
Abstract
Background
Complementary and alternative medicine (CAM) is becoming more common in medical practice, but little is known about the concurrent use of CAM and conventional treatment. Therefore, the aim was to investigate the types of CAM used and their prevalence in a regional patient cohort with breast cancer (BC).
Methods
BC patients were interviewed with a structured questionnaire survey on the use of CAM in southern Taiwan at an Integrative Breast Cancer Center (IBCC). The National Centre for Complementary and Integrative Health (NCCIH) classification was used to group responses. Over a period of 8 months, all patients receiving treatment for cancer at the IBCC were approached.
Results
A total of 106 BC patients completed the survey (response rate: 79.7%). The prevalence of CAM use was 82.4%. Patients who were employed, were receiving radiotherapy and hormone therapy, and had cancer for a longer duration were more likely to use CAM (P < .05). Multivariate analysis identified employment as an independent predictor of CAM use (OR = 6.92; 95% CI = 1.33-36.15). Dietary supplementation (n = 69, 82.1%) was the type of CAM most frequently used, followed by exercise (n = 48, 57.1%) and traditional Chinese medicine (n = 29, 34.5%). The main reason for using CAM was to ameliorate the side effects of conventional therapies. Almost half (46.4%) of these CAM users did not disclose that they were using it in medical consultations with their physicians. Most chose to use CAM due to recommendations from family and friends.
Conclusion
A large portion of BC patients at the IBCC undergoing anti-cancer treatment courses used CAM, but less than half discussed it with their physicians. Given the high prevalence of CAM, it would be justifiable to direct further resources toward this service so that cancer patients can benefit from a holistic approach to their treatment.
Keywords
Introduction
Complementary and Alternative Medicine (CAM) is a wide-ranging, non-mainstream branch of medicine. It employs natural products, mind–body therapies, and entire health care systems. 1 In recent decades, its use by cancer patients has grown, especially that by breast cancer (BC) patients.2,3 The use of CAM among BC patients is widespread worldwide, ranging from 21% to 98% of BC patients, and the pattern of use differs according to socioeconomic status, geography, culture, spiritual beliefs, and therapeutic availability.2,4,5
BC patients who use CAM often do so to reduce the side effects of treatment and to improve both their health and quality of life. 4 Patients with cancer in different countries use different types of CAM. The majority of Chinese patients who have cancer, for example, use Traditional Chinese Medicine (TCM), 6 whereas those in the United States and Europe usually prefer homeopathy and naturopathy.7,8
Patients in Taiwan, which is home to a modern Chinese society with a two-tiered medical system, use both Western medicine and TCM. The 2 systems operate together, and the costs of both types of treatment have in general been covered by the National Health Insurance (NHI) program since 1995. 9 TCM is based on the concepts of Yin-Yang, Meridians, and the Five Elements. This system involves Chinese herbal medicine (CHM), acupuncture, moxibustion, and traumatology manipulative therapy.10,11 The NHI sets clear boundaries distinguishing TCM from CAMs such as folk remedies, nutrients or spiritual healing. 11
Few studies have assessed the different types of CAM used in Taiwan because non-covered CAM is generally seen as insufficiently legitimate for policy research. 12 To our knowledge, only 1 report from another research group has found that 55.7% of BC patients in Taiwan use some form of CAM, with TCM usage being as high as 35.6% and BC survivors being amongst the highest users. 13 More knowledge is needed, however, regarding which specific CAM modalities patients are most likely to seek out during the courses of their anti-cancer therapies. The objective of this cross-sectional study was to describe the prevalence and types of CAM that patients with BC use while concurrently receiving conventional treatment in Taiwan.
Methods
Study Design and Subjects
A cross-sectional descriptive survey design was used to collect data with a questionnaire on CAM therapies for patients with breast cancer. A single hospital with an Integrative Breast Cancer Center (IBCC) in Kaohsiung Chang Gung Memorial Hospital (KCGMH) was the site of this study. Two assistants from the IBCC were selected based on interest in and/or experience with CAM. All data collected were returned to 1 investigator and coded for analysis. This study was approved by the ethics committees of the KCGMH (Reference Number: 20180158-7B0C501) and carried out between January 2020 and August 2020. Cancer patients on the Cancer Virtual Private Network (VPN) Registry were recruited from January 2017 to June 2019. The sample size for CAM use in the study was calculated with the subject-to-item ratio. A minimum of 65 participants were needed (13 items × 5 = 65), based on Gorsuch’s formula, to achieve a subject-to-item ratio of 5:1. 14 To compensate for the expected 20% attrition rate, the sample size was increased to 78 participants. All participants received clear explanations of the study.
Inclusion/Exclusion Criteria
Patients were eligible if they met the following inclusion criteria: speaker of Mandarin or Taiwanese; adult female with a diagnosis of breast cancer; awareness of the diagnosis; current treatment with anticancer therapy; ability to read and understand all questions; absence of any conditions that would make completing the questionnaire inappropriate or burdensome; and willingness to participate in the study. Patients whose medical histories listed mental disorders, acute illness or death were excluded. CAM users were defined as those reporting the use of at least 1 type of CAM (nutritional supplements included) more than 3 times since receiving a diagnosis of breast cancer. 15
Data Collection
Investigators were provided a list of patients receiving surgery or adjuvant therapy for breast cancer. The clinical profiles, treatment modalities, and pathological tumor characteristics of the patients were collected from the cancer registry of the IBCC. Eligible patients were invited to participate in the study, and for those who agreed to be interviewed, appointments were arranged by telephone. Face-to-face interviews lasting 20 minutes were conducted in quiet spaces at clinics. Eligible participants provided written consent before participating in this study. Data were collected and stored on a computer, and access was restricted to the researcher, a statistician, and a research assistant.
This study used the 5 categories of CAM delineated by the National Centre for Complementary and Integrative Health (NCCIH), 1 and some others were modified from Chang et al. to reflect Taiwanese culture: 16 alternative medical systems (TCM, cupping, and homeopathy), mind–body medicine (spiritual/prayer, yoga, Tai Chi, psychotherapy, and aromatherapy), biologically-based practices (dietary supplements, herbal remedies or folk medicine, and organic diet), manipulative and body-based practices (reflexology, exercise, and massage), and energy medicine (Qigong, light therapy, and electromagnets). Among all the alternative medical systems, we considered only TCM because of its widespread use in Taiwan, where people rarely use homeopathic, naturopathic, or Ayurvedic medicine. 17 Since the NHI system covers the costs of TCM, only licensed TCM doctors can prescribe or apply TCM for treatments. Patients who bought herbal medicines from non-NHI-contracted providers without first acquiring a prescription from a licensed doctor were categorized as users of therapies that were biologically based.
Questionnaire
The questionnaire ultimately contained 2 parts with 28 items in total. The first part collected information on demographic characteristics (age, religion, marital status, working status, education level, and monthly income) and clinical data (cancer stage, disease duration, current standard treatment including chemotherapy, radiotherapy, hormonal therapy use, and targeted therapy; and history of surgery, menopausal status, and comorbidities). The second part, which was based on a questionnaire previously developed by Erku, collected information on CAM use. 18 Patients reporting CAM use were asked to provide additional information, such as the type, reasons or motivations for CAM use, consultations with doctors, side effects,19,20 and perceived effects of CAM use. However, the questionnaire was modified for the purposes of the present study and some new items were added (eg, personal spending on CAM and number of CAMs used). The questionnaire was translated from English to Chinese by a professional translator. Experts (1 epidemiologist, 3 TCM doctors, and 2 nurses) approved the modified version in terms of content and face validity. The literature recommended a Content Validity Index (CVI) value of 0.95. An additional file presents the questionnaire in detail (Supplemental Additional file 1).
Data Analysis
Data were analyzed in SPSS Statistics (IBM Co., Armonk, NY, USA) version 22.0. Descriptive statistics (frequencies and percentages) were employed to analyze the sociodemographic information and patterns of CAM use in the breast cancer patients. Univariate analysis was performed with the Chi-square test or Fisher’s exact test for categorical variables and the t test for continuous variables. Multiple logistic regression analysis was used to identify the independent factors associated with CAM use. P values ≤.5 in the univariate analysis were selected for further multiple analyses. The factors included in the analysis were age, education level (primary and higher education), work status (employed or unemployed), cancer stage (early, locally advanced, or metastatic), histologic type (ductal, lobular, or unknown), chemotherapy (yes or no), radiotherapy (yes or no), target therapy (yes or no), HRT used (yes or no), and duration of breast cancer (<1 year, 1-5 years, or > 5 years). P values <.05 were considered statistically significant.
Results
Characteristics of the Participants
A total of 128 eligible patients were invited to participate, and 26 patients refused. Therefore, 79.7% of the eligible patients completed the interview (Figure 1). Of the 102 patients surveyed, 84 (82.4%) reported that they had used CAM after receiving a diagnosis of BC.

Flow chart of CAM use among patients with breast cancer.
The mean age was 51.6 years. Most participants (74.5%) were married, and 77.5% were postmenopausal. Only 25% had completed a university education. Sixty-one participants (59.8%) were working and 9.8% had a monthly household income of more than NT$ 70,000/month. Almost all (97.1%) had received surgery for breast cancer. Approximately 77.5% were hormone sensitive, 13.7% were HER-2 enriched, 11.8% were triple negative, and 75.5% were stages I to II. Almost two-thirds of the participants (64.7%) had 1 or more comorbidities, such as hypertension, hypercholesterolemia, or diabetes. About three-quarters (75.5%) had completed or were receiving adjuvant chemotherapy at enrollment, while 50% were currently receiving hormone therapy. More details of the demographic data for this patient cohort are shown in Table 1.
Sociodemographic Characteristics of CAM Users and Non-CAM Users.

Abbreviations: CAM, complementary and Alternative medicine; SD, Standard deviation; NTD, New Taiwan dollar; HER, Human Epidermal Growth Factor Receptor.
Significantly different at P < .05.
Pattern of CAM Use
There were significant differences in the proportions of CAM and non-CAM users in work status, duration of cancer, radiotherapy and HRT (Table 2). For work status and duration of cancer, the differences were significant (P < .05). CAM use was also significantly higher in participants who had received radiotherapy (P = .01) and those who were employed (P = .04).
Association Between CAM Use and Sociodemographic Characteristics.

Abbreviation: SD, Standard deviation.
Multivariable logistic regression was done. Odd ratios were adjusted for age, education level, work status, cancer stage, histologic type, chemotherapy, radiotherapy, hormone therapy, and duration of cancer, with P ≤ . 5.
Statistically significant.
The sociodemographic and medical factors related to CAM use in BC patients are listed in Table 1. The univariate logistic regression indicated that working women (odds ratio [OR] = 3.79; 95% CI = 1.29-11.15), patients receiving radiotherapy (OR = 4.55; 95% CI = 1.23-16.87), and those receiving hormone therapy (OR = 3.15; 95% CI = 1.03-9.62) were more likely to be users of CAM. A disease duration of 1 to 5 years was also found to be associated with a greater likelihood of CAM usage. After adjustments for potential confounding factors (age, education level, work status, cancer stage, histologic type, chemotherapy, radiotherapy, hormone therapy, and duration of cancer), the results indicated that employed women were more likely to use CAM than were their unemployed counterparts (OR = 6.92; 95% CI = 1.33-36.15).
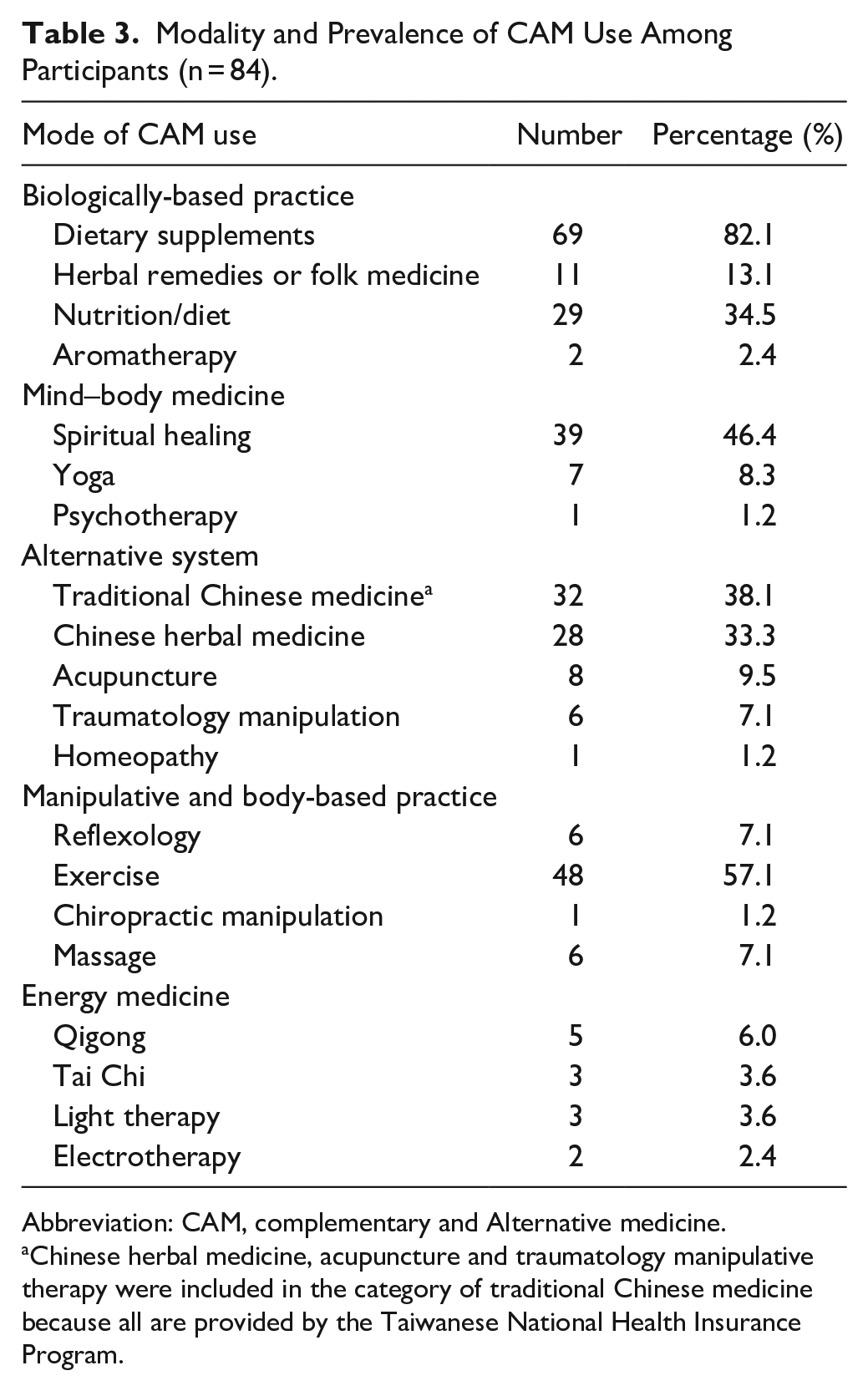
Table 3 presents the prevalence of use of the 5 CAM modalities. Dietary supplements (82.1%) were the most commonly used modality, followed by exercise (57.1%) and spiritual healing or prayer. About one third of the participants reported the use of TCM, the most dominant type of which was CHM (76.8%). Acupuncture and traumatology manipulation use were rare (0.4%). The most commonly used supplements, as shown in Figure 2, were high protein milk (59.4%), followed by vitamins and minerals (33.3%), L-glutamine (23.2%), algae (18.8%), and calcium (13%).
Modality and Prevalence of CAM Use Among Participants (n = 84).
Abbreviation: CAM, complementary and Alternative medicine.
Chinese herbal medicine, acupuncture and traumatology manipulative therapy were included in the category of traditional Chinese medicine because all are provided by the Taiwanese National Health Insurance Program.

Frequency of use of different types of dietary supplements by the study participants (n = 69).
Reasons for Using CAM and Perceived Benefits From Its Use
Table 4 presents the characteristics of CAM use in the study participants. The most commonly-cited sources of information on CAM were family members, relatives, and friends (50%), followed by health care professionals (25%) and other cancer patients who used CAM (16.7%). The most commonly cited reason for using CAM was “decrease side effects of conventional therapy” (51.2%), followed by “family tradition/culture” (41.7%), “health care/nutrition support” (40.5%), and “recommended by other patients” (31%). Nearly half (46.4%) of the CAM users did not report their CAM use to their physicians. The main reason they gave for not reporting it to their physicians was that they did not believe that consultation with a doctor was necessary (46.2%). Some of the respondents also reported that they believed CAM would not affect the Western medicine treatment (43.6%). Most CAM users (97.6%) experienced no side effects from CAM use, and 90.5% stated that they intended to continue using CAM. Only 7.2% of CAM users reported dissatisfaction with their CAM use.
Patterns of CAM Use (n = 84).

Abbreviations: CAM, complementary and Alternative medicine; NTD, New Taiwan dollar.
More than 1 answer was applicable.
Discussion
The results of our study indicated that in Taiwan, the use of CAM is widespread in BC patients who are also receiving conventional treatment. The prevalence of CAM use we report (82.4%) is higher than those of surveys conducted in other Asian countries, such as Malaysia, Japan and Korea, where the prevalences are 34.8%, 44.6%, and 67%, respectively.21-23 Dietary supplements were the most commonly used type of CAM, followed by exercise and spiritual healing. This finding differs from a report by Ting et al., which indicated that CHM was the most commonly used type of CAM in Taiwanese patients with BC. 24 This difference can be ascribed to the earlier study not excluding herbal remedies or folk medicine from the category of TCM. The other major difference can be ascribed to the current survey being conducted in regular CAM users receiving anti-cancer therapies at a medical center, whereas the earlier study was conducted at an undetermined time after breast surgery in a regional hospital.
Despite the decreasing use of CAM, according to national telephone surveys conducted in Taiwan in 2007 and 2011, 25 the use of CAM is still high in BC patients. The reasons why these patients use CAM and their perceptions of its effectiveness have rarely been reported. In our study, the main indications for CAM use were decreasing the side effects of cancer treatment, family culture, and health support, which is consistent with other reports.4,17 More than 60% of CAM users reported satisfaction with their CAM use and expressed high willingness to continue using it. This finding may explain the high rate of CAM use in our study population. That high rate raises concerns about possible interactions between conventional and CAM therapies. For example, some CHMs may reduce the efficacy of chemotherapy, thereby decreasing its effectiveness in overcoming the disease.26,27 A previous study reported that using herbal remedies during adjuvant chemotherapy for BC could lead to abnormal liver function. 28 In addition, the lack of transparency in the use of dietary supplements by patients may present significant challenges. In this study, 82.1% of the respondents reported having used dietary supplements, and most of these frequently relied on high-protein milk, vitamins, glutamine, and algae. These agents are known to have antioxidant effects which, through multiple mechanisms, can change the pharmacokinetic profiles of drugs administered concomitantly. 29
More troublesome is that most patients reported using multiple CAM therapies in combination. This pattern of usage complicates any efforts to research the effectiveness of CAM with traditional trial designs. We also found that 46.4% of the BC patients who used CAM did not notify their physicians, the main reason being their belief that it was unnecessary, or that it would not interfere with the effects of Western medicine. Indeed, most oncologists in Taiwan have negative views of CAM usage in conjunction with anti-cancer therapies, 30 so related information might not be provided by patients. There is a need for a platform on which patients can disclose their use of all CAMs, and evaluations of potential supplement– or herb–drug interactions need to be conducted during clinical assessments. 31 Simultaneously, efforts are needed to provide better evidence on integrative approaches and to encourage full disclosure and candid discussion among patients, oncologists and TCM practitioners. 32
In our study, the second and third most commonly-used forms of CAM were exercise and spiritual healing (Table 3). Physical activities and exercise may effectively lower the risk and severity of diseases through implementation in a system like that proposed by Jagannathan et al. 33 In our study, 46.4% of the patients also used spiritual healing, specifically prayer, and 80.4% of the patients with BC employed religiosity and spiritual beliefs as coping mechanisms (Table 1). A common practice in all religions in Taiwan, including Buddhism and Taoism, is to incorporate religious beliefs into one’s daily practices, with prayer, worship and exercise (Siu-kiann) being integral pieces of the culture. The prevalent use of both therapies might be ascribed to the common perception that such products, being natural, have no deleterious effects, despite the lack of any scientific support for these beliefs.
As in previous studies, BC patients in this study who were employed, 34 had longer disease durations, 35 and were receiving radiotherapy and hormone therapy 36 were likely to use CAM. BC patients with longer disease durations usually experience higher levels of distress and anxiety about their disease progression. In response, they tend to seek out CAM more than others do. 37 The benefits of CAM in treating the side effects of conventional BC treatment are recognized in many areas. Interestingly, in our patients receiving radiotherapy/hormone therapy, CAM use did not reach statistical significance after a multivariate analysis. An association was found between CAM use and working status, which could simply reflect the greater accessibility to medical information of the employed in Taiwan. Such proactive behavior on the use of CAM is viewed cautiously and skeptically; it is perceived as adopting an optimistic approach and exercising agency in managing one’s personal health by selecting treatments relevant to one’s needs. 38
This study had a few limitations. First, it was cross-sectional in nature. Thus, selection bias could have influenced the results, and no conclusions regarding causality with CAM use can be drawn. Our study focused on CAM use after BC diagnosis, so whether it was only relevant to fighting BC specifically could not be determined. Second, the study was conducted at a single medical center and had a small sample size, so the findings cannot be generalized to all Taiwanese BC patients. Third, self-selection bias might have attracted more CAM users than non-CAM users. Fourth, in Taiwan, a distinction is made between alternative therapy, TCM, and dietary supplements at the legislative level; however, the respondents may not have used or understood the specific definitions of these terms. Conflation of their meanings may have led to over- or underreporting of the use of different forms of CAM. Finally, the non-CAM users may have included patients who had used CAM intermittently or briefly and thus not met the minimum required frequency. This could have led to underestimation of the number of CAM users. A larger-scale, multicenter survey with greater sample diversity should be conducted to develop findings with higher accuracy.
Conclusion
The present study confirms the prevalence of CAM use in BC patients in Taiwan, and the results indicated that the most common forms are dietary supplements, exercise, and spiritual healing. For these patients, the main sources of information about CAM are family, friends, and relatives, and nearly half of the patients do not inform their doctors of their CAM use. Given the danger of potential interactions between cancer and CAM therapies, as well as the limited amount of research in this area that has been conducted to date, it is necessary to systematically evaluate the effectiveness, education and safety of the use of CAM. Furthermore, health care providers should update the evidence on CAM use whenever possible in the cancer journey and investigate the possible effects of CAM on prognosis in BC patients.
Supplemental Material
sj-docx-1-ict-10.1177_1534735420983910 – Supplemental material for Complementary and Alternative Medicine Use in Breast Cancer Patients at a Medical Center in Taiwan: A Cross-Sectional Study
Supplemental material, sj-docx-1-ict-10.1177_1534735420983910 for Complementary and Alternative Medicine Use in Breast Cancer Patients at a Medical Center in Taiwan: A Cross-Sectional Study by Chieh-Ying Chin, Yung-Hsiang Chen, Shin-Chung Wu, Chien-Ting Liu, Yun-Fang Lee and Ming-Yen Tsai in Integrative Cancer Therapies
Supplemental Material
sj-pdf-1-ict-10.1177_1534735420983910 – Supplemental material for Complementary and Alternative Medicine Use in Breast Cancer Patients at a Medical Center in Taiwan: A Cross-Sectional Study
Supplemental material, sj-pdf-1-ict-10.1177_1534735420983910 for Complementary and Alternative Medicine Use in Breast Cancer Patients at a Medical Center in Taiwan: A Cross-Sectional Study by Chieh-Ying Chin, Yung-Hsiang Chen, Shin-Chung Wu, Chien-Ting Liu, Yun-Fang Lee and Ming-Yen Tsai in Integrative Cancer Therapies
Footnotes
Acknowledgements
We thank all our colleagues from the Integrative Breast Cancer Center of Kaohsiung Chang Gung Memorial Hospital for their enthusiastic help in this work. CY Chin and YH Chen contributed equally to this work.
Author Contributions
MY Tsai and CY Chin designed the study. CY Chin and YF Lee acquired the data. MY Tsai, CY Chin, and YH Chen analyzed the data and drafted the figures. MY Tsai and CY Chin wrote the manuscript. SC Wu and CT Liu provided clinical insights and references for oncology. MY Tsai and YH Chen revised the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Taiwan Ministry of Health and Welfare (MOHW107-CMAP-M-114-122111) and funded by Chang Gung Memorial Hospital (CMRPG-8I0381 & 8I0382), China Medical University (CMU109-S-37), and Taiwan Ministry of Science and Technology (MOST 109-2320-B-039-030).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.