
Abstract
Objective:
The aim of this systematic review and meta-analysis of randomized controlled trials (RCTs) was to evaluate the effects of acupuncture and moxibustion (AM) in women with breast cancer-related lymphedema (BCRL).
Methods:
We retrieved RCTs published before January 24, 2021, from the MEDLINE, EMBASE, Cochrane Library, Web of Science, China National Knowledge Infrastructure (CNKI), Chongqing VIP (VIP), and Wanfang databases. RCTs that compared acupuncture and/or moxibustion intervention with other treatments were included. A random effects or fixed effects model was used based on the heterogeneity findings. Study quality was evaluated using the Cochrane risk of bias tool.
Results:
We included 14 RCTs in the analyses, of which 4 RCTs adopted acupuncture, 4 RCTs used moxibustion, and the rest used both. AM significantly reduced arm circumference at the elbow crease compared to routine care (Mean deviation (MD) = −7.26, 95% confidence interval (CI) = −8.30 to −6.21, P < .00001). There was a significant difference between AM and diosmin tablets in the effective index for upper limb lymphedema (MD = 24.68, 95% CI = 24.82-30.53, P < .00001), the range of motion of the shoulder during protraction (MD = 6.77, 95% CI = 2.81-10.73, P = .0008), and adduction (MD = 4.17, 95% CI = 1.02-7.32, P = .01). There was a significant difference between moxibustion and pneumatic circulation (MD = −0.51, 95% CI = −0.85 to −0.17, P = .003) in the visual analog score (VAS) for swelling. Finally, compared to the blank control, acupuncture reduced the VAS for pain (MD = −1.33, 95% CI = −1.52 to −1.15, P < .00001; heterogeneity (I2) = 0%, P = .57).
Conclusion:
Our results suggest that AM is effective in the treatment of BCRL. AM may reduce arm circumference at the elbow crease (compared to routine care), increase effective index for upper limb lymphedema (compared to oral diosmin tablets), improve the range of motion of the shoulder during protraction and adduction (compared to oral diosmin tablets), and decrease the VAS for both swelling (compared to pneumatic circulation) and pain (compared to blank control).
Introduction
Breast cancer (BC) is the most frequently diagnosed cancer among women worldwide, and its incidence is gradually increasing. 1 Fortunately, with the advancement of early screening and diagnosis, the 5-year survival rate of BC patients is almost 90%. 2 However, these survivors are at an increased risk of long-term complications because of surgery as well as radiation-related therapeutic exposures. 3 BC-related lymphedema (BCRL) is one of the most frequent complications of BC and its treatment procedures, which has a profound effect on the patients’ quality of life and upper limb function. 4 Further, swelling can cause physical discomfort such as fatigue, stiffness, pain, heaviness, tension, numbness, and restricted mobility, which can trigger mental disorders and anxiety in women with lymphedema.5,6
Lymphedema cannot be completely cured, although there are some methods for its prevention and management. 7 Consequently, limiting the development of edema and improving symptoms have become a common challenge faced by clinicians and patients. Current treatments for BCRL include education during the decompression phase, the use of fitted compression garments during maintenance, manual lymphatic drainage, compression bandaging, and exercise; but the efficacy of these measures remains uncertain. 7
Acupuncture and moxibustion (AM) have long been used in the treatment of various diseases and physiological disorders in Chinese medicine, and it is becoming increasingly popular worldwide. Acupuncture involves the insertion of fine metal needles into specific areas of the body (acupuncture points or acupoints) to facilitate the recovery of health. In contrast to the mechanical stimulation of acupuncture, the effect of moxibustion is mainly realized by thermal stimulation when the moxa stick is ignited. Clinically, acupuncture and moxibustion can be used alone or in combination. In recent years, studies have been conducted on the treatment of BCRL with AM, and preliminary results have shown the therapeutic potential of AM. Some studies have demonstrated that AM may stabilize symptoms and reduce arm circumference in cases with BCRL.8-10 Some studies suggest that AM is well tolerated, but there is no significant advantage in changing the arm circumference of BCRL patients.11,12 These differences may be due to different study designs, statistical analyses, and sample sizes. Therefore, it is crucial to determine whether AM is safe, feasible, and effective in patients with BCRL. Here, we performed a systematic review and meta-analysis of clinical randomized controlled trials (RCTs) to answer this question.
Methods
This protocol followed the PRISMA guidelines (http://www.prisma-statement.org/). Our study was registered on the PROSPERO website with identifier CRD42021241686.
Literature Search
We searched the relevant English/Chinese medical literature in the MEDLINE (via PubMed), EMBASE, Cochrane Library, Web of Science, China National Knowledge Infrastructure (CNKI), Chongqing VIP Chinese Science and Technology Periodical (VIP), and Wanfang databases, published until January 24, 2021. The search terms used were as follows: breast neoplasms, breast cancer, breast carcinoma, lymphedema, acupuncture, needle, needling, moxibustion, moxa, moxabustion, moxacone, randomized controlled trial, controlled clinical trial, randomly, and RCT. Chinese translations of these search terms were used for the Chinese databases. The database search strategy is provided in Supplemental Appendix 1. Unrelated articles were automatically excluded based on their titles and abstracts. We read the rest of the articles carefully to see if they met the selection criteria. All searches were independently conducted by 2 researchers, and a third researcher arbitrated the disputes.
Study Selection Criteria
Types of studies
RCTs were included.
Types of participants
The patients were women with lymphedema, which was caused by BC and its treatment procedures (surgery and/or radiotherapy). There were no restrictions on participants’ BC stage, lymphedema grade, age, or country.
Types of interventions
In the treatment group, only needle acupuncture was allowed, and other forms of acupuncture (such as point injection, laser acupuncture, or electroacupuncture) were not allowed. Similarly, for moxibustion treatment, only burning Artemisia vulgaris was allowed and other herbs were not included. The treatment group received acupuncture and/or moxibustion without any restriction of manipulation techniques. The control group received any other treatment except acupuncture or moxibustion.
Types of outcomes
Any result involving changes in edema was considered a primary outcome, which was assessed by measuring the circumference of the arm or the volume of the fluid content in the limb. The secondary outcomes included visual analog score (VAS) for swelling/pain, range of motion (ROM), quality of life scores, bioimpedance, and the rate of AM-related adverse events (AEs) (such as bruises, hematomas, pain, allergies, burns, local infections, cough, or nausea).
Articles that met any of the following conditions were excluded: (1) unavailable original full text, (2) duplicating published literature, (3) incomplete or missing research data, (4) studies without comparable baselines, and (5) animal experiments, letters, reviews, or commentaries.
Quality Assessment and Data Extraction
Cochrane Risk of Bias Assessment tool (Cochrane Collaboration) was used to assess the risk of bias. 13 The following types of bias were assessed: (1) random sequence generation, (2) allocation concealment, (3) blinding of participants and personnel, (4) blinding of outcome assessment, (5) incomplete outcome data, (6) selective reporting, and (7) other bias. Each item was classified into 3 types: low-risk, high-risk, and unclear risk. The quality of the included trials was independently evaluated by 2 reviewers, and disagreements were resolved by a third researcher.
Equivalent information collected from the selected studies: first author’s name, year of study, age of the participants, sample size, inclusion criteria, status of lymphedema, intervention, primary acupoints, course of treatment, retention time, and outcomes. Two researchers checked the extracted data for consistency, and a third researcher arbitrated any dispute.
Statistical Analysis
Dichotomous data were analyzed using odds ratio with 95% CIs. For continuous outcomes, data were analyzed using the mean difference with 95% CIs. A meta-analysis of the trials was carried out when at least 2 trials that analyzed the data for a specific outcome were included.
Heterogeneity among the studies was detected using P and I2 statistics. 14 A random effects model was adopted when heterogeneity was observed (P < .05 and/or I2 > 50%); otherwise, a fixed effects model was adopted. Subgroup and sensitivity analyses were performed to dissect the heterogeneity. Clinical heterogeneity was defined as differences in participants, treatment, outcome characteristics, or research setting. When more than 10 studies were included, publication bias was investigated using the funnel plot, Begg’s test, and Egger’s test. A significant difference was assumed at P < .05.15,16
All data were analyzed using the STATA 12.0 (StataCorp LP, College Station, TX, USA) and RevMan 5.3 (Cochrane Collaboration, Oxford, UK) software.
Results
Study Selection
The PRISMA flow diagram (Figure 1) displays the selection process. 17 We found 822 articles by searching the databases (MEDLINE, EMBASE, Cochrane Library, Web of Science, CNKI, VIP, and Wanfang). After excluding 69 duplicate articles, 2 researchers conducted independent review and exclusion. Based on the title and abstract, 713 articles did not meet the selection criteria and were excluded. Of the remaining 40 papers, 24 were excluded for the following reasons: 3 studies were duplicated, 3 studies were not RCTs, the population did not include BCRL patients in 7 studies, in 10 studies the experimental intervention was not acupuncture and/or moxibustion, and 3 articles did not report relevant outcomes. Finally, 1412,18-30 articles were included in our analysis.

Flow diagram of studies selection.
Study Characteristics
Fourteen RCTs with 758 participants were included in this review. Four12,20,21,29 of the included RCTs were published in English, and the remaining18,19,22-28,30 were published in Chinese. One RCT 12 was conducted in the USA, 1 RCT 20 was conducted in Australia, and the remaining18,19,21-30 were conducted in China. The results of 13 RCTs12,18,19,21-30 involved changes in arm circumference, but the measurement methods were not uniform. The secondary outcomes in the included RCTs were bioimpedance, shoulder joint ROM, VAS for pain, VAS for swelling, quality of life scores, and AEs. Four studies12,20,28,29 described the follow-up. The summarized characteristics of the 14 RCTs are presented in Table 1.
Characteristics of Included Randomized Controlled Trials.

Abbreviations: AE: adverse event; UK: unknown; N: number of patients; EIL: effective index for upper-limb lymphedema, EIL (%) = (upper-limb arm circumference before treatment – upper-limb arm circumference after treatment)/(upper-limb circumference of the affected arm before treatment – upper-limb circumference of the unaffected arm before treatment); ROM: range of motion; QLQ – Likert: Likert scale was used to evaluate quality of life; VAS: visual analog score; QOL-UK: unknown quality of life scale; EORTC – QLQ: Core Quality of Life Scale developed by the European Organization for Research and Treatment of Cancer; QLQ – CCC: Chemobiotherapy Quality of Life Scale for Cancer Patients in China.
AM and Control Interventions
Of the 14 RCTs, 4 RCTs12,20,23,24 adopted acupuncture, 419,28-30 used moxibustion, and the rest18,21,22,25-27 used both. The most commonly used acupoints were TE.5 (Waiguan), LI.15 (Jianyu), LI.11 (Quchi), LI.14 (Binao), SP.9 (Yinlingquan), TE.14 (Jianliao), and LI.4 (Hegu). The frequency of AM ranged from once a week to once per day. Retention time ranged from 5 to 30 min. The total number of AM treatments ranged from 7 to 45, while the course of AM treatment ranged from 2 to 9 weeks.
In most cases, the experimental group and the control group had a similar treatment frequency. One study 12 used a wait-list control comparison. Four RCTs19,21,25,26 used oral drug therapy as control; 1 study 19 used hydrochlorothiazide and spironolactone, while the rest21,25,26 used diosmin tablets. In 3 studies,23,24,27 the interventions used in the control group were also used as the basic treatment in the experimental group. Three RCTs28-30 chose pneumatic circulation as a control, while the control group in 3 other studies18,20,22 received routine care.
The interventions of each trial are presented in Table 2.
Specific Intervention Measures for the Experimental Group and the Control Group.

Abbreviations: AM: acupuncture and moxibustion; Ashi: this refers to an acupuncture point without a specific name or definite location, the site of which is determined aby tenderness or other pathological responses, also called ouch point; Nt: total number of treatments; UK: unknown; Tid: 3 times a day; Qid: once every other day; Qd: once a day; Bid: twice a day.
Risk of Bias
The risk of bias assessment is shown in Figure 2. All the included trials mentioned randomization. Only 2 studies21,25 did not describe the randomization method in detail, indicating an increased selection bias. Four studies12,20,28,29 emphasized allocation concealment. Due to the characteristics of AM, it was difficult for the practitioners to incorporate blinding. None of the included studies had a clear description of the blinding of outcome assessments. Nine studies18,19,21-27 did not report dropouts, and we assessed the risk of attrition bias of these studies as “unclear.” One trial 20 did not report all the outcomes mentioned in the published protocols in the results, which could cause a high risk of selective outcome reporting. We found 1 trial 12 at low risk, and all outcomes were presented in a pre-specified way. We assessed the risk of the rest18,19,21-30 of the studies as “unclear,” because although they appeared to report all outcomes in their Methods section, the protocol was not available.

Risk of bias. (a) Overall quality assessment. (b) Individual quality assessment.
Changes in Arm Circumference
Effective index for upper limb lymphedema 21 (%) = upper limb arm circumference before treatment−upper limb arm circumference after treatment/upper limb circumference of the affected arm before treatment−upper limb circumference of the unaffected arm before treatment.
Eleven studies12,18,19,22-25,27-30 reported the circumference (cm) of different parts of the affected limb, while 2 studies21,26 reported the effective index for upper limb lymphedema at 10 cm above the elbow. The results are presented in Table 3.
Comparison of Changes in Arm Circumference Between Acupuncture Group and Control Group.
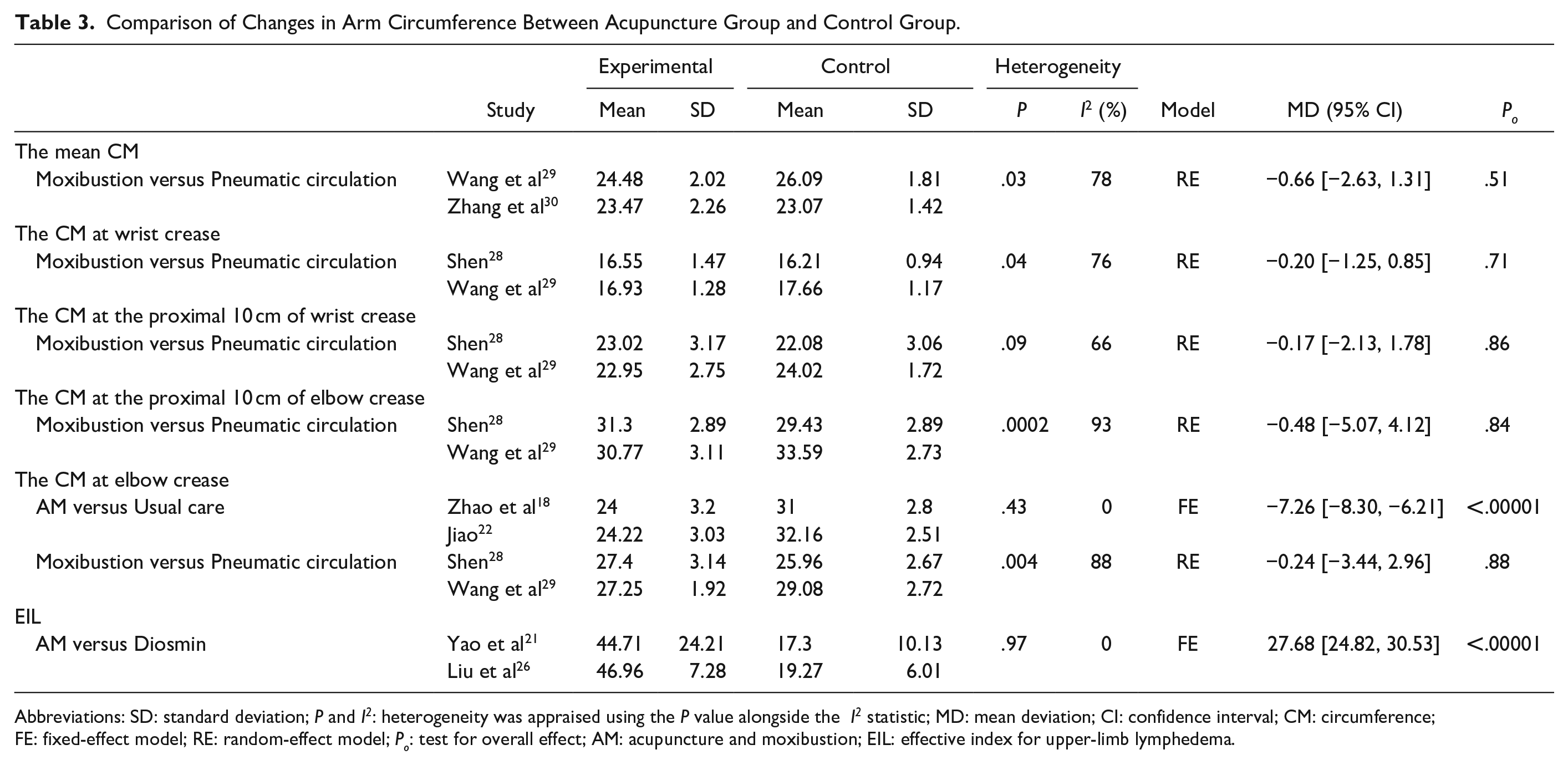
Abbreviations: SD: standard deviation; P and I2: heterogeneity was appraised using the P value alongside the I2 statistic; MD: mean deviation; CI: confidence interval; CM: circumference; FE: fixed-effect model; RE: random-effect model; Po: test for overall effect; AM: acupuncture and moxibustion; EIL: effective index for upper-limb lymphedema.
Regarding the mean arm circumference29,30 (the average value of wrist crease, 10 cm proximal to the wrist crease, elbow crease, and 10 cm proximal to the elbow crease) of the affected side, a random effects model was adopted due to high heterogeneity (I2 = 78%, P = .03). Meta-analysis showed no significant difference between the moxibustion and pneumatic circulation groups (MD = −0.66, 95% CI = −2.63 to 1.31, P = .51). Similarly, no difference was observed at the wrist crease, proximal 10 cm of the wrist crease, or 10 cm proximal to the elbow crease.28,29 However, 2 studies18,22 that compared AM versus routine care at the elbow crease showed a significant difference (MD = −7.26, 95% CI = −8.30 to −6.21, P < .00001; heterogeneity (I2) = 0%, P = .43). Moreover, no difference was found between moxibustion and pneumatic circulation at the elbow crease.28,29 The control and intervention groups of the 2 studies19,25 that were not consistent with the aforementioned studies were not combined for analysis. Four other studies12,23,24,27 only provided the difference between before and after treatment, but did not provide specific values reflecting the circumference after intervention. Additionally, since the outcomes of the 4 studies did not come from the same location on the affected side, the 4 studies could not be combined with each other. Regarding effective index for upper limb lymphedema, we found that there was a significant difference between the AM group and the oral diosmin tablet group (MD = 24.68, 95% CI = 24.82 to 30.53, P < .00001; heterogeneity (I2) = 0%, P = .97).
Shoulder Joint ROM (in degrees)
Two studies21,26 reported changes in the ROM of the shoulder in anteflexion, protraction, abduction, adduction, intorsion, and extorsion (Table 4). We observed that AM could improve the ROM in the protraction (MD = 6.77, 95% CI = 2.81-10.73, P = .0008; heterogeneity (I2) = 0%, P = .65), and adduction (MD = 4.17, 95% CI = 1.02-7.32, P = .01; heterogeneity (I2) = 0%, P = .78) directions, but there was no significant difference in ROM for the other directions in the control group. In addition, both control groups were treated with oral diosmin tablets.
Comparison of Shoulder Joint ROM Between AM Group and Oral Diosmin Tablets Group.

Abbreviations: SD: standard deviation; P and I2: heterogeneity was appraised using the P value alongside the I2 statistic; MD: mean deviation; CI: confidence interval; FE: fixed-effect model; RE: random-effect model; Po: test for overall effect.
VAS
The results of 2 studies23,24 showed that acupuncture could significantly reduce the patients’ VAS for pain (MD = −1.33, 95% CI = −1.52 to −1.15, P < .00001; heterogeneity (I2) = 0%, P = .57). In addition, the intervention in the control group of both the studies included functional exercises, while the intervention in the experimental group involved acupuncture treatment based on functional exercises.
Three studies28-30 reported the VAS for swelling. Three studies on the effects of moxibustion versus pneumatic circulation showed a significant difference (MD = −0.51, 95% CI = −0.85 to −0.17, P = .003; heterogeneity (I2) = 0%, P = .96) (Figure 3).

Forest plots of VAS.
Bioimpedance and Quality of Life
Bioimpedance was mentioned as an outcome indicator in 2 studies.12,20 However, 1 study 20 reflected the change in bioimpedance, while another 12 showed the specific values before and after treatment; therefore, the results were not combined.
Although 5 studies21,26-28,30 showed that AM could significantly improve the quality of life, the assessment scales they used were not uniform. One study 28 used the scale developed by the European Organization for Research and Treatment, 1 study 21 used a Likert scale, 1 applied 30 the scale that is generally used for Chinese cancer patients, and the remaining 2 studies26,27 did not mention specific scales.
AE
Four studies12,20,25,28 have reported the AEs of AM in detail. The AE report showed that some participants had local symptoms; bruises (45 cases) were the most common, followed by discomfort (3 cases), hematoma (2 cases), pain (2 cases), burns (2 cases), severe swelling (1 case), cough (1 case), and skin infection (1 case).
Follow-up
Among the 4 studies12,20,28,29 that referred to the follow-up, the study by Smith et al. 20 explained that the 3 months follow-up data was not provided in the article as the staff did not have the resources to perform final measurements for the participants. Bao et al. 12 found that the size of the affected arm increased by nearly 10% compared with the unaffected arm, 3 months after treatment and not immediately after treatment. Wang et al. 29 and Shen 28 found that 1 month after the end of treatment, some patients’ limbs began to show varying degrees of swelling.
Discussion
Main Findings
Our results showed that AM reduced the circumference at the elbow crease more than other treatments, but no difference was found at other measurement points (wrist crease, 10 cm proximal to the wrist crease, and 10 cm proximal to the elbow crease). This finding is also supported by the results shown in the summary statistics in our study; LI.11, an acupoint located on the elbow crease, was selected for physical stimulation in most trials. This indicates that appropriate acupoint selection can have a better curative effect locally on the affected limb. Anatomically, the elbow joint, connecting the upper arm and forearm, is composed of the lower end of the humerus, the upper end of the ulna, and the upper end of the radius. In daily life, compared to most other joints, the elbow joint is always in a state of frequent and large arc movements. 31 Therefore, reducing the degree of edema at the elbow joint and allowing the elbow joint to recover is very important for patients with BCRL. In this respect, AM may have an advantage over routine care.
Regarding effective index for upper limb lymphedema and shoulder joint ROM, the results of the RCTs by Yao C and Liu Xiaofang were combined for analysis. Although only 2 studies could be analyzed, the same experimental group and control group minimized confounding factors, which gave the results a certain degree of credibility. In the case of oral diosmin, the tablets are first hydrolyzed into geraniol by the action of intestinal flora, which then enter the systemic circulation. However, AM is an invasive treatment that directly acts on the lesion, especially when the Ashi points (acupoints without a specific name or an exact location; the location is reflected by tenderness or other pathological reactions, also called tender points) are selected. This may explain, at least in part, why AM may improve the effective index for upper limb lymphedema and ROM of the shoulder joint more than diosmin tablets.
With regard to AM lowering the VAS pain scores in patients with BCRL, it is worth noting that previous studies32,33 have also shown that AM is effective in the treatment of chronic pain. In addition to clinical reports, Yu et al. 34 proposed that the cause of pain relief by acupuncture may be related to the increased connectivity between the precentral gyrus and middle frontal gyrus. However, in the present meta-analysis, this conclusion should be considered with caution. Because the experimental group (acupuncture and functional exercises) included in the study added acupuncture to the control group (functional exercises), we cannot completely rule out that the synergistic effect of the combined treatment exceeds the sum of the 2 separate treatments.
Unlike the VAS score for pain, the conclusion regarding the VAS score for swelling is definitive; moxibustion may lower patients’ VAS scores for swelling than pneumatic circulation. Pneumatic circulation is achieved with mechanical compression equipment or intermittent pneumatic compression equipment, which is used to apply pressure to the affected limb to improve blood and lymphatic circulation. Moxibustion, as a warm stimulation, can dilate blood vessels, increase blood flow, and improve microcirculation. In addition, moxibustion provides warm stimulation suitable for the human body, so that the patient has a pleasant emotional experience and a healthier psychological state. Therefore, considering that both interventions can improve circulation, moxibustion may be more effective than pneumatic circulation based on the VAS score for swelling obtained by the patient’s own subjective feelings.
This meta-analysis revealed that AM may cause discomfort, bruises, hematoma, pain, skin infection, burning, severe swelling, and coughing. However, AEs were mostly grade I or II, and no grade IV AEs were observed. After timely and effective treatment, no serious complications occurred. The participants were able to tolerate the treatment, and there were no treatment-related deaths. Finally, the 1 to 3 months follow-up survey of 3 RCTs indicated that lymphedema in some patients had recurred; therefore, there is no evidence to confirm that AM has a sustained effect on BCRL.
Strengths and Limitations
To our knowledge, this is the latest and most comprehensive meta-analysis summarizing the results regarding the effects and safety of AM for BCRL. This review conducted a meta-analysis based on different control methods to avoid clinical heterogeneity of samples that may affect the results of the study. In contrast to previous meta-analyses,9,10,35,36 strict filtering criteria were implemented for the studies included in this review. For the included RCTs, the intervention group had to be ordinary acupuncture and/or ordinary moxibustion, in order to eliminate the effects of other measures (such as electroacupuncture, laser, traditional Chinese medicine, massage, and cupping, among others) to the extent possible. Furthermore, to obtain more definitive conclusions, we discussed acupuncture and moxibustion separately.
This study has some limitations. First, most of the included articles were of poor quality. Several studies lacked details of allocation concealment, and none of the articles mentioned blinding to the outcome assessors. Second, the analysis was based on small sample sizes, so the results should be interpreted carefully. Third, we cannot fully exclude the effect of AM manipulation on the study outcomes. Finally, although we differentiated acupuncture and moxibustion, we did not further compare their efficacy or study the synergistic effects of acupuncture and moxibustion due to the small number of included studies.
Future Perspectives
The selection and combination of acupoints play an important role in the effectiveness of treatments. For BCRL, all trials focused on local acupoints on the upper limbs. These findings are consistent with those of previous studies. 36 However, the mechanism of specific acupoint stimulation and acupoint combination requires further study. Moreover, different studies measured the circumference of the affected limb at different positions as outcome indicators, which made it difficult to aggregate analyses. In future trials, it may be a better option to report the changes in the circumference of the upper limbs at 4 positions (wrist crease, 10 cm proximal to the wrist crease, elbow crease, and 10 cm proximal to the elbow crease) at the same time. Finally, since the efficacy of the different control groups is still uncertain, we suggest that in future studies, pneumatic circulation or routine care could be used for comparison in addition to waiting lists or sham acupuncture control.
Conclusion
Overall, our study results further clarify that AM has a certain efficacy in the treatment of BCRL. AM may reduce arm circumference at the elbow crease (compared to routine care), increase effective index for upper limb lymphedema (compared to oral diosmin tablets), improve shoulder joint ROM in the protraction and adduction directions (compared to oral diosmin tablets), reduce VAS for swelling (compared to pneumatic circulation), and decrease VAS for pain (compared to blank control). Although AM demonstrates more advantages than the other therapies, more compelling evidence is essential to confirm the benefits of AM.
Supplemental Material
sj-pdf-1-ict-10.1177_15347354211044107 – Supplemental material for Effects of Acupuncture and Moxibustion on Breast Cancer-Related Lymphedema: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Supplemental material, sj-pdf-1-ict-10.1177_15347354211044107 for Effects of Acupuncture and Moxibustion on Breast Cancer-Related Lymphedema: A Systematic Review and Meta-Analysis of Randomized Controlled Trials by Yu Gao, Tingting Ma, Mei Han, Mingwei Yu, Xiuhui Wang, Yiren Lv and Xiaomin Wang in Integrative Cancer Therapies
Footnotes
Acknowledgements
The authors would like to thank Ling Wang for excellent technical support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant (No. Z191100008319006) from Beijing Science and Technology Plan Project.
Supplemental Material
Supplemental material for this article is available online.