
Abstract
Purpose. Patients with hematological malignancies often present with reduced muscle and physical functions, which are caused by the disease or related treatment. Moreover, patients with hematological malignancies rapidly develop low hemoglobin levels, and this may affect muscle and physical functions. This study aimed to identify the influence of hemoglobin levels on muscle and physical functions in patients with hematological malignancies. Methods. Using a cross-sectional study design, this study included 60 patients with hematological malignancies (mean age = 68.0 ± 10.2 years, women 56.7%) who were hospitalized for chemotherapy- and radiotherapy-related side effects and underwent examination for skeletal muscle mass (SMM), muscle strength, physical function, activities of daily living (ADLs), psychological status, and quality-of-life (QOL), including physical symptoms. Participants were divided into 3 groups according to tertiles of hemoglobin levels: low (n = 19), middle (n = 20), and high (n = 21). Evaluation items were compared among the 3 groups. Results. There was no significant difference among the 3 groups in terms of SMM. The low hemoglobin group showed significantly higher values of fatigue and dyspnea and lower values of muscle strength, ADLs, and QOL than the high hemoglobin group. Conclusions. Hemoglobin levels did not affect SMM; however, muscle weakness, decrease in physical function, physical symptoms such as fatigue and dyspnea, and decline in ADLs and QOL were observed in patients with low hemoglobin levels.
Introduction
In recent decades, the survival rates of patients diagnosed with hematological malignancies have gradually improved.1,2 The annual number of new patients with hematological malignancies, such as lymphoma, leukemia, and multiple myeloma, is estimated to be 918 000 worldwide. 3 In Japan, >45 000 people are diagnosed annually with hematological malignancies, 4 which means that patients with hematological malignancies during and after treatment are increasing. Consequently, attention should not only be paid to curing the disease, but also to the long-term consequences of the disease and the associated treatment. 5 Repeated chemotherapy and radiotherapy, which are typically used to treat hematological malignancies, can induce physical and mental symptoms, such as pancytopenia (derived from nutritional deficiencies and bone marrow suppression),6-9 nausea, vomiting, anorexia,9,10 cancer-related fatigue, 11 and anxiety and depression12,13 as well as symptoms of the hematological malignancy itself. Furthermore, these symptoms can cause a decrease in physical function,14-16 which can lead to the deterioration of activities of daily living (ADLs) and quality-of-life (QOL). 15 Kilgour et al 17 showed that hand grip strength was independently associated with survival in cancer patients. Additionally, Go et al 18 reported that sarcopenia was associated with intolerance to chemotherapy and poor prognoses in lymphoma patients. These facts indicate the importance of focusing on muscle and physical functions. Although various factors are thought to be involved in the deterioration of muscle and physical functions, the precise mechanism is not clearly known. Hemoglobin level is considered to be one of these factors; a previous study found that low hemoglobin level was an important factor that influenced muscle strength in patients with hematological malignancies. 19
Low hemoglobin levels result in various adverse health outcomes, including not only low muscle strength, but also impaired walking; increase in fatigue, anxiety, and depression; and decline in QOL in community-dwelling people.20-24 In patients with malignancies, low hemoglobin level may be caused by multiple factors; it could be a direct result of the cancer or the result of cancer treatment, such as chemotherapy. 25 A high proportion of patients with hematological malignancies, whose treatment is centered on chemotherapy, have low hemoglobin levels. 26 Therefore, we hypothesized that low hemoglobin levels adversely affected muscle mass and physical function in patients with hematological malignancies. In fact, an association between functional capacity and hemoglobin levels has been reported in lung cancer patients. 27 A previous study also reported that hemoglobin levels were associated with exercise tolerance in patients with hematological malignancies who were undergoing hematopoietic stem cell transplantation. 28 However, no previous reports have revealed any relationship between hemoglobin levels and muscle and physical functions in patients with hematological malignancies undergoing chemotherapy, radiotherapy, or chemoradiotherapy. In addition, there have been no studies on the characteristics of patients with low hemoglobin levels through multifaceted evaluation of physical symptoms, psychological distress, ADLs, and QOL.
Hence, this study aimed to assess the influence of hemoglobin levels on muscle and physical functions, ADLs, and QOL in patients with hematological malignancies. The novelty of this study lies in the fact that, through multifaceted evaluation, we examined the associations of hemoglobin that could influence deterioration of muscle function. If these associations are identified, hemoglobin levels may be used as screening tools for deterioration of muscle function in patients with hematological malignancies; these results may become important basic data leading to changes in clinical settings in the field of rehabilitation medicine.
Methods
Study Design and Participants
This was a cross-sectional, observational study conducted at Nagasaki University Hospital. This study was approved by the hospital ethics committee before the start of the study (approval number, 15072757), and written informed consent was obtained from all participants prior to study enrollment. The inclusion criteria were as follows: (1) inpatients diagnosed with hematological malignancies; (2) hospitalization for chemotherapy, radiotherapy, or chemoradiotherapy; (3) prescription for rehabilitation; (4) age >20 years; and (5) those in whom evaluations of muscle function, physical function, ADLs, psychological distress, and QOL were conducted. The exclusion criteria were as follows: (1) communication difficulties, (2) poor general health status, (3) severe heart disease, (4) severe respiratory disease, (5) hepatic or renal failure, and (6) cerebrovascular or orthopedic disease that could influence muscle mass and/or physical function.
The sample size was calculated using a common sample size calculation software (G*Power, version 3.1.9.2 for Windows; Dusseldorf, Germany) and was determined based on differences in hand grip strength. 29 With the effect size calculated from the mean and SD, the statistical power and level of significance for the study were set at 0.95 and 0.05, respectively, and the sample size for each group was calculated as 16 participants.
Measurements
Baseline age, sex, body mass index (BMI), blood chemistry (hemoglobin, C-reactive protein [CRP], albumin, total protein, and lymphocytes) data, cancer type, treatment, days since hospitalization, days since treatment, and disease duration data were collected from medical records. Participants were evaluated for muscle and physical function, ADLs, psychological distress, and QOL at the start of rehabilitation.
Muscle Function
Muscle function was evaluated as a primary outcome. Skeletal muscle mass (SMM) was measured using bioelectrical impedance analysis via a Physion MD system (Physion Co, Ltd, Kyoto, Japan). Impedance measurements were performed at a frequency of 50 kHz with a current of 500 µArms and an impedance range of 10 to 1500 Ω. Accuracy was ±1%, ±0.5 Ω (50-1000 Ω), or ±2%, ±0.5 Ω (other impedance range), and the resolution capability was 0.1 Ω. All measurements were performed in the supine position with the arms slightly abducted from the body, forearms pronated, and legs spread slightly apart. The impedance value of each body segment (upper arm, forearm, thigh, lower leg, and trunk) was measured using 2-lead bioelectrical impedance analysis systems (distal first, proximal second). The current-introducing (source) electrodes were placed on the dorsal surface of the right and left metacarpal and metatarsal bones, respectively. For the first distal lead measurement, voltage-sensing (detector) electrodes were placed on the middle point of the ulnar and radial styloid as well as the medial and lateral malleolus. For the second proximal lead measurement, the source electrodes were arranged in the same manner as those used for the first measurement while the detector electrodes were placed on the proximal ends of the radius and tibia. From these processes, the impedance value of each segment was measured, and SMM was calculated by programming. The validity of this equipment has been verified previously 30 and has been applied to the prediction of skeletal muscle volume.31,32 The appendicular SMM was normalized for stature and referred to as the appendicular skeletal muscle mass index (SMI, kg/m2).
Hand grip strength and isometric knee extensor strength were assessed as markers of muscle strength. Hand grip strength was measured using a standard adjustable-handle dynamometer (TKK 5101; Takei Scientific Instruments Co Ltd, Niigata, Japan). The measurements were taken in the standing position, with the patient’s arm held at zero abduction and flush against the body. A single attempt of maximum value was recorded in kilogram force. Isometric knee extensor strength was measured using hand-held dynamometers (HHDs; µ-tas F-1; ANIMA Co, Tokyo, Japan) in the sitting position on a chair with the knee joint flexed at approximately 90°. The HHD sensor was placed on the distal anterior surface of the lower leg, and a belt was placed over the HHD and tied to the leg of the chair. Knee joint extension at maximum exertion was performed for approximately 5 s and was repeated twice. The result was expressed in kilogram force, and the highest value was entered into the analysis.
Physical Function
Physical function was evaluated by a timed up and go test (TUGT). It was measured as an index of functional mobility, which included walking speed, strength, and balance. Participants were instructed to rise from a chair of standardized height, walk a fixed distance of 3 m, turn, return to the chair, and sit down again. 33 The validity and reliability of TUGT has been previously reported.33,34 After several TUGT attempts were performed, the fastest time was recorded in seconds.
Activities of Daily Living
ADLs were evaluated using the Eastern Cooperative Oncology Group (ECOG) Performance Status (PS) and the Functional Independence Measure (FIM). The ECOG PS scoring was defined as follows: 0, fully active, able to perform all predisease activities without restriction; 1, restricted in physically strenuous activity but ambulatory and able to perform work of a light or sedentary nature; 2, ambulatory and capable of all self-care, but unable to perform any work activities, as well as up and about >50% of waking hours; 3, capable of only limited self-care, confined to bed or chair for >50% of waking hours; and 4, completely disabled, cannot perform any self-care, totally confined to bed or chair. 35 FIM assessed function (activity) and the need for assistance. This measurement consists of an 18-item scale that measures independence in performing tasks, including feeding, grooming, dressing, toileting, mobility, and cognition. 36 Each item is rated on a scale of 1 to 7 (1 = total assistance, 5 = needs supervision, 6 = modified independence, 7 = independent). A low score reflects the burden of care in each area measured. The reliability and validity of FIM has been reported.36,37
Psychological Distress
The sum-total score of the Hospital Anxiety and Depression Scale (HADS) was used to evaluate psychological distress. This is a widely used and validated questionnaire for assessing psychological morbidity in cancer patients 38 and comprises 7-item anxiety and 7-item depression subscales. Items are rated 0 (best status) to 3 (worst status), and the scores of each subscale are summed. Possible scores for each subscale range from 0 to 21 points. Higher scores reflect worse anxiety and depression.
Quality of Life
QOL was measured using The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-C30. This is a cancer-specific, self-report questionnaire and consists of the global QOL scale (2 items), 5 functional scales (physical, role, emotional, cognitive, and social functioning), 3 symptom scales (fatigue, pain, and nausea/vomiting), and 6 single items. The 2 items of the global QOL scale are applied to a modified 7-point Linear Analogue Scale. All other items are scored on a 4-point categorical scale ranging from 1 (not at all) to 4 (very much). All scales and single items are transformed to a 0 to 100 scale. For the global QOL scale and 5 functional scales, a higher score represents a better level of functioning, whereas for the symptom scales and items, a higher score means a higher level of symptoms. 39
Statistical Analysis
Single regression analysis was performed to confirm the relationship between hemoglobin levels and muscle function in this study. With reference to a previous study that divided cancer patients into 3 groups according to tertiles of fatigue levels, 40 participants were divided into 3 groups according to tertiles of hemoglobin levels: low, middle, and high hemoglobin levels. The Kruskal-Wallis test was used to compare these 3 groups. Analysis of covariance (ANCOVA) was performed to confirm the influence of potential confounding factors, such as age, sex, BMI, blood chemistry data, cancer type, treatment, days since hospitalization, days since treatment, disease duration, psychological distress, and physical symptoms, that could affect the relationship between hemoglobin levels and muscle function.
Statistical analysis was performed using IBM SPSS Statistics version 23 software (IBM Corp, Armonk, NY). Data were presented as mean ± SD. P <.05 was considered statistically significant.
Results
The patient selection process is shown in Figure 1. Of the 79 eligible patients with hematological malignancies, 60 (26 men, 34 women) participated in the study. Table 1 shows the demographic and clinical characteristics of the analyzed patients. The mean age was 68.0 ± 10.2 years, the mean BMI was 21.1 ± 3.4 kg/m2, and the mean hemoglobin level was 10.2 ± 2.3 g/dL. More than half of the patients (58.3%) were diagnosed with lymphoma. Days since hospitalization and treatment were 10.2 ± 12.1 days and 4.2 ± 12.4 days, respectively. The disease duration was 448.4 ± 651.5 days.

Flowchart of the recruitment procedure.
Demographic and Clinical Characteristics Data of Patients With Hematological Malignancy.

Abbreviations: BMI, body mass index; CRP, C-reactive protein.
The demographic and clinical characteristic data of patients with hematological malignancies, as classified by hemoglobin levels, are shown in Table 2. There were no significant differences in age, sex, CRP levels, treatment, pretreatment or posttreatment, days since treatment, or disease duration among the 3 groups; however, BMI, hemoglobin, albumin and total protein levels, lymphocytes, cancer type, and days since hospitalization were significantly different among the 3 groups.
Demographic Data of Patients With Hematological Malignancy Classified by Hemoglobin Level. a

Abbreviations: BMI, body mass index; CRP, C-reactive protein.
Kruskal-Wallis test for the comparison of low, middle, and high. P1, low versus middle; P2, low versus high; P3, middle versus high.
Muscle Function
Single regression analysis showed that although there was no significant association between hemoglobin levels and SMM (P = .534) or SMI (P = .749), hand grip strength (P = .009) and isometric knee extensor strength (P = .004) were significantly related to hemoglobin levels. In comparison among groups, there was no significant difference in SMM (P = .241) or SMI (P = .128) among the 3 groups. For hand grip strength, a significant difference was observed (P = .026), with the low hemoglobin group having significantly lower values than the high hemoglobin group (P = .021). Similarly, isometric knee extensor strength differed significantly among the 3 groups (P = .042), with the low hemoglobin group having significantly lower values than the high hemoglobin group (P = .035; Table 3). We adjusted for each potential confounding factor during ANCOVA; the relationship between hemoglobin levels and hand grip strength showed borderline significance only with adjustment for BMI (P = .077), and a significant relationship was observed after adjustment with other potential confounding factors (Table 4). Similarly, a significant relationship between hemoglobin levels and isometric knee extensor strength was observed after adjustment with all potential confounding factors (Table 4).
Muscle and Physical Function, ADLs, Psychological Distress of Patients With Hematological Malignancy Classified by Hemoglobin Level. a

Abbreviations: ADLs, activities of daily living; SMM, skeletal muscle mass; SMI, skeletal muscle mass index; kgf, kilogram force; TUGT, Timed Up and Go Test; ECOG PS, the Eastern Cooperative Oncology Group Performance Status; FIM, Functional Independence Measure; HADS, Hospital Anxiety and Depression Scale.
P1, low versus middle; P2, low versus high; P3, middle versus high.
Relationship Between Hemoglobin Levels and Muscle Strength Adjusted by Each Potential Confounding Factor During ANCOVA.
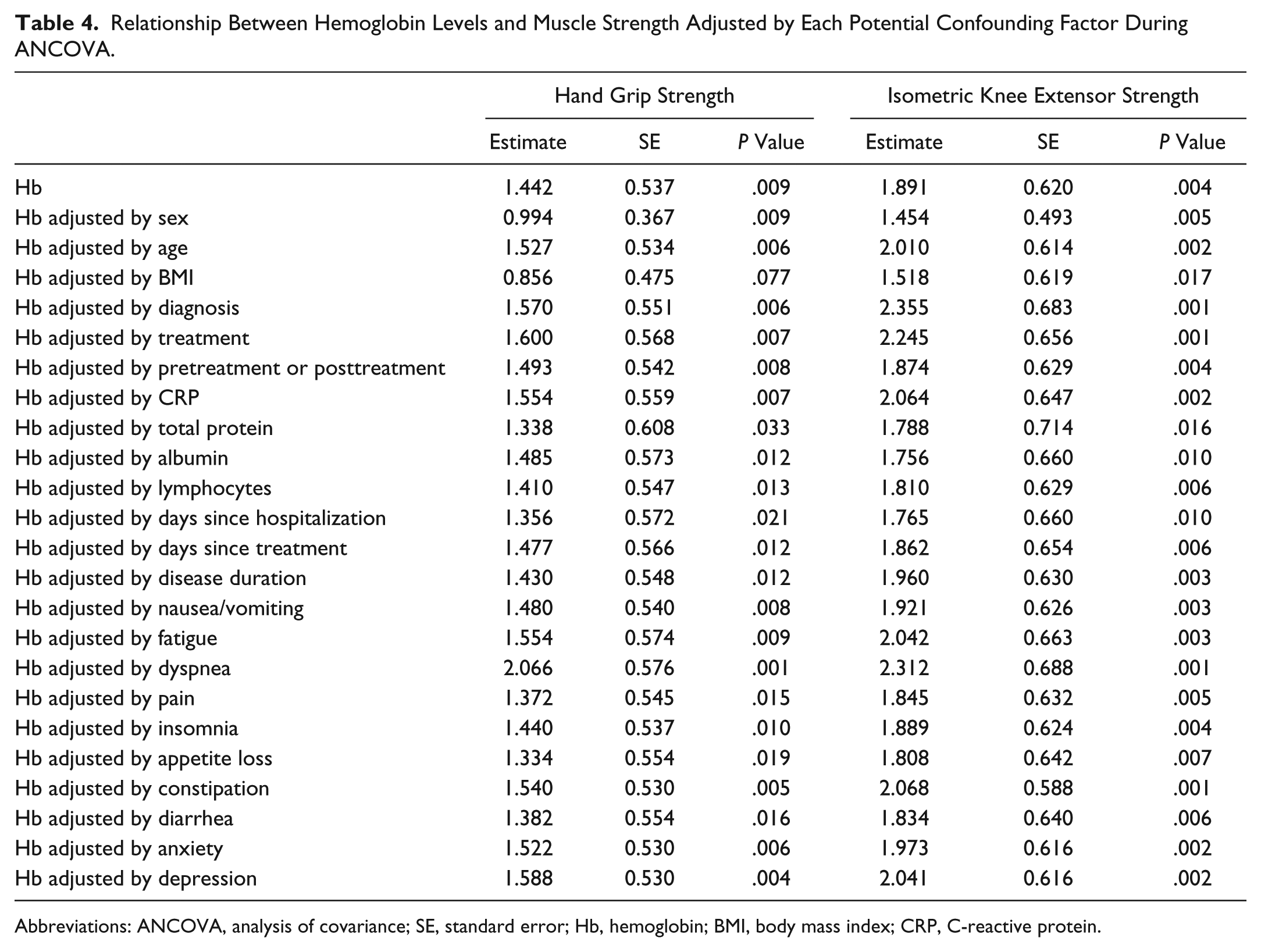
Abbreviations: ANCOVA, analysis of covariance; SE, standard error; Hb, hemoglobin; BMI, body mass index; CRP, C-reactive protein.
Physical Function
No significant difference in TUGT (P = .090) was found among the 3 groups (Table 3).
Activities of Daily Living
Significant differences were observed in PS (P = .013) and FIM (P = .003). The low hemoglobin group showed higher values of PS than the high (P = .021) and middle (P = .044) hemoglobin groups. For FIM, the low hemoglobin group had significantly lower values than the high (P = .015) and middle (P = .005) hemoglobin groups (Table 3).
Psychological Distress
No significant differences were observed in HADS score for either total (P = .289), anxiety (P = .209), or depression (P = .578) assessment among the 3 groups (Table 3).
Quality of Life
For QOL, there were significant differences in physical (P = .010), role (P = .008), fatigue (P = .034), dyspnea (P = .004), and pain (P = .037) values among the 3 groups (Table 5). The low hemoglobin group showed significantly lower values than the high hemoglobin group in the physical (P = .007) and role (P = .006) categories; the low hemoglobin group also had higher values than the high hemoglobin group for the fatigue (P = .033) and dyspnea (P = .003) categories. For pain, the low hemoglobin group showed higher values than the middle hemoglobin group (P = .037; Table 5).
QOL of Patients With Hematological Malignancy Classified by Hemoglobin Level. a

Abbreviation: QOL, quality of life.
P1, low versus middle; P2, low versus high; P3, middle versus high.
Discussion
This is the first study to investigate the influence of hemoglobin levels on muscle and physical functions, ADLs, and QOL in patients with hematological malignancies. After categorizing patients into tertiles of hemoglobin levels, there was no significant difference among the 3 groups for SMM or SMI, whereas the low hemoglobin group showed significantly higher values of fatigue and dyspnea and lower values of muscle strength, ADLs, and QOL than the high hemoglobin group.
Patients with hematological malignancies often show a decrease in SMM. 15 In previous studies, hemoglobin levels were found to be associated with SMM in elderly populations.41,42 Although Hai et al 43 showed that community dwelling adults with sarcopenia had low hemoglobin levels, this factor was not associated with sarcopenia in the reported multivariate model. Additionally, Huang et al 44 reported that hemoglobin levels did not put patients at a higher risk for low muscle mass in elderly populations. Based on previous studies and results of the current study, hemoglobin levels may not directly affect SMM in patients with hematological malignancies. However, PS-defining ADLs, according to activity levels, showed significantly lower values in the low hemoglobin group in this study. Therefore, we inferred that there is a possibility that muscle wasting resulting from decreased physical activity may progress over time. Therefore, this effect should be further elucidated in future longitudinal studies. Nevertheless, even though a reduction in SMM caused by low hemoglobin levels was not found, other factors involved in muscle wasting need to be studied in the future. Also, the low hemoglobin group showed lower values of hand grip and isometric knee extensor strength than the high hemoglobin group. In general, muscle mass is a major determinant of skeletal muscle strength. 45 Although SMM was equal among the 3 groups in this study, it is interesting that muscle strength differed between them. In this study, we showed that hemoglobin levels influenced muscle strength by simple regression analysis; consistent with our results, some studies have demonstrated that low hemoglobin levels can cause a decline in oxygen delivery to skeletal muscle, 46 and this negatively affects muscle strength.21,41,47 In other words, it was possible that hemoglobin levels affected muscle strength. However, it was considered that other factors were involved in the relationship between hemoglobin levels and muscle strength. In fact, previous studies have suggested the involvement of other factors. For example, hemoglobin levels were negatively correlated with fatigue, 48 which is the most common chronic symptom in cancer patients receiving cytotoxic chemotherapy 49 ; moreover, Kilgour et al 17 reported that fatigue was negatively correlated with muscle strength. Therefore, ANCOVA was performed to confirm the confounders that affect the relationship between hemoglobin levels and muscle strength. We adjusted for each potential confounding factor during ANCOVA; the relationship between hemoglobin levels and hand grip strength showed borderline significance only with adjustment for BMI (P = .077), and a significant relationship was observed after adjustment with other potential confounding factors. Similarly, a significant relationship between hemoglobin levels and isometric knee extensor strength was observed after adjustment with all potential confounding factors. Therefore, hemoglobin levels were suggested to have affected muscle strength.
In previous studies, low hemoglobin level was an independent risk factor for decline in physical function.21,42,50 In this study, although no significant difference was observed, a borderline significance was found among the 3 groups for TUGT score, which is a measurement of physical function. TUGT can measure walking speed, strength, and balance. The low hemoglobin group had muscle weakness and high values of fatigue, which might affect the decline in physical function. In this study, the low hemoglobin group also showed higher values of dyspnea than the high hemoglobin group. It has been suggested that low hemoglobin levels are involved in dyspnea, which is presumed to have been caused by hypoxia associated with a decline in oxygen delivery. 51 Given et al 52 indicated that dyspnea was significantly related to the decline of physical function. Therefore, dyspnea might also affect the decline of physical function.
Indicators of ADLs, such as PS and FIM, were significantly decreased in the low hemoglobin group. These results were similar to those reported by Mancuso et al 27 and Denny et al 53 for patients with lung cancer as well as by Hirani et al 42 for community-dwelling elderly people. It was inferred that physical symptoms, such as fatigue and dyspnea, combined with a decrease in muscle strength and physical function might be associated with a decrease in ADLs. Furthermore, the low hemoglobin group had a significantly lower QOL in this study. Previous studies have shown that low hemoglobin levels are associated with a decline in QOL,25,28,41 which supports our results. Additionally, it has been reported that physical symptoms, such as fatigue and dyspnea, are associated with decreasing QOL.28,54 Therefore, in addition to dysfunction, disabilities, and decrease in QOL, it is possible that low hemoglobin levels were also associated with these physical symptoms.
It has been shown that low hemoglobin levels are negatively associated with depression in a previous study. 28 However, this result differs from that of our study, where hemoglobin levels were not related to anxiety and depression. This indicates that factors other than hemoglobin level are involved in the psychological distress of patients with hematological malignancies. Tecchio et al 55 revealed that gender, obsessive-compulsive symptoms, intratensive personality traits, and a lower performance status predicted a higher level of depression during hematopoietic stem cell transplantation. Factors related to psychological distress in patients with hematological malignancies undergoing chemotherapy can be studied in the future.
This study has limitations. First, it excluded patients for whom assessments could not be performed. Therefore, an analysis could not be performed for cases that tend to involve muscle and physical function deterioration resulting from a low motivation for rehabilitation. Second, the sample size was small. We selected hand grip strength as an outcome and estimated the sample size with reference to a previous study. 29 Therefore, the sample size of this study might be sufficient. However, we could not exclude the possibility that patients with the same characteristics were recruited, which may induce selection bias. From the viewpoint of generalization, a multicenter investigation with a large sample size will be necessary in the future. Third, although verification of causality and control of confounding factors by multivariate analysis were thought to be desirable, they could not be performed because of the small sample size; these analyses need to be performed in future studies. Fourth, we did not quantify physical activities that may affect muscle function, and future studies will be required to clarify this issue.
Conclusion
In this study, hemoglobin levels did not affect SMM, whereas muscle weakness and decrease in physical function were observed in patients with low hemoglobin levels. Additionally, physical symptoms, such as fatigue and dyspnea, and decline in ADLs and QOL were also observed in patients with low hemoglobin levels.
Footnotes
Acknowledgements
The authors thank the members of the Department of Rehabilitation, Nagasaki University Hospital, and the Department of Locomotive Rehabilitation Science, Nagasaki University Graduate School of Biomedical Sciences, for their support; this research would not have been possible without their leadership and cooperation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by JSPS KAKENHI, Grant Number JP26282156.