 to 12 repetitions, at an intensity of 70% to 80% of their estimated 1 repetition maximum. The RT-HIIT sessions concluded with 3 × 3 minute bouts of high-intensity interval exercise at a rating of perceived exertion of 16 to 18, with each bout split by 1-minute recovery, on a cycle ergometer. The AT-HIIT group initiated each session with 20 minutes of moderate-intensity (rating of perceived exertion = 13-15) continuous aerobic exercise followed by the same high-intensity interval exercise as in RT-HIIT.
Usual Care
The UC group received printed written information on physical activity advice based on the American College of Sports Medicine for cancer survivors, directly after baseline testing. 21
Statistical Methods
Cancer-related fatigue was the primary endpoint of the OptiTrain trial and was the basis for the power calculation.17,18 In the current study, descriptive statistics were used to summarize demographic and treatment data.
In each of the 3 arms of the OptiTrain trial (RT-HIIT, AT-HIIT, and UC), symptom burden scores were calculated for all 32 items on the MSAS, according to the MSAS manual. Symptom burden scores ranged between 0 and 4. 19 Only symptom burden scores above 0.5 (high burden) were included for further analysis. 16 The cutoff point of 0.5 was chosen based on findings from a previous study, where associations were found between the presence of symptom clusters among cancer patients and survival duration, independent of other prognostic factors. 22 The symptom cluster analysis, with principal component analysis (PCA) as the extraction method and varimax rotation method with Kaiser normalization was conducted with the symptom burden scores for each of the 3 study arms. A fixed number of 3 components in the PCA was chosen, comparable to a previous study, 16 as we expected that many symptoms would be assigned to the same component or symptom cluster. Furthermore, we argued that this would be helpful to determine core (burdensome) symptoms and perform between-group comparisons. Only symptoms with a factor loading ≥0.5 were included in a component. PCAs were performed at each measurement time (baseline, 16 weeks, and 12 months after baseline).
The most prominent burdensome symptom in a component was the symptom with the highest factor loading.
Core burdensome symptoms were defined as symptoms present in 1 of the 3 symptom clusters at most study assessments and in all 3 study arms. To explore differences in symptoms between the groups at 16 weeks and 12 months post-baseline, we used linear mixed models with Bonferroni correction, controlling for baseline values, menopausal status, and tumor receptor status. Data not normally distributed were log-transformed prior to linear mixed models analyses. Standardized effect sizes (ES) were calculated as described previously.18,23 ES with scores of 0.2 to 0.5, 0.5 to 0.8, and >0.8 were considered small, medium, and large effects, respectively. 24 The results were considered statistically significant at the 5% level (P < .05). All calculations were done with the IBM SPSS version 25 statistical package for Windows.
Results
In total, 240 women were randomized into the OptiTrain study and 206 women completed baseline testing. The CONSORT study flow chart is shown in Figure 1. The demographic and clinical characteristics of the original patient sample for this secondary analysis are listed in Table 1. One hundred seventy-seven women completed the MSAS at all 3 time points and were included in the current analysis. There were no significant differences in baseline and treatment characteristics between those who completed the follow-up at 12 months compared with those who completed the 16-week time point measurements. No patients had died or had a recurrence at the 12-month time point. Attendance rates for participants in the RT-HIIT and AT-HIIT groups were 68% and 63%, respectively, and adherence to the training program was 83% in the RT-HIIT group and 75% in AT-HIIT group.18,25

CONSORT diagram: participant flow through the OptiTrain study.
Baseline Participant Characteristics.

Abbreviations: RT-HIIT, resistance and high-intensity interval training; AT-HIIT, moderate-intensity aerobic and high-intensity interval training; UC usual care; SD, standard deviation; BMI, body mass index; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2.
Formation of Symptom Clusters
Three symptom clusters were formed; these were labelled “emotional cluster,” “treatment-related toxicity cluster,” and “physical cluster” based on the burdensome symptoms that composed these clusters. Table 2 summarizes the respective symptoms and their factor loadings in the 3 clusters over time.
Symptom Clusters With Burdensome Symptoms and Factor Loadings a .

Abbreviations: RT-HIIT, resistance and high-intensity interval training group; AT-HIIT, moderate-intensity aerobic and high-intensity interval training; UC, usual care.
Symptom burden scores above 0.5 (high burden) were included in the principle component analysis. This eliminated 11 symptoms at baseline (“cough,” “numbness or tingling in hands or feet,” “problems with urination,” “vomiting,” “itching,” “dizziness,” “difficulty swallowing,” “mouth sores,” “weight loss,” “swelling of arms or legs,” and “changes in skin”), 11 symptoms at 16 weeks (“cough,” “nausea,” “problems with urination,” “vomiting,” “diarrhea,” “itching,” “dizziness,” “difficulty swallowing,” “mouth sores,” “weight loss,” and “constipation”), and 22 symptoms at 1 year (“cough,” “nausea,” “feeling drowsy,” “feeling bloated,” “problems with urination,” “vomiting,” “shortness of breath,” “diarrhea,” “worrying,” “problems with sexual interest or activity,” “itching,” “lack of appetite,” “dizziness,” “difficulty swallowing,” “mouth sores,” “change in the way food tastes,” “weight loss,” “hair loss,” “constipation,” “swelling of arms or legs,” “I don’t look like myself,” and “changes in skin”).
Longitudinal Changes in Symptom Clusters
Baseline
At baseline, 3 burdensome symptoms (eg, “I don’t look like myself,” “feeling irritable,” and “feeling sad”) were present in the emotional cluster in all 3 study arms. Only “nausea” and “sweats” overlapped in all 3 study arms in the treatment-related toxicity cluster and physical cluster, respectively. The absolute number of burdensome symptoms was more diverse between the 3 study arms in the treatment-related toxicity and physical clusters, summarized in Table 2.
Sixteen Weeks Post-Baseline
At 16 weeks, the symptom clusters of the 3 study arms were composed of different symptoms compared with the 3 study arms at baseline. Furthermore, the symptom clusters consisted of different overlapping symptoms between the 3 study arms compared with baseline. For the emotional cluster, “worrying” was the most prominent burdensome symptom in the RT-HIIT group and “feeling irritable” the most prominent burdensome symptom in the AT-HIIT and UC groups. The most prominent burdensome symptoms in the treatment-related toxicity cluster were “changes in the way food tastes” for the RT-HIIT and AT-HIIT groups, and “lack of appetite” for the UC group. In the physical cluster “feeling bloated,” “lack of appetite,” and “difficulty sleeping” were the most prominent burdensome symptoms for the RT-HIIT, AT-HIIT, and UC groups, respectively.
Twelve Months Post-Baseline
In all 3 study arms, the symptom clusters consisted of a lower absolute number of burdensome symptoms compared with baseline and 16 weeks. Moreover, the symptom clusters consisted of less overlapping symptoms between the 3 study arms compared with baseline and 16 weeks. The emotional cluster at 12 months was composed mostly of the same burdensome symptoms as those reported at baseline. In the emotional cluster, “feeling irritable,” “difficulty concentrating,” and “lack of energy” were the most prominent burdensome symptoms in the RT-HIIT, AT-HIIT, and UC groups, respectively.
The most prominent burdensome symptoms in the treatment-related toxicity cluster were “dry mouth” for the RT-HIIT and AT-HIIT groups and “numbness” for the UC group. In the physical symptom cluster, “sweats” was the most prominent burdensome symptom in the RT-HIIT and AT-HIIT groups and “dry mouth” the most prominent burdensome symptoms for the UC group.
Core Burdensome Symptoms Within the Respective Symptom Clusters
The emotional cluster consisted of 5 core burdensome symptoms in all 3 study arms at most time points: “feeling nervous,” “feeling sad,” “problems with sexual interest or activity,” “feeling irritable,” and “I don’t look like myself.” The treatment-related toxicity cluster was composed of 5 core burdensome symptoms: “dry mouth,” “nausea,” “numbness or tingling in hands or feet,” “diarrhea,” and “changes in the way food tastes.” The physical cluster consisted of 2 core burdensome symptoms: “feeling drowsy” and “sweats.”
Longitudinal Differences in Core Symptoms in the Intervention Groups
The mean symptom burden scores at all 3 time points, between-group differences at 16 weeks and at 12 months, as well as ES for differences in core burdensome symptoms are shown in Table 3. Longitudinal changes in mean symptom burden score for those core burdensome symptoms in the different study groups are depicted in Figure 2.
Core Symptoms With Mean Symptom Burden Scores and Between-Group Differences.
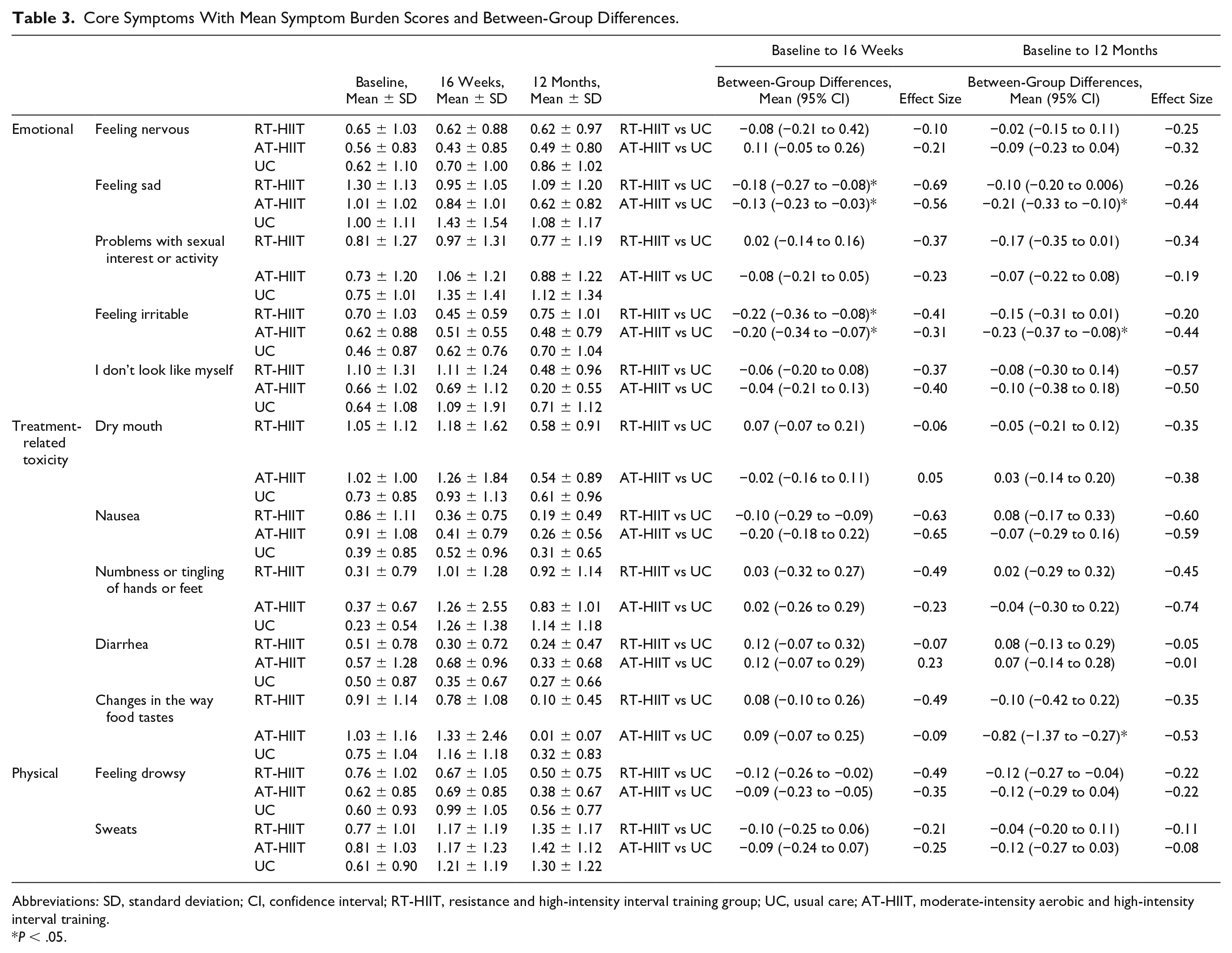
Abbreviations: SD, standard deviation; CI, confidence interval; RT-HIIT, resistance and high-intensity interval training group; UC, usual care; AT-HIIT, moderate-intensity aerobic and high-intensity interval training.
P < .05.
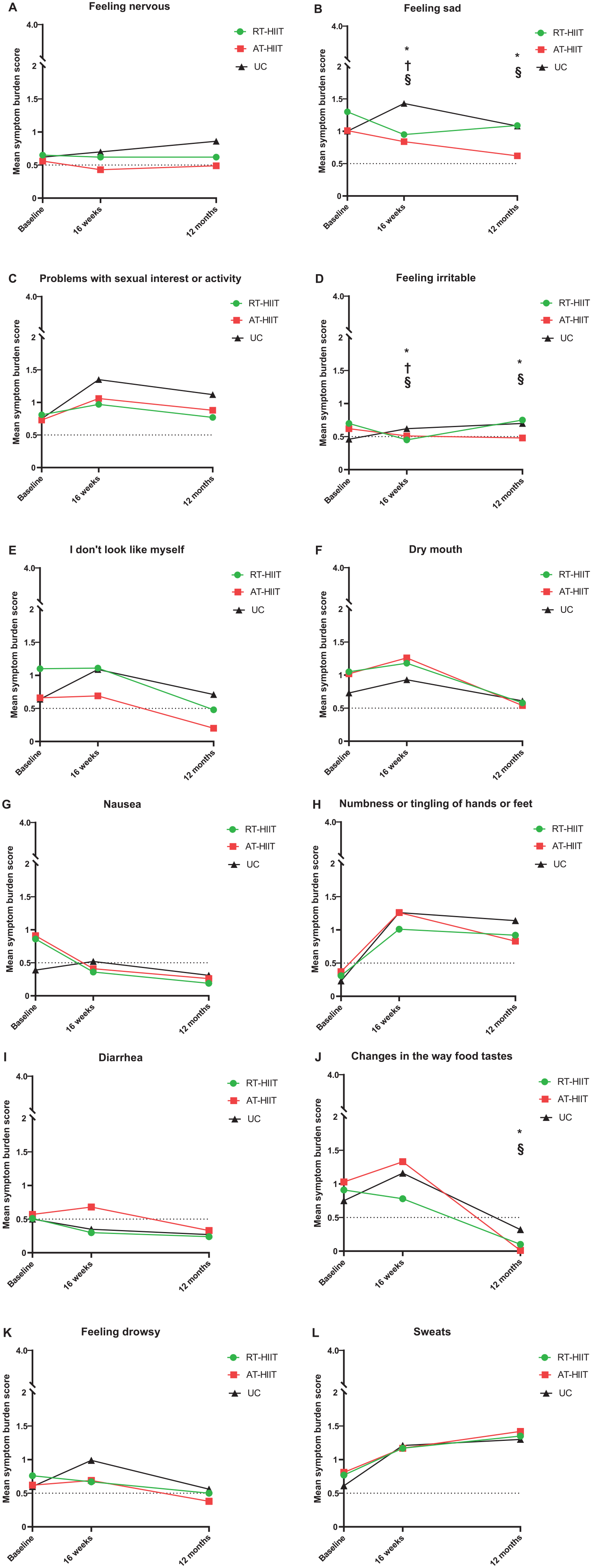
Core symptoms and change in mean symptom burden score over time.
At 16 weeks, patients in both exercise groups reported significantly lower symptom burden scores for “feeling sad” (RT-HIIT vs UC: ES = −0.69; AT-HIIT vs UC: ES = −0.56) and “feeling irritable” (ES = −0.41 RT-HIIT; ES = −0.31 AT-HIIT), compared with the UC group. At 12 months, the AT-HIIT group had significantly lower scores for “feeling sad” (ES = −0.44), “feeling irritable” (ES = −0.44), and “changes in the way food tastes” (ES = −0.53), compared with the UC group.
No adverse events were reported as a result of the testing or the exercise sessions.
Discus sion
The most important finding from the current analysis was that patients in the OptiTrain cohort who were randomized to AT-HIIT and RT-HIIT reported significantly lower symptom burden scores for “feeling sad” and “feeling irritable” at 16 weeks, compared with UC. This beneficial effect of physical exercise was persistently present in the AT-HIIT group at 12 months post-baseline. Results from this analysis provide important new insights in alleviating symptom burden through physical exercise interventions and offer potential self-care strategies in this relatively large subgroup of cancer patients.
The symptom clusters were labelled after the main origin of symptoms in the respective clusters, that is, emotional, treatment-related toxicity, and physical symptoms. The symptoms included in the emotional and physical symptom clusters in our patient cohort are largely overlapping with those in previous studies in patients with breast cancer.10,13,15,16,26 In the current study, the treatment-related toxicity symptom cluster consisted of various symptoms, for example, “changes in the way food tastes,” “dry mouth,” and “nausea,” that were partially overlapping with previously reported gastrointestinal symptom clusters.15,16 Participants in the current study had already received 1 course of chemotherapy, contrary to the study by Browall et al, 16 and thereby were already experiencing a range of treatment-induced side effects at baseline. This can be an explanation for the (partial) difference in symptoms present in the cluster, compared with other studies. 16 All symptom clusters showed a number of consistently present individual core burdensome symptoms, as well as several symptoms entering and exiting the clusters at the respective study assessments.15,16 These changes have also been observed in the other longitudinal studies assessing symptom clusters in patients with (early-stage) breast cancer and reflect the dynamic nature of symptom clusters.15,16 This can be explained by differences in the treatment phase at the 3 study assessment time points, the use of high symptom burden scores (>0.5) as cutoff for the PCA, as well as the low absolute number of symptoms in the symptom clusters at the 12-month post-baseline assessment.
In the emotional symptom cluster, at 16 weeks post-baseline, a beneficial effect in both exercise groups was found for the core burdensome symptoms “feeling sad” and “feeling irritable,” compared with UC; and this effect was preserved at the 12-month post-baseline assessment in the AT-HIIT group.
Several physiological as well psychological mechanisms may contribute to this positive effect of physical exercise on emotional well-being. Elevated serum endorphin concentrations, released by intensive aerobic exercise, have been associated with changes in mood state (eg, euphoria), altered pain perception, and responses to several hormones, such as cortisol.27,28 Previous findings from the OptiTrain study showed that patients in the RT-HIIT group reported significantly lower pain sensitivity than those in the UC group at 16 weeks post-baseline. 25 In addition, a number of psychological hypotheses can explain these results. The “distraction hypothesis” describes that exercise provides distraction from negative and worrying thoughts, leading to a “mental time-out,” which can, in turn, cause a mood-lifting effect. 29 Furthermore, the “mastery hypothesis” implies that the effects of completing an effortful task, such as exercise, could bring out a feeling of mastery which, in itself, elevates mood. 27 Supporting the mastery hypothesis, beneficial effects were previously found for “role functioning” in the RT-HIIT group at 16 weeks. 18 Moreover, the “self-efficacy hypothesis” highlights the importance of self-regulation and self-empowerment. Patients are more likely to maintain adherence to self-set goals when they experience a higher level of perceived self-efficacy. 30
This positive effect of physical exercise on emotional well-being might also be linked to increased activity levels after completion of the intervention. A study in breast cancer patients demonstrated that patients who participated in a physical exercise intervention (consisting of various resistance and flexibility exercises) during chemotherapy had higher levels of physical activity 60 months after completing the intervention, and it reported a more positive mood state than those in the control group. 31 In the OptiTrain cohort, the majority of patients in all 3 groups reported being more physically active at 12 months compared with baseline testing, even though no significant between-group differences were found. 17
Previous articles, a literature review in breast cancer patients and a randomized controlled trial in a geriatric population, confirmed that specifically aerobic exercise preserves emotional well-being.32,33 The underlying mechanisms that support the specific positive effect of aerobic exercise on emotional well-being are unclear. There might be a connection with the neurobiological mechanisms, mediated by factors such as brain-derived neurotrophic factor, insulin-like growth factor 1 (IGF-1), and vascular endothelial growth factor, but there are no hard data supporting this hypothesis.34-36
Notably, patients in all 3 study arms reported the core burdensome symptom “problems with sexual interest or activity” consistently high throughout all study assessments. Sexual dysfunction in breast cancer patients is a clinically relevant problem that is known to increase during chemotherapy, persists long after completion of oncological treatment,37,38 and can lead to changes in body image with a negative impact on quality of life.39,40 However, it is a topic not regularly brought up by either physicians or patients, due to various personal and cultural reasons. 41
Our data highlight the long-term beneficial effects of physical exercise interventions on the burdensomeness of emotional symptoms. These findings underscore the need for awareness of physicians and nurses involved in care for breast cancer patients for such emotional symptoms, including mood disturbances and sexual dysfunction, and confirm that physical exercise can be an effective self-care strategy to ameliorate such problems.
In the treatment-related toxicity cluster, a significant beneficial effect of AT-HIIT was recorded for “changes in the way food tastes” at 12 months post-baseline, with a medium effect size. Chemotherapy, particularly taxane-based chemotherapies, affect gustatory function through various mechanisms and cause temporary taste changes. 42 Studies show that taste changes usually recover within 6 months of chemotherapy completion.42,43 This is in line with the trajectory of “changes in the way food tastes” that we observed in our cohort, where patients in all 3 study arms reported lower symptom burden scores at the 12 months post-baseline study assessment. The reason why patients in the AT-HIIT group reported lower symptom burden of taste changes is not known, but it might relate to more successful coping strategies 15 that results in a lower rate of self-perceived complaints.
The physical cluster consists, in part, of various menopausal symptoms patients experience during treatment, either caused chemotherapy-induced menopause and/or side effects from endocrine therapy. 44 The physical exercise intervention showed no significant effect on “feeling drowsy” and “sweats” in the RT-HIIT and AT-HIIT group at 16 weeks and 12 months. This is in line with a previous study, where no statistically significant effects of physical exercise on endocrine symptoms were found. 45
A recent review underscored the need for establishing efficacious interventions for alleviating various symptom clusters in cancer patients. 46 Up to now, only mind-body and cognitive-behavioral strategies interventions showed limited beneficial effects on symptom clusters47-49; all studies demonstrated beneficial effects on pain, fatigue, and emotional symptoms,47,48 and one of the studies also found beneficial effects on gastrointestinal symptoms. 49 The present analysis is, to our knowledge, the first to explore the effect of (2 different) physical exercise interventions on the presence of symptom clusters, as well as on core burdensome symptoms within these clusters.
Physical exercise can be promoted in the clinical setting as an effective supportive self-care intervention for women with early breast cancer, 50 and our study confirms that such an intervention can lead to improved emotional well-being.
The main strengths of this analysis are a long follow-up period and the detailed description of clusters of burdensome symptoms in 2 types of supervised exercises regimens. Limitations of this analysis include that the first study assessment was performed after 1 course of chemotherapy that influenced symptom burden in our analysis due to acute side effects of chemotherapy treatment.
Conclusion
In conclusion, the current analysis showed that RT-HIIT, AT-HIIT, and UC displayed “emotional,” “treatment-related toxicity,” and “physical” symptom clusters with a dynamic composition over time. Furthermore, both participants in the resistance or aerobic training combined with high-intensity interval training groups experienced an amelioration of burdensome emotional symptoms, such as “feeling sad” and “feeling irritable.” This effect was seen directly after chemotherapy completion and persisted up to 12 months post-baseline for the AT-HIIT group, which underscores the potential value of physical exercise during curative breast cancer treatments as a way to improve and maintain emotional well-being in patients with breast cancer.
Footnotes
Acknowledgements
The authors would like to thank the participants in the OptiTrain Trial, Karolinska University Hospital, for the use of their facilities, and Malin Backman for the collection of questionnaire data and supervision of the exercise sessions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swedish Cancer Society (130452, CAN 2016/334 to YW), the Cancer Society of Stockholm (131242 161262 to YW), the Swedish Cancer and Traffic Accident Foundation (F-C-001225 to YW), the Strategic Area in Health Care Sciences at Karolinska Institutet (Fellowship to KAB), and the Swedish Society for Medical Research (SLS 50514 to Helene Rundqvist). The funders have no role in the study design, data collection or analysis, decision to publish, or preparation of the article.