
Abstract
Objective
Alexithymia, characterized by difficulty identifying and describing feelings, coupled with an externally-oriented thinking style, is a transdiagnostic trait associated with various disorders. Despite its prevalence, targeted interventions remain limited. This study developed a digital intervention tool for alexithymia based on an affective process framework and evaluated its effectiveness in improving alexithymic symptoms through a randomized controlled trial, thereby filling a gap in the existing study.
Methods
Functional impairments were analyzed across four key stages of emotional processing, leading to the identification of core components: attention bias modification (ABM), mindfulness training, vocabulary training, and expressive writing exercises. A user-friendly digital tool incorporating these elements was designed and tested.
Results
A randomized controlled trial (n = 47, TAS-20 ≥ 61) demonstrated that the experimental group experienced a significant reduction in TAS-20 scores compared to the control group. Furthermore, improvements were observed in measures of depression, anxiety, stress, mindfulness, emotional differentiation, and overall emotional processing. Importantly, improvements in emotional well-being were correlated with engagement in the training process, and user evaluations of the program were highly positive.
Conclusion
These results support the efficacy of the digital intervention in enhancing emotional abilities and mitigating alexithymia, offering a scalable and accessible solution for individuals struggling with this condition.
Keywords
1. Introduction
Alexithymia is a personality construct affecting approximately 10-15% of the general population 1 and a significantly higher percentage of clinical samples, for example, approximately 50% of individuals with ASD present with alexithymic features,2,3 and this prevalence rate is about 35% in patients with schizophrenia. 4 Epidemiological evidence consistently demonstrates that alexithymia is not only common but also systematically elevated in groups with emotional and psychiatric disorders, suggesting its potential role as a broad vulnerability factor across diagnostic categories. It is characterized by a constellation of difficulties: struggling to identify and describe feelings, coupled with a predominantly externally-oriented thinking style. 5 Recent research on mood disorders further supports this perspective, showing that multiple facets of alexithymia are significantly associated with symptoms of depression, anxiety, and stress, collectively accounting for approximately 14.6% to 16.4% of the variance in these symptoms. Moreover, different dimensions of alexithymia exhibit distinct patterns of association with various psychopathological features. 6 These findings reinforce the view that alexithymia is not limited to deficits in processing negative emotions but instead reflects a broader disruption in affective processing. This seemingly simple deficit has profound implications, acting as a transdiagnostic factor implicated in a wide array of physical and mental disorders, including depression, anxiety, substance use disorders, and chronic pain. 7 Beyond diagnostic categories, individuals with alexithymia often experience significant impairments in social functioning, a diminished quality of life, and demonstrably poorer outcomes in therapeutic settings, highlighting the urgent need for effective interventions. 8
While previous research has largely focused on the structural components of alexithymia, such as Difficulty Identifying Feelings (DIF) and Difficulty Describing Feelings (DDF), 9 a process-oriented approach is increasingly recognized as crucial for developing targeted interventions. This perspective emphasizes the dynamic nature of emotional processing, moving beyond static descriptions to explore the underlying mechanisms that contribute to alexithymia. Influential models, such as Preece et al. (2017)’s attention-appraisal model 10 and Smith et al. (2019)’s three-process model (encompassing affective reaction generation, representation, and cognitive control), 11 underscore the importance of understanding how emotions are processed, or not processed, in individuals with alexithymia. Accumulating empirical evidence, particularly regarding the associations between alexithymia, diminished arousal, and impaired interoception/regulation, underscores the presence of aberrant emotional processing across critical stages, including attentional allocation, conscious awareness, evaluative appraisal, and expressive articulation. 12 These processing anomalies offer crucial insights for the development of targeted, mechanism-based interventions. 13
At the attention stage, individuals with alexithymia often exhibit insufficient attention to emotional information.14,15 This can manifest as an attentional deficit, where emotional cues are simply missed or go unnoticed, 16 or as a defensive avoidance of emotional stimuli, potentially serving as a maladaptive coping mechanism to manage overwhelming or difficult emotions.12,17 In either case, the result is a reduced focus on emotions, hindering subsequent processing. Promising interventions for this stage include Attention Bias Modification (ABM) training, which aims to modulate attentional biases through probabilistic manipulation of cue-probe pairings with emotional faces, thereby facilitating top-down attentional control. 18 Although the ABM paradigm typically involves external emotional stimuli, its therapeutic efficacy hinges on top-down attentional control and the indirect modulation of the default mode network (DMN), 19 which in turn may influence interoception—a process central to alexithymia. Individuals with alexithymia often exhibit impairments in emotional self-awareness, which have been linked to reduced functional connectivity within DMN regions involved in self-referential processing, such as the medial prefrontal cortex. 20 By training individuals to allocate attentional resources toward external emotional cues, Attention Bias Modification (ABM) training can strengthen the cognitive control network. This improvement in attentional control may generalize to internal processing, potentially enhancing interoceptive awareness in individuals with alexithymia. Although clinical applications remain relatively limited, the theoretical translatability of attention bias training to alexithymia, coupled with its ease of digitalization, 21 offers a direct impetus for interventions targeting attentional processes in this population.
The awareness stage in alexithymia is characterized by functional deficits in sensing and experiencing emotions. This often stems from insufficient arousal in response to emotional stimuli11,22 and impaired interoceptive awareness23,24 – the ability to accurately perceive and interpret internal bodily sensations.25,26 This impairment means individuals struggle to accurately detect and interpret the internal body signals that are intrinsically linked to emotional experience. 27 Strategies focusing on enhancing interoception are therefore critical. Mindfulness-based interventions, emphasizing non-judgmental awareness of bodily sensations, particularly internal cues, have amassed considerable evidence supporting their efficacy in enhancing interoceptive abilities. 28 Within alexithymia treatment, mindfulness training is a mainstream and demonstrably successful approach, 29 with its mechanisms of action frequently linked to improvements in interoception and emotional awareness.30,31 Notably, online mindfulness practices have yielded non-inferior outcomes compared to traditional therapy, 32 making the integration of interoceptive mindfulness exercises into comprehensive digital interventions both necessary and highly feasible.
The evaluative stage encompasses the intertwined processes of appraising emotions and responding to them. In alexithymia, this stage is characterized by a tendency to rate both positive and negative emotions more neutrally, reflecting a fundamental difficulty in appraising the significance and meaning of emotional experiences. 12 Research consistently highlights aberrant emotional regulation, particularly within the appraisal process, in individuals with alexithymia.33–35 This impaired appraisal is often linked to undifferentiated emotional schemas, leading to a generalized sense of distress and difficulty in identifying specific emotions.36–38 Consequently, psychotherapies, such as Cognitive Behavioral Therapy, Emotional Schema Therapy, and Gestalt therapy, have focused on targeting emotional regulation processes in alexithymia, showing promise in improving emotional regulation and modifying maladaptive emotional patterns. 39 Expressive writing provides a versatile framework for integrating therapeutic elements, facilitating emotional reappraisal, catharsis, and sublimation in individuals with alexithymia.40,41 Consequently, integrated interventions combining expressive writing with established psychotherapeutic techniques are undoubtedly crucial.40,41
The accurate identification and articulation of emotions in alexithymia is significantly impacted by insufficient emotional granularity – the ability to precisely differentiate/describe between emotional experiences. 42 This is further compounded by impaired language function, which is believed to hinder the development and representation of discrete emotional concepts,7,43,44 thereby making it difficult to label, understand, and communicate emotional nuances. They may also employ defensive responses to intense emotions, such as avoidance and suppression, which can paradoxically exacerbate their distress.45,46 Therefore, targeted interventions, in addition to the expressive writing techniques previously discussed, should also focus on cultivating basic emotional vocabulary and expressive skills in individuals with alexithymia. Research suggests that emotional vocabulary learning and enriched emotionally-situational knowledge instruction can improve emotional granularity,47–49 initiating a positive feedback loop that enhances emotional percepetion and experience. 50 Consequently, these elements should be integrated into the overall intervention framework.
While research on interventions for alexithymia is relatively rich, encompassing various therapeutic approaches and techniques—including psychodynamic therapy,51,52 Cognitive Behavioral Therapy, 53 mindfulness-based programs,29,54 and expressive writing or related modalities55,56—these approaches remain focused on traditional methods and often lacks a cohesive, integrated approach. Their effectiveness is further limited by the high comorbidity of alexithymia, which can reduce treatment responsiveness across disorders, 13 and by the fact that many interventions focus on the comorbid condition rather than directly targeting core emotional processing deficits. Although these traditional approaches can reduce alexithymia severity—with studies reporting significant post-treatment declines 57 — several limitations remain: a lack of personalization, 52 reliance on one modality, 58 limited theoretical specificity in multimodal programs, 59 and barriers related to cost and accessibility in clinician-delivered treatments. 57 These shortcomings align with broader critiques that disorder-specific, manualized treatments are often too rigid and insufficiently mechanism-focused. Accordingly, Hofmann and Hayes (2018) advocate for a process-based therapy framework that prioritizes empirically validated mechanisms of change. 60 Therefore, understanding the process-level abnormalities is crucial for developing targeted interventions. By addressing specific impairments — improving attentional allocation on emotions, enhancing interoceptive awareness, refining emotional appraisal through schema-focused and cognitive restructuring, and facilitating emotional expression and articulation — we can foster more effective emotional processing in individuals with alexithymia. Therefore, integrated, process-oriented interventions are essential for effectively addressing the multifaceted nature of this condition.
Moreover, the integration of digital technologies offers a promising avenue for enhancing the accessibility and scalability of these interventions. Digital interventions offer a promising avenue for addressing mental health concerns due to their accessibility, affordability, and potential for widespread dissemination. 61 With the widespread adoption of smartphones and the internet, digital intervention tools have demonstrated significant efficacy in the realm of emotional disorders, such as anxiety and depression. 62 Their core advantages lie in overcoming spatiotemporal limitations, reducing perceived mental health stigma, and enhancing service accessibility, thereby offering convenience to individuals unable to receive traditional face-to-face treatment. 63 Furthermore, digital interventions can be easily tailored to individual needs and preferences, potentially enhancing engagement and adherence. 64
This study aimed to develop and validate a comprehensive digital intervention for alexithymia, grounded in an affective process framework. Specifically, the research will first involve designing and developing a user-friendly digital intervention tool that incorporates evidence-based techniques targeting these core processs such as emotional identification, processing, and expression, and will ultimately comprise four distinct intervention modules: Attention, Awareness, Evaluation, and Articulation; Subsequently, we will empoly a randomized controlled trial design to systematically examine the effectiveness of the digital intervention in reducing alexithymia symptoms and improving related outcomes, including emotion regulation capacity and quality of life. By adopting a mechanism-based approach and leveraging the potential of digital technology, this study seeks to contribute to the development of more effective and accessible interventions for alexithymia.
2. Methods
2.1. Digital intervention for alexithymia: Software overview
This digital intervention for alexithymia was developed using a process-oriented approach, including needs analysis, module design, technical implementation, testing & optimization, and deployment & maintenance. The development was guided by implication-drived emotional processing model (Attention - Awareness – Evaluation- Articulation) and informed by user interviews and expert feedback. The goal was to translate evidence-based techniques into engaging digital experiences. Godot 4.0 was selected for core functionality integration. Its 2D/3D rendering pipelines and audio management system facilitated cross-platform adaptation of key intervention components. This intervention is compatible across Windows, macOS, and Android/iPadOS platforms.
The digital intervention tool comprises four core modules, each targeting a specific stage of emotional processing:
The program interface follows a sequential and modular design. Screenshots of the main functional modules can be seen in Figure 1. This software is currently in the prototype stage (only support simply Chinese)and can be downloaded from https://xinglikeji.itch.io/yjqd. To obtain access and usage rights, please contact the author to request a “license.” Four core modules of the digital intervention for alexithymia.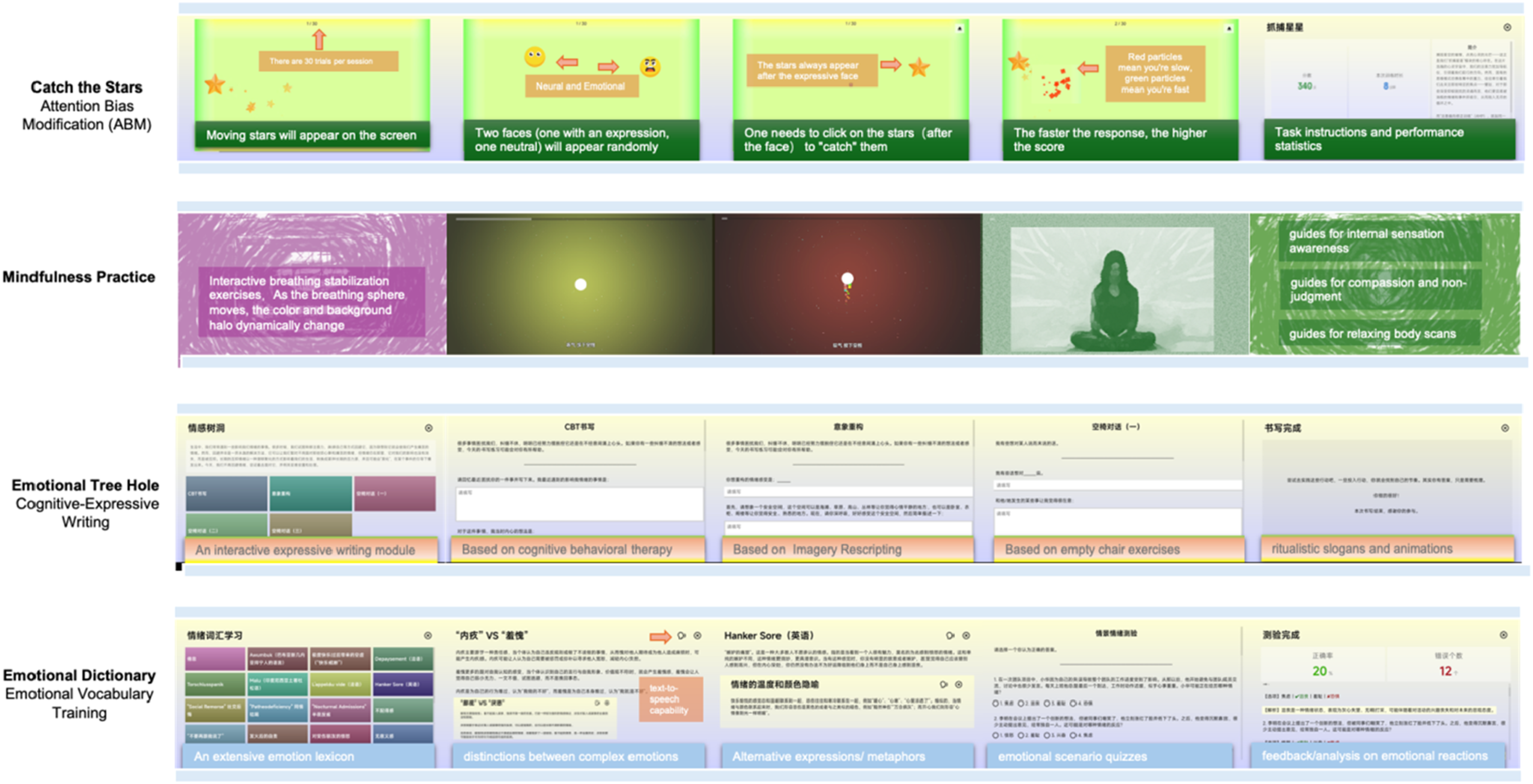
2.2. Participants
Participants scoring high on alexithymia measures (TAS-20 ≥ 61) were recruited through online advertisements and community outreach. All participants were from China. Inclusion criteria required participants to be between 18 and 65 years of age, score 61 or higher on the TAS-20, individuals experiencing subjective emotional distress who are seeking help and possess access to a smartphone or computer with internet connectivity. Exclusion criteria encompassed a history of severe mental illness (e.g., psychosis, bipolar disorder), a history of cognitive impairment, and current engagement in psychotherapy or use of psychiatric medication.
A power analysis was conducted to determine the minimum sample size needed to detect a statistically significant effect. We referred to a recent systematic review of psychological treatments for alexithymia, which reported within-group pre–post effect sizes quantified as Cohen’s d (Hedges’g) ranging from 0.41 to 13.25 (median = 1.42). 39 These unusually large values reflect the use of within-group effect size calculations based on raw pre–post changes in small samples across highly heterogeneous interventions. To adopt a conservative and realistic estimate for our planned between-group comparisons, we also considered meta-analyses of digital mental health interventions for emotional symptom improvement, which showed smaller effect sizes (g = 0.52 - 0.75).65,66 Based on these sources, we anticipated a Cohen’s d of 1.0 for our primary outcome (representing a slightly smaller effect than the median observed in traditional alexithymia interventions). With a two-tailed alpha of 0.05 and a power of 0.95, the analysis indicated a minimum of 27 participants per group. Based on an estimated alexithymia prevalence of at least 10% in the general population, we initially screened 540 individuals through online questionnaires and community outreach, and selected those with alexithymia who expressed interest in participating in the intervention. After applying inclusion and exclusion criteria, 47 eligible participants were ultimately selected. Given the long duration of the intervention cycle and anticipating a potentially attrition rate in the experimental group, the sample size for the experimental group was intentionally allocated to be larger than that of the control group. Consequently, the 47 participants were assigned to the experimental (n = 25) or control (n = 22) group using a computer-generated sequence. Although the final sample size was slightly below the initial target, the achieved power remained sufficient to detect a medium effect.
The study protocol was approved by the Institutional Review Board (IRB) of Beijing Language and Culture University (reference number: 2024BYLL50). Written informed consent was obtained from all participants prior to study initiation. As this project was designed as a preliminary pilot study conducted in a non-clinical university setting and did not involve medical treatments or health-related clinical endpoints, it did not fall under the categories requiring registration on ClinicalTrials.gov (NCT). Therefore, no NCT registration was obtained. Following the study, participants in the control group were offered the opportunity to participate in the intervention program. All participants received course credit or a monetary incentive for their participation.
2.3. Measures
2.3.1. Toronto Alexithymia scale (TAS-20)
A 20-item self-report questionnaire measuring alexithymia in Chinese. 67 The scale uses a 5-point Likert scale for scoring, where 1= strongly disagree and 5= strongly agree. Five items are reverse-scored (Items 4, 5, 10, 18, and 19). The TAS-20 consists of three subscales: Difficulty Identifying Feelings (DIF), Difficulty Describing Feelings (DDF), and Externally Oriented Thinking (EOT). The total alexithymia score is the sum of responses to all 20 items, while the score for each subscale factor is the sum of the responses for that specific subscale. The TAS-20 uses the following cut-off scores: a score of ≤ 51 indicates non-alexithymia, a score of ≥ 61 indicates alexithymia, and scores between 52 and 60 suggest possible alexithymia. 68
2.3.2. Depression Anxiety Stress Scales (DASS-21)
A 21-item self-report questionnaire measuring symptoms of depression, anxiety, and stress. 69 The DASS-21 consists of three subscales: Depression, Anxiety, and Stress.
2.3.3. Five Facet Mindfulness Questionnaire (FFMQ-15)
A self-report questionnaire measuring five facets of mindfulness: Observing, Describing, Acting with Awareness, Non-Judging of Inner Experience, and Non-Reactivity to Inner Experience. 70 This study used a 15-item abbreviated version. 71 Elevated scores are indicative of increased emotional granularity.
2.3.4. Range and Differentiation of Emotion Evaluation Scale (RDEES)
A 14-item self-report questionnaire measuring the range and differentiation of emotional experiences. 72
2.3.5. Emotional Processing Scale (EPS)
A 25-item self-report questionnaire measuring difficulties in emotional processing. 73 The total score indicates the severity of emotional processing deficits; higher scores reflect greater impairment.
2.3.6. Demographic questionnaire
A self-developed questionnaire was administered in both the pre-test and post-test to collect participants’ demographic information, including age, gender, and educational level.
2.3.7. Digital intervention user experience questionnaire
A self-developed questionnaire was used in the post-test to assess participants’ feedback on their experience with the digital intervention tool. The questionnaire included the following components: user involvement (rated on a 0–100 scale, with higher scores indicating greater involvement); tool operability (rated on a 9-point scale, with higher scores indicating better operability); emotional experience during use (rated on a 10-point scale, where 0 indicates “very unpleasant” and 10 indicates “very pleasant”); and willingness to recommend (binary scoring: 0 = unwilling to recommend, 1 = willing to recommend), which assessed whether participants would recommend the tool to others.
2.4. Procedure
Prior to the intervention, all participants completed a battery of baseline assessments, including the TAS-20, DASS-21, FFMQ-15, RDEES, and EPS. Following baseline assessment, participants were randomly assigned to either the experimental or control group.
Intervention protocol for two weeks.

The digital intervention tool consists of four core exercise modules, designed to be completed in a structured manner. The estimated completion time for each module is as follows: • “Catch the Stars” (Attention Bias Modification Training): 3-5 minutes per session (30 trials) • Mindfulness Practice (11 Guided Audio Meditations): Approximately 10 minutes per session • Emotional Vocabulary Learning (30 Emotional Terms, 15 Scenario-Based Quizzes): Approximately 3 minutes • Cognitive-Expressive Writing (Cognitive Behavioral Therapy Writing, Imagery Rescripting, Empty Chair Techniques): Approximately 10 minutes per session
The 14-day training program incorporated these modules into daily sessions lasting approximately 15 -20 minutes per day. The specific schedule for each week is detailed Table 1 above
Following the 14-day intervention period, all participants, in both the experimental and control groups, completed the same assessments administered at baseline.
2.5. Data analysis
The trial was open-label for participants due to the nature of the behavioral intervention. However, the researchers performing the data analysis were blinded to the group allocation until the primary analyses were completed. Data were analyzed using SPSS version 26.0 and phthon for the visualization. Repeated measures ANOVA was used to examine the effects of the digital intervention on alexithymia symptoms and related measures. The Greenhouse-Geisser correction was applied when the assumption of sphericity was violated. Post-hoc analyses were conducted using Bonferroni corrections to adjust for multiple comparisons. Effect sizes were calculated using partial eta squared (η 2 p ).
2.6. Transparency and openness
This study prioritizes transparency and reproducibility, adhering to the TOP Guidelines. We achieved Level 2 for Data, Materials, and Code Transparency, and Level 1 for Preregistration. Data, materials, and analysis code are available on the Open Science Framework (OSF): [https://osf.io/nvdah/?view_only=8536e56324cc4569846a276e2f440752]. While we aimed for full data sharing, privacy restrictions prevent public access to the raw dataset. However, a de-identified subset will be available upon request and ethical approval.
3. Results
3.1. Demographic characteristics
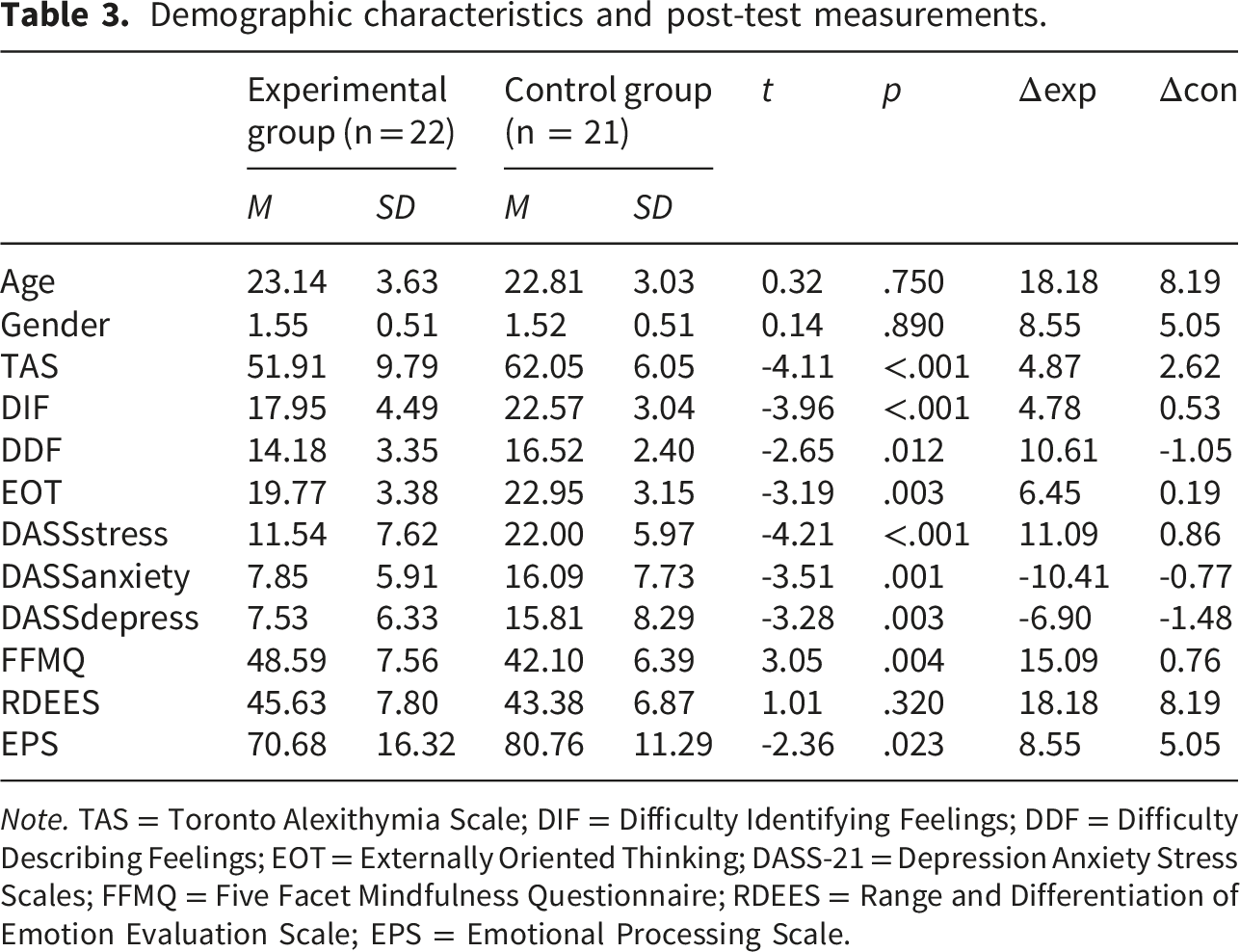
During the course of the study, three participants were lost from the Experimental Group (equipment issues, scheduling conflicts, concerns over compensation) and one participant was lost from the Control Group (lack of response following contact). Consequently, the final sample for data analysis comprised 43 valid datasets (see Figure 2). The experimental group consisted of 22 participants (mean age = 23.14 years, SD = 3.63; 10 female, 12 male), while the control group comprised 21 participants (mean age = 22.81 years, SD = 3.03; 10 female, 11 male). No significant differences were found between the two groups in terms of age or gender distribution (p > .005). Furthermore, there were no significant baseline differences between the groups in alexithymia symptoms or emotional state (p > .005). Descriptive statistics are presented in Tables 2 and 3. CONSORT flow diagram of study participants. Note. The diagram illustrates the number of participants assessed for eligibility, randomly assigned to each study condition, receiving or discontinuing the allocated intervention, lost to follow-up, and included in the final primary outcome analysis. Demographic characteristics and baseline measurements. Demographic characteristics and post-test measurements. Note. TAS = Toronto Alexithymia Scale; DIF = Difficulty Identifying Feelings; DDF = Difficulty Describing Feelings; EOT = Externally Oriented Thinking; DASS-21 = Depression Anxiety Stress Scales; FFMQ = Five Facet Mindfulness Questionnaire; RDEES = Range and Differentiation of Emotion Evaluation Scale; EPS = Emotional Processing Scale.

3.2. Primary outcomes: Impact on alexithymia symptoms
A significant time × group interaction was found for TAS-20 scores (F (1, 41) = 15.14, p < .001, η
2
p
= 0.27, large effect), with the experimental group showing a significant decrease from baseline (M = 70.09, SD = 5.50) to post-intervention (M = 51.91, SD = 9.79), p < 0.001, while the control group did not (p > .05). Significant time × group interactions were also present for the TAS-20 subscales: DIF, DDF, and EOT [F (1, 41) = 6.00,p = .019, η
2
p
= 0.13 (large effect), F (1, 41) = 5.64, p = .022, η
2
p
= 0.12 (large effect),F (1, 41) = 13.93,p = .001, η
2
p
= 0.25 (large effect), respectively], indicating that the intervention improved emotion identification and description, and reduced externally-oriented thinking. The effect was most pronounced for EOT (p = .001); see Figure 3 for the changing details. Alexithymia symptoms changes before and after training.
3.3. Secondary outcomes: DASS-21, FFMQ, RDEES and EPS
Significant time × group interactions were also observed for DASS-21 scores, F (1, 41) = 26.59, p < .001, η
2
p
= 0.39 (large effect); FFMQ scores, F (1, 41) = 22.41, p < .001, η
2
= 0.35 (large effect); RDEES scores, F (1, 41) = 6.21, p = .017, η
2
p
= 0.13 (large effect); and EPS scores, F (1, 41) = 14.05, p = .001, η
2
= 0.26 (large effect). Post-hoc analyses indicated that the experimental group showed significant improvements in depression, anxiety, stress, mindfulness, emotional differentiation, and emotional processing compared to the control group (see Figure 4). Secondary outcome changes before and after training.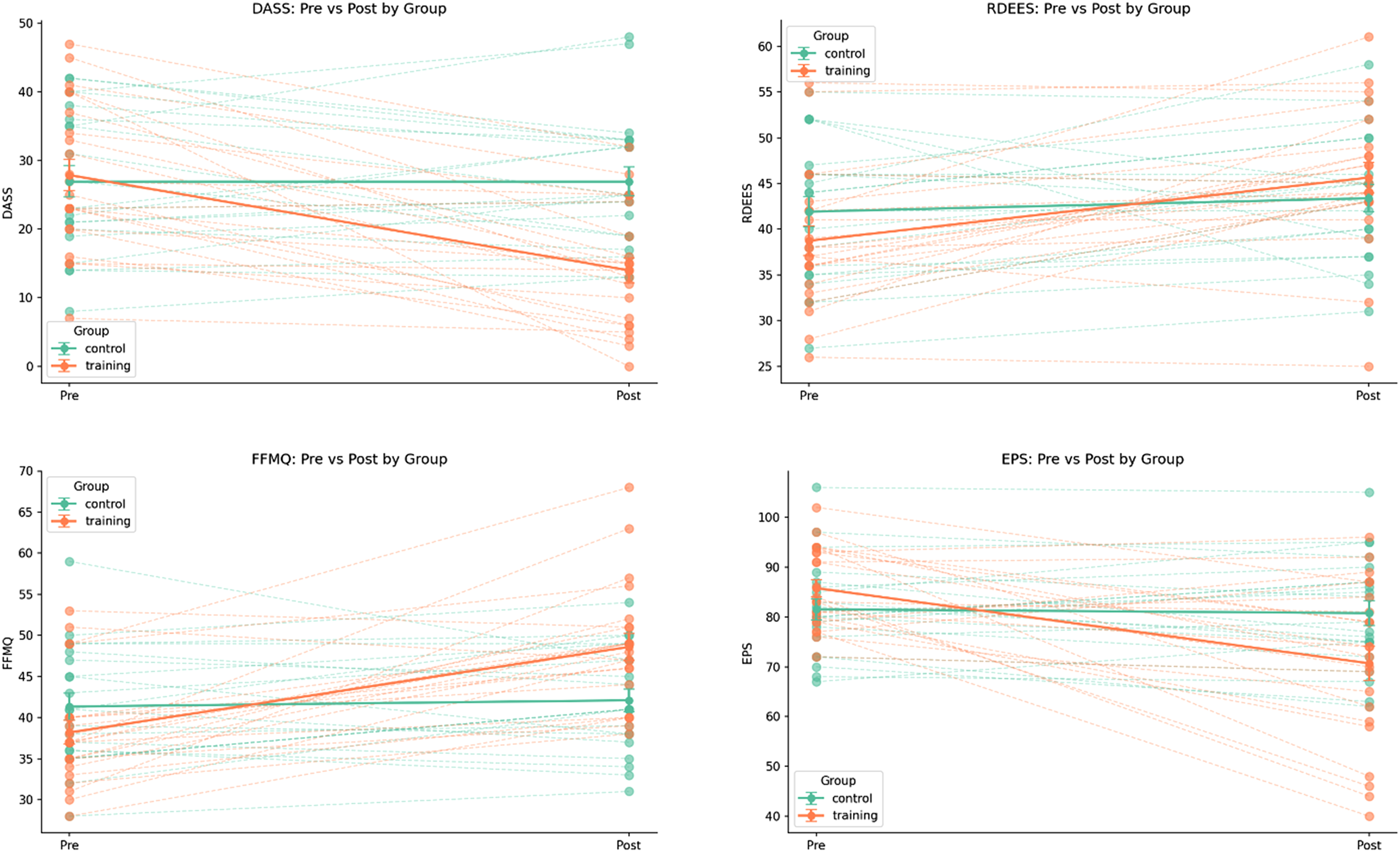
3.4. Relationship between symptom changes and training indicators
We conducted correlation analyses on the change scores (pre-to post-intervention) for alexithymia symptoms, secondary emotional outcomes, and mindfulness, see Figure 5. In the experimental group, these changes were highly intercorrelated (| r |=0.40-0.83, ps < .05) and significantly associated with proactively reporting days of completion (r = 0.68, p < .001) and a rating score reflecting training engagement (r = 0.716, p < .001). In contrast, changes in the control group were relatively random, lacking this pattern of covariation (ps > .05). This further suggests that the positive changes in alexithymia and emotional well-being observed in the experimental group were directly attributable to the intervention and were modulated by training engagement. Correlation between training gains/emotional changes and training parameters. (a). Unlike the control group, where emotional changes appeared relatively random. (b). The experimental group showed a strong interconnectedness among various emotional indicators, (c). These indicators were also significantly correlated with self-reported training engagement. (d). And the number of days the training was completed with high quality.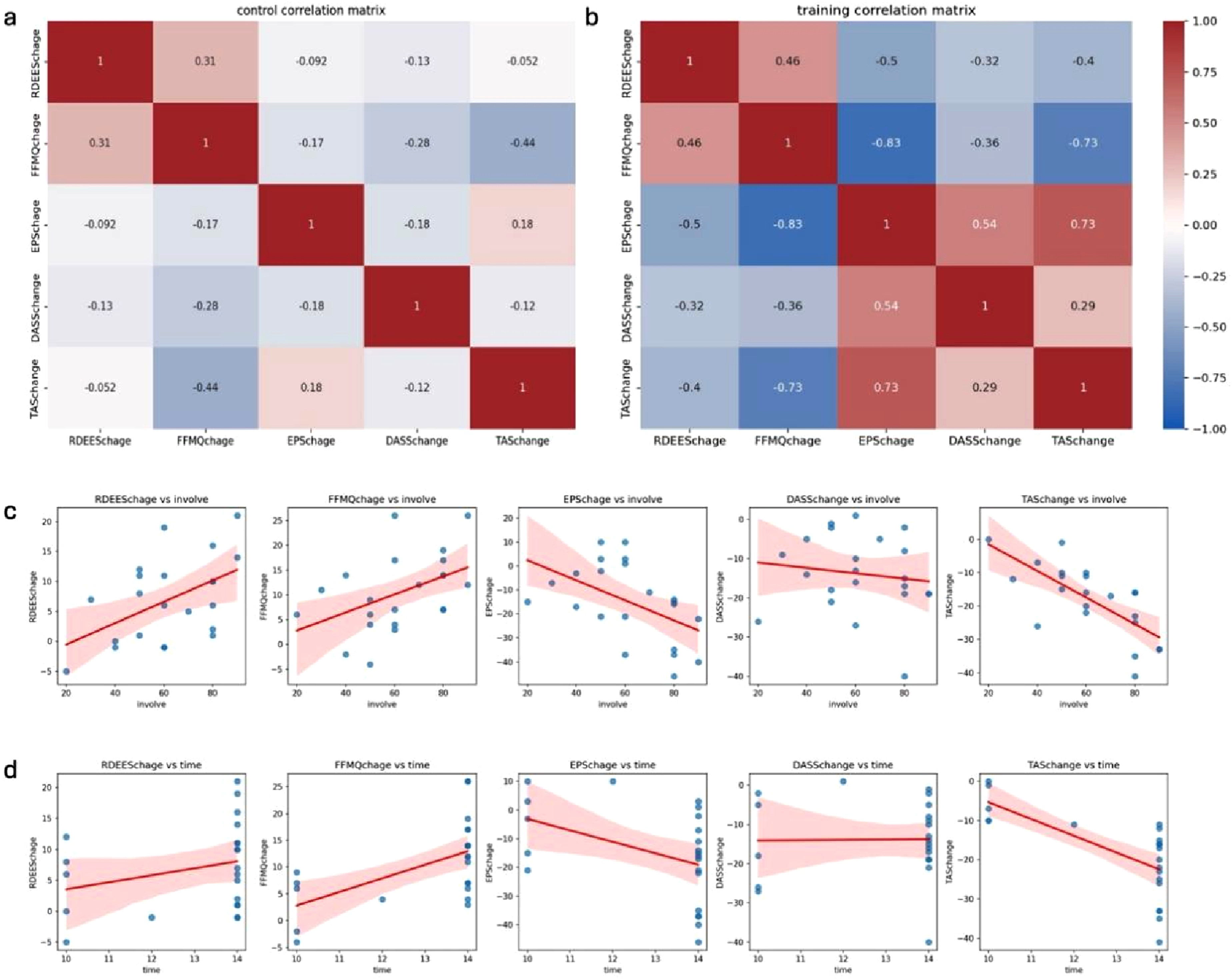
3.5. Usage and experience ratings
Participants provided positive feedback on the alexithymia training software, rating it highly on a 10-point scale for ease-of-use (M = 7.73) and emotional experience (M = 7.81). A large majority (95.4%) would recommend the tool. Textual analysis of 23 pieces of feedback text revealed predominantly positive sentiment. Key themes included: (1) Support for the software as a valuable tool for improving emotional awareness; (2) Concerns about operational issues (e.g., typing vs handwriting for emotional process); and (3) Suggestions for interface enhancements (e.g., more engaging visuals). Detailed feedback is available in the data link.
4. Discussion
This study provides compelling preliminary evidence for the efficacy of a meticulously designed digital intervention targeting alexithymia within an affective process framework. Our findings strongly suggest that specifically addressing emotional processing deficits and associated defensive mechanisms can yield significant improvements in emotional awareness, regulation, and expression. The observed reduction in Toronto Alexithymia Scale (TAS-20) scores within the experimental group, coupled with concomitant improvements in related outcomes such as depression, anxiety, stress, mindfulness, emotional differentiation, and overall emotional processing, collectively supports the effectiveness of this digital intervention.
The digital intervention offers a promising avenue for addressing alexithymia due to its inherent accessibility, affordability, and potential for widespread dissemination. The strategic incorporation of a gamified Attention Bias Modification (ABM) task, guided mindfulness meditations, interactive emotional vocabulary exercises, and structured expressive writing prompts likely contributed to the intervention’s overall effectiveness by engaging participants in a diverse array of activities that directly target distinct aspects of emotional processing.
Although mindfulness training is one component of our multi-modal intervention and has been shown to improve interoceptive awareness and emotional functioning in alexithymia,29,31 recent literature also highlights that mindfulness practice may produce null or even adverse effects. 74 Such outcomes are often underreported due to the absence of clear operational definitions and standardized assessment procedures for negative experiences.75–77 This concern is particularly relevant for alexithymia, as reduced emotional awareness and defensive avoidance may increase sensitivity to challenging internal experiences. To address this issue, our study did not rely on mindfulness as a standalone technique; instead, our this study distinguishes itself from previous research by adopting a mechanism-based approach and developing a comprehensive digital intervention that addresses multiple stages of emotional processing, moving beyond symptom management to target underlying cognitive and emotional processes. 78 Moreover, we incorporated structured assessments of emotional processing, differentiation, stress, and mindfulness rather than depending solely on spontaneous self-reports. The significant intercorrelations observed in the experimental group between improvements in alexithymia symptoms, secondary emotional outcomes, and mindfulness further support this mechanism-based approach. The observed intercorrelations between improvements in alexithymia symptoms, secondary emotional outcomes, and mindfulness support the potential utility of such mechanism-informed multi-component interventions, though the present sample size limits strong mechanistic claims.
From baseline (T1) to post-intervention (T2), and controlling for potential time effects, the intervention tool demonstrated beneficial effects across all measured dimensions of alexithymia. The experimental group exhibited a marked decrease in TAS-20 scores, as well as scores on the Difficulty Identifying Feelings (DIF), Difficulty Describing Feelings (DDF), and Externally-Oriented Thinking (EOT) subscales, relative to the control group. The pattern observed across the alexithymia dimensions suggests that the digital intervention may have influenced mechanisms central to the development and maintenance of alexithymic traits. Rather than representing isolated skills, alexithymia is increasingly conceptualized as a multidimensional disturbance involving reduced interoceptive awareness, limited emotional conceptualization, and habitual avoidance of internal experiences.79,80 From this perspective, improvements following the intervention may reflect changes in these core processes rather than surface-level shifts in questionnaire scores. Furthermore, the study found broader psychological improvements in the experimental group — such as reduced stress and enhanced mindfulness and emotional differentiation—also fits with contemporary models of alexithymia as a transdiagnostic vulnerability factor. High alexithymia has been linked to dysregulated physiological arousal, maladaptive emotion regulation strategies, and impaired processing of affective cues. 81 Interventions that improve mindful awareness and emotion differentiation may mitigate these mechanisms by fostering more precise emotional representations and enabling more adaptive regulatory responses. 82 Thus, the observed psychological benefits likely reflect downstream effects of strengthening core emotional processing capacities.
One particularly meaningful observation concerns the pronounced change in externally oriented thinking (EOT). EOT is considered the most behaviorally expressed and potentially most modifiable facet of alexithymia, as it reflects a persistent attentional bias away from internal states and toward external, concrete information. 83 Prior research has shown that individuals high in EOT tend to underutilize emotional cues in daily life and demonstrate attenuated physiological and neural responses to emotionally salient stimuli. 84 Indeed, a critical first step in addressing alexithymia is fostering awareness of emotions and understanding their significance for the individual,83,85 which then enables subsequent adjustments and behavioral changes. Interventions that increase emotional salience, promote reflective awareness, or facilitate embodied engagement with emotional experiences are therefore theorized to directly target the mechanisms underlying EOT. The present training, which repeatedly emphasized the value of noticing, monitoring, and reflecting on internal cues, appears consistent with this pathway.
The positive association between symptom improvement and training engagement further underscores the importance of user experience. Individual training duration and a rating score reflecting training engagement were significantly correlated with improvements in alexithymia symptoms, secondary emotional outcomes, and mindfulness. This suggests that greater participation in the intervention was linked to more substantial positive changes.29,86 This finding is corroborated by user feedback, with participants rating the software highly for ease-of-useand emotional experience on a 10-point scale, and 95.4% indicating they would recommend the tool. Textual analysis of feedback highlighted suggestions, such as the limited emotional writing experience associated with typing compared to handwriting,87,88 which, while minor, provide valuable insights for future iterations of the software to further enhance user experience and potentially increase engagement.
Despite the overall effectiveness of the digital intervention, it is important to note that Figures 2 and 3 reveal substantial individual variability in symptom-change trajectories. Such heterogeneity is common in alexithymia research, as individuals differ widely in their baseline levels of emotional awareness, cognitive–affective processing styles, and responsiveness to psychological interventions. While the present findings demonstrate that the digital tool can meaningfully reduce alexithymia severity and associated symptoms—such as stress, anxiety, and depression—the pronounced between-person variation suggests that not all individuals benefit to the same extent. This highlights the need for caution in generalizing the current results, particularly given the relatively modest sample size and reliance on a non-clinical population. Although these characteristics allowed us to test the feasibility and preliminary efficacy of the tool, they also limit conclusions regarding its broader applicability. Future research should therefore examine whether similar effects emerge in larger and more clinically diverse samples, explore individual-difference predictors of treatment responsiveness, and evaluate whether adaptive or personalized intervention components could better accommodate variability in emotional processing profiles. Such work would further clarify the conditions under which digital interventions for alexithymia are most effective and support their refinement and potential dissemination.
As a preliminary proof-of-concept study, this research has several limitations that warrant consideration. First, the current study represents a preliminary efficacy trial with a relatively small sample, and the design does not allow for strong causal inferences regarding underlying mechanisms. Future studies with larger, fully powered samples and multi-method assessments—including behavioral and physiological indices—are warranted to validate specific mechanisms of change. Second, on the technical level, the interface of the digital alexithymia intervention tool still has room for optimization. Future efforts should focus on improving the following aspects: adding adaptive layouts to automatically switch between horizontal and vertical screen modes based on the user’s device type (tablet/PC), developing a personalized theme system that allows users to customize emotional training scenarios (e.g., selecting natural landscapes or abstract art as backgrounds for mindfulness practice), thereby enhancing emotional immersion; updating the existing emoticon library and enriching the emoticons used in the attention bias game to improve the user experience; strengthening the inter-module linkage by constructing a cross-module emotional profile, for example, when emotional vocabulary such as “anxiety” frequently appears in the writing module, automatically triggering targeted content of related entries in the emotional dictionary (including relevant metaphor stories and test questions); finally, increasing the program’s feedback mechanisms, such as setting achievement badges and task rewards, to improve user engagement and enjoyment. In terms of experimental design, there are also some limitations that need to be addressed in future research. The absence of a follow-up period prevents us from determining whether the intervention’s effects are immediate or sustained. In addition, the reliance on subjective self-reports without objective validation may oversimplify the complexity of emotional processing. Ideally, future assessments should incorporate multiple levels of measurement, including subjective reports, behavioral observations, and physiological indicators, to effectively differentiate the unique contributions of each training component or process.
5. Conclusion
In summary, the digital intervention tool is effective in promoting emotional awareness, attention to emotions, and improving emotional consciousness in alexithymia individuals. As a short-term, symptom-targeted intervention, it has achieved the expected results and showed promise as an effective and accessible tool for improving emotional processing abilities and reducing alexithymia symptoms. By adopting a mechanism-based approach and leveraging the potential of digital technology, this study provides a foundation for the development of more effective and scalable interventions for alexithymia and contributes to the growing body of literature on interventions for alexithymia. However, there is still a long way to go from recognizing and distinguishing emotions to describing them in accurate language and appropriately processing them. In the future, it will be necessary to develop richer intervention modules and formulate longer-term, personalized intervention programs.
Supplemental material
Supplemental Material - A mechanism-based digital intervention for alexithymia: Design, development, and validation of a multi-modal approach
Supplemental Material for A mechanism-based digital intervention for alexithymia: Design, development, and validation of a multi-modal approach by Wen Wang, Ya-meng Xu and Dong-ni Pan in Digital Health.
Supplemental material
Supplemental Material - A mechanism-based digital intervention for alexithymia: Design, development, and validation of a multi-modal approach
Supplemental Material for A mechanism-based multi-modal digital intervention for alexithymia: A feasibility and efficacy study by Wen Wang, Ya-meng Xu and Dong-ni Pan in Digital Health.
Supplemental material
Supplemental Material - A mechanism-based digital intervention for alexithymia: Design, development, and validation of a multi-modal approach
Supplemental Material for A mechanism-based multi-modal digital intervention for alexithymia: A feasibility and efficacy study by Wen Wang, Ya-meng Xu and Dong-ni Pan in Digital Health.
Footnotes
Acknowledgements
The authors gratefully acknowledge the technical support provided by Daotuan Wang. The authors sincerely thank Beijing Shengxin Technology Development Group Co., Ltd. for its crucial collaboration in the co-development and translational research of the digital intervention prototype. We also gratefully acknowledge the financial support from Beijing Shengxin Company for covering the article processing charges and other essential resource assistance throughout the research and publication process.
Ethical considerations
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All experimental protocols were pre-registered and approved by the ethics committee of the Beijing Language and Culture University (2024BYLL50).
Consent to participate
Informed consent was obtained from all individual participants included in the study. The research team placed a high emphasis on ensuring participant privacy and confidentiality, ensuring that all obtained data was exclusively utilized for research objectives.
Author contributions
Dong-ni Pan: Conceptualization, Manuscript Writing (original draft and review & editing). Wen Wang: Execution of the study, Data analysis, Support for Manuscript Writing (review & editing). Ya-meng Xu: Execution of the study, Data analysis, Support for Manuscript Writing (review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was supported by the Fundamental Research Funds for the Central Universities of Beijing Language and Culture University (Grant No. 24QN28 to Dong-ni Pan), and Beijing Shengxin Technology Development Group Co., Ltd.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Reporting protocol
Supplemental material
Supplemental material for this article is available online.