
Abstract
Introduction
Among the myriad of identified risks associated with cancer development and poorer prognosis, behavioral risk factors including poor diet, physical inactivity, and obesity are potentially modifiable via preventive and interventive efforts. Wellness interventions that integrate personalized nutrition counseling and exercise training have achieved modest short-term weight loss, but do not target the underlying mechanisms of obesity onset and maintenance, resulting in more than 80% to 85% of individuals regaining weight lost or even exceeding pre-intervention weight within 3 to 5 years post-intervention.1,2 Among women, 55% of all cancers are associated with overweight and obesity, compared with 24% among men, 3 yet effective long-term behavioral treatments for obesity remain elusive. Systematic reviews have repeatedly shown that obesity interventions among cancer survivors that utilize a comprehensive approach with dietary, physical activity, and behavior modification components are the most successful in the short term.4-6 However, to date, the behavior modification components of such interventions have largely been based solely on cognitive behavioral approaches, and few studies have evaluated the specific therapeutic components that contribute to intervention efficacy, or how underlying psychophysiological mechanisms are affected. 4 There is, therefore, a pressing need for studies of obesity interventions for cancer survivors that disentangle the mechanistic effects of cognitive intervention components from exercise and nutrition components. Moreover, novel therapeutic interventions that target the underlying maladaptive cognitive and affective mechanisms of obesity development and maintenance are needed.
The etiology and epidemiology of obesity is complex and multifactorial in nature, but is thought to be driven in part by appetitive dysregulatory mechanisms. Eating highly palatable food, such as energy-dense food with high fat and sugar content, is a potent reward that can be become increasingly salient and overconsumed in patterns that mirror other disorders of appetitive regulation such as addiction. 7 Animal models 8 and human neuroimaging studies9,10 demonstrate appetitive dysregulation in brain reward systems during both the development and maintenance of excess adiposity. Such reward dysregulation may be explicated by the allostatic model of addiction,11,12 which proposes that overstimulation of neural reward circuits with potent and addictive rewards (like highly palatable and calorie-dense foods) can increase sensitization to appetitive stimuli coupled with reduced capacity to experience pleasure from natural rewards. With regard to obesity, this allostatic process of shifting reward thresholds may result in an attentional bias toward food cues13,14 and decreased sensitivity to nonfood natural rewards. 15 Decreased responsiveness to rewards has also been observed among cancer patients and may contribute to lower cancer-related quality of life.16,17
Appetitive dysregulation may encourage eating behaviors triggered by the sight of palatable food (ie, “external eating”), especially when exacerbated by the deficits in interoceptive awareness that prevent overweight and obese individuals from detecting signals of satiety that could otherwise be used to regulate food consumption. 18 The conceptual definitions of interoceptive awareness proposed by both Mehling et al 19 and Farb et al 20 integrate both metacognitive awareness of internal body signals and evaluative interpretation of those signals. In contrast to dysfunctional interoceptive awareness in obesity, adaptive interoceptive awareness involves attention to body sensations as a means of self-regulation, thereby facilitating disengagement from maladaptive cognitive and behavioral patterns. 21
To remediate deficits in appetitive regulation and interoceptive awareness, a therapeutic integration of mindfulness, cognitive reappraisal, and savoring techniques has been proposed.22,23 Specifically, mindfulness may be used to enhance both attentional control and interoceptive awareness.24,25 Disengagement of attention from appetitive cues coupled with awareness of interoceptive signals can then facilitate reappraisal—a reframing of the meaning of appetitive stimuli that can in turn increase contextually appropriate inhibitory control over urges. This process may then facilitate savoring, the practice of amplifying natural reward processing via intentionally focusing and sustaining attention on the sensory features of pleasant experiences (ie, visual, olfactory, gustatory, tactile, etc) as well as one’s positive affective and somatic response to that experience. 22 With regard to food-related reward, mindfulness training has been shown to increase food enjoyment and liking,26,27 which are in turn associated with increases in positive mood following eating 28 and reduced caloric consumption. 29 Such effects might be understood in light of the restructuring reward hypothesis, 22 which proposes that using mindfulness, reappraisal, savoring to increase the value of natural, healthy rewards will decrease the relative reward value of maladaptive appetitive stimuli, and thereby attenuate attentional bias toward those stimuli with consequent effects on decreasing addictive behavior. To the extent that obesity is driven by allostatic mechanisms, shifting valuation toward natural nonfood rewards and away from unhealthy, calorically dense food rewards may treat appetitive dysregulation underlying obesogenic behavior.
As such, this study pilot tested Mindfulness-Oriented Recovery Enhancement (MORE), 30 an integrative behavioral intervention designed to target mechanisms underlying appetitive dysregulation, as an added component to exercise and nutrition counseling for overweight or obese cancer survivors. MORE is unique among extant therapies in that it unites traditional mindfulness training with cognitive reappraisal and savoring strategies designed to reverse the allostatic shift in reward salience, which may in turn exert salutary effects on addictive behaviors and the neurobiological processes that drive them. 22 MORE has demonstrated therapeutic effects in disorders of appetitive dysregulation such as alcohol dependence, 31 illicit drug dependence, 32 opioid misuse, 33 nicotine addiction, 34 and internet gaming disorder. 35 In addition to its clinical outcomes, studies have revealed the mechanisms of MORE, including decreasing attentional bias to addiction-related cues 36 and increasing psychophysiological indices of natural reward responsivity33,34,37 that were in turn associated with decreases in craving and addictive behaviors. Although other mindfulness-based interventions have demonstrated efficacy for cancer survivors in meta-analyses,38,39 MORE has not yet been tested as an intervention for cancer survivors, nor has it been tested for obesogenic behaviors that confer risk of cancer recurrence.
The aims of this Stage I pilot randomized controlled trial (RCT) were the following: (1) to establish the feasibility of combining MORE with exercise and nutrition for overweight and obese cancer survivors; (2) to identify potential therapeutic mechanisms of the MORE intervention; and (3) to obtain effect sizes to power a subsequent Stage II trial. With regard to Aim 2, we hypothesized that adding MORE to an exercise and nutrition counseling program would result in significantly greater improvements in therapeutic mechanisms including interoceptive awareness, maladaptive eating styles, and savoring than exercise and nutrition counseling without MORE.
We also examined natural reward responsiveness and food attentional bias as potential psychophysiological mechanisms of the MORE intervention. Measuring sensitivity to appetitive food and nonfood natural rewards through self-report scales is prone to shortcomings, including social desirability bias and deficits in interoceptive awareness. 18 Appetitive response to both food and nonfood rewards may instead be objectively examined via attentional performance on cognitive tasks like the dot probe 40 and psychophysiological measures such as facial electromyography (EMG), which assesses emotional expressions based on the affective valence of sensory cues; zygomatic EMG activation, in particular, quantifies smiling in response to cues with positive affective valence. 41 Facial EMG indexes food palatability, 42 reward responsivity to positive food and nonfood stimuli among healthy controls, 43 and deficits in processing both food and nonfood rewards in individuals with eating disorders.44-46 Moreover, facial EMG in response to emotional stimuli discriminates obese from nonobese individuals.47,48 Thus, intervention-related changes in zygomatic EMG activation in response to rewarding stimuli may indicate remediation of the appetitive dysregulation that undergirds obesogenic behaviors in cancer survivors. As such, in accordance with the restructuring reward hypothesis, we hypothesized that boosting the salience of natural rewards (as measured by zygomatic EMG responses) through the mindful savoring techniques taught in MORE would attenuate the relative salience of appetitive cues and thereby mediate the effect of MORE on reducing food attentional bias.
Methods
Participants
Participants met study inclusion criteria if they were female, 18 years and older, English speaking, had a body mass index (BMI) ≥25 kg/m2, and had a history of a cancer diagnosis (active or in remission). Females were selected due to their heightened risk of cancer recurrence associated with being overweight or obese. Participants were excluded if they had prior experience with mindfulness training, current participation in a regular exercise program, unstable cardiac disease, presence of a clinically unstable systemic illness judged to interfere with treatment (determined by physician evaluation), substance dependence in the past year, psychotic disorders, and less than 90 days since surgery or radiation treatment. Participants were recruited between 2014 and 2015 through direct referrals from oncologists at the Huntsman Cancer Hospital and through flyers posted in the hospital. See Figure 1 for the CONSORT study flow diagram.

Flow diagram of the progress through the study.
Procedures
Following a preliminary phone screen, potential participants were screened for eligibility in person. Eligible, consenting participants reported demographics and completed self-report measures, as well as a dot-probe task, during which EMG data were collected via a Biopac MP150 data acquisition system (Biopac Systems, Goleta, CA). Following this assessment, participants were randomly allocated (1:1) via computerized random number generator to either a standard exercise and nutrition program offered at Huntsman Cancer Hospital called Personalized Optimism With Exercise Recovery (POWER) or MORE plus POWER (MORE POWER). The allocation list was stored in a protected file inaccessible to assessment personnel in order to ensure staff were blind to each participant’s group assignment. Participants were then assessed by a physician, dietician, and exercise specialist who evaluated various physical health metrics. After participants completed the 10-week POWER or MORE POWER intervention, they completed postintervention self-report and psychophysiological assessments. BMI, weight, and waist circumference were measured at a 3-month follow-up. Informed consent and study procedures were conducted in compliance with the authors’ institutional review boards and standards set forth by the Declaration of Helsinki. Participants were not compensated for study participation (Institutional Review Board#: 00069214, University of Utah).
POWER Intervention
The POWER program integrates dietary counseling, individualized exercise prescription, and self-monitoring. Over the 10-week intervention, participants received 2 exercise sessions a week directed by a cancer rehabilitation exercise specialist, as well as 4 sessions of nutrition counseling from a registered dietitian. Exercise sessions were an hour long and conducted in a group format in order to provide social support comparable to that provided by the MORE intervention.
MORE Intervention
MORE unites complementary aspects of mindfulness training, third-wave cognitive behavioral therapy, and principles from positive psychology into an integrative mind-body therapy. 30 MORE was originally developed to address substance use disorders, but for this study, the MORE manual was modified for treating maladaptive eating behaviors, exercise avoidance, and excess adiposity. Experiential exercises were also adapted to address cancer survivorship in order to enhance relatability to the target audience. MORE sessions involved mindfulness training to promote interoceptive awareness and increase control over appetitive automaticity; reappraisal training to promote negative emotion regulation; and savoring training to ameliorate reward processing deficits. MORE is typically conducted in weekly 2-hour sessions, but in order to match MORE to the established POWER program, session length was reduced to 1.5 hours; this reduction in length was achieved by abbreviating time spent in group processing. MORE sessions were administered by a Master’s-level licensed clinical social worker, who received intervention training and supervision directly from the developer of MORE. Each session was audio-recorded and reviewed by the last author to monitor therapist adherence to the modified treatment manual via a fidelity measure that specified both prescribed and proscribed therapist behaviors. Deviations from manualized treatment protocol were reviewed during weekly clinical supervision meetings and corrected by the therapist in subsequent sessions. No major deviations were noted, and minor deviations were observed infrequently, particularly as adherence improved over time.
Each MORE session included formal mindfulness meditation and experiential exercises, debriefing of those exercises, homework review, and weekly didactic material covering the following topics: gaining awareness of automatic habits via mindfulness; regulating negative emotions through mindful reappraisal; savoring pleasant experiences derived from nonfood rewards; regulating food craving through mindfulness; overcoming craving by coping with stress; promoting acceptance; awareness of impermanence; defusing relationship triggers; cultivating meaning in life; and developing a mindful recovery plan.
Measures
Feasibility
Data relating to recruitment (number of potential participants approached, excluded, and enrolled), treatment initiation, and retention (number of participants who withdrew, were lost to follow-up, and who provided data) were captured during the trial.
Body Composition
Registered dietitians assessed weight, waist circumference, and waist-to-hip ratio.
Eating Behaviors
The Dutch Eating Behavior Questionnaire (DEBQ), 49 a 33-item instrument, was developed to measure eating styles that may contribute to excess adiposity. All items are answered on a 5-point Likert-type scale (1 = Never, 5 = Very often). The DEBQ includes 3 subscales that were used to assess restrained (α = .89), emotional (α = .96), and external (α = .93) eating behavior.
Interoceptive Awareness
The Multidimensional Assessment of Interoceptive Awareness (MAIA) 19 is a 32-item multidimensional instrument that utilizes a 6-point Likert-type scale (0 = Never, 5 = Always) in order to assess 8 constructs: noticing (α = .76), not distracting (α = .88), attention regulation (α = .82), not worrying (α = .49), emotional awareness (α = .91), self-regulation (α = .67), body listening (α = .90), and trusting (α = .72).
Savoring
Savoring in the past week was measured with momentary savoring items from the Ways of Savoring Checklist. 50 The momentary savoring measure (α = .88) was composed of items asking to what extent in the participants tried to intensify their experience of pleasant events in the moment.
Food Attentional Bias
Attentional bias toward food cues was measured through the administration of a dot-probe task. This task was generated in E-Prime 2.0 (PST Inc, Pittsburgh, PA) and presented on a laboratory computer. During the task, which was composed of a block of 64 trials, each trial began with a fixation cross-presented for 500 ms. Participants were then presented with both food and neutral images selected from the International Affective Picture System. 51 Photos were matched for visual complexity, color, and figure-ground relationships and displayed side by side for either 50 or 2000 ms (with the brief latency to measure implicit initial attentional orienting and the longer latency to measure attentional disengagement). Food images included 12 photos of highly palatable foods (eg, pizza, hamburgers, ice cream), while the neutral images depicted common household items. Following each trial, a target probe replaced one of the images and was displayed for 100 ms, and participants were instructed to indicate the location of the probe on the screen with a left/right button press. Order and duration of cue presentation, as well as the left or right position of the images and target probe on the screen, was randomized and counterbalanced within and between each participant assessment.
Reward Responsiveness
Responsiveness to reward was measured with facial EMG using 2 surface 4 mm Ag/AgCl shielded electrodes with signal-conductive gel placed over zygomaticus major muscle regions, which produce smiling expressions. 52 Raw EMG signals were recorded continuously at 1000 Hz through a Biopac MP150 EMG100C EMG amplifier (Biopac Systems, Goleta, CA). Zygomatic activity during attention to rewards was monitored during the administration of a dot-probe task, also generated in E-Prime and structured identically to the food dot-probe task, but using images of nonfood natural rewards paired with neutral images all selected from International Affective Picture System. Nonfood natural reward images included smiling people, babies, intimate couples, and beautiful scenery; the same set of images has been used to assess the effects of MORE on reward responsiveness in other studies.33,37 Neutral pictures were matched to reward images in terms of visual complexity, color, human/nonhuman content, and figure-ground relationships. Images were displayed side by side for either 50 or 2000 ms across a single block of 64 trials. EMG responses were averaged over trials within the block.
Statistical Analyses
For food attentional bias data, trials with extreme response times (more than 3 SD above the individual mean) were discarded as outliers.53-55 Error trials were also discarded.53,54,56 Food attentional bias scores were calculated by subtracting their mean response time to probes replacing highly palatable food images from their mean response time to probes replacing neutral images. Positive bias scores indicated an attentional bias toward visual highly palatable food cues.
For reward responsiveness assessment, raw zygomatic EMG data were cleaned and average rectified offline. To remove noise unrelated to zygomatic activity, a band pass filter removed signals below 10 Hz and above 500 Hz, and a line frequency filter eliminated all 60 Hz signals associated with noise from AC current. 57 Average rectified EMG was derived via a time constant of 20 ms.
Intention-to-treat (ITT) analyses were conducted on the entire randomized sample (N = 51). In order to assess any significant differences between participants who dropped out and those who completed the study, independent t tests and χ2 test for independence were conducted, which revealed no significant differences between completers and noncompleters across demographic and physical health variables. Little’s MCAR (missing completely at random) test 58 was used to analyze patterns of missing data, which demonstrated that data were MCAR, therefore enabling maximum likelihood estimation to be employed to handle missing data. Per protocol analyses were conducted as secondary analyses on the sample of patients who had received the full intervention dose (N = 29). Maximum likelihood estimation procedures include data from all cases, included those measured at only one time point (eg, treatment noncompleters or nonstarters), reducing potential bias resulting from listwise deletion or last-observation carried forward techniques. Outcomes were analyzed using mixed effects linear models, treating study treatment and time (baseline vs post-intervention) as fixed effects, with the primary parameter of interest being the treatment × time interaction term.
Results
Participant Characteristics
Study participants were 51 adult women aged 29 to 76 years (mean [M] = 57.92, standard deviations [SD] = 10.04) with a mean BMI of 34.69 kg/m2 (SD = 7.39), mean weight of 208.17 (SD = 39.13), a mean waist circumference of 106.03 (SD = 14.85), and a mean waist-to-hip ratio of 0.90 (SD = 0.06). Most participants were White/Caucasian (96%), with 1 Black/African American and 1 Hispanic/Latino individual in the sample. The majority had a breast cancer diagnosis history (N = 45), due to direct involvement of breast cancer oncologists in the development of the study, while 6 participants had histories of varying types of cancers with associated obesity risks,59-64 including ovarian (N = 2), endometrial (N = 1), kidney (N = 1), colon (N = 1), and multiple myeloma (N = 1), who were primarily recruited through flyers posted in the wellness center. In the year prior to the study, 14% had a household income of < $25 000, 20% earned $25 000 to $49 999, 26% earned $50 000 to $74 999, 12% earned $75 000 to $99 999, and 28% earned $100 000 or more. At baseline, participants reported exercising an average of 2.0 (SD = 2.4) days per week, with 47.8% reporting no exercise, 30.4% reporting light-intensity exercise, 21.7% reporting moderate-intensity exercise, and no participants reporting high-intensity exercise. There were no significant baseline between-groups differences in cancer type, age, income, education, BMI, weight, or waist circumference, indicating that randomization was successful.
Feasibility
Of the 110 participants who were originally screened, 57 (52%) were excluded from participation due to a range of issues including BMI being too low (n = 3), no cancer diagnosis (n = 1), previous mindfulness experience (n = 2), medical complications related to cancer that prevented participation in a physical exercise program (n = 10), scheduling conflicts with study interventions (n = 21), geographic barriers (n = 8), and declined to participate or lost contact (n = 12). Of the 51 participants who were assessed and randomized to intervention conditions, 37 (73%) initiated the study interventions and attended one or more sessions, and 29 (79% of those who attended one or more sessions) completed the treatments. Four participants were lost to posttreatment assessment. The majority (77%) of nonstarters cited inability to meet the time commitment required by study involvement as a reason for their withdrawal from the study prior to the beginning of treatment. The remainder of the nonstarters withdrew due to unrelated medical issues that precluded their continued participation in the study. The treatment retention rate among starters was high, with 82% of those who began MORE receiving a full dose (N = 14; completed 7 or more sessions). Among control condition participants who started the POWER program, 75% also received a full dose (N = 15), demonstrating that the additive MORE component enhanced instead of detracting from retention rates despite the increased time commitment involved.
Therapeutic Mechanisms
Mixed effects linear models analyzed potential therapeutic mechanisms in the ITT sample (Table 1), and revealed significant time × treatment interaction on MAIA subscales related to noticing body sensations (F[1, 32.82] = 7.41, P = .01), attention regulation (F[1, 26.12] = 6.66, P = .02), self-regulation (F[1, 8.45] = 8.15, P = .006), and body listening (F[1, 31.49] = 14.78, P = .001), indicating that MORE POWER significantly increased several facets of interoceptive awareness to a greater extent than POWER alone. Significant time × treatment interactions were also observed for external eating (F[1, 38.93] = 6.80, P = .01) and savoring (F[1, 20.62] = 5.58, P = .03), indicating that MORE POWER resulted in larger improvements in these variables over time than POWER alone.
Intention-to-Treat Time and Time × Treatment Interactions.
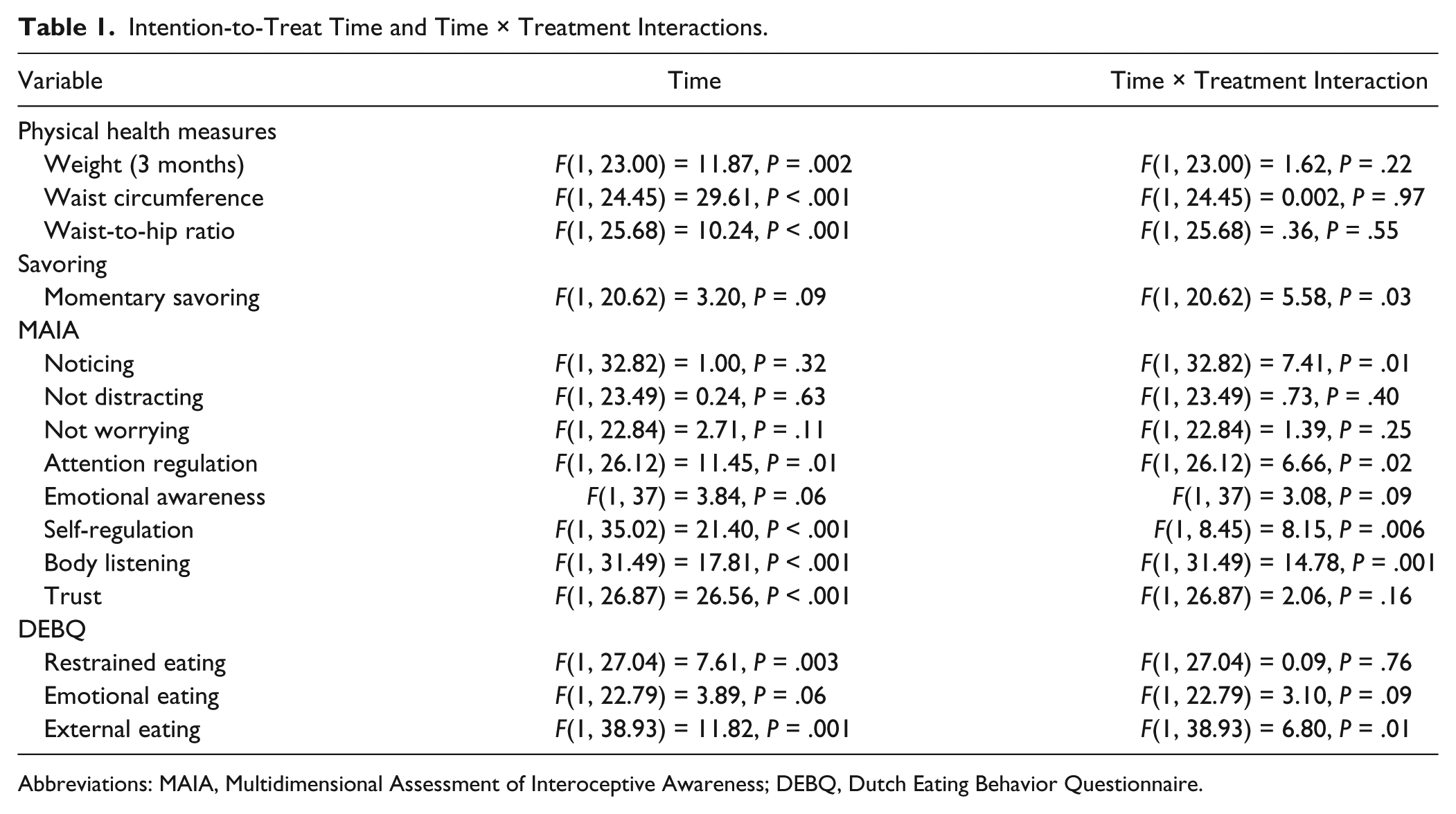
Abbreviations: MAIA, Multidimensional Assessment of Interoceptive Awareness; DEBQ, Dutch Eating Behavior Questionnaire.
With regard to effects on psychophysiological mechanisms, a significant time × treatment interaction was observed for smiling during attention to natural rewards, measured through zygomatic EMG (F[1, 29.56] = 5.56, P = .03), indicating that MORE POWER led to significantly greater increases in smiling to natural reward cues than POWER alone. Moreover, a significant time × treatment interaction was found on food attentional bias for cues presented for 50 ms (F[1, 28.09] = 12.21, P = .002), which indicated that MORE POWER significantly decreased attentional bias to food cues relative to POWER alone.
Secondary analyses of therapeutic mechanisms conducted on the per protocol sample also revealed significant time × treatment interaction on MAIA subscales related to noticing body sensations (F[1, 24.71] = 5.66, P = .03), self-regulation (F[1, 25.46] = 5.60, P = .03), and body listening (F[1, 26.03] = 14.12, P = .001), as well as momentary savoring (F[1, 22.22] = 5.77, P = .03). Significant time × treatment interactions were also observed for the same physiological mechanisms, including smiling during attention to natural rewards (F[1, 24.56] = 6.36, P = .02) and food attentional bias for cues presented for 50 ms (F[1, 28.86] = 7.99, P = .008), replicating findings from the ITT analyses.
Subsequent path analyses (Figure 2) conducted in AMOS 22.0 with Full Information Maximum Likelihood estimation tested whether the effects of MORE on reducing food attentional bias (the “C” path: β = −.51, P = .006) were mediated by increasing reward responsiveness. In this model, participation in MORE POWER was associated with increased zygomatic EMG during attention to natural rewards (the “A” path: β = .47, P = .02), and smiling was significantly associated with decreased food attentional bias (the “B” path: β = −.42, P = .04). After controlling for responsiveness to natural rewards, treatment was no longer a significant predictor of food attentional bias (“c”: β = −.31, P = .11)—suggesting the presence of mediation. Hayes’ PROCESS macro 65 was then used to test the bootstrapped indirect effect, which was significant as indicated by the confidence interval not spanning zero (B = −19.21, standard error = 13.38, confidence interval = −49.70 to −.16).
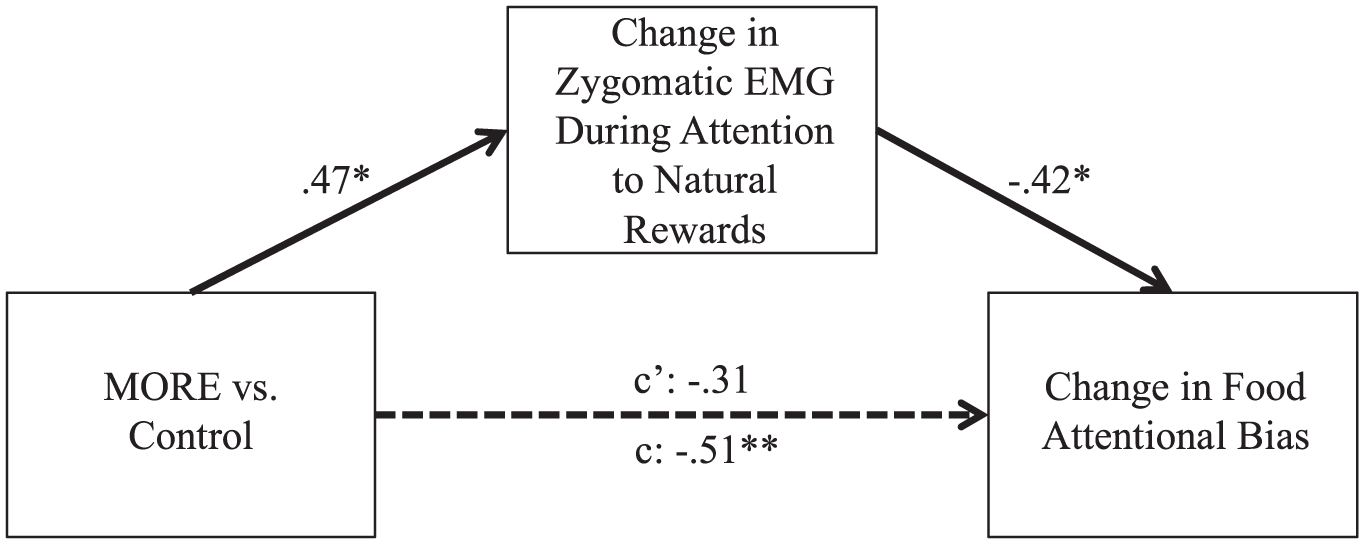
Path analysis demonstrating that change in zygomatic electromyography (EMG) mediates the effect of Mindfulness-Oriented Recovery Enhancement (MORE) on food attentional bias. Numbers represent standardized β coefficients.
To determine the preliminary clinical significance of this mediational finding using an experimental medicine approach to assessing behavior change, 66 we examined associations between changes in the mechanistic intervention target (food attentional bias) and obesity outcomes. After adjusting for pretreatment weight and waist-to-hip ratio, decreases in food attentional bias were significantly associated with lower waist-to-hip ratio at posttreatment (β = .28, P = .01).
Effect Size Estimation of Treatment Effects to Power a Subsequent Trial
Participants in the MORE POWER condition showed statistically significant improvements and large effect sizes on several therapeutic mechanisms (Table 2), including the MAIA subscales of attention regulation (Mdiff = 0.81, SDdiff = 0.57, P < .01, D = 0.88), emotional awareness (Mdiff = 0.76, SDdiff = 0.54, P < .001, D = 0.97), self-regulation (Mdiff = 1.09, SDdiff = 0.59, P < .001, D = 1.20), body listening (Mdiff = 1.65, SDdiff = 0.49, P < .001, D = 1.50), and trust (Mdiff = 0.76, SDdiff = 0.54, P < .01, D = 0.80), while POWER only participants showed no statistically significant improvement in interoceptive awareness. MORE POWER participants also showed statistically significant decreases in emotional (Mdiff = −6.61, SDdiff = 4.82, P = .02, D = −0.68) and external eating (Mdiff = −5.57, SDdiff = 3.94, P < .001, D = −1.27), as well as statistically significant improvements in savoring (Mdiff = 1.76, SDdiff = 1.24, P = .02, D = 0.67). While the study was not powered to detect group differences in weight loss outcomes, both MORE POWER and POWER conditions showed significant weight loss at 3 months follow-up (M weight loss = 9.85; F[1, 23] = 11.87, P = .002). Although there were no between-groups differences in changes in waist-to-hip ratio by 3-month follow-up, only the MORE POWER intervention group evidenced statistically significant decreases in waist-to-hip ratio from pre- to posttreatment (Mdiff = −0.06, SDdiff = 0.01, P = .04, D = −1.33).
Primary and Secondary Outcomes: Within-Group Analyses a .

Abbreviations: ES, within-group effect size (Cohen’s D); MAIA, Multidimensional Assessment of Interoceptive Awareness; DEBQ, Dutch Eating Behavior Questionnaire.
Data are given as mean (standard deviation).
Conclusion
This Stage 1 RCT demonstrated the feasibility of integrating a mindfulness-based therapy, MORE, into an exercise and nutrition program for overweight and obese cancer survivors, as evidenced by a substantial number of eligible participants initiating and being retained in the combined mind-body intervention. Given the well-known difficulty of recruiting and retaining cancer survivors in behavioral intervention studies, 67 interest in participating in the current study interventions was moderately high, demonstrated by the fact that we recruited the target sample size in less than a year and <11% of participants declined to participate or maintain contact with study staff. Yet, barriers including scheduling conflicts, geographic distance, and medical complications precluding participation revealed key challenges in deploying group-based behavioral interventions for a cancer survivor population. Beyond issues of feasibility, the present study also identified therapeutic mechanisms of MORE, showing that the adding MORE to an exercise and nutrition program significantly improved cognitive and affective factors related to underlying mechanisms of appetitive dysregulation and obesogenic behaviors.
Notably, MORE significantly decreased attentional bias toward food cue, and reduced self-reports of externally cued eating behaviors. Although we did not examine the neural correlates of this effect, decreases in attention to calorie-dense food stimuli might be associated with reduced activation in brain regions associated with food reward—a finding observed in a functional magnetic resonance imaging (fMRI) pilot study of obese cancer patients participating in a behavioral lifestyle intervention. 68 Taken together with data from previous studies demonstrating significant effects of MORE on attentional biases31,36 and neural responses to addiction-related stimuli, 34 the present findings suggest that MORE may reduce the extent to which individuals are “triggered” to engage in appetitive behavior. It should be noted that effects were observed on dot-probe trials when food cues were presented for 50 ms, suggesting that MORE may reduce automatic attentional orienting to palatable food stimuli. In the present study, decreases in food attentional bias were significantly associated with improvements in waist-to-hip ratio, a marker of visceral adiposity that has been shown to predict cancer risk 69 and mortality. 70 Hypothetically, patients in the MORE POWER intervention whose attention became less biased toward the sight of palatable food stimuli may have been better able to reduce their consumption of calorie dense foods, resulting in decreases in abdominal obesity that might ultimately be protective against cancer recurrence.
In addition, MORE significantly increased the self-reported capacity to savor positive experiences and heightened zygomatic EMG responses (eg, smiling) to natural nonfood rewards—replicating previously demonstrated effects of MORE on increasing autonomic, 37 EEG, 33 and fMRI 34 indices of natural reward processing. In these three prior studies, increased physiological indices of natural reward processing were associated with decreases in craving and/or consumption of addictive substances. Recently, in a sample of chronic opioid users, MORE was found to increase cardiovascular responsiveness to cues representing natural rewards relative to drug-related reward cues, with this shift in relative reward responsiveness predicting clinically significant decreases in opioid misuse. 71 Data from the present study parallel these earlier results by demonstrating that increases in EMG indices of natural reward responsiveness mediated the effects of MORE on decreasing the food attentional bias, suggesting that MORE may indeed modify associative learning mechanisms by strengthening cognitive control functions to restructure the relative salience of food and nonfood rewards in line with goal states (e.g., weight loss and overall health promotion). Taken together with these earlier results, the current mediational finding provides evidence for the reward restructuring hypothesis 22 by suggesting that amplifying responsivity to natural rewards may attenuate the relative value of appetitive cues (manifested in the present study by a decrease in food attentional bias), and thereby potentially decrease addictive behavior.
In the present trial, MORE was also associated with significant improvements in self-reported interoceptive awareness, a mechanism that may prevent overeating in the face of ubiquitous encounters with appetitive cues in the obesogenic sociocultural environment.18,72 By noticing body sensations via mindfulness techniques, individuals may become more attuned to interoceptive signals of hunger and satiety. Furthermore, the ability to self-regulate by mindfully attending to body sensations might provide a means of coping with food craving. Also, given that interoceptive brain activity has been shown to be dysregulated among breast cancer patients experiencing chemotherapy-induced peripheral neuropathy, 73 the effects of MORE on enhancing interoceptive awareness may be especially beneficial for cancer survivors. To be clear, the observed effects were on self-reported interoceptive capacity. Future studies should examine the effects of MORE on performance-based measures of interoception (e.g., heartbeat detection tasks, testing of gastric capacity thresholds) 74 to determine if increasing awareness of the physiological condition of the body can confer benefits for healthy eating.
The primary limitation of the present study relates to the measurement of weight-related outcomes in a sample of cancer survivors, which is challenging given the potential long-term effects of therapies including surgery, radiation, chemotherapy, and hormone modulation on fatigue, reduced mobility, loss of lean muscle mass, and increased adiposity. 75 Future studies should control for individual differences in cancer disease progression and cancer treatment due to their potential to confound accurate measures of weight-related outcomes; unfortunately, we were unable to control for these variables as covariates in the present pilot study due to the modest sample size. Also, the present study was limited by the body composition measures utilized, which could not accurately differentiate changes in fat versus muscle tissue. Future studies should include more reliable, objective measures of fat and fat-free mass, such as dual-energy X-ray absorptiometry analysis. The effects of MORE on weight loss should also be investigated in overweight and obese participant samples without cancer, where measurement of adiposity is uncomplicated by the many potential confounders introduced by cancer and cancer treatment. In addition, given the pilot nature of this trial, the sample size does not provide optimal statistical power. However, the purpose of the present study was to obtain effect sizes to inform an optimally powered clinical trial. Larger and more ethnically/racially diverse samples composed of patients with a wider array of diagnoses would enhance the generalizability of future studies. In that regard, there was some cultural bias in the food dot-probe task, in that the food images presented might not be salient to other cultural groups, and thus expanding the diversity of the sample might require modification of food stimuli used in the task. It should be acknowledged that there were a number of attriters and nonstarters in the study, which may be due in part to the unstable health of recent cancer survivors. The study was also limited by the lack of follow-up data across all variables, which precludes an understanding of the duration of treatment effects, as well as a lack of process data including daily mindfulness practice, home exercise, and nutrition, all of which likely influenced intervention effects. Unfortunately, due to the absence of these data, we do not know to what extent the addition of MORE led to changes in diet and exercise patterns. Future efficacy tests of MORE for more diverse samples of overweight and obese individuals should employ full-scale RCTs with longitudinal assessment of clinical outcomes and process variables including daily measures of mindfulness practice, home exercise, and nutrition.
In conclusion, study results indicate that although adding MORE to an exercise and nutrition program did not significantly improve weight loss among cancer survivors, the mindfulness, reappraisal, and savoring skills taught in this integrative intervention may modulate mechanisms implicated in obesogenic behaviors, including interoceptive awareness, attentional bias, and natural reward responsiveness. Whether changes in these mechanisms are necessary or sufficient for clinically significant weight loss in this population is as yet unknown. Findings from this early stage pilot RCT suggest that MORE may have promise for targeting the appetitive dysregulation underlying loss of control over eating and excess adiposity, which might reduce risk for cancer-related morbidity and mortality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Eric L. Garland was supported by NIDA Grant R01DA042033 and NCCIH Grant R61AT009296 during the preparation of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.