
Abstract
Keywords
Background
Primary soft tissue sarcomas (STS) arising from male urinary and genital tract are rare tumors, accounting for only 1% to 2% of all malignancies of the genitourinary (GU) tract and 7% to 10% of all are intrascrotal tumors.1-4 The most common site of origin is paratesticular, followed by prostate/seminal vesicles, kidney, bladder, and penis, with more than 75% arising from the spermatic cord.1-4
Paratesticular sarcoma mostly have an aggressive behavior with a high incidence of local recurrence and distant dissemination. Investigations specifically regarding the clinical management of paratesticular sarcomas have been difficult because of their rarity, and treatment recommendations come from small single-institution series and are largely borrowed from the experience of retroperitoneal sarcomas. 5
The only standard therapeutic approach is complete and extensive surgery, including orchiectomy with high cord ligation and wide local resection of all surrounding soft tissues. To date, the usefulness of retroperitoneal lymphadenectomy (RPLND) and adjuvant treatments is controversial; nevertheless, selective combination of chemotherapy and radiotherapy might represent the optimal treatment in addition to surgery.1-3,6 Modalities and timing of the follow-up as well as therapeutic recommendations in case of recurrence necessarily conform to the standard guidelines for other STS. 7
This report is focused on adult primary paratesticular mesenchymal tumors with emphasis on 4 case presentations and discussion of differential diagnosis and clinical management of these rare sarcomas in our referral center.
Case Presentations
Four out of 274 patients have been identified in our sarcoma population. The mean age was 54 years (range = 45-73). The histotypes showed liposarcoma in 2 cases and leiomyosarcoma in the remaining 2 cases. In all 4 cases, the disease was localized at presentation, patients underwent complete surgery, and no adjuvant treatments were done. Three cases presented a recurrence of disease at a mean follow-up of 86 months (range = 60-106 months), more than 7 years later. Two cases were treated with a second surgery and chemotherapy and 1 case only with chemotherapy.
In this article, we report a detailed description of these cases, which could be considered of particular interest due to the rarity of site in a context of rare tumors.
Ethics Approval and Consent
Ethics approval has been obtained for this study by the local Institutional Ethical Committee of the Azienda Ospedaliero-Universitaria Policlinico Sant’ Orsola-Malpighi (Approval Number 164/2017/O/Oss; June 16, 2017), and no further written informed consent was required for the retrospective part of the study. Written informed consent was obtained from the patients for publication of this case report and any accompanying images.
Case Descriptions
Case 1
A 45-year-old patient was referred to our institution in March 2017 after incomplete surgical excision of a solid neoformation of the left hemiscrotum. The histological findings of the surgical specimen concluded to high-grade leiomyosarcoma, negative IIC for S-100 and CD-34, positive for actin, desmin, and caldesmon (Figure 1A and B).

(A) Hematoxylin and eosin 20×. Leiomyosarcoma composed of fascicle of eosinophilic spindle cells with moderate to severe nuclear atypia and mitotic activity. (B) Tumors cells show diffuse expression of desmin.
The patient reported the presence of a palpable tumefaction in the scrotum since 20 years, which had gradually increased over time. Considering the incomplete excision and grading, a multidisciplinary team meeting with urologists, radiotherapists, and oncologists opted for an extended resection surgery; thus, the patient underwent left radical orchiectomy and excision of scrotal skin and dartos.
No adjuvant chemotherapy or radiotherapy was indicated, and the patient started a follow-up program.
At last follow-up visit, 18 months after surgery, the patient is in good clinical condition and with no evidence of disease relapse at computed tomography (CT) scan.
Case 2
In February 2010, a 53-year-old patient had a low-grade liposarcoma of the left spermatic cord removed. No adjuvant therapy was performed, and then, the patient underwent regular follow-up. Seven years later, he reported a 2-month history of abdominal pain and increase in abdominal circumference. A CT scan demonstrated an irregular voluminous mass of 13.7 × 13 × 12 cm in the left iliac fossa, with dislocation of the bladder and compressive effect on the left iliac vein and an additional solid neoformation over the previous one, in contact with the inferior pole of the ipsilateral kidney (Figure 2A, B, and C).

Contrast-enhanced computed tomography (CT) scan, axial view, shows voluminous mass entirely occupying the abdominal cavity (A) and dislocating the bladder (B). Additional solid neoformation in contact with the inferior pole of the ipsilateral kidney (C).
The patient underwent a CT-guided biopsy of the principal mass with a histological diagnosis of dedifferentiated liposarcoma.
In November 2017, the patient developed abdominal pain due to growth of masses. An “en bloc” surgical removal of the voluminous mass with left nephroureterectomy and hemicolectomy was performed. A pathological examination showed minimal disease residue evaluated as vascular R1 (Figure 3). The final histological evaluation confirmed a dedifferentiated liposarcoma, grade 3 with amplification of MDM2 (Figure 4A, B, and C).

Surgical removal of the voluminous mass en bloc with left nephroureterectomy and hemicolectomy.
(A) Hematoxylin and eosin 20×. High-grade dedifferentiated liposarcoma. Dedifferentiated areas with increased cellularity and pleomorphism overlap with undifferentiated pleomorphic sarcoma. (B) MDM2 immunostaining: diffuse immunostaining in high-grade dedifferentiated areas. (C) Fluorescent in situ hybridization (FISH): dedifferentiated liposarcoma with high MDM2 amplification (MDM2—orange signals and CEP12—green signals; DAPI, ×100).
Given the aggressiveness of the disease and the positive margins, a protocol of adjuvant chemotherapy with epirubicin and ifosfamide as the standard in the adjuvant setting for liposarcoma of the retroperitoneum, trunk, and extremities was planned. However, a postsurgery CT scan showed persistence of the disease in pelvis and abdomen. Due to a significant volume of residual disease, we decided to start a first-line chemotherapy with doxorubicin plus olaratumab. An early partial response was observed after 2 months of treatment. We decided to continue with olaratumab maintenance treatment, which is still ongoing.
Case 3
In January 2009, a 46-year-old man underwent left orchiectomy and hernioplasty after the occasional finding of a paratesticular mass, during investigations conducted for an inguinal hernia. Due to clinically suspected inguinal lymph nodes, a lymphadenectomy was performed. Histological examination revealed a well-differentiated sclerosing liposarcoma of the spermatic cord (diameter = 9 × 7.5 cm) with lipoma-like areas. Testis and epididymis were free from neoplasia, whereas tumor cells were present on the surgical margin of the spermatic cord.
Considering in particular the low grade of differentiation, no adjuvant treatments were performed and a follow-up program was planned. After 9 years, a CT scan revealed a retroperitoneal solid tissue mass in the left paraortal site (maximum axial diameter about 5 × 3 cm, with an extension of about 7 cm) suspected of being a gastrointestinal stromal tumor and a peritoneal nodulation of about 2 × 2 mm with a hypodense central area. A CT-guided biopsy of the peritoneal lesion was conducted, and it was concluded to represent metastasis from dedifferentiated liposarcoma.
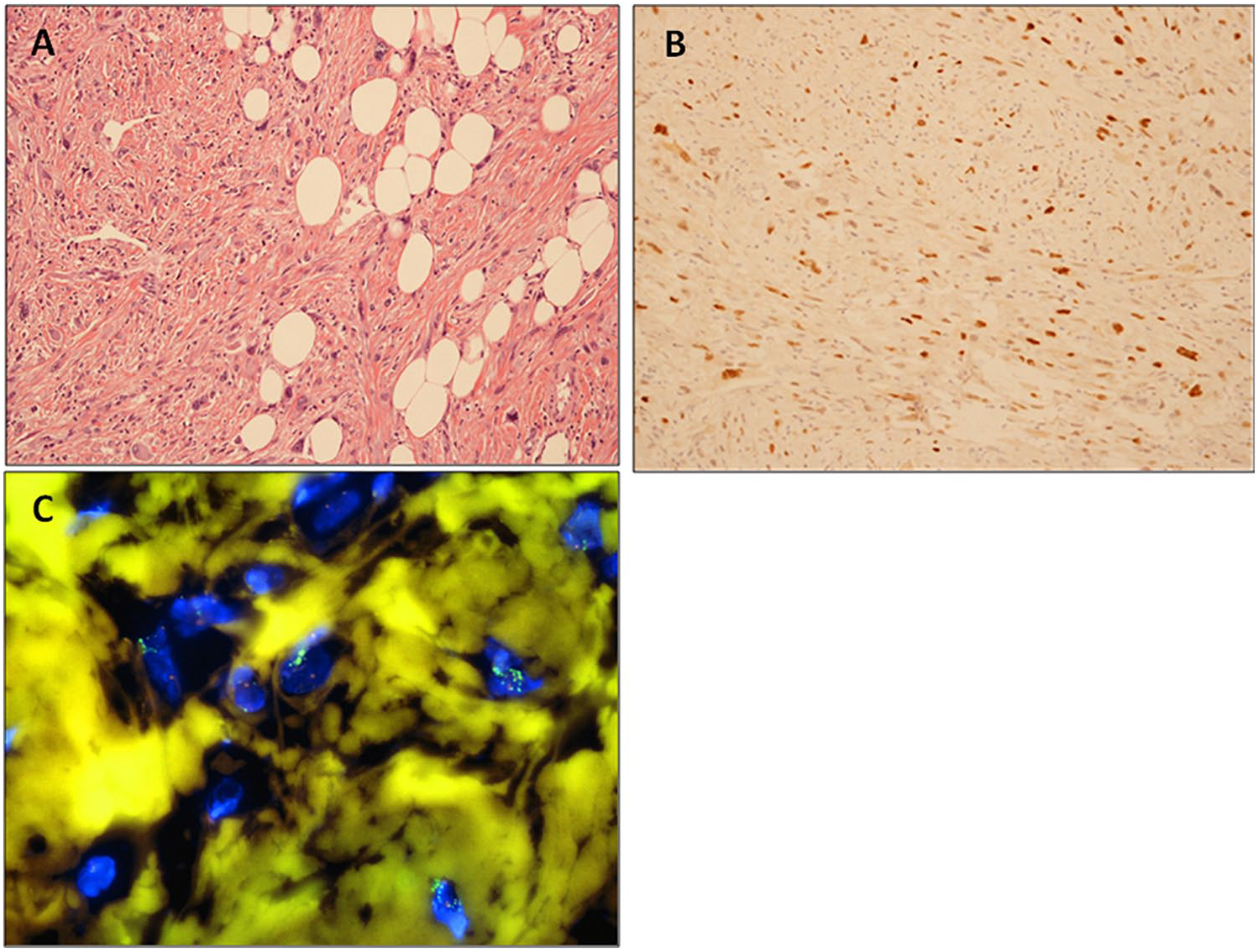
Due to slow progression of disease and young age of the patient, a surgical resection of the 2 masses (the biggest one and the peritoneal nodule) was planned. However, surgical exploration showed widespread peritoneal disease also involving abdominal aorta, thus resulting in a debulking-only intervention. The final histological evaluation confirmed a dedifferentiated liposarcoma, grade 2 (Figure 5A and B), positive for amplification of MDM2.

(A) Hematoxylin and eosin 20×. Low-grade dedifferentiated liposarcoma. Non-lipogenic areas exhibit low-grade spindle cell morphologic features. (B) MDM2 immunostaining: MDM2 is overexpressed but in few tumor cells in low-grade dedifferentiated liposarcoma.
Thus, the patient started a first-line chemotherapy with doxorubicin plus olaratumab. The CT assessment during and at completion of 6 cycles showed disease stability, and the patient is, thus, currently continuing to receive monotherapy with olaratumab as a maintenance program.
Case 4
In February 2017, a 73-year-old man was admitted to our institute after failed chemotherapy attempt performed in another center for a pulmonary recurrence of leiomyosarcoma of the spermatic cord.
The patient had a history of orchiectomy performed 3 years before for a dedifferentiated leiomyosarcoma of the spermatic cord, grade 3. Tumor necrosis was superior to 15% and surgical margins free from neoplasia. Atrophic testicular parenchyma was disease-free. No adjuvant treatments were performed after surgery considering extension of the intervention and the age and comorbidities of the patient. Three years after surgery, multiple bilateral lung metastases were detected, and a first-line treatment with continuous infusion of ifosfamide was performed for 4 cycles with progressive disease as best response. It was possible to expect poor response of disease to this scheme, considering the specific sarcoma histotype. Lung metastases further grew, and the patient decided to consult us for a second opinion. Given the patient’s age and the presence of cardiologic contraindications for the use of anthracycline, we decided for a second-line therapy with trabectedin. A CT scan performed after 4 cycles showed partial response to treatment, and the patient currently has good clinical performance status and is still continuing to receive the same therapy.
Discussion and Conclusions
Primary paratesticular tumors are rare, only accounting for 7% to 10% of all intrascrotal tumors. They predominantly originate from the spermatic cord. Most paratesticular tumors are benign, primarily lipomas, but also hemangiomas, lymphangiomas, and leiomyomas.
Among malignant tumors, the most common reported histotypes are liposarcoma and leiomyosarcoma, followed by rhabdomyosarcoma, malignant fibrous histiocytomas (MFH), fibrosarcoma, and angiosarcoma. 8 Liposarcoma, leiomyosarcoma, and MFH occur predominantly in old age, with a peak incidence reported in the 50 to 70 year olds, while rhabdomyosarcoma is the most common malignant mesenchymal tumor in children and young adults.9,10
Sarcomas of the paratesticular region most often arise from the spermatic cord (which originates from the mesoderm layer of the embryo), the testicular tunica, the epididymis, the external inguinal ring, or from the soft tissue (dartos muscle) of the scrotal wall. 8 Depending on whether they originate above or below the external inguinal ring, they can grow as inguinal masses or scrotal masses, the latter clearly distinct from the testis.
Sarcomas of the spermatic cord and the epididymis drain into the retroperitoneal lymph nodes, while the scrotal sarcoma drains into the inguinal, external, and internal iliac nodes.
Clinical presentation is usually nonspecific, mainly characterized by a sense of weight or compression due to mass effect or alternatively completely asymptomatic, except MFH, which can give rise to very painful masses due to the inflammatory characteristics of this histotype. 5
The importance of differential diagnosis is crucial, and the hypothesis of sarcoma should be always kept in mind in case of a large solid irregular or necrotic mass in the inguinal or scrotal region. Indeed, there are several conditions that have the same clinical presentation of paratesticular sarcoma, including inguinal hernia, hydrocele, spermatocele, cyst, and epididymitis, whose correct diagnosis is made even more difficult by the complex anatomy of the scrotum.
Ultrasonography is the primary step in testicular imaging workup, with a sensitivity of 95% to 100% in distinguishing intratesticular from extratesticular lesions and a remarkable accuracy in the diagnosis of cysts, hydrocele, and epididymitis. However, it often proves to be not conclusive to establish the malignancy of a lesion; therefore, CT scan and magnetic resonance imaging may be helpful in refining tumor location, tissue, and morphologic features.
With suspicion of a paratesticular malignancy, biopsy for histological characterization is mandatory.
The relative paucity of cases reported in literature makes it difficult to document the natural history of such tumors, and information used to guide treatment is based on case series and literature reviews. The first case of a paratesticular tumor ever reported was a sarcoma, described in 1845 by Hinman and Gibson. 11 Currently, no clear and specific consensus exists regarding proper treatment.
Surgery remains the gold standard for localized disease and chemotherapy for metastatic and/or unresectable disease. Thus, the standard clinical practice guidelines for sarcoma should be followed, taking into account the literature recommendations by histotype. 7
In our experience, we observed 4 cases of paratesticular sarcoma, 2 cases of liposarcoma and 2 cases of leiomyosarcoma. The clinical behavior was heterogeneous, ranging from indolent to aggressive course. In the 3 patients who experienced relapse, disease recurred after many years and was characterized by a transformation of the histology toward more aggressive and dedifferentiated forms, with regard to primary tumor. In 2 cases, the relapse was in the abdomen, and in 1 case, it was in the lung, as expected considering primary histotypes. In fact, leiomyosarcoma usually present distant metastases, and liposarcomas mainly relapse locally.
In the first case, a slow-growing paratesticular leiomyosarcoma, progressively grown over a period of 15 to 20 years, is described. Acceleration of tumor growth in the past period led the patient to consult, resulting in surgery judged incomplete.
Our clinical resolution was to do extended surgery with removal of the testicle and ipsilateral spermatic cord, the scrotal dermal layer, and the dartos. Due to the absence of residual disease in the removed tissues, we resolved not to carry out further treatments. One year and a half after surgery, the patient is still disease-free.
In the second case, we have witnessed a massive abdominal relapse of paratesticular liposarcoma, extremely aggressive, rapidly grown to enormous size, reached in a few weeks. The patient was asymptomatic. Surgery was performed due to high risk of short-term complications from mass effect (ie, abdominal occlusion, obstruction of ureters). However, in case of highly aggressive histotype and massive recurrence, surgery alone should not be considered the standard option but must be integrated with systemic chemotherapy and/or radiotherapy.
In the third case, there was a delayed and indolent abdominal relapse, diagnosed during annual follow-up of the paratesticular liposarcoma that was removed almost 9 years earlier. In this case, in contrast to the others, surgical margins of the primary tumor were positive.
Similarly, in case 4, the relapse occurred after a long period of 5 years, and the patient was asymptomatic. All 3 patients received chemotherapy at recurrence.
Given the encouraging data reported in literature, an anthracycline and olaratumab-based chemotherapy was chosen in 2 cases. Olaratumab is a fully human immunoglobulin G subclass 1 monoclonal antibody that inhibits platelet-derived growth factor receptor-α. The antitumor activity of olaratumab has been tested in vitro and in vivo, and inhibition of tumor growth has been observed in cancer cell lines, including glioblastoma and leiomyosarcoma cells. This drug was the first-in-class antibody to be approved by regulatory authorities for the treatment of advanced STS in combination with doxorubicin, based on the results of the Phase Ib/II trial by Tap et al. 12 The median progression-free survival in Phase II was improved for patients treated with olaratumab plus doxorubicin compared with those treated with doxorubicin monotherapy (6.6 vs 4.1 months, P = .0615). Moreover, final analysis of overall survival (OS) showed a very significant advantage in median OS (26.5 months with olaratumab plus doxorubicin vs 14.7 months with doxorubicin alone, P = .0003), with a gain of 11.8 months. Unfortunately, the recently reported preliminary results of ANNOUNCE, 13 the phase III study of olaratumab in combination with doxorubicin in patients with advanced or metastatic STS, did not confirm the previous reported clinical benefit of olaratumab in combination with doxorubicin as compared with doxorubicin alone, a standard-of-care treatment. Olaratumab was well tolerated, no new safety signals were identified, and the safety profile was comparable between treatment arms, but the study did not meet the primary endpoints of OS in the full study population or in the leiomyosarcoma subpopulation. The effort now is to better understand the different results between the 2 trials, determine the appropriate next steps for olaratumab development, and eventually test new combination regimens.
Today, we cannot recommend olaratumab in patients with paratesticular sarcoma until new indications or data become available.
In one case, we highlight the possibility of using trabectedin in metastatic paratesticular leiomyosarcoma, treatment that was well tolerated despite the patient’s advanced age and that achieved a partial response. Trabectedin is a marine compound, characterized by a peculiar mechanism of action. 14 It is not just a DNA binder but also it affects key processes regulating cell cycle growth, death, and progression, hitting both tumor cells and tumor microenvironment. Trabectedin has shown its efficacy in pretreated patients, especially affected by liposarcoma and leiomyosarcoma, in large and randomized phase II and III trials that have led to its approval in several countries worldwide. The benefit of the antitumor activity of trabectedin was observed in all subgroups of patients analyzed. Moreover, due to its good safety profile, mainly characterized by transient, noncumulative, and easy manageable toxicities, trabectedin represents a treatment choice accessible also for elderly patients and appropriate for long-lasting period. 15
A wide variety of systemic agents is currently available for patients with advanced disease. However, a globally accepted or favorite regimen and standard algorithm of treatment does not exist. Current options include high-dose ifosfamide, dacarbazine, gemcitabine alone, or in combination with docetaxel or dacarbazine. 7
More recently, other 2 innovative therapies have been introduced and they are currently part of the therapeutic armamentarium, positively affecting disease control and patients’ quality of life: the effective oral inhibitor of the vascular endothelial growth factor (VEGF)–VEGF receptor pathway pazopanib, and the new microtubule dynamics inhibitor eribulin for nonadipocytic and adipocytic soft tissue sarcoma, respectively.16,17
With regard to reported experience and data on primary paratesticular malignancies, currently, the large single-institution–based publications include the following:
362 cases of primary spermatic cord tumors, the largest cohort studied to date, prospectively collected in the Surveillance, Epidemiology, and End Results database from 1973 to 2007 8
57 cases of paratesticular sarcoma from the 25-year Memorial Sloan Kettering Cancer Center experience (1997-2003) 6
56 cases of paratesticular sarcoma from a larger retrospective analysis of 188 patients affected by GU sarcoma treated at the West China Hospital from 1985 to 2010 18
Rodríguez et al 8 utilized a large population-based cancer registry to characterize demographics, pathology, treatment characteristics, and outcomes of spermatic cord tumors: 362 cases were collected, the most common histotype being liposarcoma (168 cases), followed by leiomyosarcoma (71 cases), histiocytoma (47 cases), rhabdomyosarcoma (31 cases), and fibrosarcoma (8 cases). The median OS was 11.8 years for the entire cohort. Survival differed by histologic type, liposarcoma having the best disease-specific survival at 5 and 10 years (95% and 90%, respectively), while leiomyosarcoma and histiocytoma histologic subtypes were observed to be the most aggressive. Multivariate analysis revealed that tumor grade, stage, histologic type, and lymph node involvement were independently predictive of prognosis.
In the Sloan Kettering experience, 6 the primary tumor site was paratesticular in 57 cases among 131 analyzed. The most common histological subtypes were liposarcoma (25 cases), leiomyosarcoma (11 cases), and rhabdomyosarcoma (11 cases) in the paratesticular group. In particular, 68% of patients presented high-grade paratesticular sarcoma, with 16% showing metastatic disease at diagnosis. The median OS between all groups (paratesticular, bladder, kidney, prostate) was 7.6 years, with a 5-year survival rate in the paratesticular group of 54%. In patients who underwent complete surgical resection, the 5-year survival rate was 65%. On univariate analysis, unfavorable prognostic factors for disease-specific survival were metastasis at presentation, high tumor grade, large tumor size, incomplete surgical resection, and positive surgical margin. On multivariate analysis, only 2 variables remained significant predictors of disease-specific survival, including tumor size (hazard ratio [HR] = 1.1, 95% confidence interval [CI] = 1.02-1.17) and absence of metastasis at diagnosis (HR = 4.9, 95% CI = 1.4-17.2). In this retrospective study, the role of neoadjuvant and adjuvant treatments was not analyzed.
In the West China Hospital retrospective analysis, 18 a total of 188 patients affected by GU sarcoma were included, with 56 cases of paratesticular sarcoma (22 liposarcoma, 10 leiomyosarcoma, 18 rhabdomyosarcoma, and 6 other sarcoma), of which 78.6% were high grade and 32% metastatic at entry. OS at 1, 3, and 5 years was 91.3%, 64.0%, and 47.7%, respectively, among all patients, and estimated median OS was 55 months. The Kaplan-Meier curve of OS stratified by primary tumor site showed longer OS in the prostate and bladder groups and worse data for the paratesticular group. 18 Between all subgroups, with univariate analyses, liposarcoma histotype, high histological grade, metastatic disease at diagnosis, a lack of surgical resection, positive surgical margin, and the application of radiotherapy were predictive of unfavorable OS. Multivariate analyses showed that patients younger than 50 years, high histological grade, a lack of surgical resection, and chemotherapy were the independent prognostic predictors of poor OS. A large proportion of patients who underwent surgical resection developed local recurrence, in particular, 64.7% of cases, and median OS after recurrence was 42 months.
The use of a population-based cancer registry of the United States reported by Rodríguez et al 8 has allowed to obtain fundamental epidemiological information regarding these rare tumors. In particular, it was possible to extrapolate data on incidence rate, age at diagnosis, race, and risk and prognostic factors. However, few data about clinical management of these patients have been provided by this analysis. In particular, data about patients, the radiation dosage, delivery methodology employed, and the type of drugs administered are still missing. Therefore, only limited clinical conclusions and interpretations regarding treatment outcomes can be drawn from this analysis.
In all reported series, complete surgical resection has a strong impact on patients’ outcome, achieving prolonged disease-specific survival. Radical inguinal orchiectomy and resection of the tumor with large negative margins provides ideally the best clinical outcomes. In contrast, the role of prophylactic lymph node dissection remains unclear. Proponents of lymphadenectomy indicate that the metastatic potential to regional lymphatics may be as high as 29%. 19 However, the true incidence of nodal metastasis has never actually been documented, and the general consensus has been that the most common histotypes, liposarcoma and leiomyosarcoma, rarely involve locoregional lymph nodes, as they frequently recur locally or spread by blood extension. 7 To assess the benefit of extensive RPLND, Banowsky and Shultz 19 reviewed 101 cases of spermatic cord sarcoma, 29 of which were subjected to RPLND. Of these, 17 patients had isolated lymphatic dissemination. Lymphadenectomy did not demonstrate impact on survival. In all the largest case series, it is not specified whether surgery included lymphadenectomy or not.
Moreover, literature concerning benefit of adjuvant therapy after complete surgery is inconclusive because of the small numbers. By mutating already established concepts related to retroperitoneal sarcomas, adjuvant radiotherapy should be considered in case of positive margins, and chemotherapy in case of high risk of distant metastasis (large tumor size, high grade, high proliferative index, and presence of necrosis).
What is more, the role of radiotherapy/chemotherapy is still controversial in terms of impact on survival, although negative data may be affected by patients’ selection bias.
Some authors recommend adjuvant radiotherapy for high-grade testicular sarcoma or for patients with high risk of local recurrence.5,20,21
In their series of 21 patients, Catton and colleagues 22 observed a 5-year disease-free survival rate of 56% in the case of surgery alone and 100% when surgery was followed by adjuvant radiotherapy (P < .01). Fagundes and colleagues 5 analyzed 18 patients from the Massachusetts General Hospital, half of whom received adjuvant radiotherapy coupled with orchiectomy, while the remaining half received surgery alone. They reported no local failures in patients receiving adjuvant locoregional radiotherapy compared with a 56% recurrence risk (5 out of the 9 patients) in those treated with orchiectomy alone. 5 These findings suggest that adjuvant radiation may control local microscopic disease and reduce the risk of locoregional relapse.
In the retrospective analysis of data of the West China Hospital, the 43 patients managed with a combination of surgical resection plus radiotherapy plus chemotherapy had a mean survival of 55 months versus 76 months for the 67 patients treated with surgery plus chemotherapy, 39 months for the 8 patients treated with surgery plus radiotherapy, 69 months for the 29 patients treated with surgery alone, and 13 months for the 25 patients treated without surgery. The use of radiotherapy appeared being associated with an unfavorable outcome, but authors concluded that it might have resulted from a selection bias.
However, regardless of adjuvant therapy, our cases, in line with data reported in literature, suggest that long-term follow-up is recommended given the high recurrence rates, often delayed, of paratesticular sarcomas.
In conclusion, due to low prevalence, prospective trials are not feasible for these tumors; thus, principles of therapy are based on case series and retrospective studies. In all reported cases, it is clear that complete surgical excision is the most important therapeutic approach, while benefits of adjuvant radiotherapy/chemotherapy and/or retroperitoneal lymph node dissection are still under investigation.
Our case series illustrates the entire clinical path of these patients from diagnosis to follow-up, through surgery and the possible use of adjuvant treatments. Moreover, in cases of disease recurrence, therapies were always chosen after multidisciplinary evaluation and consisted of second surgery and/or chemotherapeutic treatment.
Our small series confirms that recurrence is the Achilles heel of most paratesticular sarcomas, which can occur several years after initial treatment; long-term follow-up is, therefore, strongly recommended.
It is important to collect and report case studies/single-center experiences, and in cases of disease recurrence, the therapeutic measures adopted after multidisciplinary evaluation, consisting of second surgery and/or chemotherapy treatment using innovative or investigational drugs. In fact, these can represent complete and useful examples for the scientific community of clinical management of patients affected by this rare and aggressive neoplasm.
Footnotes
Authors’ Note
Annalisa Astolfi is also affiliated with Department of Biomedical and Specialty Surgical Sciences, University of Ferrara, Ferrara, Italy.
Author Contributions
LG and MS described and interpreted the patient data and were the major contributors in writing the manuscript. MDG, MR, MC, VT, MC, and AF performed surgery and have been involved in drafting the manuscript. VDS, FB, and FN performed imaging and have been involved in drafting the manuscript. MGP, EC, and MF performed the histological and pathologic examination of the surgical tissue and have been involved in drafting figures. AA, VI, and MN have been involved in drafting and revising the manuscript. MAP was the major contributor in concept and designed and revised the manuscript. All authors read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.