
Abstract
Introduction
Dumping syndrome, also referred to as rapid gastric emptying syndrome, is a gastrointestinal disease usually caused by gastric surgery. Hertz 1 first described the postprandial symptoms associated with rapid gastric emptying after gastroenterostomy. Wyllys et al 2 introduced the term “dumping” for this syndrome.
Gastric cancer is commonly diagnosed in locally advanced or metastatic stage because of its late-developed physical signs. Therefore, surgical therapy, suggested by its prognosis, is considered as the only curative option despite advances of perioperative chemotherapy and radiological therapy. Massive resection like total gastrectomy or Roux-en-Y reconstruction is recommended for diffuse type or depending on tumor location, and limited resection such as subtotal gastrectomy is considered for palliation or in very elderly patients. 3 As a result of surgery, dumping syndrome is one of the major complications that is to be managed for postoperative care of gastric cancer patients.
Dumping syndrome is classified into 2 types based on characteristics of the symptoms. Early dumping syndrome is associated with gastrointestinal responses due to rapid gastric emptying, occurs within 10 to 30 minutes after meals, and results in symptoms such as nausea, vomiting, epigastric pain, bloating, and diarrhea. Late dumping syndrome is associated with neurohormonal responses, occurs 1 to 3 hours after meals, and results in vasomotor symptoms such as flushing, dizziness, palpitation, desire to lie down, and postprandial hypoglycemia with hyperinsulinemia. Consequently, dumping syndrome causes patients to develop a fear of eating, which results in malnutrition and weight loss and decreases quality of life. Konishi et al 4 and Nguyen et al 5 reported that rapid gastric and intestinal transit is a major pathology of dumping syndrome. The pancreatic β-cell causes dumping syndrome patients to suffer from hypoglycemia due to hyperinsulinemia.6,7 Intestinal hormones, such as GLP-1, which increases after meals, are also suggested to be involved in dumping syndrome.7,8 Dumping syndrome is primarily caused by gastric surgery but also by congenital microgastria 9 or a dislocated feeding tube. 10
The incidence of dumping syndrome is reported in 24.18% of patients who undergo a Roux-en-Y gastric bypass (RYGB),11-13 approximately 20% of patients who undergo a vagotomy with pyloroplasty, and up to 50% of patients who undergo an esophagectomy.14-18 Another study reported that 20.5% of patients who had other types of procedures, such as a sleeve gastrectomy and a vagotomy, also had an incidence of dumping syndrome.11-13
Dumping syndrome is diagnosed based on symptoms that become aggravated after meals, provocation tests, laboratory tests, gastric surgical history, or basal circumstances of rapid gastric emptying. Scale and scoring systems for dumping syndrome have been introduced, such as Sigstad’s score, 19 Postgastrectomy Syndrome Assessment Scale (PGSAS)-45,20-22 and Dumping Symptom Rating Scale (DSRS). 23 Provocation tests are also used, which include the oral glucose tolerance test and the hydrogen breath test. Laboratory and radiologic tests are helpful in making a diagnosis for late dumping syndrome patients, which include plasma glucose, insulin, GLP-1 after meals, and gastric emptying scintigraphy tests. 24
Current treatment for dumping syndrome includes pharmacological and surgical interventions. Dietary supplements (pectin, guar gum, acarbose25-30), somatostatin analogs (pasireotide,5,31-33 octreotide 31 ), miglitol,34-36 iraglutide, 37 exendin-(9-39), 38 and diazoxide 39 are prescribed for postprandial hypoglycemia or hyperglycemia caused by dumping syndrome. The GLP-1 receptor blocker can improve hypoglycemia caused by dumping syndrome. 40 RYGB reversal41,42 is an option to eliminate cause of dumping syndrome. Endoluminal revision 43 is also considered for complications of RYGB. A loop duodenojejunal bypass 44 is performed for dumping syndrome caused by RYGB or esophageal replacement. 45 Dietary management 46 is recommended to be combined with other interventions. Patients should consume a reduced amount of food at each meal and should delay fluid intake until at least 30 minutes after meals. 46 High-fiber and protein-rich foods, fruits, and vegetables are also recommended. 47 Limiting glucose 48 can reduce symptoms.
Previous systematic reviews have been conducted to evaluate the symptoms based on the type of surgery, but no review on the effect and efficacy of herbal medicine has been conducted. Studies on herbal medicine treatment for dumping syndrome are limited in case reports, case series, and controlled trials.
The aims of this review were to gather information on current research and to evaluate the effectiveness and the safety of herbal medicine in the treatment of dumping syndrome.
Methods
Criteria for Considering Studies for This Review
The protocol for this review was registered at PROSPERO ID CRD42018090538 on March 19, 2018 (archived at http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42018090538).
Search Methods for the Identification of Studies
The following databases were searched: PubMed, EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL), AMED, CINAHL, CNKI, Wanfang, VIP, CiNii, and 7 Korean medical databases (Koreantk, Oasis, RISS, DBPOA, KISS, KISTI, and NDSL). All searches ended in March 2018. The search terms included “Dumping syndrome,” “Postprandial syndrome,” and so on (see Appendixes A and B). Search strategies were used to find related studies, and a modified search formula for characteristics of each database was applied.
Study Selection
Two authors (BP and SH) selected studies for eligibility and checked them against the inclusion criteria independently. All randomized controlled trials (RCTs) were included in this review without restrictions on time or language.
Inclusion Criteria
Only RCTs of herbal medicine treatment for dumping syndrome patients were included. The patients were diagnosed with dumping syndrome based on their symptoms followed by any type of gastrointestinal surgery, and they were included without any restriction of sex, age, race, country, and onset. All treatments using herbal medicines were included without any limitations on number, administration methods, dosages, and durations of treatment. It was determined that the control treatments would include any type of conventional therapy, placebo medication, and no treatment. Primary outcomes included improvement in symptoms assessed by validated tools, such as Sigstad’s scoring system, Art’s questionnaire, the DSRS, overall symptoms improvement, and so on. Secondary outcomes included adverse events and quality of life. Trials that were case reports, cross-over designed, nonrandomized, and noncontrolled, and those that included nonherbal therapy, such as acupuncture or moxibustion, were excluded.
Data Extraction and Management
Two authors (BP and SH) extracted the data from the included studies independently. The data were extracted using a standard data extraction approach that included methodology, participants, intervention, duration of treatment, outcomes, and conclusions.
Assessment of Risk of Bias in Included Studies
Two authors (BP and SH) independently assessed the risk of bias, which is described in the Cochrane Handbook for Systematic Reviews of Interventions. The quality of studies was categorized into low, unclear, or high risk of bias according to the risk for each important outcome within the included studies, including adequacy of the generation of the allocation sequence, allocation concealment, and blinding and whether there were incomplete outcome data or a selective reporting of the results. Studies that met all criteria were categorized as a low risk of bias, studies that met none of the criteria were categorized as a high risk of bias, and those with insufficient information to draw a conclusion were categorized as an unclear risk of bias.
Data Analysis
Data analysis was performed using RevMan 5.3 (The Nordic Cochrane Centre, Copenhagen, Denmark; The Cochrane Collaboration, 2016) software. Binary outcomes were summarized using a risk ratio (RR) with a 95% confidence interval (CI) for relative effect and a risk difference with 95% CI for absolute effect. The continuous outcomes were summarized using mean difference with a 95% CI. If there were sufficient data (similar clinical characteristics, such as study design, participants, interventions, control, and outcome measures) and an acceptable statistical heterogeneity, the data were pooled, and a meta-analysis was performed using the random effect model. Statistical heterogeneity was detected by the I2 test, and an I2 > 50% indicated the possibility of statistical heterogeneity among the studies. If the I2 was larger than 75%, which means there was a clear statistical heterogeneity among studies, the results from each study were evaluated independently rather than pooling the data for analysis. A funnel plot analysis was considered to detect publication bias.
Results
Results of the Search
From the 16 electronic databases, 830 articles were identified (Figure 1). After excluding duplicate studies and articles that did not meet the inclusion criteria on the basis of reading the title and abstract, the full texts of 24 articles were retrieved and evaluated. After browsing full-text articles, 21 articles were excluded; 3 were not RCT, and 19 did not discuss dumping syndrome49-69 (Table 2). Consequently, 3 trials were included for the review process and data analysis70-72 (Table 1).

Flow chart.
Included Studies.
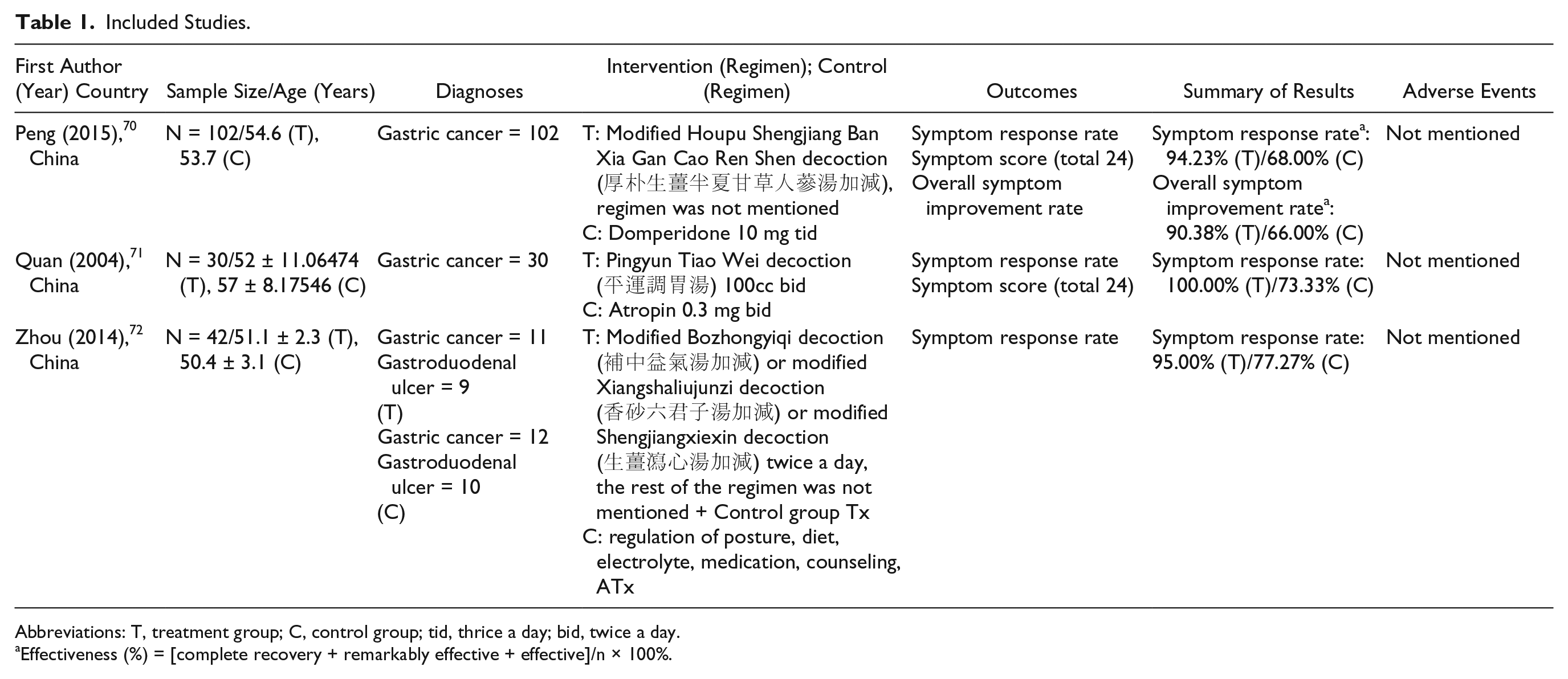
Abbreviations: T, treatment group; C, control group; tid, thrice a day; bid, twice a day.
Effectiveness (%) = [complete recovery + remarkably effective + effective]/n × 100%.
Excluded Studies by Full-Text Screening.

Abbreviations: RCT, randomized controlled trial; QOL, quality of life.
Characteristics of the Included Studies
A total of 174 dumping syndrome patients were included, and there was no report of dropouts. All 3 trials included dumping syndrome patients without a classification of surgery or disease cause or a classification of early/late dumping syndrome. One trial 71 did not report patients’ characteristics, such as age or sex. The mean sample size was 58 patients, but no trial reported the calculation sequence of the sample size. The duration of treatment ranged from 10 to 35 days.
All 3 trials used different herbal decoctions via oral administration. Two trials70,71 used 1 decoction during the trial, but 1 trial 72 used 3 modified decoctions according to individual symptom patterns based on oriental medicine diagnoses.
For the control group treatment, 2 trials used conventional pharmacotherapy. One 70 used domperidone, and the other 71 used atropine; however, another one 72 used a complex therapy for the control group, which included postural and diet regulation, counseling, and acupuncture.
Outcome Assessment
All the included studies used the symptom response rate, which was designed to evaluate subjective symptoms of dumping syndrome and is similar to the Likert-type scale. This scale lists gastrointestinal symptoms, such as epigastric discomfort, belching, loss of appetite, general weakness, abdominal distension, loose stool, hyperperistaltic sound, and postprandial somnolence. Two trials70,72 used the overall symptoms improvement rate, which is scored based on the improvement of symptoms after treatment as complete recovery, remarkably effective, effective, or not effective.
Risk of Bias of Included Studies
According to the predefined methodological quality criteria, all 3 trials were evaluated by 2 authors (BP, SH). All 3 trials mentioned the randomization, but no trials reported the generation of sequence, blinding, or dropout. All studies appeared to have a high risk of bias in the blinding of both patients and operators. Because none of the trials was found to have preregistered protocols in the electronic databases, “selective reporting” was basically assessed as an “unclear risk of bias” by checking the methods and results sections from each trial (Figure 2).

Risk of bias of included studies.
Therapeutic Effects of Interventions: Herbal Medicine Versus Conventional Medicine
As pharmacotherapy and other types of diet and lifestyle supportive management are conventional therapies for dumping syndrome, all 3 trials were only analyzed for the therapeutic or adjunctive effects of herbal medicine against conventional therapies (Figure 3).

Forest plot of included studies.
Two trials70,71 investigated herbal medicine compared with conventional medication for dumping syndrome. These studies reported results using the symptom response rate, but different herbal decoctions were used. One trial 70 reported that 14 days of modified Houpu Shengjiang Ban Xia Gan Cao Ren Shen decoction administration (RR = 1.35, 95% CI = 0.98-1.85) led to a better improvement compared with the domperidone group but did not identify a significant difference between groups. The other trial 71 reported that 10 days of Pingyun Tiao Wei decoction administration (RR = 1.39, 95% CI = 1.13-1.70) was found to have a significant effect on improving the symptom response rate score when compared with the atropine group. The meta-analysis showed significant effects of herbal decoction compared with conventional medication (n = 132, RR = 1.37, 95% CI = 1.16-1.63, P = .0003, I2 = 0%).
One trial 70 also reported results using the overall symptoms improvement rate. Fourteen days of modified Houpu Shengjiang Ban Xia Gan Cao Ren Shen decoction administration (RR = 1.37, 95% CI = 1.10-1.70) was found to have a significant effect on improving the symptom response rate score when compared with the domperidone group.
One trial 72 investigated adjunctive herbal medicine compared with the group provided with conventional care for dumping syndrome. Using the overall symptoms improvement rate, the author reported that 21 to 35 days of herbal decoctions (RR = 1.23, 95% CI = 0.96-1.58) treatment, which included modified Buzhongyiqi decoction, modified Xiangshaliujunzi decoction, or modified Shengjiangxiexin decoction, with conventional care relieved patients’ symptoms, but there was no significant effect on improving the symptom response rate score when compared with the conventional treatment group.
Adverse Events
None of the studies mentioned adverse events following herbal medicine treatment.
Discussion
According to the 3 trials that reported the results of 174 dumping syndrome patients who were administered herbal medicines for their symptoms, which were measured by the symptom response rate and the overall symptoms improvement rate, the modified Houpu Shengjiang Ban Xia Gan Cao Ren Shen decoction was shown to significantly improve the score compared with conventional medicine; however, for the Pingyun Tiao Wei decoction, modified Buzhongyiqi decoction, modified Xiangshaliujunzi decoction, and modified Shengjiangxiexin decoction, significant improvement was difficult to determine.
Electronic databases that were likely to contain most trials that investigated herbal medicine were searched; however, only 24 studies were identified after screening, and 21 studies did not match the review’s objectives. Therefore, a small number of trials for dumping syndrome patients who were treated with herbal medicine met the inclusion criteria. This suggests that further research is needed to evaluate the effectiveness of herbal medicine in treating dumping syndrome. Although there was a lack of quality related to study design, the trials indicated that using herbal medicine to treat dumping syndrome could be more beneficial than conventional therapy alone. Currently, only an unclear possibility of the effectiveness of herbal medicine in treating dumping syndrome is suggested, and thus RCTs with an improved design and performance are needed.
Although the databases were searched without limitations related to language and country, all included trials were published in China. This suggests that the conclusions of these trials could contain publication bias if there is a positive tendency of researchers and journals in China.
The trials evaluated the effectiveness of herbal medicine on symptom scores related to gastrointestinal symptoms. There are clear limitations to interpret the result, as included trials of this review evaluated categorical scores about improvement of symptoms. None of the included trials considered Sigstad’s score, PGSAS-45, DSRS, provocation tests that are already been established; laboratory tests for blood glucose or insulin; or radiological evidence of rapid gastric emptying. Although all trials showed a positive effect after treatment, information related to changes, such as blood glucose after meals, hyperinsulinemia, or quality of life, was not found. In addition, the scale used for the trials mostly referred to early dumping syndrome symptoms and did not specify whether the symptoms were related to early or late dumping syndrome. Thus, whether herbal medicine is effective for early or late dumping syndrome is unclear.
As the result shows, there were improvements in both herbal medicine group and conventional medication group. Although Quan’s 71 result did not show significant benefit of herbal medicine as shown in Figure 3, Analysis 1, the meta-analysis that was performed in low heterogeneity showed favor to herbal medicine within level of significance. However, the change of overall symptom improvement rate was compared with different control managements in each of the studies as shown in Figure 3, Analyses 2 and 3; and therefore, it was not proper to synthesize and perform meta-analysis. Additionally, owing to lack of sufficient sample size (n = 132 in Figure 3, Analysis 1), these synthesized data were not fully considered to conclude a single firm opinion. If more samples are retained in further studies, it will give a better view of the effectiveness of herbal medication.
Various herbal formulas were used in each trial, respectively, but were composited with similar herbs that relieve gastrointestinal symptoms. Herbs such as Zingiberis Rhizoma Recens (生薑; ginger), Pinelliae Tuber (半夏), Magnoliae Cortex (厚朴), which are used by Peng 70 and Zhou, 72 and herbs like Coicis Semen (薏苡仁), Codonopsis Pilosulae Radix (黨蔘), which are used by Quan 71 and Zhou, 72 are to facilitate and improve digestive function. However, Zhou 72 modified the herbal decoction depending on disease pattern diagnosis (辯證) of each patient. This results in a change of treatment group not only by the individual herbal action but also by systemic pattern of each patient. As an example, Zhou 72 used 3 different decoctions, modified Buzhongyiqi decoction (補中益氣湯加減) for energy-depression of digestive system pattern (中氣下陷), modified Xiangshaliujunzi decoction (香砂六君子湯加減) for energy deficiency of digestive system pattern (脾胃虛弱), and modified Shengjiangxiexin decoction (生薑瀉心湯加減) for pathologic wet heat of digestive system pattern (濕熱中阻). Therefore, strict interpretation of the results would be needed, while the authors suggested the potential effectiveness of herbal medicine with current evidence. Pharmacologic mechanisms of these herbs are partially known. For example, Zingiberis Rhizoma Recens contains phytochemicals like gingerol, which affect the gastric mobility and secretion of gastric acid. 73 Pinelliae Tuber is reported to have antiemetic effect via chemoreceptor trigger zone. 74 Magnoliae Cortex contains magnolol, which is thought to be related with gastric histamine release, and antiemetic effect.75,76 Most herbs that were used in trials are related with digestive function; however, more research is needed to discuss the mechanism of herbal medicine because of various combination of herbal decoctions and also pattern diagnosis of each patient.
After treatment, the symptoms of all the patients who participated in all trials were reduced, but there was no follow-up observation after improvement. As dumping syndrome is a recurring syndrome based on diet and its gastric emptying mechanism, the symptoms should be observed during the posttreatment period. Whether the recurrence of symptoms could be prevented could not be determined due to a lack of information. In addition, the evaluation of adverse events was not mentioned. In future research studies, reporting adverse events must be considered to obtain high-quality evidence and to apply the findings to clinical practice.
There was no declaration of dropouts during the trials. None of the included studies mentioned clear randomization or blinding methods. Moreover, the concealment of allocation was not reported. Although these trials were RCTs, there is a high risk of bias related to overestimating the effect of herbal medicine due to a lack of reliability and inadequate randomization.
Conclusion
Herbal medicines may improve the gastrointestinal symptoms of dumping syndrome patients compared with conventional medicine; however, the included trials had limitations, such as a lack of information, a lack of quality, and a small sample size. Additional research studies that include adequate methodological procedures to prevent biases and a larger sample with results calculated by statistical methods are needed to clearly determine the effectiveness of herbal medicine in treating dumping syndrome.
Footnotes
Appendix A
Appendix B
Author Contributions
Conceptualization: Bongki Park
Data curation: Bongki Park, Seungcheol Hong
Formal analysis: Bongki Park, Seungcheol Hong
Investigation: Bongki Park, Seungcheol Hong
Methodology: Bongki Park
Project administration: Bongki Park, Dong-Jun Choi
Software: Seungcheol Hong, Hyeonseok Noh
Supervision: Bongki Park, Hyeonseok Noh, Dong-Jun Choi
Validation: Bongki Park, Seungcheol Hong, Dong-Jun Choi
Writing—original draft: Bongki Park, Seungcheol Hong
Writing—review and editing: Bongki Park, Hyeonseok Noh, Dong-Jun Choi
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.