
Abstract
Retroperitoneal sarcomas are rare. Dedifferentiated liposarcomas (DDLs) are high-grade tumors with a high propensity for local recurrence and metastasis and are associated with reduced survival. Radical resection remains the standard treatment of sarcomas. Meanwhile, Viscum album L. extract (VAE) is used in cancer patients owing to its cytostatic and immunomodulating effects and to its ability to improve patients’ quality of life.
Case Presentation:
A 68-year-old male patient underwent a resection of a DDL (T2 N0 M0, FNCLCC grade 2, stage IIIA) in the retroperitoneum. Three months after this first surgery, a recurrence occurred, and was treated with neoadjuvant and adjuvant doxorubicin plus ifosfamide and surgery (resection). A second recurrence—11 months after the second surgery—was treated with surgery and radiotherapy. The patient then began to undergo VAE treatment (0.2 mg-2 mg, subcutaneously, thrice a week). After the VAE treatment was initiated, the patient reported improved quality of life. A third recurrence—12 months after the third surgery—was treated with surgery, radiotherapy, and with an increased dose of VAE (20 mg). Sixty-nine months (5.8 years) after the fourth surgery a fourth recurrence occurred. It was again treated with surgery, along with a month of intravenous VAE infusions and subsequent subcutaneous VAE (20 mg) treatment. Finally, a fifth recurrence—5 months after the fifth surgery—was treated with subcutaneous and intravenous VAE applications and eribulin. The patient died 11 months after the last recurrence; he received a total of 103 months (8.6 years) of VAE treatment and achieved 10.5 years of survival.
Conclusion:
The case presented herein shows a long-time survival and a prolonged recurrence-free interval in a patient with retroperitoneal DDL treated with surgery, chemotherapy, radiotherapy, and VAE injections. On the basis of the antitumoral and immunomodulating effects of VAE and on the reported prolonged survival of VAE-treated patients with other types of tumors, the adjunct VAE treatment is presumed to have contributed to the favorable outcome. Regarding the clinical relevance of VAE treatment, further investigations are needed.
Introduction
Retroperitoneal sarcomas account for 10% to 15% of all soft tissue sarcomas, that is, approximately 2.7 cases per million population in the U.S. 1 Seventy percent of the cases are liposarcomas that appear to arise from the precursors of adipocytes. 2 This pattern of development makes retroperitoneal liposarcomas extremely rare tumors, accounting for only 0.1% of all malignancies. 3 The pathological subtypes of liposarcomas according to the WHO classification are as follows: well-differentiated liposarcoma (WDL), dedifferentiated liposarcoma (DDL), myxoid liposarcoma, pleomorphic liposarcoma, and liposarcoma not otherwise specified (NOS). 4 DDLs are defined as non-lipogenic sarcomas that are juxtaposed to WDL; they may occur as a recurrence of WDL or may arise de novo (90%). 5 DDLs are high-grade tumors that demonstrate an aggressive local growth and an increased risk of local recurrence and tumor-related death. 2
Radical surgical excision remains to be the mainstay of treatment. 5 Because of the typically large size and anatomic complexity of these tumors upon diagnosis, a resection with microscopically negative margins is often not achieved and thus locoregional recurrence frequently occurs. Approximately 25% of patients will develop distant metastatic disease after the successful treatment of their primary tumor. The risk of metastasis increases to 40% to 50% in tumors measuring >5 cm, in tumors located in the deep fascia, and in intermediate- or high-grade tumors. 6 The 5-year disease-specific survival rates range from 20% to 69%, 7 and the most important predictive factor for survival is tumor resectability. 8 The reasons for unresectability are an extensive vascular involvement (aorta, vena cava, and/or iliac vessels) or the presence of multiple peritoneal implants. 9
Viscum album extracts (VAEs) are obtained from European mistletoe (V. album L.), a hemiparasitic shrub that grows on different host trees (eg, ash [fraxini], apple [pini], oak [quercus], pine [pini]); VAEs contain various bioactive substances, the most studied of which are viscotoxins and mistletoe lectins. 10 Numerous studies have shown that VAE demonstrates strong cytotoxic and apoptosis-inducing effects, stimulates immune reactions, inhibits tumor cell migration and neo-angiogenesis, and downregulates various cancer genes involved in tumor progression.11-16 VAE is used as an injectable standardized preparation and is administered parenterally (subcutaneous and intravenous); the dosing schedule of VAE is increased based on individual patient responses. The intratumoral or intracavitary application of VAE at high dosages has been reported occasionally.17-20 Studies found that VAE improved the quality of life of patients21,22 and had promising effects on prolonging the survival time23,24 of cancer patients. Small trials and single case reports have described partial and complete tumor remissions usually after local high-dose VAE applications.25-28 To the best of our knowledge, this is the first reported case of DDL treated with VAE. However, the use of VAE has been studied in other types of sarcomas. In a randomized study with long-term follow-up, adjuvant VAE treatment prolonged the post-relapse disease-free survival after the second relapse in osteosarcoma patients (106 months [2-144] vs 7 months [3-134]). 29 In this study, no relapse was observed in 5/9 patients in the VAE arm, whereas all patients in the etoposide arm showed relapses (HR = 0.287, 95% CI: 0.076-0.884, P = .03). As described in a case report, the recurrent malignant fibrous histiocytoma (undifferentiated pleomorphic sarcoma) in the left lower extremity of a patient remitted after 12 intratumoral VAE applications; the patient remained recurrence-free for 15 months under continuous subcutaneous VAE treatment. 30 Moreover, case series and preclinical studies have reported promising results for the treatment of sarcomas or sarcoma cells with VAE.31-34
Case Presentation
A 68-year-old Peruvian man had been suffering from lumbar pain for several days. His CT scan revealed a mass compressing his right ureter and iliac vessels. He underwent exploratory laparotomy with radical resection of a retroperitoneal tumor (10 cm × 8.3 cm × 8 cm), as well as ileocecectomy and ileocecal anastomosis. Pathological analysis (Figure 1) showed that the tumor was a DDL (T2 N0 M0, FNCLCC grade 2, stage IIIA, <50% necrosis, R0). This diagnosis was corroborated by immunohistochemistry markers (ie, the positivity of D33 and NSE and negativity of h-CD and S100). One month after the surgery (for details of the disease course, see Figure 2), his initial postoperative scan showed the absence of disease. However, 2 months later (3 months after the surgery), his new CT scan revealed a 1.6 cm × 2.3 cm mass anterior to the right iliac vessels (first recurrence). He received neoadjuvant chemotherapy with doxorubicin plus ifosfamide (6 cycles). Then he underwent resection of the retroperitoneal tumor (R0) and right ureterectomy. The patient further received 3 cycles of doxorubicin plus ifosfamide postoperatively. Eight months after chemotherapy (11 months after the second surgery), a control imaging revealed 2 anterior psoas masses measuring 1.5 cm × 1.5 cm and 1.3 cm × 1 cm (second recurrence). The biopsy of one of the lesions revealed a malignant spindle cell neoplasm compatible with DDL. Two months later, the CT scan showed that the masses had enlarged to 3.0 cm × 1.9 cm and 2.1 cm × 1.6 cm. However, CT scans and a chest x-ray revealed no evidence of metastatic disease. The patient underwent a third surgery wherein the 2 masses and a right pelvic mass were resected entirely (R0). At this point, the patient sought for different treatment options involving an integrative approach. Three months later, he came to the Centro Médico Antroposófico (CMA) and became our patient.
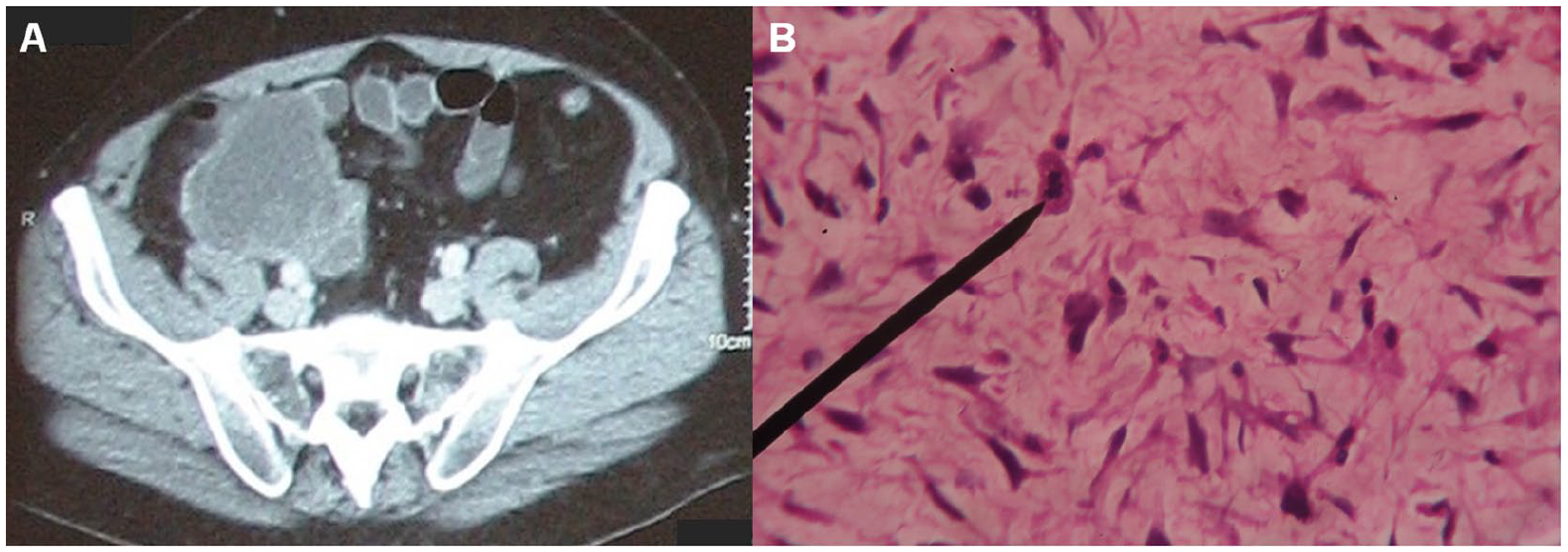
Primary tumor of the patient. (A) Heterogeneous soft tissue tumor with irregular borders at the retroperitoneum in the right iliac fossa. (B) Biopsy of the tumor (×40): dedifferentiated liposarcoma FNGCLCC grade 2, abnormal mitosis.
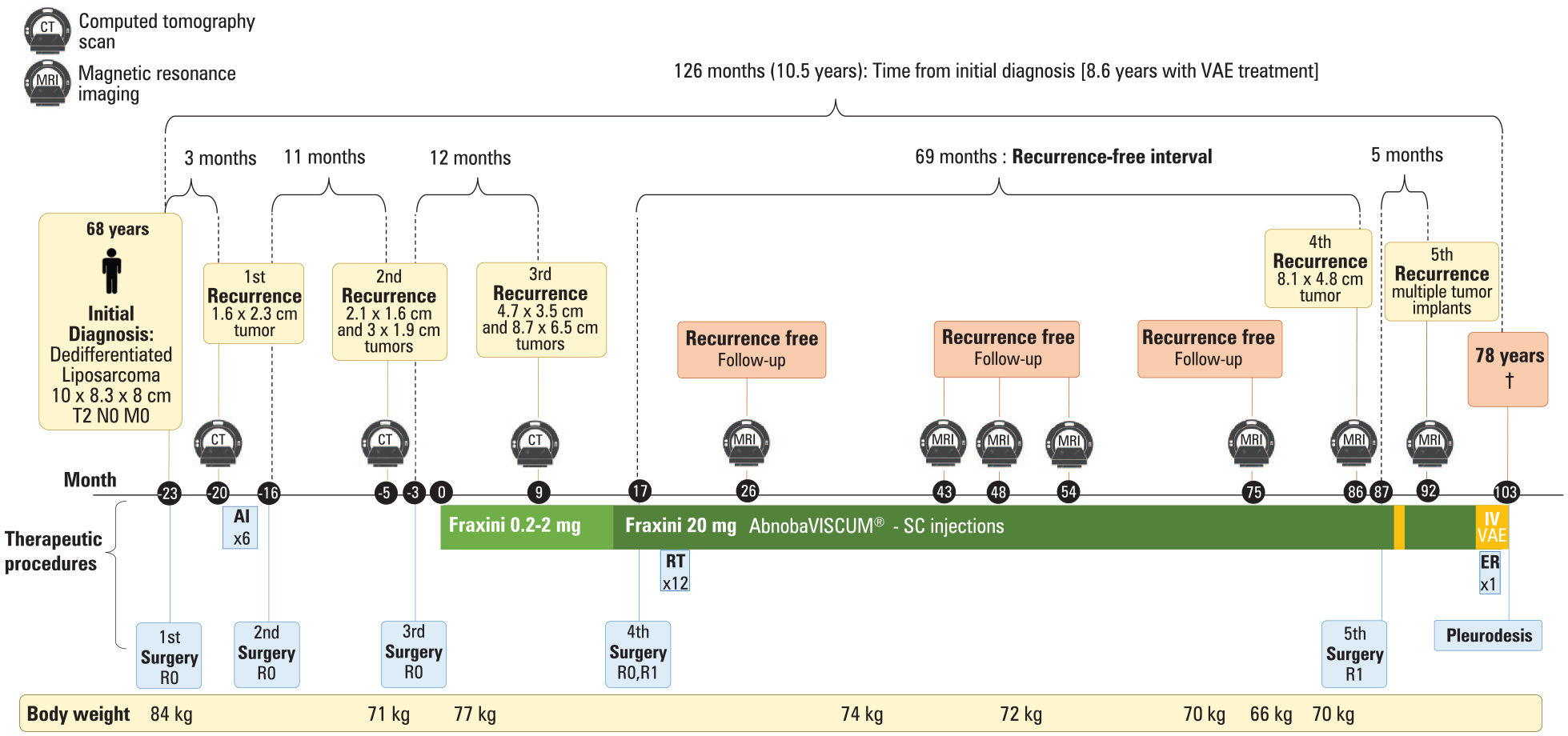
Timeline of the patient with recurrent retroperitoneal dedifferentiated liposarcoma.
The recommended treatment was subcutaneous injections of VAE obtained from the host tree ash (AbnobaVISCUM® Fraxini); the injections were given thrice per week in increasing doses. The application of VAE Fraxini in the periumbilical area started at 0.2 mg; after 6 months, the dose was increased to 2 mg, which was then maintained for 7 months. The subcutaneous VAE injections occasionally induced self-limited local erythema and swelling of the skin around the application site, which could be tolerated by the patient. Nine months after the VAE treatment was initiated (12 months after the third surgery), a retroperitoneal mass measuring 4.1 cm × 3.0 cm was noticed (third recurrence). After 5 more months, the dose of VAE was increased to 20 mg thrice per week. Three months later, the patient underwent resection (fourth surgery) of a right iliac fossa tumor (a mass measuring 4.7 cm × 3.5 cm with a moderate amount of surrounding fibroadipose tissue) and a right juxtarenal psoas tumor (a well-encapsulated, focal fibro-fatty soft tissue measuring 8.7 cm × 6.5 cm with central areas of probable necrosis). Both tumors were DDLs (FNCLCC grade 3, pT2b). The patient had a negative margin resection (R0) for the larger sarcoma, and the other exhibited focal involvement by the tumor. A cholecystectomy (mild chronic cholecystitis and cholelithiasis) and appendectomy were also performed, and both organs were negative for tumor. Additionally, he received 12 cycles of three-dimensional conformal radiotherapy post-surgery.
As a result of the previous surgeries, which involved a partial right ureter resection with psoas bladder hitch, the patient developed obstructive renal failure as evidenced by the right ureteral obstruction and abnormal serum creatinine levels. The patient then underwent a right percutaneous nephrostomy with stent placement.
Throughout this time, the patient continued to receive VAE Fraxini. Follow-up magnetic resonance imaging was performed periodically post-surgery. Three-month breaks without VAE Fraxini application were set twice per year after obtaining the first negative follow-up magnetic resonance imaging result. The frequency of subcutaneous VAE Fraxini application was reduced to twice per week from month 54 on. The patient reached a recurrence-free interval of 69 months; however, the magnetic resonance imaging performed on month 86 of VAE Fraxini treatment showed a mass in the right iliac fossa. The tumor measuring 8.1 cm × 4.8 cm (FNCLCC grade 3, pT2b) was resected. The tumor showed areas of well-differentiated liposarcoma, which were mixed with areas of intermediate to highly dedifferentiated myxoid fibrosarcoma and high-grade undifferentiated pleomorphic sarcoma. The tumor was relatively well-circumscribed and mostly surrounded by fibroconnective and fibroadipose tissues of variable thickness. However, the resection margins were involved by the sarcoma. One month after the surgery, the VAE treatment was resumed. The patient started receiving intravenous infusion of 100 mg VAE obtained from pine as host tree (Helixor® P); the injections were administered in 500 mL of standard saline solution over 2 hours thrice a week. The dose was increased by 100 mg per application until 400 mg was reached which was maintained until 12 applications were completed. Then, the patient was subjected again to subcutaneous injection with 20 mg VAE Fraxini thrice per week. Five months after the surgery, multiple abdominal and retroperitoneal nodular tumor implants were detected, and their number and size increased within the following 9 months. For 2 weeks, the patient received intravenous infusion of VAE (Helixor® P, maximum dose: 400 mg) followed by subcutaneous infusion of 20 mg VAE Fraxini. One of the implants caused urinary tract obstruction, and the patient developed renal and abdominal pain, which was treated with buprenorphine 20 mg/25 cm2 transdermal patches and with anthroposophic remedies (Wala® Solum Inject, Wala® Plexus coeliacus D15, Wala® Bryonia/Stannum, Weleda® Formica comp injections, thrice per week). Weleda® Equisetum sulfuratum tostum D3 was applied (thrice a day) to support the urinary function. When the pain was relieved and controlled, intravenous infusions of VAE were resumed. He also received 1 cycle of eribulin (1.65 mg IV infusion). In month 103 of the VAE treatment, the patient underwent pleurodesis due to pleural effusion; however, he died 2 weeks later. Altogether, the patient received a total of 103 months (8.6 years) of VAE treatment and achieved 10.5 years of survival.
Within approximately 2 years during which the first 3 surgeries were performed, the patient’s weight decreased from 84 kg to 71 kg. Since the VAE treatment started, the patient’s quality of life progressively improved as seen in his increased appetite, resulting in weight gain (up to 77 kg) during the low-dose VAE treatment. After the fourth surgery, his weight was 70 kg to 74 kg. After the fifth surgery, his weight decreased to 66 kg and then increased again to 70 kg (Figure 2). The ideal body weight based on his height (172 cm), gender, and age is 54.7 kg to 74.0 kg.
Antecedents and Concomitant Therapies
The patient was married and had 3 grown-up children. He had a history of tobacco use, but he quit after being diagnosed with DDL. He consumed alcoholic beverages occasionally. His medical history included diphtheria and hemorrhoidectomy. His father died of leukemia, and his paternal uncle had an unknown cancer of the lower extremity. Further medications included allopurinol tablets for high blood uric acid level and a combination preparation of hydrocodone 10 mg and bitartrate and acetaminophen 500 mg tablets for left lumbar region pain. The patient stopped taking these medications on month 18 of VAE treatment.
Discussion
We report herein a case of a male patient with recurrent DDL localized in the retroperitoneum and treated with adjuvant VAE. He received a total of 103 months (8.6 years) of VAE treatment and achieved 10.5 years of survival. The patient died 11 months after the last recurrence of his multiple abdominal and retroperitoneum nodular tumor implants (5 months after his last surgery). With the increased dosage of VAE treatment, he attained a recurrence-free interval of 69 months (5.8 years), while after the 3 previous recurrences the intervals ranged from 3 months to 12 months. The first 4 recurrences were resected surgically. Neoadjuvant and adjuvant doxorubicin plus ifosfamide were administered after the first recurrence, which was followed by a second recurrence after 11 months; after the third recurrence, the patient received radiotherapy as an additional treatment. For the fifth recurrence, the patient received eribulin as yet another additional treatment. VAE was started after the second relapse and was intensified after the subsequent relapses. During the VAE treatment, the patient reported improved quality of life.
A DDL behaves as a high-grade sarcoma with a high propensity for local recurrence and metastasis. Even a patient who undergoes complete tumor resection has high rates of future local recurrence. 35 The 5-year local recurrence rates for DDL is 80% whereas that for WDL is 50%. 3 Our patient underwent surveillance periodically for early detection of recurrences. His first recurrence was 3 months after the primary tumor resection. Then, he received neoadjuvant and adjuvant doxorubicin plus ifosfamide. In different clinical trials, this combined chemotherapy has demonstrated a response rate of up to 12% to 34% depending on the subtypes, and a disease control rate of 45% to 77%.36-38 Our patient showed an improved recurrence-free interval given that his second recurrence appeared 11 months later. The third recurrence appeared after approximately the same interval (14 months). Thus, the VAE dose was increased 10-fold to 20 mg. Most studies described relevant immune stimulation at high VAE dosages. 39 High-dose VAE treatments are applied either subcutaneously, 40 via intravenous infusion, 27 or intratumoraurally 17 to achieve an enhanced tumor control 28 or to substantially improve the quality of life21,22,41-43 with occasional tumor remission.25-27,44,45 Prior to the fourth recurrence, the patient reached 69 months (5.8 years) of recurrence-free interval, during which the patient was subjected to a long-term high-dose VAE treatment and 12 cycles of radiotherapy. Retrospective studies showed that the use of postoperative radiotherapy reduced the risk of local recurrence and extended the recurrence-free interval compared to when radiotherapy was not administered; however, the postoperative radiotherapy exerted no effect on survival.46,47 VAE has been shown to in vitro and in vivo improve DNA-repair of radiation-, ultraviolet radiation-, and cyclophosphamide-induced damage of lymphocytes and further in the gamma-ray damaged peripheral blood mononuclear cells. This radioprotective effect could explain the reduction of adverse effects and the improved tolerability to radiotherapy in cancer patients treated with VAE. 48 Furthermore, there are animal experiments that the combination of VAE and radiotherapy increase the effectiveness of both. 49 Altogether, the 12 cycles of radiotherapy—adjuvant to continuous application of VAE—could result in additional effectiveness. The occasional erythema and swelling around the application site were expected reactions, which indicated immune stimulation and are used as bases for dose adaption. 50
Histologically, a DDL has a broad morphologic spectrum. Usually, it has the appearance of an undifferentiated pleomorphic sarcoma or spindle cell sarcoma with moderate cellularity and cellular atypia, wherein cells are disposed in loose fascicles and display pattern-less distributions with variable degrees of necrosis.2,5 Of the 2 tumors removed during the third recurrence, 1 had a moderate amount of surrounding fibroadipose tissue, whereas the other was well-encapsulated and had a focal fibro-fatty soft tissue with central areas of probable necrosis. Encapsulation is described as the formation of a layer of connective tissue that is interposed between a neoplastic tissue and a normal tissue that encloses the tumor; encapsulation is associated with a better prognosis. 51 Encapsulation of the tumor under VAE treatment has been described in a case report on adenoid cystic carcinoma after intratumoral applications 52 ; moreover, experts have reported that the use of intravenous VAE 53 induced an immune response against colorectal carcinomas. The tumor removed in the fourth recurrence was relatively well-circumscribed and mostly surrounded by fibroconnective and fibroadipose tissues of variable thickness. These features—well-circumscribed and fibroconnective tissue—are the characteristics of the encapsulation process and of benign neoplasms that are frequently removed through surgery. 51
Clinically, the curative management for localized DDL is surgical resection combined with or without radiotherapy. There is an increasing number of studies on new molecular therapeutic targets and chemotherapy for the systemic treatment of patients with advanced or metastatic liposarcoma. For instance, in about 90% of WDL/DDL cases, the oncogene encoding cyclin-dependent kinase 4 (CDK4) is continuously amplified; CDK4 is a crucial promoter of cell proliferation. 54 Thus, CDK4 expression was higher by approximately 10-fold in WDLS/DDLS than in normal fat tissue. 55 Palbociclib—a CDK4/6 inhibitor—showed a certain degree of efficacy in the treatment of CDK4+ WDL/DDL, reaching a 66% progression-free survival (PFS) rate at 12 weeks and a median PFS of 18 weeks. However, palbociclib demonstrates a grade 3 to 4 toxicity as seen in the occurrence of neutropenia (50%) and thrombocytopenia (30%). 56 Meanwhile, VAE preparations (Viscum alone and Viscum + TT) have showed a strong downregulation of CDK4 in 3 osteosarcoma cell lines (U2OS, 143B, and Saos-2). 57 In the fifth recurrence, our patient received eribulin, a microtubule inhibitor used after an anthracycline-containing regimen; the use of eribulin demonstrated an overall survival advantage in liposarcoma and leiomyosarcoma. 58
The reported 5-year overall survival for WDL (grade 1), grade 2 DDL, and grade 3 DDL were 93%, 57%, and 21%, respectively. 59 The prognostic factors after the resection of locally recurrent retroperitoneal sarcomas are recurrence-free interval length, surgical clearance, and histology. Long-term tumor control and survival rates are poorer for patients with high-grade histologies,2,5 with rapidly progressing tumors, 3 with short recurrence-free intervals, 60 and with resected tumors with a positive margin.35,60 Our patient achieved 10.5 years of survival with improved quality of life.
There is experimental evidence that the bioactive principles of VAE and especially mistletoe lectins and viscotoxins—alone or in combination—show anti-tumor properties by inducing apoptosis,14,61 by cell cycle interaction causing a substantial delay in progression to S phase, 62 by affecting tumor angiogenesis13,63 and by gene modulation in tumor cells.64,65 Mistletoe pharmaceutical preparation has also been reported to contain molecular compounds that inhibit glycoprotein P (Gp-P), 66 a protein that acts as a transmembrane drug pump and is part of the ABC multiple extrusion carrier proteins (ABCB1). This intentional inhibitory effect can lead to an increase in the cytoplasmic concentration of the drugs (chemotherapeutic agents) and their cytotoxicity. 67 Furthermore, some of the immunological activities of VAE from preclinical and clinical studies include the increase of leukocytes, eosinophils, granulocytes, and lymphocytes;68,69 the induction of specific antibodies against VAE constituents; 70 the increase of activity of natural killer cells 69 and granulocytes 71 and the secretions of cytokines; 72 and the enhancement of dendritic cell maturation, 73 cellular, and humoral immune response. 74 The immunomodulating effects of VAE75-77 (enhancing the host defense system to promote tumor control) and possibly the antitumoral properties of VAE, along with the reports on prolonged survival of VAE-treated patients with other types of tumors,24,27,44,78 have led us to presume that the adjunct VAE treatment contributed to the favorable outcome in our patient. Regarding the current state of evidence, this paper presents a single case, so VAE applications cannot replace surgery or other effective anticancer treatments.
Conclusions
The case presented herein describes the long-time survival and the prolonged recurrence-free interval in a patient with retroperitoneal DDL treated with surgery, chemotherapy, radiotherapy, and long-term VAE injections. On the basis of the antitumoral (cell cycle delay and apoptosis induction) and immunomodulating effects of VAE and based on the reported prolonged survival of VAE-treated patients with other types of tumors, the adjunct VAE treatment is presumed to have contributed to the favorable outcome in our patient. Further investigations are needed to investigate the clinical relevance of VAE treatment in sarcomas.
Footnotes
Acknowledgements
We thank Dr. Cesar Vela-Velasquez from the Instituto de Investigación de Citopatología (CITOPAT) for the histological images and Dr. Yober Espinoza Zárate from “Centro Médico Antroposófico (CMA)” for MRI/CT scan images and reports. This case report was prepared following the CARE guidelines. 79
Authors’ Contributions
M.R. conceptualized this report, wrote the manuscript, and prepared the graph. Y.V. was the treating physician, provided the patient information, and reviewed the manuscript. P.W., G.S.K., and H.K supervised the writing of the report and the publication process and reviewed the manuscript. All authors have read and approved the final version of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by “Stiftung Integrative Medizin, Stuttgart, Germany and Christophorus Stiftung, Stuttgart, Germany [263 CST]”.
Informed Consent
Written informed consent regarding the publication of the patient’s medical report and the accompanying images was obtained from the patient himself before his death.