
Abstract
Introduction
Breast cancer is the most common female cancer and second most common cancer worldwide. 1 The Polish National Cancer Registry recorded over 18 600 new cases, and almost 6500 breast cancer deaths in Poland in 2016. 2 It is estimated that in the coming decade, around 20 000 Polish women per year will be diagnosed with the disease. 3 Early detection is the most effective way of tackling breast cancer: if the disease is diagnosed when confined to the breast, 5-year survival reaches 98.6%, 4 but if the disease has spread to regional lymph nodes, or is disseminated, survival declines to 83.8% and 23.3%, respectively. 5
When comparing breast cancer statistics in Poland with Western Europe or even the United States, the rate of survival was significantly inferior (77.4% vs 90.0% in Western Europe—EUROCARE-4 study). 6 The causes were ineffective early diagnostics, owed to a preliminary lack of breast cancer outreach programs, low participation in screening, and ineffective health care systems, causing delays in therapy. 7 According to data from the Main Coordination Centre for Population Based Programme for Early Detection of Breast Cancer, only 35% of entitled women (aged 50-69 years) take part in screening programs in Poland. 8 While this number is certainly low, it was shown that early detection of breast cancer by mammography in women aged 40 to 69 years is associated with a reduction in breast cancer mortality. 9 In a reduced subset of these patients (40-59 years old), 47% of breast cancer neoplasms are detected, 10 owing to a significant number of patients who are not included in the nationwide screening program.
Unfortunately, in Poland, mammographic screening is offered by the Ministry of Health to women between 50 and 69 years of age. In women younger than 50 years, mammographic screening is not offered as part of the program, 11 and an individual approach to the identification of early breast cancer in younger women is suggested based on an assessment of the risk of developing the disease. 9 Literature shows that the age range to be included in screening programs is still not optimal and should be further increased from 40 to 74 years in Poland,10,12 while epidemiological data show that around 7% of all breast cancer cases are diagnosed in women younger than 40 years of age. 13 For this group, the most frequently suggested diagnostic examinations are ultrasound and magnetic resonance imaging (MRI). 14 Although breast self-examination is easy to perform, it appears ineffective for the detection of early-stage disease and is recommended mainly to increase breast cancer awareness. Physical examination by physicians, nurses, or other health professionals appears similarly ineffective. 15 Therefore, new methods should be examined to tailor to the younger population, where no guidelines currently exists.
Ultrasound is safe and widely used for assessing palpable breast abnormalities in young women. However, the false-negative rate for clinically occult lesions may be up to 47% resulting in diagnostic and therapeutic delay. 16 Ultrasound is also characterized by a relatively high false-positive rate, reaching up to 8.1% when used without an adjunctive modality.11,17 False positives are also a problem with MRI, which, coupled with high cost and requirement for contrast, means that MRI is unsuitable as an early diagnosis tool.11,15 There is, therefore, a need for a cost-effective method for the early diagnosis of breast cancer in younger women.
Thermography is a noninvasive imaging technique that can detect breast cancer at an early stage because cancer cells have a higher metabolic rate and augmented blood supply and are hence at a higher temperature than surrounding healthy tissue. 18 In 1956, Lawson observed that skin temperature above breast tumors is increased. 19 Thermographic breast imaging using infrared cameras has been investigated as a tool for cancer detection. 20 Despite promising results, however, the technique has not been approved for early detection 21 mainly because of a lack of standardized examination protocols and devices, poor reproducibility, lack of authoritative guidelines for interpreting thermographic images, and poor quality of research articles. 22
The Braster Tester (Braster SA, Ozarów Mazowiecki, Poland) is a liquid crystal (LC) thermography device developed to provide high-resolution contact thermographic images of the breasts. It provides color images (thermograms) indicating the temperature variation over the surface of the breast in direct contact with a LC foil. The images are recorded with a digital camera built into the device. Breast malignancies appear in thermograms as areas of increased temperature or thermal asymmetry. The technology was assessed in 3 observational substudies, totaling 1350 women, with 500 cancerous cases detected and a pathway for automatic detection of the thermograms in the future. 23 Additionally, a case report using the device showed its clinical efficacy in the target population (female subject was 39 years old), where the lesion was undetected on mammography due to breast density but visible on contact thermography. 24
The purpose of the present pilot study was to evaluate the safety and provide a preliminary evaluation of the ability of contact thermography, using a Braster device, to detect breast cancer. Specific aims were the following: (1) to compare C-statistic, sensitivity, and specificity for thermography between groups of women of differing age (<50 years and ≥50 years) with abnormal breast ultrasound; (2) to estimate predictive values of positive and negative thermography findings in women with abnormal breast ultrasound; and (3) estimate the false-positive rate for thermography in women with normal breast ultrasound.
Patients and Methods
This was a prospective study on women presenting consecutively at 6 specialized outpatient breast centers in Poland for screening breast examination. Study design and protocol were approved by the Ethics Committee of the Krakow Chamber of Physicians; the study complied with Declaration of Helsinki guidelines.
Patients
Women were eligible if they underwent a breast ultrasound (with outcome Breast Imaging Reporting and Data System [BIRADS] 1, 2, or 4A-5), had no breast surgery over the previous year, no core biopsy over the previous 3 months, no previously diagnosed breast cancer, were not pregnant or lactating, and had no symptoms/signs of local or generalized infection. Those recruited signed an informed consent form that also gave permission to use medical information (clinical characteristics, ultrasound, mammography, and pathology findings) for study purposes. A total of 274 women, 25 years of age and older, were recruited consecutively between June 2015 and April 2016. Mammography was performed in some patients younger than 50 years and in all women older than 50 years of age. The thermographic examination was performed at least 2 hours after breast ultrasound but during the same day. This allowed the breast to cool to physiologic temperatures, which mitigated potential artefacts.
Tested Medical Device
Braster is a certified class IIa medical device that uses a thermosensitive LC foil to acquire red, green, blue (RGB) images from the surface of the breast (contact thermography). Braster consists of a camera, light-absorbing dome, light source, and detachable LC foils (Figure 1). A series of images are acquired when the device is applied to a subject’s breast, with the foil being held against the breast for a period of 15 seconds and subsequently removed and transferred to another area of the breast, following a clockwise pattern. Since a single application does not usually cover the entire breast, the examination procedure captures several such application sequences, covering each area of the breast (3 or 5 applications per breast, depending on breast size).

Simplified schematic of the Braster device.
The overall body temperature of the patient varies; thus, the breast thermogram interpretation methods rely on relative temperature rather than absolute temperature. In order to obtain interpretable images of such relative temperatures for subjects with different breast temperatures, foils with 3 different temperature ranges are used. Foil 1 has a thermal range of 31.5°C to 33.1°C; foil 2: 32.8°C to 34.4°C; and foil 3: 34.1°C to 35.7°C. When the LC foil is illuminated with polychromatic (white) light, a certain range of wavelengths is selectively reflected, and the remaining light is absorbed by the absorption layer of the foil. 25 These foils are manufactured to have identical color profiles within their active temperature ranges. 23
Thermographic Examination
Thermography was performed with the Braster device by trained medical staff. Adverse events, serious adverse events, and events considered causally related to use of the Braster were recorded. Patients were required to abstain from alcohol for at least 2 hours prior to the examination and refrain from physical exertion for at least 30 minutes before. Thermographic images of both breasts were obtained, and the findings were assessed independently by 2 trained radiologists blinded to patient clinical, ultrasound, mammography, and biopsy finding, and in case of disagreement, the image was sent to a third radiologist also blinded to patient data.
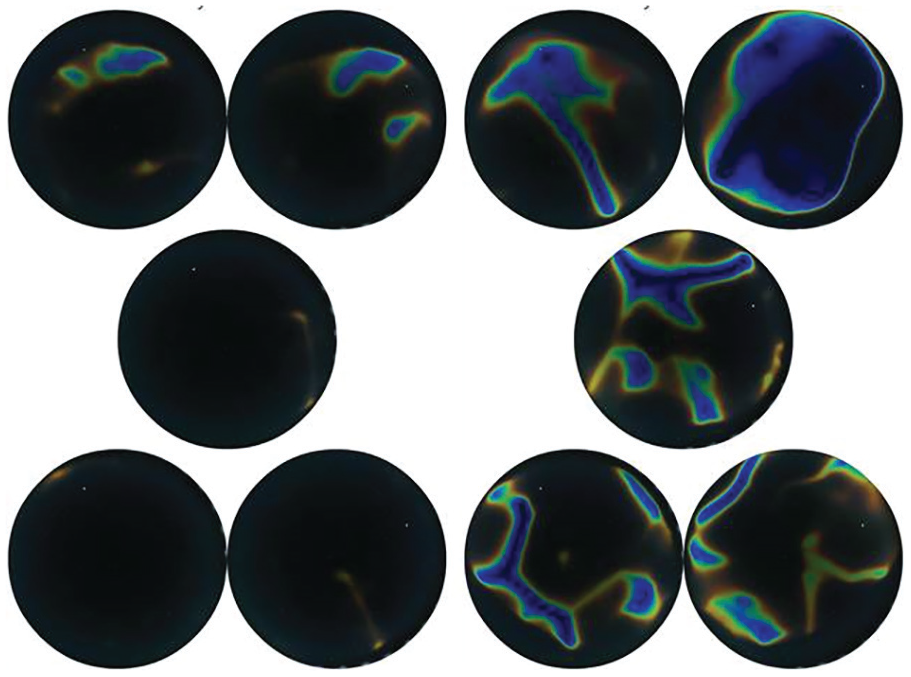
The radiologists followed a preestablished protocol for assessing thermograms, involving comparison of the thermal and structural characteristics of both breasts. Three characteristics were considered: (1) Thermal anomaly score: absolute difference in the number of distinct warm areas in both breasts (Figure 2). This was performed manually with the radiologist counting the warm areas in both breasts. A result was clinically significant for a pathology if there are more than 2 warm areas visible in either breast. Temperature score: characterized by temperature differences between the breasts comparing the color distribution in the 2 thermograms (possible score range 0-5). This was also performed manually, using a color scale (Figure 3). If the color saturation of the warmest structure, found in both breasts, was over 2 gradient points, the result was clinically significant for a pathology. Risk indicators: determining the presence/absence of 3 extraordinary situations indicating increased breast cancer risk: (a) nonlinear thermal anomaly in breast of interest of area at least 4 times greater than the warmest area in the contralateral breast (Figure 4); (b) linear thermal anomaly in upper inner quadrant of breast of interest, not longer than 5 cm, running toward the center of the breast (absent in contralateral breast); (c) branched linear thermal anomaly in breast of interest not present in contralateral breast. Images without discernible thermal anomalies were considered negative or normal.

Difference in the number of areas with elevated temperature, as well as the maximal temperature differences between the breasts when comparing 2 thermograms together.

Color scale for interpretation of thermograms.
Nonlinear thermal anomaly area in the right breast at least 4 times greater than the warmest area in the contralateral breast.
Statistical Methods
Data were summarized as medians with interquartile ranges, or percentages. The primary endpoint was the C-statistic (area under receiver operator characteristic [ROC] curve) as measure of the ability of the thermographic findings to distinguish histologically confirmed breast cancer from noncancer, in women with abnormal breast ultrasound (BIRADS ≥4A), stratified by age (<50 years; ≥50 years). To determine this endpoint, we derived a linear predictor of malignant disease status from a logistic regression model that included the ordinal thermal anomaly score, the ordinal temperature score, and the 3 binary indicators of increased breast cancer risk, as independent variables. The linear predictor thus obtained was used to produce the ROC curve.
Secondary endpoints were sensitivity, specificity, and positive and negative predictive values, in each age group, in women with BIRADS ≥4A on ultrasound. We also estimated the false-positive rate, by age group, in women with normal breast ultrasound (BIRADS 1-2). Secondary endpoints were estimated at the Q point (closest to where sensitivity and specificity are equal) on the ROC curve. Secondary endpoints for the 2 age groups were compared with the χ2 test or normally approximated Wald test for C-statistics. False-positive rates in women with normal (BIRADS 1-2) and abnormal (BIRADS 4A, 4B, 4C, or 5) ultrasound results were also compared using the χ2 test. The analyses were performed with SAS 9.3.
Results
Characteristics of Study Participants
Of the 274 women recruited, 19 were excluded because the thermographic images were not obtained according to protocol, so 255 women were assessed: their characteristics are summarized in Table 1 according to age group. There were 135 (52%) women in <50 years group and 120 (49%) in ≥50 years group. Median age was 37 (range 25-49 years) in the younger group, and 62 (range 50-83 years) in the older group. Mammary gland size tended to be smaller in younger women. Ninety-five women in the younger group had an abnormal breast ultrasound (BIRADS ≥4A), and 40 had BIRADS 1 to 2. Eighty-seven women in older group had BIRADS ≥4A, and 33 had BIRADS 1 to 2. Based on BIRADS classification and relevant statistical and analysis data, younger women had more frequently mixed glandular structure (typically dense on a mammogram), while in older women, it appeared less dense on a mammogram. In both groups, women with abnormal breast ultrasound had similar mammary size, structure, and age to those with normal ultrasound. For women with abnormal ultrasound, the distribution of BIRADS categories was skewed toward 5 in the older group, while category 4A predominated in younger women. Women with BIRADS 1 to 2 were considered free of breast cancer and underwent no further examinations. Women with BIRADS ≥4A underwent biopsy and histological examination after thermography. Twenty-seven of 95 (28.4%) younger women with BIRADS ≥4A had breast cancer; 72 of 87 (82.8%) older women with BIRADS ≥4A had breast cancer. The high proportion of cancers in the older group is related to the predominance of BIRADS 5. The most common histological finding in younger women was fibroadenoma.
Characteristics of the 255 Women and Their Breast Lesions, According to Age.
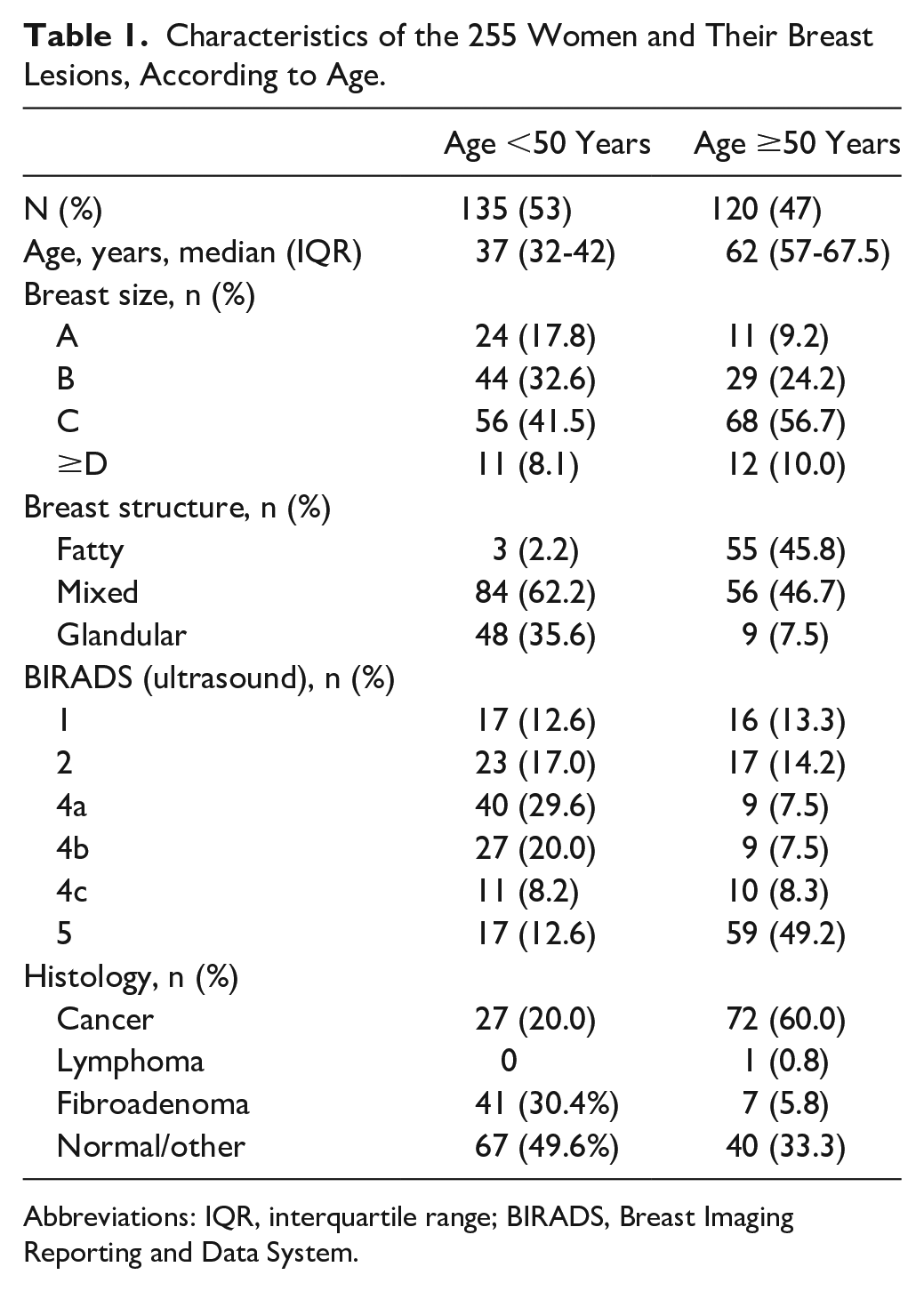
Abbreviations: IQR, interquartile range; BIRADS, Breast Imaging Reporting and Data System.
Diagnostic Performance of Thermography
The 2 scores and 3 indicators of breast cancer risk for each age group were included in a logistic regression model to assess their joint association with breast cancer risk. ROC analysis of the linear predictor (Figure 5) resulted in a C-statistic for thermography of 0.85 in the younger group and 0.75 in older group (P = .20).

Receiver operator characteristic (ROC) analysis of linear predictor derived from the thermographic imaging in women with abnormal breast ultrasound. Data stratified by age: solid line <50 years; dotted line ≥50 years. AUC, area under ROC curve is the C-statistic.
The cutoff value for abnormal thermography, derived from the Q point, was such that a positive thermographic result (indicating increased cancer risk) was associated with the presence of one or more of the following indicators: thermal anomaly score >2, temperature score >3, and presence of indictor 1 (nonlinear thermal anomaly in breast of interest of area at least 4 times greater than the warmest area in the opposite breast). Sensitivity, specificity, and predictive values based on this cutoff in the younger and older groups are shown in Table 2, where it is evident that sensitivity did not differ between the 2 groups, but specificity was lower in the older group (60% vs 87%, P = .025). Positive and negative predictive values also differed significantly between the 2 groups.
Diagnostic Performance of Thermographic Imaging in Patients With BIRADS 4 to 5 in Relation to Histologic Findings (Gold Standard).

Abbreviations: BIRADS, Breast Imaging Reporting and Data System; CI, confidence interval.
In younger women with BIRADS ≥4A, the probability of breast cancer was 28.4% (Table 1). In younger women with BIRADS ≥4 and a positive result on thermography, the probability of breast cancer increased to 71.0%. A negative thermography result in younger women with BIRADS ≥4A reduced the probability of breast cancer to 7.8%.
Forty of the younger women had a normal ultrasound (BIRADS 1-2), but 5 of these had abnormal thermographic findings, giving rise to a false-positive rate for thermography of 12.5%. This rate was closely similar to that in younger women with abnormal ultrasound (13.2%; P = .91). Thirty-three of the older women had normal ultrasound but abnormal thermography, giving rise to a false-positive rate for thermography of 36.4%, which was closely similar to the false-positive rate for thermography in older women with abnormal ultrasound (40.0%; P = .81). No adverse events associated with thermography were observed during the study.
Discussion
To the best of our knowledge, this is the first prospective study to assess contact thermography as a tool for the early diagnosis of breast cancer, using modern thermographic equipment and with the thermographic images assessed by trained radiologists blinded to the clinical and pathological characteristics of the women. We found that thermography was particularly useful for identifying malignancy in women younger than 50 years, being associated with a C-statistic of 0.85, indicating “good” ability to discriminate between cancer and noncancer, and high (87%) specificity. In older women, the C-statistic was 0.78, which, although not significantly different from that in younger women, is generally considered to indicate only satisfactory discrimination; furthermore, specificity was only 60%, significantly lower than that for younger women.
It is noteworthy that in women younger than 50 years of age, a positive thermographic result in women with BIRADS 4A on ultrasound increased the probability of breast cancer by over 2-fold. Conversely, a negative thermographic result decreased the probability of cancer more than 3-fold.
Although the literature on thermography for breast cancer is fairly extensive, 26 few published studies meet modern quality standards and most investigated infrared rather than contact thermography. 26 We only found 4 studies on contact thermography.27-30 In 1991, the study by Sforza et al 27 presented findings on 12 098 Italian women given contact thermography as part of screening. The modality had highest sensitivity (97%) in the 15- to 30-year-old group and the lowest (89%) in those older than 50 years. Specificity was also highest (95%) in women of 15 to 30 years, with lowest (50%) in women older than 50 years. These results, in contrast to our study, showed increased sensitivity and specificity in both groups, which is likely due to the inclusion criteria of screening a much younger population; 15 years old, in contrast to 25 years old in our study. Despite varying clinical characteristics, the results display similar trends, confirming that the use of contact thermography in a younger population provided more favorable results.
The 1990 study of Yokoe et al 28 reported contact thermography findings in 162 Japanese women, in 45 of whom 55 breast cancers were diagnosed. Sensitivity and specificity were 81.5% and 83.5%, respectively; however, the study did not present clinical characteristics or age ranges. These results show congruity to our study, despite a different ethnic group being screened. The sensitivity and specificity closely emulated our results; however, without knowing the population demographics, it is difficult to establish reproducible results.
In 1974, Bothmann et al 29 published, in German, results of retrospective study on 19 461 women given breast examination, mammography, and thermography: 2002 had abnormal histology and a further 500 had abnormal cytology; 86% of the women with confirmed breast cancer had abnormal thermography, so that sensitivity and specificity were 73% and 71%, respectively; however, sensitivity fell to 23% in women with lobular carcinoma in situ. The authors did not present participant characteristics or eligibility criteria. Regardless of lack of participant characteristic data, the results closely resembled our older population (older than 50 years), on a significantly larger sample size. The study also stratified patients according to the histological findings, in contrast to age, potentially having an overall effect on statistical analysis.
The 1972 article of Davison et al 30 reported findings in 105 women with palpable breast abnormalities examined by LC thermography. The breast was painted black and a LC preparation sprayed over the blackened surface. The technique had a sensitivity of 82.3%. Despite the technological differences, the technique boasted paralleled sensitivity.
Although the findings of these 4 studies are generally promising, they are difficult to compare with ours because of differences in thermographic technique and study design, including different study populations and reporting protocols.
When comparing contact thermography to other thermography modalities (ie, infrared), the information provided is similar; however, both methods have several advantages as well as limitations. In a study comparing the 2 modalities in measuring mean skin temperatures at rest, during exercise, and during recovery, it was shown that there is a poor agreement between contact and infrared devices. 31 The literature pointed out that infrared devices may not be suitable for monitoring in the presence of metabolic stress, often overestimating the results. In breast cancer, as the metabolic stress is increased, these data unequivocally translates to a potential for overdiagnosis, when compared with contacting devices. As the contacting device is directly applied to the skin, temperature perturbations related to differences in sudation and air circulation over the patient’s skin are eliminated. However, temperature is not measured in a linear manner using infrared radiation, but it is instead registered as a color map, which needs to be translated into temperature in order to perform an image analysis. The need for a controlled environment, 32 using infrared cameras, constitutes a large limitation in its widespread use. Another advantage is reducing the distance from the potential cancerous area, posing a likely increase in detection accuracy.
When comparing our results with other imaging modality, that is, sonography, mammography, or the combination of the two, the reports show a sensitivity in the vicinity of 57% to 97% for mammography alone and 49% to 100% for ultrasound. Specificity was between 36% and 97% for mammography and 29% to 100% for ultrasound. 33 The combination of the techniques showed a rise in the sensitivity between 4% and 22%, while most studies show a slight decrease in specificity (on average 0.3%). 34 By adding another modality, like thermography, we may further increase the sensitivity; however, this would need to be examined. Adding thermography or any other modality has its benefits; however, we should additionally examine false positives and negatives, cost, time needed for diagnostic examinations, and risk/benefit analysis of adding more examinations.
In addition, our pilot study aimed to determine the C-statistic for thermography using ultrasound findings. We did not compare thermography with other imaging modalities: a future study could compare these modalities head-to-head to obtain a more direct indication of the adjunctive utility of thermography. A possible study limitation is that the medical staff in the sites received training on performing thermography examination only at the beginning of the study, with a single verification after the fifth patient. More extensive training and performance monitoring would probably increase sensitivity and specificity and reduce false positives.
To conclude, the data produced by this study indicate that LC contact thermography with the Braster device is promising for the early detection of breast cancer and deserves further evaluation, especially in women younger than 50 years of age. Such women are not eligible for screening in most European countries (notwithstanding the increasing breast cancer incidence in this age group),35,36 and for whom an optimal modality for early detection has not been defined.
Footnotes
Acknowledgements
The authors thank Don Ward for help with the English.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DHZ, AK, PK, JS, AC, and PB received compensation from Braster SA for consultancy and services provided in relation to this study. The other authors have no conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.