
Abstract
Background:
Patients with cancer receiving tumor therapy often suffer from oral mucositis.
Objectives:
The aim of this project was to summarize experiences with nursing procedures by experts in integrative oncology and to establish recommendations for nursing interventions that can prevent or cure mucositis.
Methods:
The study design was an interdisciplinary consensus process based on a systematic literature search.
Results:
The panel discussed and agreed on 19 nursing procedures, which included mouthwashes, such as teas, supplements, oil applications, and different kinds of ice cubes to suck, as well as flaxseed solution, propolis, and mare milk. Twelve interventions were classified as effective, with effectiveness for OraLife, propolis, sea buckthorn pulp oil, marshmallow root tea also for xerostomia, Helago chamomile oil, mare milk, and Saliva Natura rated as highly effective in clinical experience. In the systematic literature search, a total of 12 out of 329 randomized controlled trials and meta-analyses on chamomile (n = 3), Calendula (n = 1) and sage (n = 1), propolis (n = 2), and sucking ice cubes (cryotherapy; n = 5) met all inclusion criteria. Trial evidence for effectiveness in oral mucositis was revealed for propolis and cryotherapy.
Conclusions:
The current evidence supports the use of some nursing procedures (f.e. propolis for 2 and 3 grade mucositis) for improving oral mucositis during cancer therapies. There is still a need to define general clinical practice guidelines for the supportive treatment of mucositis, as well as for more interdisciplinary research in this area.
Keywords
Introduction
Cancer therapies, such as radiotherapy (RT) of the head and neck, various chemotherapies (CT) or hematopoietic stem cell transplantation (HSCT), often cause oral mucositis.
1
This condition leads to oral pain, significant dysphagia resulting in weight loss, decreased quality of life, and therapy discontinuation. Ulcerative lesions can also be secondarily infected and potentially lead to systemic sepsis in immune compromised patients.
1
Oral mucositis affects over 75% of high-risk patients,
2
and thus needs to be urgently addressed in treatment and care for both inpatients and outpatients. In particular, the use of an integrative oncology approach in the prevention and treatment of oral mucositis seems promising. Integrative oncology is defined as a patient-centered, evidence-informed field of cancer care that utilizes mind and body practices, natural products, and/or lifestyle modifications from different traditions alongside conventional cancer treatments. Integrative oncology approach aims to optimize health, quality of life, and clinical outcomes across the cancer care continuum and to empower people to prevent cancer and become active participants before, during, and beyond cancer treatment.
3
Integrative oncology approach requires a multidisciplinary team work including all necessary health professionals such as physicians, nurses, and psychologists. 3 Especially nurses play a key role in the care of oral mucositis within this team. According to our own clinical experiences, nurses in German-speaking hospitals with naturopathic and/or anthroposophic medicine backgrounds often use various applications to prevent or improve mucositis in supportive care for cancer patients.1,4 Therefore, we first needed to identify which integrative oncology strategies different hospitals regularly apply for the prevention or therapy of radio- or chemotherapy-associated mucositis, how these methods are integrated and applied, and whether they are effective and safe. Because of the lack of standardization and differences in levels of evidence in clinical management of oral mucositis, research is needed in this area.5-7 There are limited studies based on consensus processes in the literature in this purpose. The aim of the guideline was to define standards for commonly used integrative oncology approaches in the supportive treatment of mucositis through a structured interdisciplinary consensus process.
Methods
Design
This guideline is based on an interdisciplinary consensus process followed by a systematic literature search. First, we conducted an integrative oncology nursing expert consensus to identify commonly used supportive treatment strategies for mucositis, as well as their perceived efficacy and safety in clinical practice. After expert consensus assessment, a systematic literature search of the identified interventions was conducted.
Consensus Process
We conducted a symposium on nursing in integrative oncology in Essen, Germany, in September 2017. We invited university hospitals and hospitals with expertise in integrative oncology nursing procedures, who also do research in the field of integrative oncology. Additionally, we invited nurses with a high clinical expertise who train nurses in the field of integrative oncology nursing procedures. Experts (nurses, physicians, psychologist) in the field of integrative oncology participated from 6 different institutions in German-speaking countries: Evang. Kliniken Essen-Mitte (academic teaching hospital), Medizinische Hochschule Hannover (University hospital), Filderklinik (nonprofit, anthroposophic hospital), Kantonsspital St. Gallen (Comprehensive Cancer Centre), Robert-Bosch-Krankenhaus (academic teaching hospital), CONGO trial group with StädtischesKlinikum Karlsruhe (academic teaching hospital), Universitätsklinikum Tübingen (University hospital), and Universitätsklinikum Heidelberg (University hospital). This interdisciplinary expert group represented institutes using integrative oncology approaches in clinical practice. To ensure an adequate diversity in expertise, nurses, physicians, and one psychologist with experience in the field of integrative oncology were brought together. The symposium’s purpose was to develop clinical and research recommendations for supportive treatment of mucositis, which are commonly used in clinical practice through a consensus procedure.
In the first round of the consensus process, all nursing procedures for mucositis were collected and discussed by the experts with regard to application and experience with this indication. A total of 19 treatments were evaluated by the expert panel. In a second round, every application was evaluated within the expert panel for safety (rated S = safe or nS = not safe), effectiveness based on clinical experience (CE; rated on a 6-point Likert-type scale from CE 0 to CE 5, with CE 0 = no effect in clinical experience and CE 5 = maximum effect in clinical experience), patient education (rated PE 0 = patient education is not necessary or PE 1 = patient education is necessary), and practical feasibility (rated PF = feasibility not limited, PFt = feasibility limited due to time requirements [more than 15 minutes], or PFc = feasibility limited due to high costs). The financial effort was classified as high when therapy costs exceeded 30€ per month. For consensus, each of the 6 institutions held 1 vote per nursing application only when this method was commonly used in their institution. It was further decided by usual care, practicability, cost, and similar factors whether the method was generally applicable in prevention and/or therapy and/or whether its use was limited to immune-suppressed patients, for example, HSCT.
Literature Search Process
In the literature search, we investigated all 19 treatments discussed in the consensus process. The identified frequently used approaches in the prevention or treatment of oral mucositis were then evaluated based on a systematic literature search in PubMed, the Cochrane Central Register of Controlled Trials (CENTRAL), EMBASE as well as in specialized complementary medicine databases including the CAM summaries, the German version of Onkopedia, and Memorial Sloan Kettering Cancer Center (MSKCC) “About Herbs” database. For PubMed, the complete search strategy was “mucositis or stomatitis” and “cancer” and “(chamomile or Kamistad or Salvia or Repha-Os or Saliva Natura or marshmallow root or flaxseed or propolis or oil extraction or almond oil or cryotherapy or tea or Traumeel or OraLife or mare milk)” (Table 2; see supplementary file, available online). The search strategy was adapted for the other databases as appropriate. Additionally, national and international medical guidelines (AWMF, MASCC) were screened from web pages of Multinational Association of Supportive Care in Cancer 1 and Leitlinienprogramm Onkologie 4 by manual search. The last search date was November 6, 2019. The review was not registered prospectively.
The inclusion criteria were the following: (1) participants were adult cancer patients of any gender or ethnicity, any type of cancers, and any type of cancer treatments (RT, CT, HSCT); the study design was randomized controlled trial (RCT), meta-analysis, or medical guideline; (2) outcomes included oral mucositis or stomatitis measurements; and (3) studies were published in English language. Only those treatments that were evaluated by expert panel in the consensus process were included in the literature search. The study data were extracted by 2 authors (DS, BBS) independently using a standard data extraction approach that included data on study methodology, participants, interventions, comparisons, outcomes, and conclusions. The evidence level of the studies that met the inclusion criteria were evaluated using the Oxford Centre for Evidence-based Medicine (OCEBM). 8
Results
Results of the Consensus Process
Participants were mostly female (93.8%) and nurses (68.8%) or physicians (25.0%) with naturopathic and/or anthroposophical medicine backgrounds. In the setting of a 2-day symposium, the 16 expert participants from 6 different institutions in the field of integrative oncology gathered 19 nursing procedures that could be administered to prevent or treat oral mucositis. Table 1 lists the different interventions and indications and shows the results of the expert panel according to safety (also in immune-suppressed patients), effort of training, practical feasibility, and clinical experience. Table 2 shows the active ingredients of medical agents (OraLife, Saliva Natura, Kamistad STADA, RephaOs, Traumeel).
Expert Judgements for the Different Nursing Applications Based on Expert Consensus.
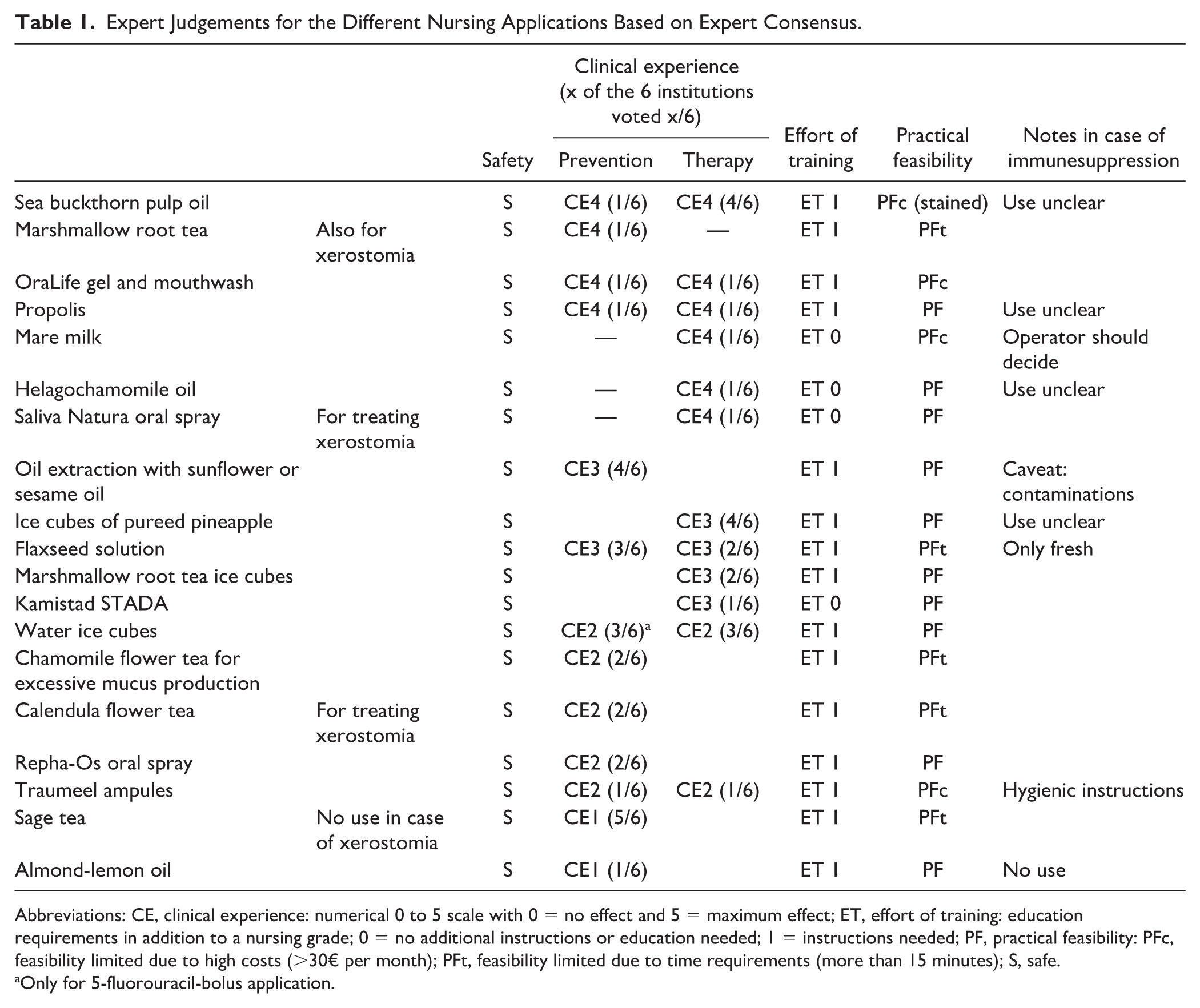
Abbreviations: CE, clinical experience: numerical 0 to 5 scale with 0 = no effect and 5 = maximum effect; ET, effort of training: education requirements in addition to a nursing grade; 0 = no additional instructions or education needed; 1 = instructions needed; PF, practical feasibility: PFc, feasibility limited due to high costs (>30€ per month); PFt, feasibility limited due to time requirements (more than 15 minutes); S, safe.
Only for 5-fluorouracil-bolus application.
Active Ingredients of Medical Agents.

The expert panel established basic safety advice for all nursing procedures: high-quality products should be used, and allergies or a version of taste or smell need to be considered. For teas, it was recommended to use a pharmaceutical quality tea. A common recommendation for all teas was to ensure a fresh preparation and the use of simple instructions such that no special education was necessary. The group did not recommend teas as an intervention in immune-suppressed patients (HSCT, leucocytes less than 1500 per µL). Due to the acquisition of the tea, the cooking procedure, and the necessary fresh preparation, all teas were classified as needing time (PFt). Teas were generally recommended to be used as mouthwash rather than as ingestions, and—if no other procedure was specified—to be used by the patient 3 times per day at a minimum and 6 times per day at a maximum to avoid toxic effects.
Prevention and Treatment of Mucositis
From experts’ opinion, the following nursing procedures were classified as high effective (CE4) for prevention of oral mucositis: sea buckthorn pulp oil, marshmallow root tea, OraLife gel and mouthwash (AgainLife), and propolis. Concerning the feasibility, OraLife and sea buckthorn pulp oil are expensive (40€ to 60€ per month), and the marshmallow root tea needs time to prepare (roots should be allowed to soak for 2 hours). Applications with a relatively effective CE3 (based on the experts’ opinion) were the sunflower or sesame oil extraction and the flaxseed solution. The experts’ institutions recommend these relatively low-cost and easy handling methods (PE1), although the flaxseed solution needs time for preparation (PFt).
Sea buckthorn pulp oil, OraLife gel, and propolis were also classified as high effective (CE4) for the treatment of oral mucositis. Additionally, mare milk, Helago chamomile oil (Helago-Pharma), and Saliva Natura oral spray (Medac GmbH) were also considered effective in the treatment of oral mucositis based on clinical experience as high effective (CE4). All were classified as easy to handle, but mare milk was classified as expensive (PFc). Ice cubes of pureed pineapple, flaxseed solution, tea ice cubes (marshmallow root), and Kamistad gel (STADA) were also recommended for treatment and rated as relatively effective (CE3).
Results of the Literature Search
The literature search revealed a total of 329 publications (128 from PubMed, 192 from EMBASE, 8 from Cochrane Library, and 1 from national and international medical guidelines by manual search1,4; Figure 1); 18 duplicates were removed. Of those, 284 publications were excluded after title and abstract screening because they were not related with oral mucositis (n = 172), not RCTs, meta-analyses, or medical guidelines (n = 89), not human studies (n = 8), and pediatric patients (n = 5), duplicates (n = 7), or the full text could not be accessed (n = 9). Another 9 studies were excluded after reading the full text because they were duplicates (n = 1), used multiple interventions (n = 3), were not published in English language (n = 1), were not RCT, meta-analyses, or medical guidelines (n = 2), were systematic reviews of more than 1 intervention (n = 1), or were a collection of different topics (n = 1).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
After reviewing the findings, 12 trials, for chamomile (n = 3), Calendula (n = 1), sage (n = 1), propolis (n = 2), and sucking ice cubes (cryotherapy; n = 5), were included. None of the included studies reported any serious adverse events, or there was lack of safety data from publications.
In detail for chamomile, 3 RCTs were found that investigated various chamomile preparations for the prophylaxis of RT-, CT-, or HSCT-induced mucositis with contradictory results (Table 3).9-11 Two guidelines1,4 have evaluated chamomile for the prevention of mucositis. However, there was no recommendation for or against the use of chamomile preparations for the prophylaxis of oral mucositis, as the evidence from clinical studies was judged as insufficient.
Characteristics of Selected Studies Included in Literature Review.

Abbreviations: 5-FU, 5-fluorouracil; ALL, acute lymphatic leukemia; AML, acute myelogenous leukemia; BUCY regimen, including cytarabine, busulfan, and cyclophosphamide; C, control; CHX, chlorhexidine; CTC, Common Toxicity Criteria; CTCAE, Common Terminology Criteria for Adverse Events; FT, further treatment; HDM, high-dose melphalan; HSCT, hematopoietic stem cell transplantation; I, intervention, IV, intravenous; MASCC/ISOO, Mucositis Study Group of the Multinational Association of Supportive Care in Cancer/International Society for Oral Oncology; NCI, National Cancer Institute; ns, not specified; OM, oral mucositis; OAG, Oral Assessment Guide; OMAS, Oral Mucositis Assessment Scale; POM, primary outcome measure; RCT, randomized clinical trial; RT, radiotherapy; TPN, total parenteral nutrition; WHO, World Health Organization.
For sage leaves, 1 RCT (n = 60) showed a significantly lower incidence of oral grade 1 chemotherapy-induced mucositis with a hydrosol of sage tea, thyme, and peppermint in addition to basic oral care. This intervention has a prophylactic effect on mucositis in comparison to controls with basic oral care alone 12 (Table 3).
For Calendula, the randomized, placebo-controlled study of Babaee et al 13 showed that the addition of an extract of Calendula flowers as mouthwash to an aqueous gel significantly reduced the level of radiogenic mucositis compared with the application of the gel alone during RT or radiochemotherapy of head and neck tumors (Table 3).
Six RCTs investigated whether oral use of propolis had prophylactic efficacy on oral mucositis compared with placebo or standard treatment. A meta-analysis of Kuo et al 14 analyzed 5 of those trials, 4 with chemotherapy-induced and 1 with RT-associated mucositis, with a total of 209 participants. The incidence of severe oral mucositis was significantly lower in the propolis group than in the control group. No side effects were reported. Furthermore, the new randomized study of Piredda et al 15 with 60 breast cancer patients concluded that propolis plus bicarbonate was safe, well tolerated, and promisingly effective in the prevention of oral mucositis in patients with breast cancer (Table 3).
According to the literature, 16 RCTs investigated whether oral use of water ice cubes had prophylactic efficacy on oral mucositis compared with no or standard treatment. The results of 7 of these studies16-22 demonstrate the efficacy of oral cryotherapy for the prophylaxis of 5-fluorouracil (5-FU; bolus administration mostly combined with leucovorin)–induced oral mucositis. Furthermore, 7 studies confirmed the efficacy of oral cryotherapy for the prophylaxis of oral mucositis due to high-dose CT with melphalan for autologous SCT23-26 or other myeloablative regimens prior to allogeneic SCT.27-29 The results of the study by Gori et al 30 showed no effects of oral cryotherapy for the prophylaxis of oral mucositis induced by low-dose methotrexate given for graft versus host disease prophylaxis after allogeneic stem cell transplantation. The results of the study by Kakoei et al 31 give an indication of the efficacy of oral cryotherapy for the prophylaxis of radiogenic oral mucositis. All mentioned studies were presented with details in the review of Peterson et al 32 and/or the Cochrane Review by Riley et al. 2 The German S3 guideline Supportive Therapy in Oncology 4 partly refers to the MASCC guideline for Oral Mucositis 1 and highlights (1) a recommendation that 30-minute oral ice chewing should be used for the prophylaxis of oral mucositis in patients receiving bolus 5-FU chemotherapy, (2) a recommendation that oral sucking of ice cubes can be used for the prophylaxis of oral mucositis in patients with HSCT with high-dose melphalan (with or without whole-body irradiation), and (3) no recommendation for or against the use of oral cryotherapy for the prophylaxis or therapy of oral radiogenic mucositis, as there is insufficient evidence. The results of the study by Lu et al 33 showed that oral cryotherapy intervention during the whole course or during the second half of the course of the cytotoxic BUCY regimen (including cytarabine, busulfan, and cyclophosphamide) in allogeneic HSCT patients was associated with a lower incidence and shorter duration of severe mucositis (≥grade 3). On the other hand, the highest incidence of severe mucositis was observed in regular oral cryotherapy group (twice a day). Moreover, cryotherapy should not be applied as a part of daily routine care because it could damage the oral mucosa. The results of the study by Park and Lee 34 indicated that cryotherapy was effective for solid cancer patients who receive 5-FU or cisplatin anticancer drugs.
Comparing Consensus-Based Results With Literature Search
The treatments listed in the consensus process shows that 7 applications were classified as high effective (CE4), and 5 applications were classified relatively effective (CE3) for prevention or treatment of oral mucositis.
In the literature research process, of the 19 applications, only 5 applications matched our inclusion criteria of systematic literature search. These 5 applications were propolis, cryotherapy/water ice cubes, chamomile, Calendula, and sage tea. The evidence level of these applications were determined as level 1a for propolis and cryotherapy, level 1b for chamomile, calendula, and sage tea (Table 4).
Comparing Consensus-Based Results With Literature Search.

Abbreviations: CE, clinical experience: numerical 0 to 5 scale with 0 = no effect and 5 = maximum effect; OECBM Level of Studies, Oxford Centre for Evidence-based Medicine; Levels of Evidence, Definition of the level of evidence are as follows: Level 1a: systematic reviews (with homogeneity*) of RCTs, Level 1b: individual RCT; RCT, randomized controlled trial.
Discussion
Cancer patients have a strong need for integrative, nondrug, self-management, and self-efficacy enhancing applications for alleviating symptoms.3,35 In conventional and even more in integrative oncology, nurses often support patients with oral mucositis with individual recommendations during their inpatient stay and provide advice to outpatients.1,21,35 Independent of scientific evidence, recommendations are based on the experiences of therapists and institutions, or on naturopathic knowledge in general. Furthermore, research is rare, the evidence is inconsistent, and most patients with cancer therapy–associated oral mucositis receive a broad range of different mouthwashes of varying quality and efficacy.2,5,9 For the first time, in the setting of a symposium, nurses, physicians, and a psychologist in German-speaking countries with naturopathic and/or anthroposophical medicine backgrounds were brought together to evaluate the usefulness of nursing procedures for oral mucositis from clinical experience and to compare these with evidence from the literature. Nineteen nursing interventions were evaluated in a consensus process from an expert panel and whether interventions are safe and/or easy to apply. Most of the applications were high effective, in the experts’ opinion (Table 1).
In the experts’ opinion, 7 procedures were classified as high effective (CE4) for prevention or treatment of oral mucositis. Except for sea buckthorn pulp oil, all interventions were only applied in one institution each, supporting the known broad range of different applications in hospitals and institutions to prevent or treat oral mucositis. This fact also limits the presented results. More institutions have expertise in and recommend 5 further applications, classified as relatively effective (CE3), all of which are relatively low-cost methods. However, the flaxseed solution and the marshmallow root tea need time and special requirements for preparation and are, therefore, not easily applicable in hospitals. The methods such as sunflower or sesame oil extraction, sea buckthorn pulp oil, and the industrial product OraLife were judged as so promising by the experts that hospitals without previous experience decided to apply these methods from then on.
The first limitation of the consensus process was the small number of participants and institutions. The second limitation is that this does not seem to be a genuine consensus process but in the majority of cases more a single expert opinion. Most listed interventions were often applied only by one center. Despite the high expertise in this panel, important therapy approaches may still be lacking. Furthermore, the efficacy was estimated subjectively and depended on the experience of 1 or 2 practitioners.
Comparing the experience-based results with the literature-based evidence, there was a noted mismatch. No interventional studies existed for 5 of the 7 applications estimated as high effective (CE4). Controlled trials were only found for oral propolis and chamomile interventions. Although the evidence for chamomile in homogeneous preparations is low and inconsistent, the studies for propolis are predominantly of high quality and had a positive outcome for efficacy.9-11,14,15
Procedures with the sunflower or sesame oil extraction, flaxseed solution, Kamistad, and ice cubes of marshmallow root tea or pureed pineapple were rated as relatively effective (CE3). In addition to the aforementioned chamomile preparation studies, only studies with pure ice cryotherapy exist.2,32 However, the guidelines support cryotherapy only for the prophylaxis of oral mucositis in patients receiving bolus 5-FU chemotherapy and in patients with HSCT with high-dose melphalan.1,4 There is no recommendation for RT-induced mucositis due to insufficient evidence. Oral sucking of ice cubes is to be considered as counterproductive in cancer-treating situations in patients with head and neck cancer, especially with cancer in the mouth or oropharynx. Altogether, published evidence for the strategies that were recommended as moderately to highly effective by the expert panel only exists for propolis and ice cubes.
Despite this growing evidence base on supportive nursing application, further research in this field is necessary. High expenditure associated with high costs might aggravate the implementation of such studies in the clinical setting. Therefore, trials on interventions that were judged as relatively effective and less time-consuming and costly (eg, sunflower or sesame oil extraction) should be initiated first to meet patients’ supportive care needs.
Conclusion
Although research is rare, from experts’ opinion, some nursing procedures (propolis for grades 2 and 3 mucositis, cryotherapy for all grades of chemotherapy-induced mucositis and also as a prophylaxis, oil applications and industrial herb preparations for prevention of mucositis) are promising for improving oral mucositis in cancer patients. It is, however, not yet possible to conclusively define the treatment standards for integrative oncology in the supportive treatment of mucositis. Further research is recommended in this area.
Supplemental Material
sj-docx-1-ict-10.1177_1534735420940412 – Supplemental material for Nursing Procedures for the Prevention and Treatment of Mucositis Induced by Cancer Therapies: Clinical Practice Guideline Based on an Interdisciplinary Consensus Process and a Systematic Literature Search
Supplemental material, sj-docx-1-ict-10.1177_1534735420940412 for Nursing Procedures for the Prevention and Treatment of Mucositis Induced by Cancer Therapies: Clinical Practice Guideline Based on an Interdisciplinary Consensus Process and a Systematic Literature Search by Diana Steinmann, Burcu Babadağ Savaş, Sabine Felber, Sosamma Joy, Isabelle Mertens, Holger Cramer, Anna Paul, Monika Layer, Nadja Klafke, Regina Stolz, Ute Heyder, Petra Neuberger, Marcela Winkler, Christel Idler, Rolf Heine, Elke Kaschdailewitsch, Heike John, Beeke Schmeling, Tatjana Zielke, Markus Horneber, Claudia M. Witt and Petra Voiss in Integrative Cancer Therapies
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The consensus conference was supported by the Karl und Veronica Carstens-Stiftung and the Erich Rothenfußer Stiftung. The sponsors provided financial support for costs for travelling, accommodation, conference rooms, and food during the meeting. Research of the first author, DS, and second author, BBS, were supported by the Rut and Klaus Bahlsen Foundation and within the project KOKON, funded by the “Deutsche Krebshilfe” (German cancer aid). The research of the last author, PV, was supported by the Karl und Veronica Carstens-Stiftung. The research of HC was supported by the Erich Rothenfußer Stiftung. No other funding was received.
Ethical Approval and Consent to Participate
All panel participants gave their verbal informed consent for the consensus process at the first symposium for nursing in integrative oncology in Essen, Germany, in September 2017. The need for written consent is deemed unnecessary according to national regulations. The need for ethical approval in Germany is only statutorily regulated for clinical trials on drugs and medical devices, and for stem cell research.36,37 The Medical Association’s Professional Code of Conduct (Berufsordnung für die in Deutschland tätigen Ärztinnen und Ärzte der Bundesärztekammer) regulates the need for further ethical approval of other research conducted by physicians stating that research projects that interfere with a human’s physical or psychological integrity or uses bodily materials or data that are relatable to a specific human need to be approved by an ethics committee. This was not the case in this consensus process. 38
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.