
Abstract
The objective of this study is to evaluate the effect of Tuina combined with moxibustion on relieving breast cancer–related lymphedema (BCRL). A randomized cross-over controlled trial was conducted at our institution. All patients with BCRL were assigned to 2 groups: Group A and Group B. In the first period (weeks 1-4), tuina and moxibustion were performed in Group A and pneumatic circulation and compression garment in Group B. The washout period took place from weeks 5 to 6. In the second period (weeks 7-10), pneumatic circulation and compression garment were performed in Group A, and tuina and moxibustion in Group B. Therapeutic efficacy was evaluated by measuring the affected arm volume, circumference, and Visual Analog Scale for swelling. Regarding the results, a total of 40 patients were included, and 5 cases were dropped. After treatment, both the traditional Chinses medicine (TCM) treatment and complete decongestive therapy (CDT) was found to reduce the volume of the affected arm (P < .05). At the endpoint (visit 3), compared with CDT, the effect of the TCM treatment was more evident than that of CDT (P < .05). After the TCM treatment, the arm circumference at the elbow crease and proximal 10 cm to elbow crease was reduced, which was statistically different from that before treatment (P < .05). Post-CDT treatment, the arm circumference at proximal 10 cm to wrist crease and the elbow crease and proximal 10 cm to elbow crease decreased, which was statistically different from that before treatment (P < .05). At the endpoint (visit 3), the arm circumference at proximal 10 cm to elbow crease of the patients treated with TCM was less than that of CDT (P < .05). Moreover, the VAS scores for swelling were better after compared with before TCM treatment and CDT (P < .05). At the endpoint (visit 3), the subjective relief of swelling by TCM treatment was greater than CDT (P < .05). Ultimately, tuina combined with moxibustion can alleviate BCRL symptoms, which is primarily reflected in reducing the affected arm volume and circumference and relieving swelling.
Trial registration: Chinese Clinical Trial Registry (Registration Number ChiCTR1800016498).
Keywords
Introduction
Breast cancer has been one of the most common malignant tumors threatening women’s health, and its incidence rate has ranked first among female malignancies. 1 With the continuous progress in the treatment methods, the survival rate of patients has improved. Meanwhile, how to improve the quality of life of patients after treatment has garnered increasing attention. Breast cancer-related lymphedema (BCRL) is often referred to as “the most terrible complication in the treatment of breast cancer.” 2 It not only severely affects the patients’ quality of life but also leads to adverse psychological states, such as depression and anxiety, 3 causing a heavy burden to them and their families.
With reference to the patient statement in the recommendations of the Clinical Practice Guidelines and the International Society of Lymphology (ISL) standards, the BCRL grades and stages are as follows (Table 1):
Lymphedema Staging Model.

Surgery and radiotherapy injure axillary lymph nodes, hindering the lymphatic reflux and causing abnormal swelling of the affected upper limb.6,7 With the development of BCRL, serious skin fibrosis and fat deposition can occur, resulting in the loss of limb function. 8 According to the data, the overall estimated incidence rate of BCRL in breast cancer patients is 21.4%, which shows that it is a common problem. 9 Therefore, improvements in the prevention and treatment are crucial for BCRL patients. Currently, there is no drug to alleviate lymphedema and no gold standard for the treatment of BCRL.10,11
The first-line non-invasive treatment of BCRL mainly includes 2 different stages: the recovery treatment and the maintenance treatment. Recovery treatment, also known as complete decongestive therapy (CDT), aims to reduce the symptoms of upper limb swelling. It usually includes manual lymphatic drainage (MLD), compression bandage, intermittent pneumatic compression, exercise, skin care, and patient education. According to the individual conditions of patients, CDT can be combined with various treatment methods. 12 Maintenance treatment is predominantly carried out after the volume of the affected upper limb is minimized through CDT, mainly including self-administered MLD, compression garment, exercise, and skin care.
Studies have demonstrated that recovery treatment and maintenance treatment may help relieve lymphedema and improve the quality of life of patients with BCRL. However, given the need for patients to receive frequent treatments, the maintenance of curative effects largely depends on patient compliance. While studies on the non-invasive treatment for BCRL have focused on CDT in its entirety, there has been limited research on the efficacy of each individual CDT component.12-14 Surgery may be effective for some patients with refractory BCRL, but it only serves as an alternative to standard treatment because of insufficient evidence. 15
According to traditional Chinese medicine theory, surgery and radiotherapy damage the patient’s meridians, resulting in qi obstruction, the inability to promote blood circulation and blood stasis. Eventually, it leads to the internal stagnation of water and blood stasis, blocking the upper limb meridians and causing edema. Tuina and moxibustion are regularly used in traditional Chinese medicine and are widely employed in the treatment of various diseases. Moxibustion can increase the peripheral blood flow and microvascular permeability at the treatment point, which helps regulate the immune and neurological functions of the human body.16,17 Tuina acts on the acupoints, muscles, and connective tissues and triggers reflexes, which then regulate the body’s function and achieve the therapeutic effect. 18 Combined with our previous clinical research observation, moxibustion can reduce the affected arm circumference and alleviate the swelling. 19 Therefore, we designed this study and combined moxibustion and tuina to evaluate their efficacy on BCRL and explore the feasibility of traditional Chinese medicine in the treatment of BCRL.
Materials and Methodology
Ethical Approval and Informed Consent
The ethics committee of The Third Affiliated Hospital of Beijing University of Chinese Medicine approved the study protocol (Certificate No. BZYSY-XJKTPJ-245). Prior to their enrollment, all patients provided their signed written informed consent.
Patients
Forty patients responded to the recruitment notices on the WeChat APP and posters in nearby public places. Concerning the inclusion criteria for this study, patients must
(a) be female;
(b) be 25 to 75 years old;
(c) have a pathological diagnosis of breast cancer;
(d) have a history of surgery with completed chemotherapy, radiotherapy, or both;
(e) have unilateral upper limb lymphedema;
(f) have an affected arm with a circumference ≥2 cm greater than that of the contralateral arm at baseline, or the volume of the affected arm ≥120 ml greater than that of the contralateral arm at baseline;
(g) sign an informed consent.
The exclusion criteria included
(a) the presence of metastases;
(b) lactation;
(c) pregnancy;
(d) serious primary diseases (heart, liver, kidney, or hematopoietic system diseases; thrombotic disease, phlebitis, or other vascular system diseases; and lymphangitis or other lymphatic diseases);
(e) the presence of limb skin trauma, ulceration, or skin disease;
(f) history of allergies;
(g) history of chronic respiratory diseases; and
(h) receiving other treatments for lymphedema.
This study was conducted at our institution from October 2018 to August 2019.
Treatment
All patients were assigned to 2 groups: Group A and Group B. In the first period (weeks 1-4), tuina and moxibustion were performed in the former, and pneumatic circulation and compression garment in the latter. The washout period took place from weeks 5 to 6. In the second period (weeks 7-10), pneumatic circulation and compression garment were both performed in Group A and tuina and moxibustion in Group B.
During the Traditional Chinese Medicine treatment, patients first received tuina for 20 minutes and then moxibustion for 20 minutes, twice every week. In the process of CDT, patients underwent pneumatic circulation for 30 minutes (twice weekly) and wore a compression garment for 8 hours daily. The patients were treated 16 times. No treatment intervention was carried out for patients in the washout period. Well-trained doctors conducted all the treatments and measurements.
Tuina and Moxibustion
In the special treatment room, the patient took off the coat and fully exposed her chest, back, and affected limbs.
Tuina
1. The patient was placed in the supine position.
a. Gently knead RN17 clockwise 10 times.
b. According to the sequence of SI, TE, and LI, the kneading manipulation is used for the continuous and gentle movement along the meridians from the wrist to the shoulder, and the whole operation is repeated 3 times.
c. According to the sequence of SI, TE, LI, LU, PC, and HT, use the grasping and rolling manipulation to stimulate along each meridian in turn. The direction of the stimulation is from the wrist to the shoulder. Gently press the SI 9, TE 5, LI 11, LU 5, PC 6, and HT11 for 3 to 5 seconds every time. Repeat the entire operation 3 times (Figure 1).
2. The patient was placed in the prone position.
a. Gently press DU 14, GB 21, SJ 5, SI 11, BL 13 (bilateral), BL 20 (bilateral), and BL 23 (bilateral) for 5 seconds.
b. Use pushing manipulation from BL 13 to BL 23 along bilateral BL. Repeat the operation 3 times (Figure 2).

Diagram of the chest and affected arm Tuina in the supine position.

Diagram of the back Tuina in the prone position.
Moxibustion
1. Moxa sticks (1.8 × 20 cm; Nanyang Hanyi Moxa Co Ltd., Nanyang, China) were cut into 5 cm segments, lit, and placed in a moxibustion box (Hanyi, 23 × 16 × 9.2 cm; Nanyang Hanyi Moxa Co).
2. The patient was placed in the prone position. The appropriate treatment points on the affected arm were selected from the following: LI 14, LU 5, LI 11, SJ 5, BL 23 (bilateral), and Ashi points. Next, the moxibustion box was then placed on the selected points for 20 minutes. The moxibustion box was removed after finishing.
During moxibustion, the patient felt warm without burning, and the local skin was red. If the patient felt burning pain, the moxibustion could be continued after lifting the moxa box for 10 to 30s.
Pneumatic Circulation
Pneumatic circulation (LGT-2200w Guangzhou Longest Science & Technology Co Ltd., Guangzhou, China)
The patient was placed in a sitting position, and the affected arm was fully exposed with the arm and heart on the same level.
The patient’s arm and shoulder were wrapped in a pneumatic circulation sleeve, and the pneumatic circulation was turned on. The pressure mode was set to step inflation and pressurization from the distal to the proximal, and the initial pressure was set to 25 mmHg. The initial pressure was gradually pressurized according to the tolerance of the affected limb during treatment, up to 60 mmHg.
After 30 minutes, the sleeve was removed, and the pneumatic circulation was turned off.
Compression Garment
Patients receiving pneumatic circulation wore a compression garment on the affected arm for 8 hours daily, and they took their compression garment off before going to bed. The patients provided their own compression garments.
Assessment of Outcomes
The primary outcome of the affected arm volume was measured with a measuring cylinder (Beijing Yangzihuamei Plexiglass factory, Beijing, China) and the affected arm circumference with a tape (wrist crease, 10 cm proximal to wrist crease, elbow crease, and 10 cm proximal to elbow crease). The key result of swelling was quantified by the Visual Analog Scale (VAS) scores. All indicators were recorded and measured at weeks 0, 2, 4, 6, 8, and 10. Each treatment period was visited 3 times.
Determination of the Required Study Size
This study adopted the standard calculation formula of a randomized cross-over controlled trial: n = (uα+uβ)2σ/δ. α = .05, β = .1. The pre-test showed that the arm circumference at 10 cm proximal to elbow crease of the pneumatic circulation group was 30.50 ± 3.95 cm, and tuina combined with moxibustion group was 29.86 ± 4.31 cm (δ = 30.50 − 29.86 = 0.64, σ = 1.18, uα = 1.282, uβ = 1.960). According to the formula, the total sample size was about 35, and the loss of follow-up rate increased by 15%. Then, the sample size was 40, with an average distribution of 20 cases in each group.
Randomization
Forty random function sequences were established using the IBM SPSS 21.0 software (IBM Corp, Armonk, NY). The generated random numbers were sealed in sequentially numbered opaque envelopes with each participant’s screening sequence number printed on the outside and the allocated group names inside the envelope. Subsequently, a statistician opened the envelope corresponding to the participant’s screening sequence number and assigned them to either Group A or B accordingly. The participants were randomly assigned to the study groups in a ratio of 1:1. It was impossible to blind the patients or treating physicians because of the nature of each treatment. However, both the researcher who evaluated the outcomes and the statistician were blinded to the group assignments and were not involved in the treatment.
Follow-up
There was no follow-up in this study.
Statistical Analysis
Considering the randomized cross-over controlled trial of this study, the baseline, “residual effect,” and “sequential effect” of the data should be tested first. If there is a “residual effect,” the data on the second period should be discarded and the independent sample t-test or rank-sum test should be carried out for the first period.
If there is no “residual effect,” continue to test the “sequential effect.” Finding no difference in the test results indicates that the setting of this research scheme is reasonable. If there is a difference in the results, use the opposite number to correct the influence of the “sequential effect” before.
Statistical Analysis
All values were expressed as mean ± standard deviation. Significant differences between the groups were statistically analyzed using the independent t-test or nonparametric test. Significant differences pre- and post-treatment in the same group were analyzed by the paired-samples t-test or nonparametric test. Discrete data were compared using the χ2 test or an accurate probability method. Then, the IBM SPSS 20.0 software was utilized for statistical analysis. The statistical significance was established at the value of P < .05.
Results
Patient Characteristics and Baseline Measurements
The first patient was enrolled in October 2018, and the last patient left the group in August 2019. A total of 40 patients were included, and 5 patients dropped out in the first period, 3 from Group A and 2 from Group B (Figure 3). In the group A, 2 patients quit the research mainly due to intolerance to the odor of moxibustion, and 1 because of infection with pneumonia. In the group B, 2 patients were lost mainly for loss to follow-up.

Flow chart of patient allocation.
Patient Characteristics and Baseline Measurements
No significant differences were found between the 2 groups, specifically in age, height, weight, BMI, surgical procedure, pathological type, tumor stage, radiotherapy, edema duration, or other assessed variables. There were also no significant differences between the groups in terms of the affected arm circumference, affected arm volume, or VAS swelling (Table 2).
Demographic Characteristics and Baseline Measurements.

Residual Effect Test and Sequential Effect Test
Residual effect test
After the “residual effect” test, the results underlined that no significant difference was present in the affected arm volume, circumference, and vas swelling score (P > .05), indicating that the treatment measures in the first period did not affect the second period (Table 3).
Residual Effect Test.

Sequential effect test
The results indicated that there was no significant difference in affected arm volume, circumference, and VAS swelling score (P > .05), indicating that there was no sequential difference in the treatment measures of this study. Combined with the “residual effect” test, it confirms the plausibility of the elution period and treatment measures of this scheme (Table 4).
Sequential Effect Test.

Comparison of Arm volume on Affected Side
After treatment, both the TCM treatment (tuina combined with moxibustion) and the CDT (pneumatic circulation and compression garment) can reduce the volume of the affected arm (P < .05). At the endpoint (visit 3), compared with CDT, the effect of the TCM treatment was more perceptible, and the treatment difference of TCM was significantly greater than that of CDT (P < .05) (Table 5). Figure 4 presents the changes in the trend of the affected arm volume in different periods.
Comparison of Affected Arm Volume (cm3).

Visit 1: baseline (week 0 and week 6); Visit 2:week 2 and week 8; Visit 3: endpoint (week 4 and week 10); Treatment difference: endpoint—baseline; TCM: tuina combined with moxibustion; CDT: pneumatic circulation and compression garment. The TCM group in Visit 1 includes Group A patients at week 0 and group B patients at week 6, while the CDT group includes Group B patients at week 0 and Group A patients at week 6. The TCM group in Visit 2 includes Group A patients at week 2 and Group B patients at week 8, while the CDT group includes Group B patients at week 2 and Group A patients at week 8. The TCM group in Visit 3 includes Group A patients at week 4 and Group B patients at week 10, while the CDT group includes Group B patients at week 4 and Group A patients at week 10.

The trend of affected arm volume changes.
Comparison of Arm Circumference on the Affected Side
Post-TCM treatment, the arm circumference at the elbow crease and proximal 10 cm to the elbow crease was reduced. It was statistically different from the pre-treatment (P < .05). Post-CDT treatment, the arm circumference at proximal 10 cm to the wrist crease, elbow crease and proximal 10 cm to elbow crease decreased, which was statistically different from the pre-treatment (P < .05). At the endpoint (visit 3), the arm circumference at proximal 10 cm to elbow crease of the patients treated with TCM was less than that of the CDT (P < .05). However, there was no significant difference in the effect of reducing the arm circumference between TCM and CDT (P > .05) (Table 6). Figure 5 illustrates the trend of the affected arm circumference changes across the different periods.
Comparison of Affected Arm Circumference (cm).

Visit 1: baseline (week 0 and week 6); Visit 2: week 2 and week 8; Visit 3: endpoint (week 4 and week 10);Treatment difference: endpoint—baseline; TCM: tuina combined with moxibustion; CDT: pneumatic circulation and compression garment. The TCM group in Visit 1 includes Group A patients at week 0 and group B patients at week 6, while the CDT group includes Group B patients at week 0 and Group A patients at week 6. The TCM group in Visit 2 includes Group A patients at week 2 and Group B patients at week 8, while the CDT group includes Group B patients at week 2 and Group A patients at week 8. The TCM group in Visit 3 includes Group A patients at week 4 and Group B patients at week 10, while the CDT group includes Group B patients at week 4 and Group A patients at week 10.
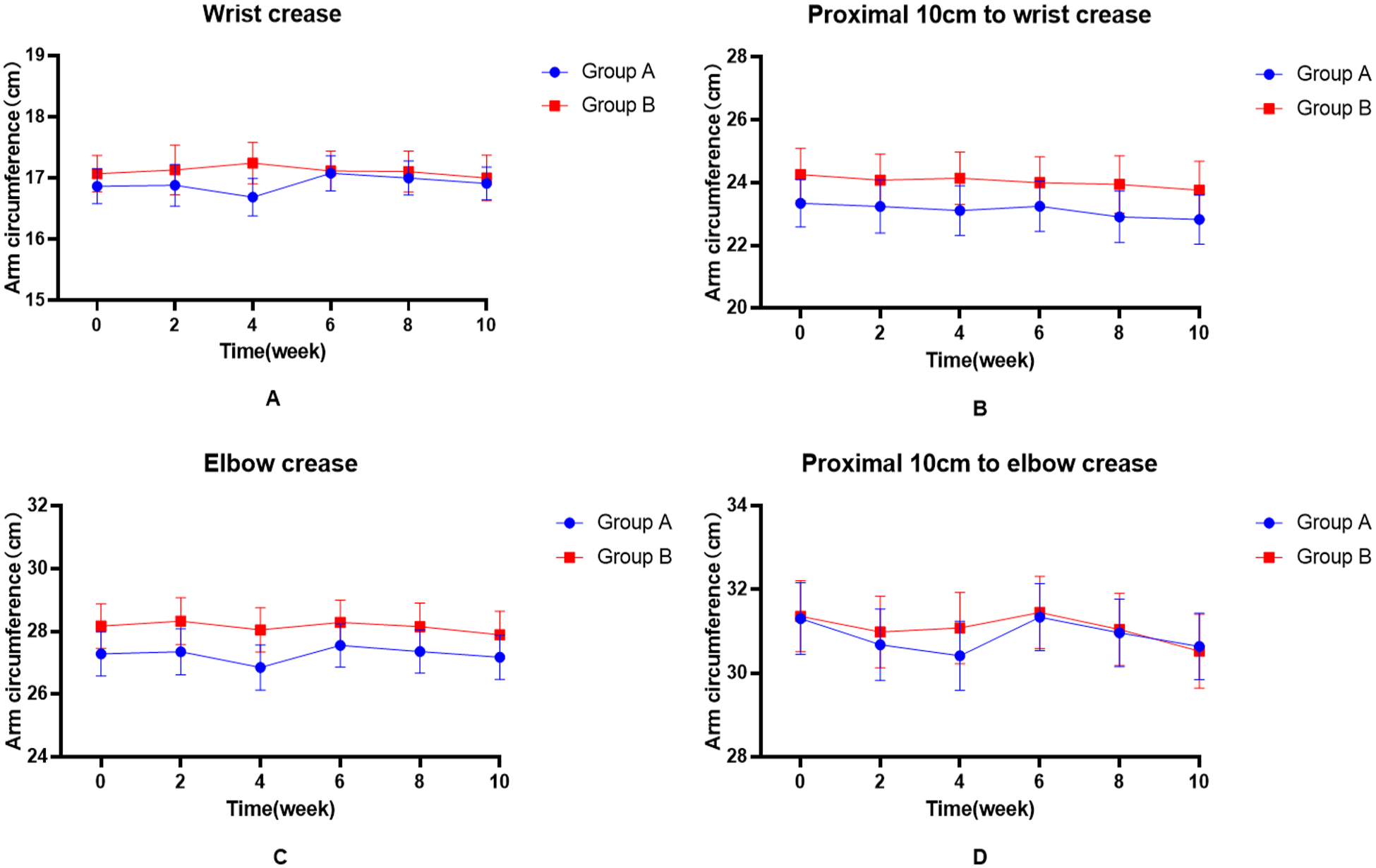
The trend of the affected arm circumference changes at different points.
Comparison of VAS Swelling Score
The VAS scores for swelling were better post- than pre-TCM treatment and CDT (P < .05). At the endpoint (visit 3), the subjective relief of swelling due to the TCM treatment was greater than CDT (P < .05) (Table 7). Figure 6 presents the trend of VAS scores for swelling changes across the different periods.
Comparison of VAS Swelling Scores.
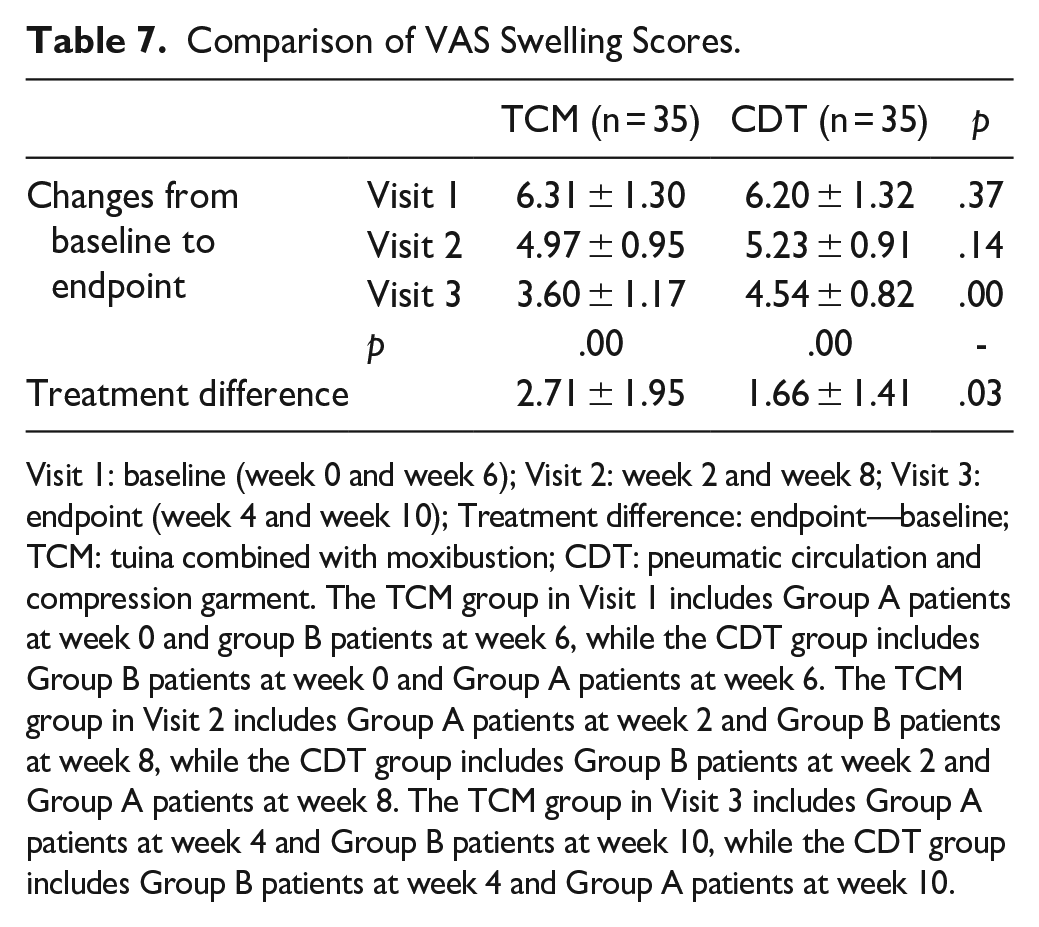
Visit 1: baseline (week 0 and week 6); Visit 2: week 2 and week 8; Visit 3: endpoint (week 4 and week 10); Treatment difference: endpoint—baseline; TCM: tuina combined with moxibustion; CDT: pneumatic circulation and compression garment. The TCM group in Visit 1 includes Group A patients at week 0 and group B patients at week 6, while the CDT group includes Group B patients at week 0 and Group A patients at week 6. The TCM group in Visit 2 includes Group A patients at week 2 and Group B patients at week 8, while the CDT group includes Group B patients at week 2 and Group A patients at week 8. The TCM group in Visit 3 includes Group A patients at week 4 and Group B patients at week 10, while the CDT group includes Group B patients at week 4 and Group A patients at week 10.

The trend of the changes in the VAS Swelling Scores.
Safety Assessment
No adverse events occurred during the treatment.
Discussion
Pneumatic circulation is frequently used in the treatment of BCRL, which is an effective addition to CDT or an alternative to MLD and compression bandaging when combined with self-lymphatic drainage.20,21 More specifically, compression bandaging or compression garment as a common intervention for subclinical BCRL has been increasingly used to prevent swelling progression. 22 Therefore, we selected the pneumatic circulation and compression garment as the control to evaluate the curative effect of traditional Chinese medicine.
Tuina is a medical method to prevent and treat diseases by various manipulations and specific limb activities on certain parts or acupoints of the human body using principles of TCM and meridian. Although tuina and MLD are performed by hand, their manipulation, strength, and operation direction differ. The primary purpose of MLD is to guide the lymph to avoid the blocking area, flow into a healthy lymphatic vessel closer to the center, and enter the venous system, 12 and the manipulations of MLD are gentle. Therefore, combined with the concept of MLD, we improved the tuina manipulation to make it more suitable for BCRL treatment and used it in this study. First, we stipulate that tuina should operate from the distal to the proximal direction, taking place in one direction, to make it conform to the direction of lymphatic reflux in the upper limbs. According to the TCM meridian theory, the circulation direction of the 3 yin meridians of the hand is “walking from the chest to the hand,” and the circulation direction of the 3 yang meridians of the hand “walks from the hand to the head.” The operation direction, from the distal to the proximal, follows the circulation of the 3 yang meridians of the hand, which is opposite to the circulation of the 3 yin meridians of the hand. Along with the TCM theory of reinforcing and reducing diarrhea, tuina in this direction functions to warm yang and activate blood circulation, purging yin and detumescence.
Second, we delved into the strength of tuina. Gentle manipulations were selected, only acting on the skin and various liquid and lymphatic structures of subcutaneous superficial tissues, to avoid stimulating the deep muscle tissue. We have always believed that more attention should be paid to the patients’ subjective swelling during BCRL prevention and treatment. Beyond the subjective swelling, the BCRL concealment characteristics also affect the patient’s psychological state and daily life. 23 Moreover, since the subjective swelling may appear before limb swelling, focusing on the subjective swelling may aid in diagnosing BCRL. A survey showed that nearly 80% of the patients undergoing breast cancer surgery know nothing about BCRL, and the physicians’ understanding of it also varies. 24 In addition, BCRL has concealment-related characteristics. Subjective swelling may appear before limb swelling. Diagnosis only depends on the changes in objective indicators like arm circumference and volume of the upper limb, making misdiagnosis easily take place. The results demonstrate the evident advantages of tuina’s combination with moxibustion, particularly in alleviating the subjective swelling. This may be associated with the local stimulation of moxibustion and tuina affecting the upper limb blood circulation and lymphatic circulation, but the specific mechanism still necessitates further analysis.
Furthermore, we found that whether TCM treatment or CDT is being selected, the effect on arm circumference reduction is more apparent from the elbow to the shoulder joint, which is consistent with the findings of a systematic review of acupuncture and moxibustion for BCRL. 25 Anatomically, the elbow and shoulder joints are in a state of frequent and large arc movement, and the local edema may be more severe. Therefore, once treated, it will easily reflect the curative effect. Simultaneously, the limb above the elbow is closer to the axillary lymph tissue than the wrist area, the interstitial fluid pressure of the limb is relatively low, and the lymph is easier to return, so the treatment effect is discernible. Therefore, in the future, we should also adjust the treatment according to the edema of different parts of the patients, so as to further benefit them. Although tuina with moxibustion alleviated BCRL, all observation indexes returned to the baseline level after the washout period, indicating that the treatment effect was maintained for no more than 2 weeks. Ultimately, understanding how to maintain the long-term effect of the treatment on BCRL is worthy of additional research.
This study still has some limitations, including no long-term follow-up, too small sample size, and no MLD in the control group. The reason is that the main purpose of this study is to evaluate the effectiveness of massage combined with moxibustion in the treatment of BCRL, so the maintenance effect of the treatment method is not taken as an observation index. However, due to the randomized cross control trial adopted in this study, we can roughly evaluate that the effect maintenance period of this therapy is 2 weeks through the setting of the washout period and the results of the preliminary trial, but it still needs to be further and accurately evaluated by the follow-up rigorous experimental design. It has been revised in this paper and discussed as the limitation of the study. Nevertheless, it is believed through the present study that adding some traditional Chinese medicine therapies such as moxibustion and massage to CDT, and then cooperating with MLD and pressure therapy may become a new idea for BCRL treatment.
Conclusion
Tuina combined with moxibustion can alleviate BCRL symptoms, which is mainly reflected in reducing the affected arm volume and circumference and relieving swelling.
Footnotes
Acknowledgements
We extend our thanks to the Galactophore Department of the 3rd Affiliated Hospital of Beijing University of Chinese Medicine.
Authors’ Note
This trial was registered in the Chinese Clinical Trial Registry (Registration Number ChiCTR1800016498).
Author Contributions
Chunhui Wang and Heng Liu wrote the manuscript. Xiaohua Pei and Yingyi Fan conceived and designed the study. Jing Shen and Le Zhao contributed to the collation and treatment of patients. Heng Liu and Yanfang Hao contributed to the collation and analysis of the data. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Capital’s Funds for Health Improvement and Research (No. CFH-2018-3-7031).