
Abstract
Keywords
Introduction
Breast cancer alone accounts for 30% of all new cancer diagnoses in US women. 1 According to the latest national cancer registration report of Korea, the incidence of cancer has been decreasing since 2011. 2 However, only incidence of breast cancer among the major cancers has shown a steady increase in Korea since 2010, and the number one female cancer in terms of incidence shifted from thyroid cancer to breast cancer in 2016. Because diagnostic examination and treatment methods for cancer have improved, the number of early cancer screenings has risen, resulting in rapid increases in the long-term survival and the 5-year cancer relative survival rates. The 5-year cancer survival rate in Korea in 2016 was 70.6%, with more than 2 out of 3 estimated to survive for more than 5 years. 2
As the survival rate increases, interest in health-related quality of life (HRQOL) is also soaring, with the view that cancer is no longer a threat to survival, but rather should be managed as a kind of chronic disease. Women younger than the age of 50 years diagnosed with breast cancer have been reported to have lower HRQOL than more elderly patient with breast cancer because they face various HRQOL problems throughout cancer diagnosis and treatment. 3 Patients with breast cancer commonly use complementary and integrative therapies to manage cancer therapy and treatment-related side effects to improve the quality of life during cancer treatment. 4 Techniques for enhancing the quality of life for such patients should be developed in a way that can be harmonized with clinical outcomes, and the main factors that influence HRQOL should be identified.
The side effects associated with chemotherapy, especially for breast cancer treatments, have long been a major concern for health specialists, as well as for patients. Chemotherapy-induced peripheral neuropathy (CIPN) is one of the neurotoxic side effects and is due to damage, inflammation, and degeneration of peripheral nerve fibers. Sensory neuropathy accompanied by motor and autonomic changes is a typical symptom of CIPN, 5 which is a common adverse effect of numerous chemotherapeutic agents and a dominant cause of pain influencing the HRQOL in cancer survivors. Antineoplastic regimens, such as oxaliplatin, cisplatin, vincristine, docetaxel, and paclitaxel, cause damage to peripheral sensory, motor, and autonomic neurons. 6 Multiple studies have shown that CIPN severity worsens with the cumulative dose of antineoplastic agents,7-10 and the prevalence of CIPN in cancer patients is reported to range from 19% to 85%. 5 When neurotoxicity is confirmed in individuals undergoing chemotherapy, it can lead to dosage reduction, a change to less effective chemotherapeutic agents, or even the cessation of treatment. 6 CIPN can interfere with the essential treatments to achieve the optimum results and can threaten quality of life. 11 Because CIPN can be extremely disabling and can negatively affect functional ability and quality of life, efforts to develop efficacious prevention or mitigation methods and treatments are ongoing.
At present, no promising remedy to prevent CIPN exists, and even the possibility of treating this syndrome is restrictive. Although clinical guidelines do not suggest a definite prevention or treatment modality, many clinicians prescribe duloxetine or pregabalin for the management of CIPN in cancer patients.12,13 On account of the limited therapeutic options for CIPN treatment, studies have proposed complementary methods for the treatment of CIPN in cancer patients and survivors. We were particularly interested in the synergetic effect of these complementary treatments in support of conventional medication. Several studies have found acupuncture to be an effective treatment for CIPN, and in most of those studies, the alleviation of the pain of peripheral neuropathy in the acupuncture group was found to be superior to that in the placebo group.14-16 Also, electrostimulation (ES) has been reported to have a beneficial effect in patients with breast cancer.17,18 Among the above-mentioned treatments, we selected low-frequency ES as an intervention because the device used for such an intervention is portable, noninvasive, and easy to apply and can be used any time and at any place for the above-mentioned adjuvant therapies, which need to be applied for certain periods at certain places. Therefore, we designed this study to investigate the efficacy and the safety of using a portable, low-frequency ES device for treating CIPN and improving HRQOL in female breast cancer patients diagnosed with CIPN after termination of chemotherapy and found to be in need of medication.
Methods
Trial Design
A single-center, randomized, sham-controlled trial was conducted at the Cancer Center of Chungnam National University Hospital. The design of the study was reviewed and approved by the Institutional Review Board of Human Research at Chungnam National University Hospital (Study Approval Number 2016-11-020). The protocol is registered on www.cris.nih.go.kr (Registration Number KCT0002357).
Participants
Recruitment was conducted from April 2017 to November 2018. Female breast cancer patients newly diagnosed with CIPN were invited to participate by a physician on the study team or were recruited through posters placed in the Cancer Center, Chungnam National University Hospital. Eligibility criteria were as follows: female patients at least 19 years of age who had been diagnosed with primary breast cancer; patients presenting within the first week after completion of chemotherapy with a diagnosis of CIPN with an average pain score of at least 5 on a Numeral Rating Scale (NRS) of pain; patients with an Eastern Cooperative Oncology Group (ECOG) performance status of 0 to 2; patients who had not taken any medication to prevent or treat neuropathy before screening; patients who were willing and able to comply with the requirements of the study; and patients who were willing and able to provide written informed consent. Exclusion criteria were the following: patients with a history of receiving chemotherapy for cancer before this diagnosis was made; patients with preexisting peripheral neuropathy due to trauma or intercurrent illness; patients with symptoms of peripheral neuropathy that were severe and needed to be treated immediately with surgical procedures or acute management; patients with a history of previous use of an acupressure wristband over a week; patients with skin inflammation at the attachment site; patients with a history of cardiovascular disorders, including the use of a pacemaker; patients with known hypersensitivity to metal or any medication; patients with uncontrolled hypertension (systolic blood pressure ≥170 mm Hg or diastolic blood pressure ≥100 mm Hg) or uncontrolled diabetes; patients with hepatic insufficiency or dysfunction (3 times higher than normal levels of aspartate aminotransferase, alanine aminotransferase, and creatinine); patients who had psychiatric disorders or who had taken medication for psychiatric illnesses; patients who were pregnant or potentially pregnant; and patients who were breastfeeding. Participants who satisfied the inclusion and the exclusion criteria were then randomly assigned to either the low-frequency ES arm or the sham ES (SES) arm. The intervention continued for 2 weeks. We obtained informed consent from each participant before starting any data collection in this study.
Interventions
The interventional medical device (Careband; Piomed Inc, Seoul, Korea) we used for managing CIPN symptoms was a wearable wristband device that generated low-frequency ES (Figure 1). Although the sham device did not generate an electrical stimulus, the appearances of the 2 devices were the same. Both the interventional device and the placebo device were labeled identically for blinding. The participants were educated to use the devices on the second stage (100 µA, 40 Hz) at least twice a day for no less than 120 minutes, which included an uninterrupted 1 hour of use, for more than 14 days. ES was applied at the unilateral PC6 acupoint, which is located approximately 3 finger breadths above the wrist crease between the palmaris longus tendon and the flexor carpi radialis tendon. 19
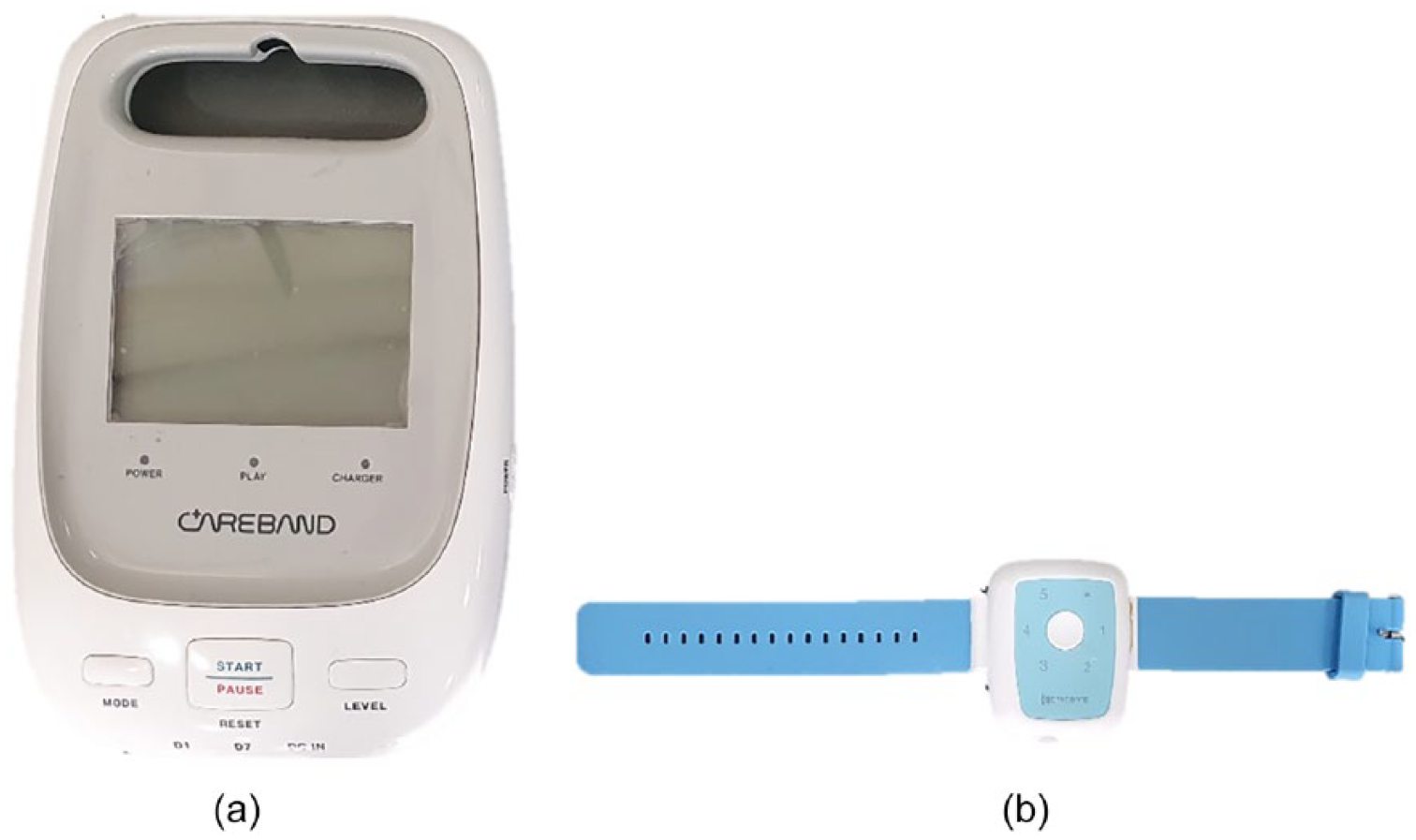
The picture of low-frequency electrostimulation interventional medical device (Careband; Piomed Inc, Seoul, Korea): (a) control box; (b) wrist band.
Duloxetine or pregabalin was prescribed to all participants from the initial treatment, and any changes in the dosage were limited. Supplementary treatments, such as physical therapy, paraffin bath therapy, and so on, for CIPN symptom alleviation were restricted.
Outcomes
Primary Outcome
The primary outcome measures were the overall intensities of the CIPN symptoms, which were assessed using an NRS, in women treated with chemotherapy for breast cancer. This scale is widely used in clinical practice, and its validity has been proven in numeral studies.20,21 Patients were asked to rate the intensity of the average daily pain due each of their symptoms on an 11-point scale ranging from 0 (no pain) to 10 (worst possible pain). The assessments were done at baseline and posttreatment at the 2-week follow-up.
Secondary Outcomes
The secondary outcome measures were the physician-rated CIPN symptom severity; the Total Neuropathy Score (TNS), a patient-self-report questionnaire; the European Organization for Research and Treatment of Cancer Quality of Life (EORTC-QLQ); Chemotherapy-Induced Peripheral Neuropathy 20 (CIPN20); perceived HRQOL; Functional Assessment of Cancer Therapy–Breast (FACT-B); and Instrument for Pattern Identification and Evaluation for CIPN (IPIE-CIPN). The TNS was graded by a physician to assess the presence, severities, and locations of symptoms. This scale was originally developed for evaluating diabetic neuropathy and was later validated in cancer patients with peripheral neuropathy.22,23 The TNS includes integrated information obtained from the grading of symptoms, nerve conduction studies, and quantitative sensory tests. The TNS combines 10 symptom scores; including sensory, motor, and autonomic symptoms; pin sensibility; vibration sensibility; and deep tendon reflex scores.24,25 Each neuropathy item was scored by a neurologist on a scale of 0 to 4, so the TNS ranged from 0 to 40.
EORTC-QLQ CIPN20 was utilized to measure the distress caused by patients’ symptoms and the functional limitations related to CIPN. This instrument includes 3 subscales assessing sensory (9 items), motor (8 items), and autonomic (3 items) symptoms. Each item is rated on a 4-point Likert-type scale ranging from 1 (not at all) to 4 (very much). 26 This technique is known to be consistently valid, reliable tool for evaluating individuals with CIPN.27,28
FACT-B was administered to measure physical, social/family, emotional, and functional well-being and has a breast cancer–specific subscale that assesses symptoms and concerns related to breast cancer patients. 29 The FACT-B is a 37-item measure, and in various international studies, it has demonstrated good reliability, validity, sensitivity, and suitability.30-32
The IPIE-CIPN was used to diagnose and evaluate CIPN from the perspective of traditional Oriental medicine.33,34 This instrument includes 30 items, which can be allotted into 4 patterns: wind arthralgia, cold arthralgia, dampness arthralgia, and arthralgia of a deficiency type. All items were rated by an Oriental medicine doctor on a 5-point Likert-type scale; higher scores indicated greater distress in each CIPN pattern.
Assessment of Safety
At each visit, participants were monitored for occurrence of any adverse events. The number and the type of adverse event were noted, evaluated by the study investigator, and reported to the Institutional Review Board of Human Research, Chungnam National University Hospital. Assessment of severity was classified as mild, moderate, or severe according to 3 levels based on maximal intensity.
Sample Size
Sample size was that used for a published protocol study 35 and was estimated based on changes in the NRS between baseline and the end of treatment. The power of this study was set at 95%, and the 2-sided significance level was set at .05. The estimated requisite number of participants was 32 per group to detect the superiority of ES by using a t test. 35 The initial aim was to recruit 40 patients for each group considering a possible dropout of 10%. We only managed to enroll 36 in the ES group and 36 in the SES group. The recruitment period was extended in an attempt to achieve the goal of 40 patients in each group, but the enrollment was terminated because the minimum number of patients (32) had been achieved and continued recruitment was proving to be difficult.
Randomization and Blinding
Eligible participants were randomly assigned to the ES group or the SES group. The accessory use of neuropathy medications during the trial was a confounding feature that could influence the outcomes. Therefore, the randomization was stratified according to the prescribed medicine for neuropathy. Randomization was conducted using SAS version V9.4 (SAS Institute Inc, Cary, NC). Its procedure was managed by a research assistant who did not take part in any of the following: interview, data collection, intervention, and statistical analysis. A link between the randomization code and the corresponding treatment stayed blinded for all other members of the study team. All study members, participants, and clinicians who evaluated outcomes were blinded to treatment allocations until the end of the study.
Statistical Methods
Evaluable participants were defined as those who had received treatment using the medical device and had completed more than one measurement of the main evaluation variable. The efficacy of the intervention was analyzed according to a Full Analysis Set (FAS). For the primary outcome, missing data were handled using the last-observation-carried-forward method. Demographic and clinical characteristics were described as frequencies and composition ratios. Categorical data were described as frequencies and percentages, and continuous data were presented as means and standard deviations. To compare with the baseline outcomes between groups, we used the independent t test or the Wilcoxon rank sum test to analyze continuous data, and we used the χ2 or Fisher’s exact test to analyze categorical data. Mean differences from baseline to the end of treatment in each group were computed to evaluate the effectiveness of treatment. The Wilcoxon rank sum test was used to analyze the differences in the primary and the secondary outcomes between groups. Clinically relevant covariates were included in these analyses. For all analyses, statistical significance was set at P < .05. All statistical analyses were done using SPSS version 22 (IBM SPSS Inc, Chicago, IL) software by a statistician blinded to patient allocation.
Results
Participant Flow
Between April 2017 and February 2018, a total of 72 subjects were screened for eligibility and were randomized into either the ES arm (n = 36) or the SES arm (n = 36). Among the participants in the ES arm, 30 completed treatment, 3 stopped taking the prescribed medicine, 1 violated the protocol by taking a prohibited medication, 1 withdrew consent, and 1 showed a low device compliance of under 70%. In the SES arm, 34 completed treatment, and 2 withdrew consent. Figure 2 shows a CONSORT diagram.

CONSORT diagram of patient recruitment, randomization, follow-up and analysis. CONSORT, Consolidated Standards of Reporting Trials; ES, electrostimulation; SES, sham electrostimulation.
Participant Characteristics
The mean age of the participants was 50 (standard deviation = 8.85) years. Demographic and clinical characteristic, such as age, height, weight, vital signs, medical history, and laboratory blood test results, showed no differences between treatment groups (Table 1). From those randomized, 61% indicated an ECOG performance score of 0, and no inflammation or abnormality was found on physical examination. Every participant had a medical history, and laboratory results were either normal or showed no differences of clinical significance. Information pertaining to demographics and clinical characteristics can be seen in Tables 1 and 2. The patient’s chemotherapy regimen and baseline disease-related features are shown in Table 3. One participant had bilateral breast cancer diagnosed with different stages. For most of the CIPN cancer patients (86%), the prescribed concurrent medication was pregabalin, and both pregabalin and duloxetine were administered to one of the participants in the ES arm because of symptom severity.
Patient Demographics and Clinical Characteristics.

Abbreviations: ES, electrostimulation; SES, sham-electrostimulation; SD, standard deviation; AST, aspartate aminotransferase; ALT, alanine aminotransferase.
Patient Baseline Clinical Characteristics.

Abbreviations: ES, electrostimulation; SES, sham electrostimulation; ECOG, Eastern Cooperative Oncology Group; AST, aspartate aminotransferase; ALT, alanine aminotransferase; NCS, no clinical significance.
Patient Chemotherapy Regimen a and Baseline Disease-Related Features.

Abbreviations: ES, electrostimulation; SES, sham electrostimulation.
One of the participants had bilateral breast cancer diagnosed with different stages; each stage was counted independently. Both pregabalin and duloxetine were administered to one of the participants in the ES arm because of symptom severity.
Numbers Analyzed
Statistical analyses were performed on all 72 patients. FAS was used so that every patient was considered in the analysis of the primary outcome. The purpose of this study was to measure carefully the effect of low-frequency ES in a small sample and to test the safety, feasibility, and acceptability of using ES, along with duloxetine/pregabalin, to treat CIPN in patients with breast cancer.
Outcomes and Estimates
Primary Outcome
The primary outcomes, which were the intensities of CIPN symptoms on the NRS, were not significantly different between the ES and the SES groups (P = .267). However, in both groups, the intensities of the CIPN symptoms were significantly reduced from baseline (ES P < .001; SES P < .001). For participants with NRS ≥6, a statistically significant result was seen in both the ES and the SES arms, but only the ES arm showed a statistically significant result in the subgroup with NRS <6 (Table 4). In the group with reduced NRS, the degree of diminution for the treatment group was larger than that for the control group, but no overall difference was found between the 2 groups (P = .072).
NRS at Baseline (V2) and Posttreatment (V3).
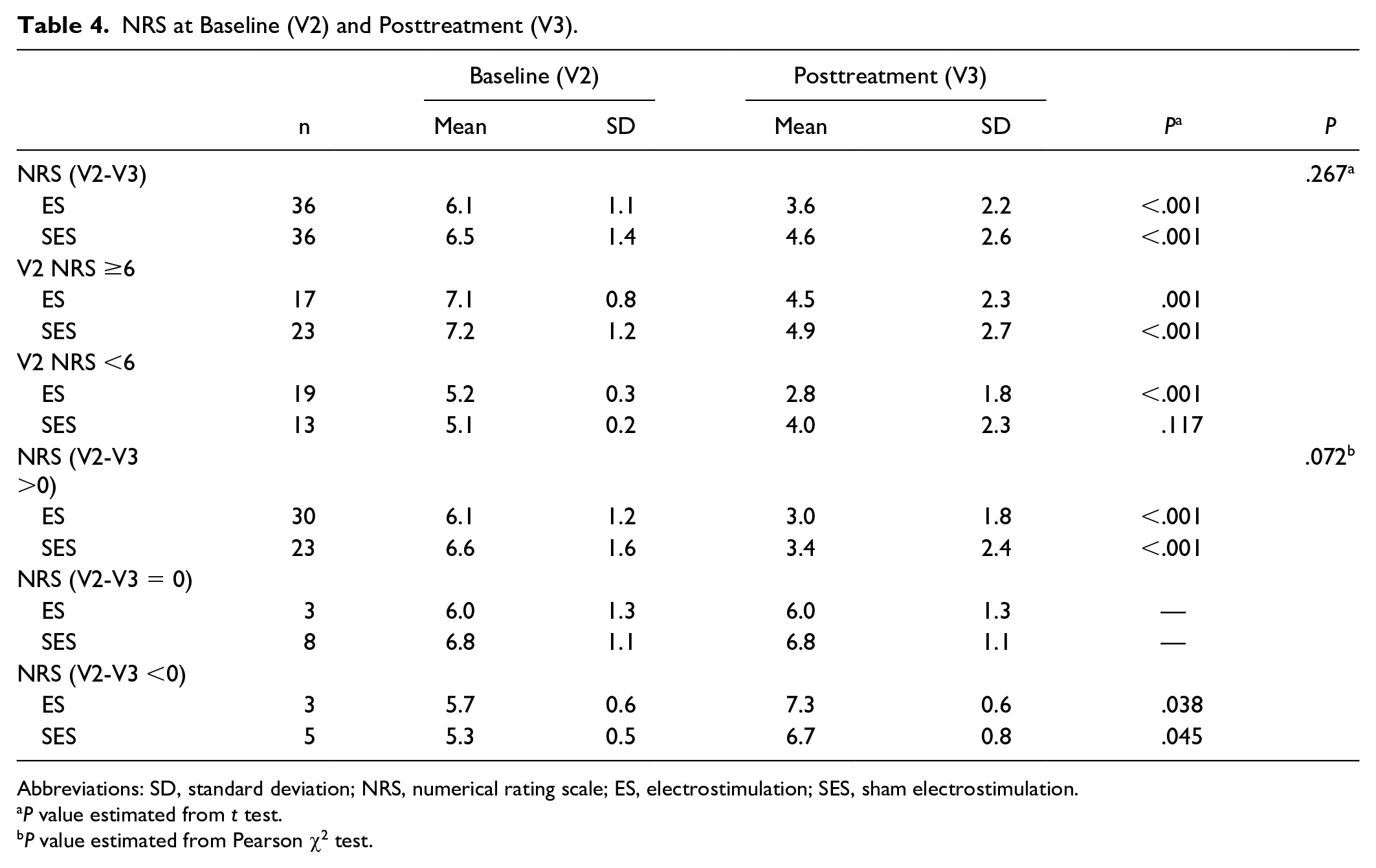
Abbreviations: SD, standard deviation; NRS, numerical rating scale; ES, electrostimulation; SES, sham electrostimulation.
P value estimated from t test.
P value estimated from Pearson χ2 test.
Secondary Outcomes
The TNS, EORTC-QLQ CIPN20, and FACT-B showed no remarkable changes from the baseline measures. Based on the TNS, no statistically significant difference was noted between the 2 groups; nevertheless, the mean change from baseline was greater in the ES arm than in the SES arm, indicating that the general neuropathy grades had improved (Table 5). Only for patients diagnosed with cold arthralgia by using the IPIE-CIPN were significant differences in general symptoms observed between the ES and the SES groups. No improvements in pain-related symptoms were observed (P = .006; Table 6).
TNS, CIPN20, and FACT-B in Electrostimulation and Sham Electrostimulation.

Abbreviations: TNS, Total Neuropathy Score; CIPN20, Chemotherapy-Induced Peripheral Neuropathy 20; FACT-B, Functional Assessment of Cancer Therapy–Breast; ES, electrostimulation; SES, sham electrostimulation; SD, standard deviation.
IPIE-CIPN in Electrostimulation and Sham Electrostimulation.

Abbreviations: IPIE-CIPN, instrument on pattern identification and evaluation for chemotherapy-induced peripheral neuropathy; SD, standard deviation; ES, electrostimulation; SES, sham electrostimulation.
Adverse Event
No serious adverse events related to ES occurred during the study. Nineteen participants reported minor adverse events: diarrhea, lymphedema, edema of the limbs, flu-like symptoms, febrile neutropenia, back pain, gastritis, pain in the extremities, adhesive capsulitis of the shoulder, and dermatitis. Most symptoms, except lymphedema and edema of the limbs, disappeared within 10 days after their appearance (Table 7).
Adverse Events Reported.

Abbreviations: ES, electrostimulation; SES, sham electrostimulation.
Discussion
Chemotherapy-induced peripheral neuropathy is a common, potentially painful, debilitating, and dose-limiting side effect of taxane-containing chemotherapy agents and affects 30% to 40% of breast cancer patients. 11 The commonly used antineoplastic substances, oxaliplatin, cisplatin, vincristine, docetaxel, and paclitaxel, cause severe acute and chronic peripheral neuropathies.6 Drugs for neuropathy include anticonvulsants, such as gabapentin, pregabalin, and carbamazepine, and antidepressants, such as amitriptyline, nortriptyline, and duloxetine. According to the clinical guidelines for CIPN published by the American Society of Clinical Oncology in 2014, the only drug recommended for the treatment of CIPN is duloxetine. 13 Evidence for the efficacy of treating CIPN with agents such as nortriptyline, gabapentin, and compounded topical gels, including baclofen, amitriptyline HCl, and ketamine, is lacking, but they are prescribed based on data that supports their having effects on other neuropathy pains. 13 Although, at present, pregabalin is widely used in clinical practice for the treatment of patients with CIPN, no convincing clinical evidence showing its efficacy has been reported to date.
When the targeted CIPN pain is above moderate to severe, an add-on drug or other treatment is necessary; therefore, a therapeutic technique that can be used along with conventional medications would be useful. In view of the absence of a standard guideline for the prevention and/or treatment of CIPN, many existing studies have searched for safe, complementary methods. We studied the effectiveness and the safety of the simultaneous use of an intervention device from the viewpoint of integrated medicine.
The scores on the NRS for the intensities of the symptoms due to CIPN declined in both the treatment and the control groups, but statistical significance was not found in the primary outcome. Concerning patients for whom the score on the NRS was reduced after treatment, the extent of the reduction was greater in the treatment group than in the control group, and this difference between the 2 groups showed borderline significance (P = .072). This indicates a possibility of having a significant result for a larger number of participants. The combination of low-frequency ES and pharmacological intervention was expected to produce synergetic effects; however, the symptoms were improved in both groups. Thus, observing any significant difference with such a small number of participants (ES n = 30; SES n = 23) would have been difficult. Finding the efficacy in this study was demanding because all participants in the treatment and the control groups took either duloxetine or pregabalin as prescribed for their CIPN. Despite the challenge, our research team thought that the use of low-frequency medical devices might be helpful in patients for whom medications had failed to reduce the symptoms of CIPN sufficiently. The more severe the symptoms of CIPN are, the more meaningful would treatment with the ES device be, thus eliminating the need for high-dose medications.
The Careband low-frequency ES device is simple to use, and because no serious side effects were observed during the treatment, it has the advantage that it can be easily used by clinicians and patients. In the current trial, lymphedema and edema of the limbs were symptoms that occurred most commonly in participants who had had their lymph nodes removed during cancer treatment. Because use of the noninvasive Careband to influence lymphatic channels for infections/infestations is implausible, remaining adverse events are expected to be associated with postoperative conditions rather than interventions. Therefore, the range of applications of the Careband low-frequency ES device is most likely much wider.
Based on a review of randomized controlled trials that evaluated the effects of electroacupuncture and transcutaneous electrical nerve simulation on patients experiencing CIPN, we concluded that the stimulation of electroacupuncture should be low frequency. Because the numbers and the durations of the interventions in the studies that we reviewed were so heterogeneous, we investigated the clinical research design for the Scrambler therapy further. Various clinical studies have reported the effect of Scrambler therapy on patients with CIPN.36-38 Ricci et al reported that cancer patients who had been treated using a cutaneous ES device showed clear reductions in chronic pain by the second week of treatment. 39
The wearable, noninvasive ES medical device used in this study is noninvasive, portable, and easy to apply. Moreover, it can be operated regardless of location or time and does not require expert hands. Given the unremitting nature of CIPN, we consider the Careband therapeutic device to be acceptable for the treatment CIPN in patients with breast cancer. The Careband low-frequency stimulator consists of a wristband, a battery, and a control box. The low-frequency signal generated from the electrode attached to the back of the band stimulates the peripheral nerves. The electrical stimulation when using the Careband device in stage 2 is 100 µA at 40 Hz. Based on existing study designs, in this study, we used the Careband device for 60 minutes per session at least twice a day. Previously, we reported a case of ES for the treatment of CIPN in a breast cancer patient, and the clinical setting was the same as that in the present study. The symptoms of CIPN, measured by using a Patient Neurotoxicity Questionnaire and the Visual Analogue Scale, showed significant improvements. 17 The analgesic effect of ES does not result from the injection of a substance with pharmacological activity into the body, but rather from the activation of the descending pain inhibitory pathway through peripheral nerve stimulation to induce analgesic efficacy.
In selecting the acupoint, important considerations, along with the therapeutic effect on CIPN, are conditions that will make the wearable devices easier to wear and will not cause inconvenience during daily activities. The acupoints selected from existing study designs are located at the end of the toe/knee joint or finger/elbow joint and include as many as 28 acupoints at a time. Despite their effectiveness in mitigating CIPN, the acupoints on the toe/knee joint and the finger/elbow joint were excluded because using a wearable device with constant electrical stimulation attached at those points would have been inconvenient in everyday life. Neiguan (PC6) is the most common acupoint used for wristband-type acustimulation. 18 It was selected because of its location and known therapeutic effects of regulating qi, having a tranquilizing effect, and relieving pain.
No clear assessment of CIPN symptoms exists to date.24,40 In this study, several assessment tools, such as the NRS, TNS, IPIE-CIPN, FACT-B, and EORTC QLQ-CIPN 20 questionnaire (the last item on the questionnaire was excluded because it was unsuitable for female patients), were administered for evaluation. Participants were diagnosed as having CIPN prior to this study by an independent assessor who did not take part in the study. Because of the wide and varied pattern of CIPN complaints, the assessments were performed using several measurement tools. The TNS scale is a scoring system that can detect minute changes in peripheral neuropathy. 24 In this study, the neurologist directly assessed the degree of peripheral neuropathy in the subjects by using the TNS scale, thereby enabling a more thorough evaluation of efficacy. The IPIE-CIPN is a measurement developed for patterning CIPN symptoms into 4 types of arthralgia.33,34 It was designed to be used as an objective and scientific diagnostic evaluation tool in clinical research and treatment by Oriental medicine physicians. Also, its reliability and validity were shown in our pervious study. 34 Due to its compatibility with the existing Peripheral Neuropathy Assessment scale, we considered it appropriate for evaluating the use of this low-frequency ES device in the treatment of CIPN in breast cancer patients. The quality of life of the subjects was assessed on the FACT-B scale and the CIPN 20, which were classified into specific subscales related to disease or symptom and made a detailed evaluation possible.26,30-32
Limitations of our study are as follows: the doses of the concurrent drugs, pregabalin and duloxetine, differed from patient to patient according to the intensities of the symptoms the patients complained of. Also, the co-administration of pregabalin and duloxetine could be the reason for the difference between the ES and the SES arms being less statistically significant. Because statistical analyses were done by using the FAS design and follow-up was only done once in 2 weeks, bias against missing data was inevitable. In addition, various arms could have been, but were not, set up to perform further studies on different acupoints, such as PC6 and ST36, or to compare therapeutic efficacies among a gabapentin with ES arm, an ES only arm, and a gabapentin only arm.
The National Comprehensive Cancer Network Guidelines for adult cancer pain recommend combining integrated interventions with pharmacological interventions as needed, particularly among vulnerable groups such as the frail and the elderly. 41 The usefulness of integrated interventions highlights the necessity for pain management to be performed through a team approach that includes a wide range of treatment options. Notwithstanding the limitations, this research is notable because it suggests another possibility, ES with a wearable device, for integrated medical care.
In this study, we observed that ES using the wearable device had a certain level of effectiveness in reducing peripheral neuropathy pain compared to the drug-only treatment, but unfortunately, we were unable to observe a superior quality of life associated with its use. Although no statistically significant difference in symptom severity was noted between the low-frequency ES and the SES groups, use of the device is worth consideration because it did have a remarkable effect in the treatment group without any serious side effects. Also, for the patients in whom the score on the NRS was lower after treatment, the use of the ES device had borderline significance, so clinicians may well consider using it to treaty CIPN patients complaining of excessive pain. For patients diagnosed with cold arthralgia by using IPIE-CIPN, the effects on their general symptoms were positive, confirming the potential of this device as a therapeutic option for patients who show symptoms of CIPN. However, additional studies are needed because the number of patients diagnosed with cold arthralgia was too small.
Conclusion
In summary, low-frequency ES was effective and safe in treating CIPN pain immediately after termination of chemotherapy for patients with breast cancer. This result shows the possibility of an integrated therapy as a safe treatment to compensate for the disadvantages of oral medicine.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI) funded by the Ministry of Health & Welfare, Republic of Korea (Grant Number HI15C0007); and the Traditional Korean Medicine R&D Project, Ministry of Health & Welfare, Republic of Korea (Grant Number HI15C0006).
Ethics Approval
The design of the study was reviewed and approved by the Institutional Review Board of Human Research of the Chungnam National University Hospital (Study Approval Number 2016-11-020).