
Abstract
Objective
This study compared Chinese herbal injections (CHIs) plus chemotherapy with chemotherapy alone in terms of clinical efficacy and safety for treating patients with esophageal cancer (EC).
Methods
Randomized controlled trials (RCTs) of CHIs combined with chemotherapy for treating EC published in English and Chinese databases were identified. The main outcomes were clinical efficacy, performance status, and adverse reactions. Random-effects models were fitted to calculate the odds ratios and 95% confidence intervals for all pair-wise comparisons.
Results
In total, 29 RCTs of eight CHIs were included in this study. The results of cluster analysis demonstrated that Compound Kushen injection plus chemotherapy was the optimal choice for improving the clinical efficacy rate. Shenfu injection was associated with a relatively high performance status. Compound Kushen injection and Shenfu injection were inferior to other CHIs in terms of preventing leukopenia and gastrointestinal side effects.
Conclusions
The combination of Compound Kushen injection with chemotherapy could improve efficacy and reduce adverse drug reactions versus chemotherapy alone in patients with EC.
Keywords
Introduction
Globally, esophageal cancer (EC) has emerged as the leading cause of cancer-related death, and it represents a major global health challenge because of its poor prognosis, increasing incidence, and high mortality rates.1–3 EC is more common in developed countries than in developing countries. Furthermore, the characteristics of EC are epidemiologically and biologically distinct, and an estimated 4,292,000 new cases and 2,814,000 deaths were estimated to occur in China in 2015.4,5 Following the approach of surgery alone, locally advanced EC frequently and eventually progresses to metastatic disease despite multimodality therapy, and chemotherapy is recommended as an adjunctive therapy for such patients.6–8 Nevertheless, improvements in the efficacy of chemotherapy have been marginal over the past three decades, and it is widely recognized that chemotherapy is associated with significant hematologic toxicity and modest effects against EC.7,9 As the critical backbone of complementary and alternative medicine, traditional Chinese medicine (TCM) has gradually gained global recognition for treating EC based on its favorable effects on symptoms and the disease, it has become a promising and active area of both fundamental and clinical research in the field of anti-cancer therapy. In addition, it has been elucidated that the anti-tumor mechanisms of TCM involve the regulation of autologous immune function, inhibition of tumor cell growth and proliferation, and induction of tumor cell autophagy and apoptosis.10–12 According to accumulated evidenced-based data, the combination of Chinese herbal injections (CHIs) and chemotherapy or radiotherapy is associated with considerable efficacy in treating patients with digestive system malignancies.13–15 However, a paucity of scientific research exists regarding the combined use of CHIs plus chemotherapy in patients with EC. Thus, the present research used network meta-analysis (NMA) to provide evidence-based hierarchies of the comparative efficacy and safety of CHIs combined with chemotherapy and provide additional insights for identifying optimal CHI-based regimens for treating EC.
Materials and methods
The procedure of the current research was conducted according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines “NMA extended version.” 16
Literature search
A comprehensive literature search was performed, tested, and directed by a well-trained librarian in consultation with our review team to identify individual studies in multiple databases from their inception to March 5, 2018. The databases searched in this study included Embase, PubMed, Cochrane Library, the China National Knowledge Infrastructure Database (CNKI), and the Wanfang Database. No language restriction was applied. The searching strategies were divided into three parts: EC, CHIs, and randomized controlled trials (RCTs). In addition, the search terms for EC included “Esophageal Neoplasms, Esophageal Neoplasm, Esophagus Neoplasm, Esophagus Neoplasms, Cancer of Esophagus, Cancer of the Esophagus, Esophagus Cancer, Esophagus Cancers, Esophageal Cancer, and Esophageal Cancers.” A combination of MeSH and free-text terms was adopted. In the Chinese databases, using CNKI as an example, the search term for EC was “esophageal cancer” together with a full-text search for “random.” Additionally, we manually searched bibliographies and added related references to ensure that all relevant RCTs were included in the analysis.
Inclusion and exclusion criteria
In the present systematic review, we included RCTs meeting the eligibility criteria as follows: RCTs using CHIs combined with chemotherapy to treat EC; patients meeting the diagnostic criteria regarding the pathology, cytology, or histology of EC, regardless of gender, race, or disease severity; and the intervention of interest in this NMA was the combination of CHIs and chemotherapy. All doses, treatment schedules, and durations of different regimens were eligible. By contrast, the patients in control group only received chemotherapy. In addition, the clinical efficacy rate and performance status were the primary outcomes of interest, and adverse drug reactions (ADRs) including leukopenia and gastrointestinal side effects were considered safety outcomes.
We excluded studies meeting any of the following criteria: diagnosis of other primary tumors; CHIs were applied non-intravenously, and the comparator treatment was not chemotherapy; the studies were not RCTs; and essential information could not be extracted, such as drug names, dosage, duration of treatment, and outcomes.
Data extraction and risk of bias assessment
The screening of citation titles and abstracts among the search records was conducted by two reviewers independently to assess study eligibility according to the inclusion and exclusion criteria. The full text of citations considered to describe potentially eligible articles was independently reviewed. The consensus principle was used to resolve disagreements between the reviewers. The following data were extracted and acquired from eligible studies: study information (e.g., title, author names, publication date), baseline characteristics of the population (e.g., sample size, age, gender, performance status, tumor status), and study characteristics (e.g., study design, items of quality evaluation, dosing regimens, treatment duration, outcomes). The quality assessment of each eligible study was performed by two investigators independently in accordance with the Cochrane Risk of Bias Assessment Tool. 17 The quality assessment was divided into seven domains, namely randomization sequence generation, allocation concealment, blinding of both participants and outcome assessors, incomplete outcome data, selective reporting, and other bias. Each domain was rated as low, unclear, or high risk according to the corresponding details in the eligible studies.
Statistical analyses
First, a pair-wise meta-analysis was performed using the random-effect model in consideration of within- and between-study heterogeneity among the included RCTs. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated and calculated to produce a summary effect size for each endpoint.18,19 The data were analyzed using WinBUGS 1.4.3 software. Bayesian inference was performed using Markov Chain Monte Carlo simulation, and 200,000 iterations were used, with the first 10,000 iterations discarded as a burn-in for annealing to eliminate the impact of the initial value in the WinBUGS program.20,21 Subsequently, Stata software (Stata Corp, College Station, TX, USA) was employed to generate network geometry, depict plots, determine the effect size, evaluate the assumptions of the network meta-analysis, and determine the relative rankings of the interventions.22–24 As a valuable graphical tool, Stata software can provide comprehensive and easily understandable methods for displaying statistical analysis results. The network geometry was determined to explore comparative relationships among the different treatments. Node sizes indicated the total sample sizes for treatments, and the line thickness corresponded to the number of trials. 25 In addition, the surface under the cumulative ranking curves (SUCRA) was applied to rank the treatments to identify superiority. The interventions with higher SUCRA values were associated with the highest probability of being more effective. SUCRA ranges between 0 and 1, where 1 indicates that the treatment had a 100% probability of being ranked first and a 0% probability of being ranked last.26,27 Conceptually, the comparison-adjusted funnel plot was completed to evaluate the clinical and methodological heterogeneity. Additionally, cluster analysis was conducted to identify the optimal regimens in consideration of two different outcomes simultaneously. The interventions in the upper right region of the cluster analysis plots were more preferable options than the other regimens.28,29
Results
Literature selection and baseline characteristics
Initially, we identified 685 references after reviewing the titles and abstracts in our comprehensive search, and 359 citations were collected for additional review after excluding duplicate and irrelevant papers through reading titles and abstracts. Then, by reading the full text of potentially eligible articles, 29 RCTs of eight CHIs met our inclusion criteria.30–58 The literature screening process is shown in Figure 1. The number of studies of each CHI was as follows: Compound Kushen injection, seven trials; Aidi injection, six trials; Xiaoaiping injection, five trials; Huachansu injection, five trials; Shenqi Fuzheng injection, two trials; Kanglaite injection, two trials; Shenfu injection, one trial; and elemene injection, one trial.

Preferred Reporting Items for Systematic reviews and Meta-Analyses flow diagram.
The 29 RCTs included a total of 1967 patients. Among them, 1001 patients were included in the CHI group, and 966 patients were included in the control group. The basic characteristics of the included studies are summarized in Table 1. A network plot of the clinical efficacy rate and performance status in the Bayesian analysis is depicted in Figure 2.
Basic characteristics of the included studies.

NR, not reported. ① Clinical efficacy rate; ② performance status; ③ adverse reaction. AD, Aidi injection; SF, Shenfu injection; SQFZ, Shenqi Fuzheng injection; KLT, Kanglaite injection; EL, elemene injection; XAP, Xiaoaiping injection; CKS, Compound Kushen injection; HCS, Huachansu injection.
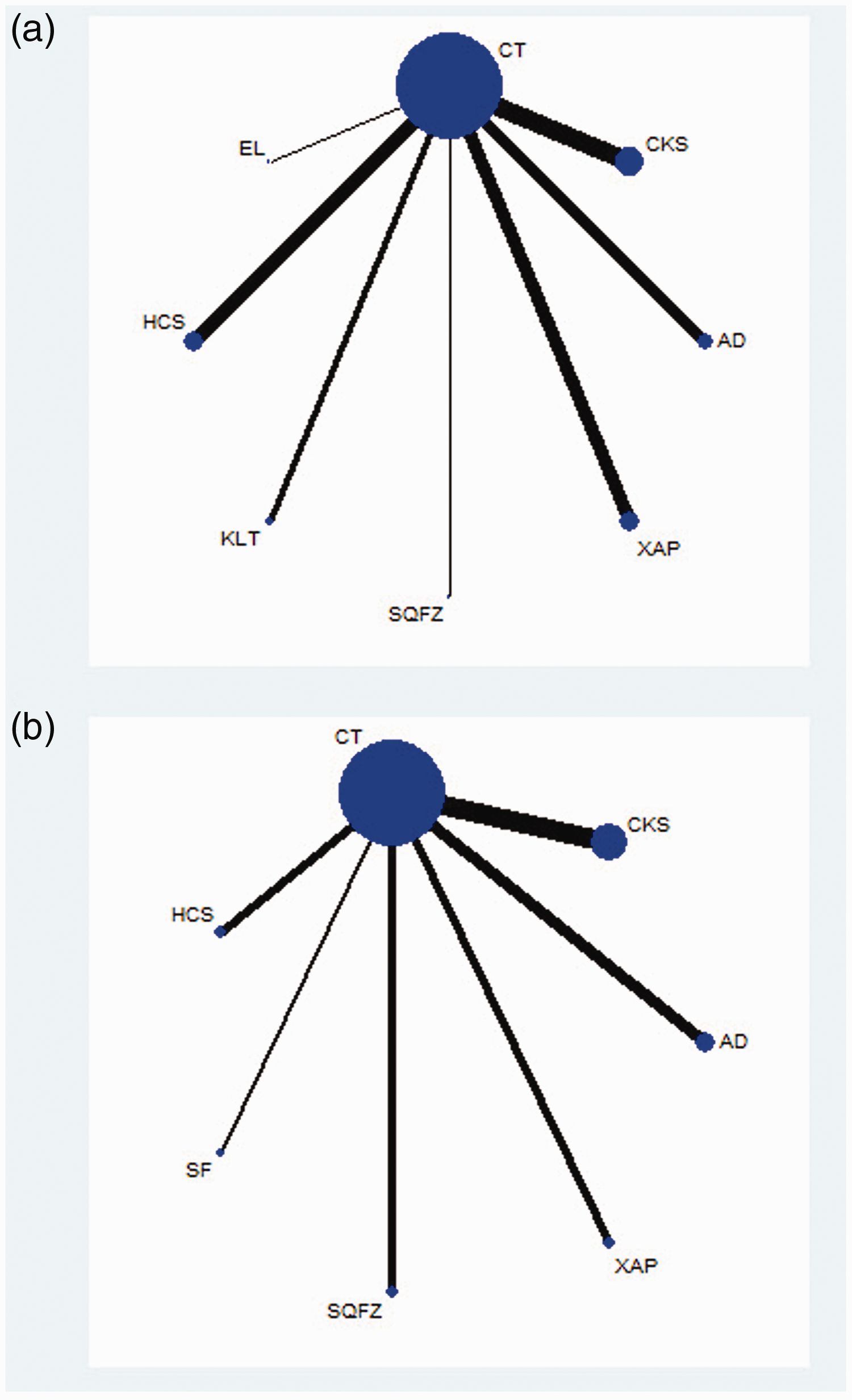
Network graph of the clinical efficacy rate (a) and performance status (b).
Quality assessment of included studies
Regarding selection bias, four (13.79%) trials adopted a random number table, and one (3.45%) trial used direct sampling to randomize subjects into groups. These studies were rated as having a low risk of bias. Only one (3.45%) trial was considered to have a low risk of performance bias because it used a blinding method. Regarding attrition bias, three (10.34%) trials were rated as low risk based on their follow-up data. The risk of the remaining RCTs was considered unclear.
In addition, the results of quality evaluation for the included RCTs indicated that 27 (93.10%) trials evaluated adverse events, whereas four (13.79%) trials described medical ethics. All 29 RCTs mentioned randomization and descried the inclusion and exclusion criteria, whereas no study described the estimation of sample size. The bias graph of the included RCTs is shown in Figure 3.

Bias graph of the included randomized controlled trials.
Clinical efficacy outcomes
Twenty-five RCTs of seven CHIs presented clinical efficacy rates. The results revealed that compared with the effects of chemotherapy only, Compound Kushen injection + chemotherapy (OR = 2.73, 95% CI = 1.55–4.85) and Huachansu Injection + chemotherapy (OR = 2.26, 95% CI = 1.20–4.17) were associated with significantly improved clinical outcomes (Table 2). According to the SUCRA of clinical efficacy, the seven CHIs were ranked as follows: Compound Kushen (72.61%) > Shenqi Fuzheng (65.83%) > Kanglaite (61.4%) > Huachansu (59.17%) > elemene (48.14%) > Aidi (46.2%) > Xiaoaiping (39.81%) (Figure 4a).
Results of the network meta-analysis of the clinical efficacy rate (upper right quadrant) and performance status (lower left quadrant).

Values in bold indicate statistically significant results. AD, Aidi injection; SF, Shenfu injection; SQFZ, Shenqi Fuzheng injection; KLT, Kanglaite injection; EL, elemene injection; XAP, Xiaoaiping injection; CKS, Compound Kushen injection; EL, HCS, Huachansu injection; CT, chemotherapy.

Rank of the cumulative probabilities for the clinical efficacy rate (a) and performance status (b).
Performance status
Fifteen RCTs of six CHIs were included in the performance status analysis. Aidi + chemotherapy (OR = 0.27, 95% CI = 0.12–0.57), Shenqi Fuzheng + chemotherapy (OR = 3.69, 95% CI = 1.52–9.41), Compound Kushen + chemotherapy (OR = 3.88, 95% CI = 2.16–6.93), and Shenfu + chemotherapy (OR = 6.77, 95% CI = 2.19–22.44) were associated with favorable responses in terms of performance status compared with the effects of chemotherapy alone (Table 2). The six CHIs were ranked in terms of performance status as follows: Shenfu (88.29%) > Compound Kushen (65.84%) > Aidi (63.84%) > Shenqi Fuzheng (62.17%) > Xiaoaiping (41.97%) > Huachansu (26.34%) (Figure 4b).
Safety outcomes
In total, 14 RCTs of six CHIs provided data regarding the incidence of leukopenia. The results demonstrated that Aidi + chemotherapy (OR = 3.29, 95% CI = 1.51–7.52), Shenfu + chemotherapy (OR = 0.22, 95% CI = 0.051–0.88), Shenqi Fuzheng + chemotherapy (OR = 0.33, 95% CI = 0.10–0.97) , Compound Kushen + chemotherapy (OR = 0.13, 95% CI = 0.049–0.32), and Xiaoaiping + chemotherapy (OR = 0.28, 95% CI = 0.090–0.78) were linked to lower rates of leukopenia than chemotherapy alone. In addition, no significant difference in clinical efficacy was observed among the CHIs (Table 3). According to the cumulative probabilities for leukopenia, the six CHIs were ranked as follows: Compound Kushen (90.47%) > Shenfu (68.45%) > Xiaoaiping (58.5%) > Aidi (53.59%) > Shenqi Fuzheng (50.28%) > Huachansu (24.85%). The top three CHIs were Compound Kushen, Shenfu, and Xiaoaiping (Figure 5c).
Results of network meta-analysis for leucopenia (upper right quadrant) and gastrointestinal side effects (lower left quadrant).

AD, Aidi injection; SF, Shenfu injection; SQFZ, Shenqi Fuzheng injection; KLT, Kanglaite injection; EL, elemene injection; XAP, Xiaoaiping injection; CKS, Compound Kushen injection; HCS, Huachansu injection; CT, chemotherapy.

Rank of the cumulative probabilities for leukopenia (a) and gastrointestinal side effects (b).
Fourteen eligible RCTs studying seven CHIs reported data regarding the incidence of gastrointestinal side effects. However, no significant differences in the rates of gastrointestinal side effects were observed among the treatments. Based on the occurrence of gastrointestinal side effects, the CHIs were ranked as follows: Shenfu (68.67%) > Shenqi Fuzheng (64.95%) > Compound Kushen (56.55%) > Aidi (53.58%) > elemene (50.78%) > Huachansu (48.57%) > Xiaoaiping (43.32%) (Figure 5d).
Additionally, the SUCRAs of different treatments for outcomes are shown in Table 4.
SUCRA values of different interventions for outcomes.

AD, Aidi injection; SF, Shenfu injection; SQFZ, Shenqi Fuzheng injection; KLT, Kanglaite injection; EL, elemene injection; XAP, Xiaoaiping injection; CKS, Compound Kushen injection; HCS, Huachansu injection; CT, chemotherapy.
Publication bias
The publication bias of the included RCTs was evaluated using funnel plots. The funnel plots were not visually symmetrical, indicating the existence of bias. The lack of negative results and large-scale clinical controlled trials might have also contributed to the bias (Figure 6).

Funnel plots of the included randomized controlled trials.
Cluster analysis
Cluster analysis of five CHIs revealed that the combination of Compound Kushen injection and chemotherapy was superior to the other regimens in terms of both clinical efficacy and performance status. Furthermore, the results for six CHIs concerning the incidence of leukopenia and gastrointestinal side effects indicated that Compound Kushen injection combined with chemotherapy was associated with lower rates of ADRs (Figure 7).
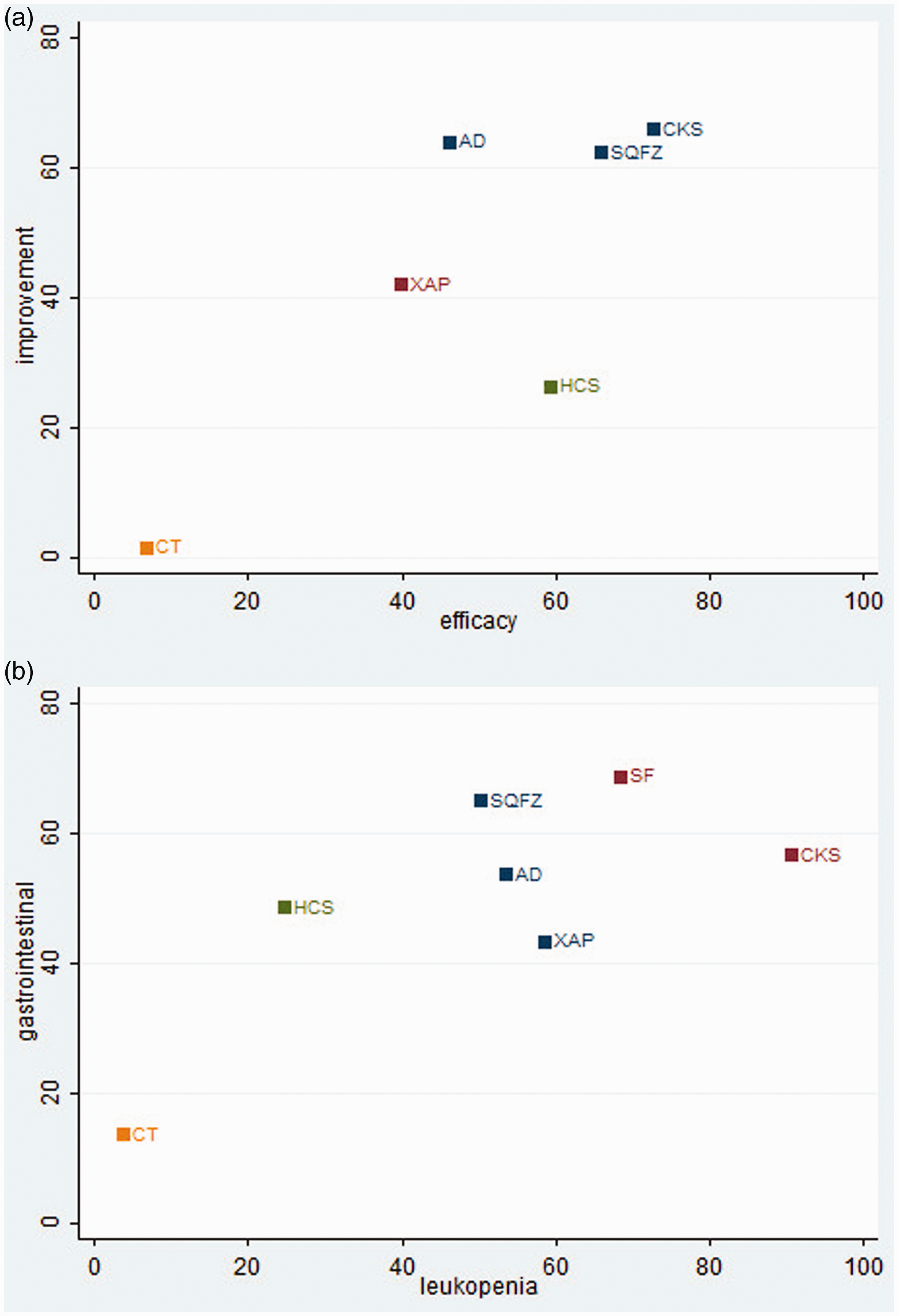
Cluster analysis plots. (a) Clinical efficacy rate (x-axis) and performance status (y-axis). (b) Rates of leukopenia (x-axis) and gastrointestinal effects (y-axis).
Discussion
We conducted the current NMA to evaluate the comparative clinical efficacy and safety of all reported combinations of CHIs and chemotherapy in the treatment of EC. Overall, the results revealed that Compound Kushen injection combined with chemotherapy was the best option for both improving clinical efficacy and reducing the incidence of leukopenia and gastrointestinal side effects.
Compound Kushen Injection is prepared from the medicinal plants Sophora flavescens and Heterosmilax chinensis. Recently, the results of clinical and pharmacological research indicated that Compound Kushen injection has utility as a selective adjunct treatment for patients with cancer. Systematic reviews have provided moderate evidence that Compound Kushen injection is beneficial for alleviating cancer-related pain, and it appears to have beneficial effects on the rates of side effects in patients receiving chemotherapy.59–61 Additionally, this CHI improved the efficacy and performance status of chemotherapy in patients with advanced colon cancer and reduced ADR rates among postoperative patients with breast cancer.62,63 The candidate anti-cancer molecular mechanisms of Compound Kushen injection include the perturbation of cell cycle progression, downregulation of actin cytoskeletal and focal adhesion genes, inhibition of tumor growth, and increases of the cell energy charge.64–67 Similarly as a variety of anti-tumor compounds, matrine and oxymatrine can inhibit the proliferation and differentiation of cancer cells, prevent metastasis and invasion, induce cell cycle arrest, accelerate apoptosis, and restrain angiogenesis, 68 and their underlying mechanisms have been validated and predicted using network pharmacology methods. The findings illustrated that the treatments target important pathways of cancers, including glycometabolism, amino acid metabolism, and PI3K-Akt signaling.69,70 Additionally, when using Compound Kushen injection in combination with chemotherapy in clinical practice, attention must be paid to ADRs to promote the rational use of TCM, improve their acceptance, and increase the recognition of the anti-cancer effects of CHIs. In addition, the selection of treatments in the clinic should also depend on multiple aspects including safety, patient preference, the specific disease situation, costs, local availability, clinician experience, and the duration of chemotherapy.
To our knowledge, this is the first study to compare different CHIs in combination with chemotherapy in the treatment of EC. Our study had several advantages. First, this study searched an extensive period and included a large sample of patients with EC. The searching strategies of our study were also more comprehensive given that both English and Chinese databases were searched and RCTs were identified using the websites of other relevant organizations. In addition, the search terms were divided into three parts, and the search strategy used a combination of MeSH terms and full-text words. Finally, our study comprehensively sorted the various outcome indicators including clinical efficacy, performance status, and rates of leukopenia and gastrointestinal side effects via cluster analysis.
Several limitations of our study should be noted. First, published data rather than individual patient information, which contains a more detailed appraisal of outcomes, were gathered in the present study. Second, the overall survival rate was the crucial indicator in the efficacy evaluation, whereas the follow-up data were insufficient for comparing the survival benefits of different CHIs. In addition, some included studies did not report randomization, blinding methods, and allocation concealment adequately, and these factors might undermine the validity of the overall findings. Finally, there may have been clinical heterogeneity because of the diversity of chemotherapeutic drugs. In this regard, our findings suggested that attention should be paid to the academic, scientific, and systematic components of clinical trials, such as recognizing the important endpoints of efficacy and safety outcomes, focusing on improving the methodological quality of clinical trials as well as the training of specialists and clinicians.
Conclusion
The available evidence in the present NMA demonstrated that the combination of Compound Kushen injection and chemotherapy was the optimal regimen in terms of efficacy and safety for patients with esophageal cancer. However, direct comparisons among different CHs are warranted and required to robustly demonstrate the possible and potential differences among these adjunctive therapies for chemotherapy.
Supplemental Material
IMR898336 Supplemental Material - Supplemental material for Systematic review and network meta-analysis comparing Chinese herbal injections with chemotherapy for treating patients with esophageal cancer
Supplemental material, IMR898336 Supplemental Material for Systematic review and network meta-analysis comparing Chinese herbal injections with chemotherapy for treating patients with esophageal cancer by Dan Zhang, Jiarui Wu, Haojia Wang, Wei Zhou, Mengwei Ni, Xinkui Liu and Xiaomeng Zhang in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The design of the study and collection, analysis, and interpretation of data were supported by the Young Scientists Training Program of Beijing University of Chinese Medicine and the National Nature Science Foundation of China (Grant nos. 81473547 and 81673829).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.