
Abstract
Keywords
Introduction
Colorectal cancer (CRC) is one of the most commonly diagnosed types of cancer worldwide; it is the third most common cancer and has the second highest cancer mortality rate.1,2 About half of CRC patients suffer from liver metastasis either at the time of diagnosis (15% to 20%) or later during the course of the disease (25%).3,4 As surgical resection of colorectal liver metastases (CRLMs) provides the greatest chance for cure and long-term survival, it is the treatment of choice for resectable CRLMs. Only approximately 20% of patients are candidates for liver resection; however, it is reported that between 12% and 33% of patients with “initially unresectable” hepatic metastases have an objective response to conversion therapy sufficient to permit a subsequent complete resection. 5 Long-term survival after surgery for CRLMs has dramatically improved: 5-year overall survival (OS) rates doubled from approximately 30% in the 1980s and 1990s to almost 60% in the last 2 decades. 5 Although there has also been notable development in chemotherapy for CRC patients, stage IV disease is usually incurable. 6 In 2 recent studies, patients with metastatic CRC had a 5-year OS of 14%, and the ratio of patients with liver metastases treated with resection was improved up to 50%.7,8 The best remedy for all patients with metastatic CRC is to improve their quality of life through systemic treatment. As such, there is a great need to develop new therapeutic strategies for metastatic CRC patients.9,10
Chinese herbal medicine (CHM), an important part of complementary and alternative medicine, has been developed over thousands of years with a unique system of theories, diagnostics, and therapies. It is now widely accepted and employed for the integrative management of CRC and other malignancies in China.11-15 Moreover, evidence-based investigations have revealed that CHM plays a significant role in tumorigenesis, reduction of toxicity, increased treatment effect, and decreased risk for CRC recurrence and metastasis.16-18 Furthermore, a prospective multicenter study 19 of 312 patients who had received comprehensive conventional treatments examined the relationship between CHM therapy and survival outcomes. The investigation revealed that long-term CHM therapy conferred prolonged survival times in CRC patients at stages II and III. However, existing studies have focused only on the benefits of CHM for CRC patients at early stages or on the influence of integrative therapy (a combination of CHM and conventional therapy) on cancer. To address this gap, the objective of this study is to explore not only whether CHM alone or adjuvant to conventional therapy can prolong the survival of CRLM patients, but also to examine the association between the duration of CHM therapy and OS.
Methods
Study Design and Participants
We conducted a retrospective cohort study from January 2008 to December 2017 at the First Affiliated Hospital of Guangzhou University of Chinese Medicine in Guangzhou, China.
The inclusion criteria were the following: (1) 18 years of age or older, (2) diagnosed with CRLM without evidence of other distant metastases, (3) with histological diagnosis of CRC, and (4) radiological evidence of hepatic metastases on either contrast-enhanced computed tomography or contrast-enhanced magnetic resonance imaging. The exclusion criteria were the following: (1) evidence of other types of malignancies or serious nonmalignant diseases, (2) the survival period was less than 6 months, (3) Karnofsky Performance Status (KPS) scores of lower than 50, and (4) incomplete follow-up data. The index date was the initial diagnosis of CRC patients with liver-limited metastases between January 2008 and December 2017. All enrolled patients began CHM therapy within 48 hours of being hospitalized, and appropriate conventional therapies were determined by clinicians after discussion with the patient.
Ethics
This study was approved by the ethics committee of the First Affiliated Hospital of Guangzhou University of Chinese Medicine, and the need for informed consent was waived (Approval No.: ZYYECK [2018] 135).
Exposure: CHM Therapy Use
We divided patients into high- or low-exposure groups according to the duration of their CHM therapy.19,20 High exposure to CHM therapy was defined as at least 6 months; shorter periods were considered low exposure. A patient was considered to be receiving CHM therapy when taking a syndrome-differentiation herbal formula prescribed by a CHM physician.
According to the therapeutic principles of CHM and our long-term clinical experience, physicians prescribe different formulas depending on tongue and pulse diagnoses and on individualized traditional Chinese medicine syndromes, which are formed by a single patient’s symptoms. In our study, CHM was based on general traditional Chinese medicine principles, such as nourishing spleen qi, soothing liver qi, removing blood stasis, and detoxification. The key formula and modifications are shown in Table 1.
Chinese Herbal Medicine Treatment Protocol for Patients Diagnosed With Colorectal Liver Metastases.

Outcome Measure
The primary outcome measure was OS. Data were acquired via the hospital’s electronic medical record system or telephone follow-up. Assessors were blinded to patient information to reduce assessment bias. All data were updated to December 30, 2018. When a specific date of death could not be retrieved, the middle day of the month in which the patient died was used. Survival time was calculated by day.
Covariates
We collected information on covariates adjusted for confounding factors or used for stratification during the baseline period. This included age, sex, the anatomical location of the tumor, tumor differentiation, number of liver metastases, KPS score, carcinoembryonic antigen (CEA) levels, types of metastasis, and whether the patient had received primary surgery, targeted therapy, radiotherapy, local therapy for liver metastases, or chemotherapy. The chemotherapy and targeted-therapy regimens used for the enrolled patients included the following: oxaliplatin + leucovorin + fluorouracil (FOLFOX), oxaliplatin + capecitabine (CAPEOX), irinotecan + leucovorin + fluorouracil (FOLFIRI), irinotecan + leucovorin + fluorouracil + oxaliplatin (FOLFOXIRI), capecitabine, tegafur + gimeracil + oteracil (TS-1), oxaliplatin, bevacizumab, and cetuximab. The clinical dose was adjusted according to side effects such as bone-marrow suppression. Details on the chemotherapy and targeted drugs, as well as the dosages used, are provided in Supplementary Material 1 (available online).
Statistical Methods
Baseline differences between high- and low-exposure groups were compared. For continuous data, the variables were represented as the mean ± standard deviation. Categorical variables were expressed as percentages. One-way analysis of variance, Kruskal-Wallis H test, and χ2 test were employed to determine any statistical differences between the 2 groups, and appropriate statistical tests were selected according to distribution and data type.
To compare differences in OS between the high- and low-exposure groups, we used the Kaplan-Meier estimator to demonstrate time-to-event data; the log-rank test was used to compare differences between the survival curves. We then performed univariate and multivariate Cox proportional-hazards regression to adjust for covariates. Based on the STROBE recommendations, we compared both unadjusted and fully adjusted analyses. Covariance adjustment depended on whether the matched hazard ratio (HR) was increased by at least 10%. 21 We adjusted age in a smooth model for sensitivity analysis. In previous studies, most authors treated the relationship between age and death as a linear association; however, in clinical practice, we have found the association between age and mortality to be nonlinear. As such, in model 2, we use generalized additive models to adjust for age (smooth). The results showed no difference between models 1 and 2.
Because KPS and chemotherapy statuses were unbalanced in the 2 groups, we performed an exploratory subgroup analysis stratified by the indicated factors.
Analyses were performed using R (www.R-project.org; The R Foundation) and Empower States (http://www.empowerstates.com; X & Y Solutions, Inc, Boston, MA) statistical software packages. All tests were 2-sided, with statistical significance set at .05. As the subgroup analysis was exploratory, we did not adjust P values for multiple comparisons.
Results
Participant Characteristics
We retrieved data regarding 1367 patients with advanced CRC between January 2008 and December 2017 through an electronic medical-record search. We screened 238 cases of CRC with liver-limited metastasis; 47 cases did not meet the inclusion criteria. Finally, 191 patients were included in the analysis (Figure 1). The high-exposure group included 126 patients, and the low-exposure group included 65 patients.

Survival.
Demographic and clinical patient characteristics are shown in Table 2. The mean age was 59.46 ± 12.47 years (range = 24-83 years), and 70 (36.65%) were female. Among the participants, 141 (80.11%) were diagnosed with LCRC (left-sided colorectal cancer), while 35 (19.89%) were diagnosed with RCC (right-sided colon cancer); 126 (68.48%) cases involved more than 2 liver metastasis niduses, and 58 (31.52%) involved less than 2 liver metastasis niduses. There were 142 (75.53%) patients who received primary surgery, while 46 (24.47%) did not. A total of 59 (31.22%) patients underwent targeted therapy. The baseline data were statistically balanced except for chemotherapy and KPS score. There were more patients who received chemotherapy (97.62% vs 82.81%) and better KPS scores in the high-exposure group.
Baseline Characteristics of all Participants (n = 191).

Abbreviations: KPS, Karnofsky Performance Status; T, tumor (topography); N, lymph node; LCRC, left-sided colorectal cancer; RCC, right-sided colon cancer; CEA, carcinoembryonic antigen.
Of the 191 included patients, 166 (86.91%) were deceased, 13 (6.81%) were alive, and 12 (6.28%) were lost to follow-up. Data regarding the OS of 141 (73.82%) patients were collected via the hospital medical-record system, and the data of 50 (26.18 %) patients were collected by telephone. Due to unavailability of the actual death dates, 41 patients (21.47%) were assigned a date of death (the middle day of the month in which they died).
Prognostic Risk Factors
Univariate analysis revealed that CHM therapy, tumor stage, tumor differentiation, tumor location, CEA levels, primary surgery, metastasis surgery, chemotherapy, targeted therapy, and local treatment were related to prognosis. Among these influences, the HRs of CHM therapy, primary surgery, metastasis surgery, chemotherapy, targeted therapy, and local treatment were <1 (protective factors). The HRs of the tumor stage, CEA levels, tumor location, and differentiation were >1 (hazard factors; Table 3).
Univariate Analysis for Variables of Overall Survival.

Abbreviations: T, tumor (topography); N, lymph node; LCRC, left-sided colorectal cancer; RCC, right-sided colon cancer; KPS: Karnofsky Performance Status; CEA, carcinoembryonic antigen.
CHM Therapy and Overall Survival
The predefined primary end point in our analysis was OS. The median OS was 26.13 months in the high-exposure group and 14.67 months in the low-exposure group (Figure 2). The 1-, 3-, and 5-year survival rates in the low-exposure group were 31.35%, 3.60%, and 0.90%, respectively, while those of the high-exposure group were 51.18%, 22.05%, and 8.66%, respectively. In particular, the high-exposure group displayed a notably decreased death risk (HR = 0.47; 95% confidence interval [CI] = 0.34-0.65; P < .001). Moreover, the trend remained unchanged after introducing the Cox proportional hazards regression model (HR = 0.444; 95% CI = 0.213-0.926; P = .030; Table 4).

Study flow diagram.
Multivariate Analysis for Variables of Overall Survivala,b.

Data presented as hazard ratio (95% confidence interval); P.
Outcome measure: Death.
Exposure variables: Amount of time taking Chinese herbal medicine (months); Two groups: >6 months or <6 months of treatment.
Adjusted model 1 adjusted for sex, age, type, tumor location, tumor differentiation, tumor stage, lymph node stage, carcinoembryonic antigen, Karnofsky Performance Status, primary surgery, metastasis surgery, chemotherapy, number of liver metastases, local treatment, and targeted therapy.
Adjusted model 2 adjusted for sex, age (smooth), type, tumor location, tumor differentiation, tumor stage, lymph node stage, carcinoembryonic antigen, Karnofsky Performance Status, primary surgery, metastasis surgery, chemotherapy, number of liver metastases, local treatment, and targeted therapy.
P < .05; ***P < .001.
Stratified Analyses
The median survival and HR of mortality for each subgroup are shown in Figure 3. After adjusting for demographic and clinical variables, higher exposure to CHM slightly reduced the risk of death in the subgroup of patients without local treatment, targeted therapy, or surgery (adjusted HR > 0.444, P < .05). This indicates that patients who have already accepted local therapy, targeted therapy, or surgery could receive a significantly reduced risk of death from higher CHM exposure (adjusted HR < 0.444, P < .05). In addition, higher CHM exposure may significantly reduce the risk of death in the subgroup of patients from 55 to 65 years of age with metachronous or moderately differentiated tumors, a KPS > 80, or more than 2 liver metastasis niduses (adjusted HR < 0.444, P < .05). High CHM exposure reduced the risk of death in the subgroup of patients with chemotherapy (HR = 0.517) and in the LCRC subgroup (HR = 0.458, P < .05). In the subgroup of patients with a KPS > 80, those with high CHM exposure had the most significantly reduced risk of death (HR = 0.203, P < .001).
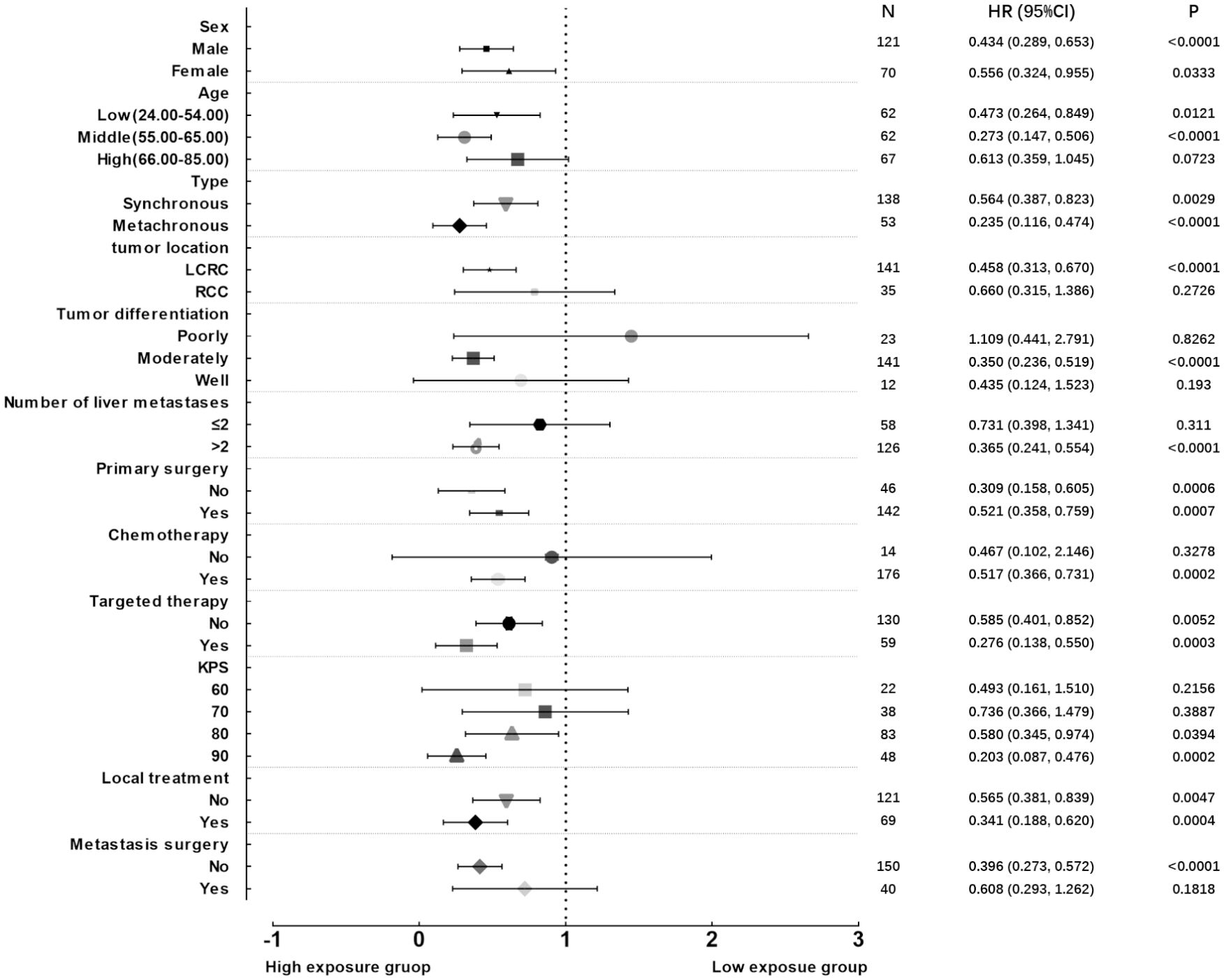
Forest plots.
Discussion
In this retrospective study of patients with stage IV CRC from 2008 to 2017, the average age was 59.46 years while the average KPS was 78.22, indicating the patients’ poor physical condition, which may have reduced the OS of the studied population. Of the 191 included patients, 166 (86.91%) were deceased. The 1-, 3-, and 5-year survival rates of all patients were 42.02%, 13.45%, and 5.04%, respectively. The median OS time was 23.07 months. In the real world, the median survival time for advanced CRC patients is estimated to be 18 months22-24; the patients in our study experienced a longer overall median survival time. These results indicate that supplementary CHM therapy was associated with OS.
In this cohort, we divided the patients into high- and low-exposure groups. Patients who accepted CHM therapy for more than 6 months experienced a preferable median OS of 26.13 months, compared with 14.67 months in the low-exposure group. Additionally, the death risk was significantly reduced by 55.6% in the high-exposure group, which is consistent with the adjusted result. The significant association between high CHM exposure and improved OS was independent of other predictors of patient outcome, including the tumor location, tumor differentiation, liver metastases, primary surgery, targeted or location therapy, and chemotherapy. These results show that patients who receive a longer duration of CHM therapy may benefit more in terms of OS.
We used propensity score matching (PSM) to ascertain equivalent variables in the 2 cohorts. The results remained stable. In the PSM model, we matched all of the covariates that had been adjusted in the Cox model. There were 28 patients matched, 14 in each group. In the PSM model, the HR was 0.52 (95% CI = 0.23-1.20; P = .1252). The high-exposure group showed a 48% reduction in the risk of death when compared with the low-exposure group. However, the result was not significant, which may due to the small sample size (Supplemental Material 2; available online).
An aspect of the study worthy of discussion is how we divided the patients into the high- and low-exposure groups. Considering the amount of information that we collected, 6 months was the shortest time point that allowed us to observe significant survival differences between the 2 groups. Moreover, we also examined survival differences between the 2 groups using 1 year of CHM therapy as the cutoff point, and the results remained stable. Thus, to facilitate clinical communication and balance the number of patients in each group, we eventually chose to use 6 months as the critical point.
The correlation between CHM exposure and OS was further confirmed in the subgroup analyses, and our results may indicate the population that would most benefit from CHM treatment. The HRs from patient subgroups were less than the total HRs, suggesting that patients with specific characteristics may benefit more from CHM than others. The subgroup exploratory analysis showed that patients with high CHM exposure who had already accepted local therapy, targeted therapy, or surgery tended to benefit more. We speculate that traditional Chinese medicine, combined with standard cancer therapy, may improve the survival time of patients; the potential mechanism may be alleviating the side effects of standard treatment or improving patients’ immunity. 25 Patients with high CHM exposure and a KPS >80 may benefit more from traditional Chinese medicine treatment, which implies that the earlier CHM therapy is accepted, the better a patient’s prognosis.
The current study provided limited data regarding the impact of CHM therapy on advanced CRC survival outcomes. In previous studies, we demonstrated that the combination of CHM and hepatic radiofrequency ablation could improve patients’ quality of life, reduce the incidence of bone marrow suppression, and prolong the half-year progression-free survival time of patients with CRLM.26,27 In our previous work, we also showed that CHM may elicit anti-inflammatory and anti-oxidative-stress responses either in vitro or in vivo; this may be due to the overall anti–colon cancer effect of CHM. Previously, we had focused only on survivors of stage II and stage III CRC. In the present study, we found that even patients with CRC at advanced stages could benefit from CHM therapy lasting more than 6 months. 19 It should be noted that the baseline data of the current study were not statistically balanced between the 2 groups in terms of chemotherapy and KPS score. It is difficult to balance the baseline in an observational study. As such, we introduced multivariate and subgroup analyses to adjust for the effects of chemotherapy and KPS score on the outcome measurement. The results revealed that patients with lower KPS scores (KPS < 80) or those who had not undergone chemotherapy could still gain the survival benefit from high-exposure to CHM therapy. The benefit, however, was not statistically significant, which may be due to the small sample size.
To date, accumulating evidence from cell cultures, animal experiments, and clinical research points to an anticancer effect of CHM.14,28,29 A multicenter prospective cohort study 19 indicated that a longer duration of CHM therapy contributed to better disease-free survival and OS among CRC survivors of postoperative stages II and III. Authors of a retrospective, observational, multicenter, cohort study 18 reported that patients who received CHM therapy could experience longer disease-free survival, while the survival benefits were more obvious in a subgroup of patients with right-sided colon cancer. Zhang et al 17 reported that the use of Jianpi Jiedu herbs, when combined with chemotherapy for advanced CRC, significantly enhanced KPS and reduced adverse events. Statistics from the National Health Insurance Research Database of Taiwan revealed that, under co-treatment involving conventional medical treatments and CHM, most CRC survivors consumed herbal therapies with the intention of relieving their gastrointestinal symptoms. Collectively, these studies may illuminate a way to make use of data from a retrospective cohort study for real-world clinical practices.
Nevertheless, the limitations of this study require further comment. First, measurement of the period of CHM exposure was not precise, which may make our results susceptible to recall bias. Second, the detailed CHM herbal formulas or herbs prescribed to each patient were not analyzed in the current study; however, we present the key formula and modifications, which could potentially benefit CRC patients. Third, we did not assess side effects in this study; however, patients with advanced cancer underwent tests to determine liver and kidney function and blood analysis every 1 to 3 months. In the long-term clinical application of traditional Chinese medicine in our hospital, no hepatorenal toxicity or other complications caused by traditional Chinese medicine have been found. The results of our other clinical studies suggest that the combination of traditional Chinese medicine and Western medicine has obvious advantages in reducing the blood toxicity and hepatorenal toxicity associated with chemotherapy. 30 Finally, the study had limited power resulting from a small sample size. Therefore, the results should be validated in future studies with large samples. Despite these limitations, we believe the study supports future evaluation of the use of CHM in integrative treatment for patients with advanced CRC. Hence, the observational results must be interpreted with prudence and validated by a randomized controlled trial to confirm the causal correlation between long-term CHM therapy and better survival outcomes.31,32
Conclusion
In sum, this retrospective study of patients with advanced CRC suggests improved patient survival outcomes with longer periods of CHM therapy. Although conclusive evidence for causality was not obtained in the current study, our findings provide the field at large further insight into the role of CHM therapy in the outcomes of patients with CRC. Higher quality scientific evidence is warranted to confirm our findings.
Supplemental Material
Supplement_material_1_Details_on_the_chemotherapy_and_targeted_drugs – Supplemental material for Effect of Chinese Herbal Medicine on the Survival of Colorectal Cancer Patients With Liver-Limited Metastases: A Retrospective Cohort Study, 2008 to 2017
Supplemental material, Supplement_material_1_Details_on_the_chemotherapy_and_targeted_drugs for Effect of Chinese Herbal Medicine on the Survival of Colorectal Cancer Patients With Liver-Limited Metastases: A Retrospective Cohort Study, 2008 to 2017 by Cui Shao, Qian Zuo, Jietao Lin, Rong Jian Yu, Yuanfeng Fu, Min Xiao, Ling Ling Sun and Lizhu Lin in Integrative Cancer Therapies
Supplemental Material
supplement_material_2_propensity_score_to_match_the_two_cohort – Supplemental material for Effect of Chinese Herbal Medicine on the Survival of Colorectal Cancer Patients With Liver-Limited Metastases: A Retrospective Cohort Study, 2008 to 2017
Supplemental material, supplement_material_2_propensity_score_to_match_the_two_cohort for Effect of Chinese Herbal Medicine on the Survival of Colorectal Cancer Patients With Liver-Limited Metastases: A Retrospective Cohort Study, 2008 to 2017 by Cui Shao, Qian Zuo, Jietao Lin, Rong Jian Yu, Yuanfeng Fu, Min Xiao, Ling Ling Sun and Lizhu Lin in Integrative Cancer Therapies
Footnotes
Acknowledgements
We would like to thank the doctors, nurses, technical staff, and hospital administration staff at the First Affiliated Hospital of Guangzhou University of Chinese Medicine.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Guangzhou Science and Technology Bureau (201904010396) and the National Natural Science Foundation of China (81573780).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.