
Abstract
Introduction
Pancreatic cancer has the lowest survival rate among all cancers.1,2 The mean survival is 14 months after resection and 5 months after palliative surgery.3-6 For patients with metastatic pancreatic cancer, standard chemotherapy treatment yields a median survival of only 6 months. The National Cancer Institute’s SEER survival monograph showed that the 5-year survival rate for 20 829 pancreatic adenocarcinoma patients was only 2.3%. 7 There is no specific indication or simple examination for early-stage pancreatic cancer; hence, early detection is difficult. 8
The combination of Chinese herbal medicine (CHM) and Western medicine (WM) to treat pancreatic cancer has shown improved prognosis and overall survival (OS). 9 CHM is commonly administered for cancer treatment, with 14.2% of patients in the United States, 55% in China, and 12.8% in Taiwan treated by CHM.10-12 Determining whether CHM can improve outcomes in pancreatic cancer is critical. 13 A recent systematic review and meta-analysis of 83 randomized controlled trials (RCTs) in cancer patients receiving CHM showed a decreased incidence of leukopenia, with a potential prophylactic benefit on white blood cell counts. 14 However, CHM in cancer treatment remains controversial, as some herbs (eg, St John’s wort, Ginkgo biloba, and Panax ginseng) interfere with the efficacy of chemotherapy or have associated toxicities.15-17 This lack of communication between Western and traditional Chinese medicine (TCM) can hinder the potential application of TCM and cause physicians to underestimate the benefits of integrating the two.
Therefore, there is a need to investigate and clarify the potential benefits and safety issues of CHM for pancreatic cancer patients. We present a rare case series of pancreatic cancer patients in whom CHM showed equivalent or superior outcomes to conventional surgery or chemotherapy. This study could facilitate interprofessional communication and improved clinical management of pancreatic cancer patients.
Methods
This was a retrospective case series of pancreatic cancer patients who received CHM treatment with/without conventional treatment (ie, surgery, chemotherapy, or radiotherapy). In Hong Kong, as the Chinese Medicine services are not incorporated with the Hong Kong SAR government, the only services supported by the Hospital Authority were provided by the nongovernment organization and the affiliated university in a model of tripartite clinic for operation, which cover only 12% of the Hong Kong Chinese population. Therefore, 88% of the TCM services were provided in the private sectors by patients paying out of pocket. 18 Patients were selected from under the management of Prof Chen Bing Zhong under the affiliation of one private clinic and one clinic from the University. The clinics served 4800 to 7000 cancer patients each year. As most patients were not managed under the Hong Kong government clinical management system, Chinese medicine practitioners (CMPs) could not access any conventional medical record of the patients. International Classification of Diseases, 10th version (ICD-10), codes were not incorporated with routine CMP care in Hong Kong. Cancer patients consulting these clinics were selected based on their last observable imaging reports, including histology, computed tomography (CT), positron emission tomography-CT, magnetic resonance imaging, and endoscopic retrograde cholangiopancreatography (ERCP) from Western medical doctors. To fulfill the inclusion criteria, the diagnoses of pancreatic cancers were cross-checked by a trained research assistant for C25.9 for ICD-10. The average time of initial diagnosis of pancreatic cancer by WM doctors to the first TCM consultation was 53.3 days. Patients received CHM in the form of concentrated CHM granules that were prescribed by the same CMP for at least 3 months, and all costs were borne by the patients themselves. The common chemotherapeutic agents given to patients were 5-fluorouracil and gemcitabine. The outcome was patient survival after the diagnosis of pancreatic cancer, which was made by Western medical doctors based on the last observable imaging reports, including histology, CT, positron emission tomography-CT, magnetic resonance imaging, and ERCP. Follow-up consultation notes were used to verify survival. The CMP prescriptions were carefully evaluated to observe the effect of compliance with TCM theory and any side effects with the use of concurrent chemotherapy, radiotherapy, immunotherapy, or targeted therapy.
Overall, 182 pancreatic cancer cases (code C25.9 according to the ICD-10) continuously treated with CHM >3 months, with one follow-up consultation per month, were purposively identified from 2005 to 2015 in the same TCM clinic in Hong Kong. Survival was defined as the time from day of diagnosis until death. The sample size was based on a convenience sampling technique from the number of cases reported during the study period. The survival time for each patient was based on the patients’ records. Trained research assistants with a structured data extraction form collected the sociodemographic data. The primary clinical outcomes are presented using simple descriptive statistics and Kaplan-Meier estimation (Supplementary Table 1 and Supplementary Figure 1, available online) for survival. Among the 182 pancreatic cancer patients, there were 35 adenocarcinoma, 4 neuroendocrine carcinoma, 1 adenosquamous carcinoma, 1 mucinous cystadenocarcinoma, 1 malignant sarcoma, and the remaining cases were collectively identified as pancreatic cancer. Data on 21 deaths that occurred are presented in this article; the remaining participants continued in the study. Potential confounders included length of CHM use and cancer stage at diagnosis. This case series was compiled according to published guidelines. 19 Informed consent was obtained from the patients at the first consultation. Ethical approval was obtained from the CUHK NTEC Ethics Committee (CREC Ref. No.: 2016.383).
Results
This study describes 21 patients at our institution who consistently received CHM and died; 5 typical cases are presented in the text below. Comparisons between cases in this study and pancreatic cancer patients in Hong Kong receiving CHM are shown in Supplementary Table 1. Patients were 30 to 87 years old at recruitment, with a mean age of 56 years. Calculation of OS is presented in Table 1. The survival and treatment conditions are summarized in Table 2. OS ranged from 4 months to 9.6 years, with a mean survival of 29.6 months and a median survival of 15.2 months. Overall, 76% of patients were alive 1 year after diagnosis (Supplementary Figure 1). The most common syndrome differentiation that classified the pancreatic cancer patients were either phlegm heat, blood stasis or Qi and blood deficiency. The TCM treatment principle for cancer using CHM followed the 4-part framework: (1) prescription of cancer sensitive herbs; (2) prescription of tonic herbs to enhance the function of the immune system; (3) prescription of herbs to relieve the patient’s symptoms; and (4) a long-term treatment to reduce the risk of recurrence, typically 5 years. The list of anticancer herbs and tonic herbs can be found in Supplementary Table 2 and Supplementary Table 3 for easy reference.
Median Survival of 21 Deceased Pancreatic Cancer Patients a .

Abbreviations: t, time; No., number; cum survival, cumulative survival.
T = 15, P(X > 15) = 0.52; t = 16, P(X > 16) = 0.41, Median survival T, thus (15-16):(15-T) = (0.52-0.41):(0.52-0.5), T = 15.2.
t (month) defined on the number of months of subjected enrolled after the diagnosis of pancreatic cancers.
No. entering interval defined on the number of subjects enrolled after the diagnosis.
Mortality condition defined on the number of death of subjects divided by the total number of subjects who were alive.
Survival Time and Treatment Conditions of 21 Cases.

Abbreviations: WM, Western medicine; TCM, traditional Chinese medicine.
Case 1 (Case No. 0000424)
Case 1 (male, age 77 years) presented with progressive asymptomatic jaundice in September 2001, with fatigue and 20-pound weight loss within 1 month. Serum total bilirubin was 100 µmol/L, alanine aminotransferase was 856 U/L, aspartate aminotransferase was 120 U/L, γ-glutamyl transpeptidase was 994 U/L, and CA19-9 was 323 U/mL. Pancreatic head cancer was confirmed after ultrasound scan, CT scan, and ERCP (Figure 1). Pathology of tumor was not available. Since surgery was unfeasible and the patient refused chemotherapy, only biliary stenting was performed for bile secretion bypass. The patient commenced sole treatment with CHM in October 2001. Prior to that, he weighed 95 pounds and had experienced weight loss, mild yellowish sclera, irregular chills and fever, poor appetite, fatigue, and dry and bitter mouth. He defecated 1 to 2 times/day. The TCM diagnosis included light purplish tongue, mild yellowish coating, and taut and slippery pulse. Using TCM theory, the syndrome differentiation was (1) dampness of heat with Qi stagnation, (2) phlegm and blood stasis, and (3) deficiency of Qi and blood. The first treatment formula prescribed included Bupleurum chinense DC, Scutellaria baicalensis Georgi, Angelica sinensis (Oliv.) Diels, Codonopsis pilosula (Franch.) Nannf., Atractylodes macrocephala Koidz., Poria cocos (Schw.) Wolf, Citrus medica L. var. sarcodactylis Swingle, Curcuma longa L., Curcuma phaeocaulis Valeton, Artemisia capillaris Thunb., Coix lacryma-jobi L. var. ma-yuen (Roman.) Stapf, Polyporus umbellatus (Pers.) Fries, Smilax glabra Roxb., Agrimonia pilosa Ledeb., Patrinia villosa Juss., and Hedyotis diffusa Willd. Follow-up prescriptions were adjusted based on the assessment of inadequate anticancer regimen and supplement deficiency with adherence to the syndrome differentiation practice of TCM. After 1 month of CHM treatment, his jaundice was relieved, liver function normalized, and general performance significantly improved. On November 21, 2001, CT scan showed no enlargement or metastasis of the existing tumor. He continued CHM treatment. Another follow-up CT scan (January 14, 2002) showed no tumor in the pancreas. With weight gain, improved appetite, and energy, the patient continued CHM until September 4, 2010. His OS was 9 years. He died at age 86 of old age rather than complications from pancreatic cancer.
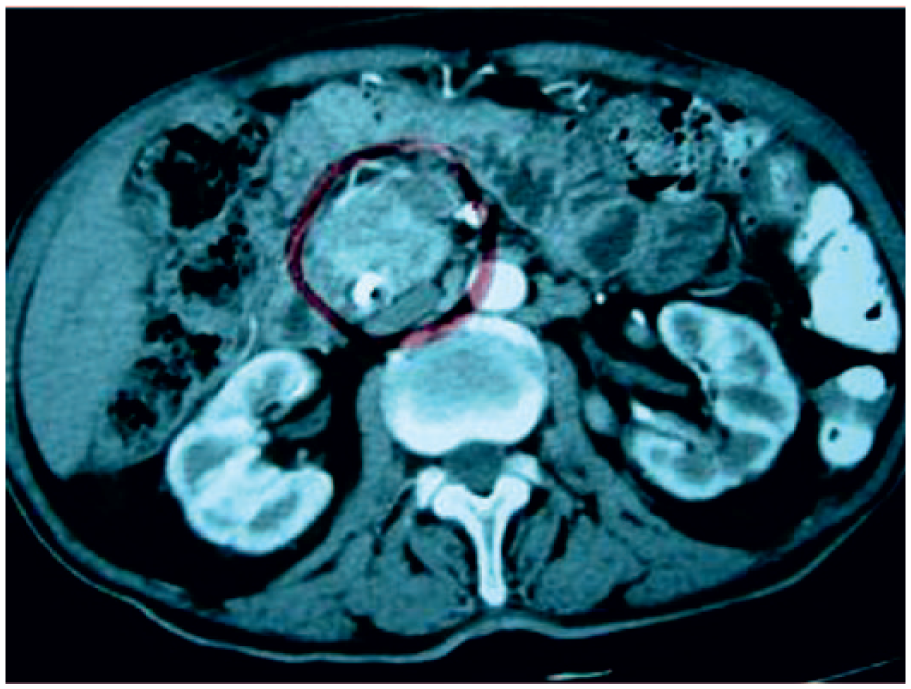
Computed tomography (CT) scan image of Case No. 0000424 (Case 1), who received Chinese herbal medicine (CHM) treatment only and had a prolonged survival of 9 years.
Case 2 (Case No. 0000942)
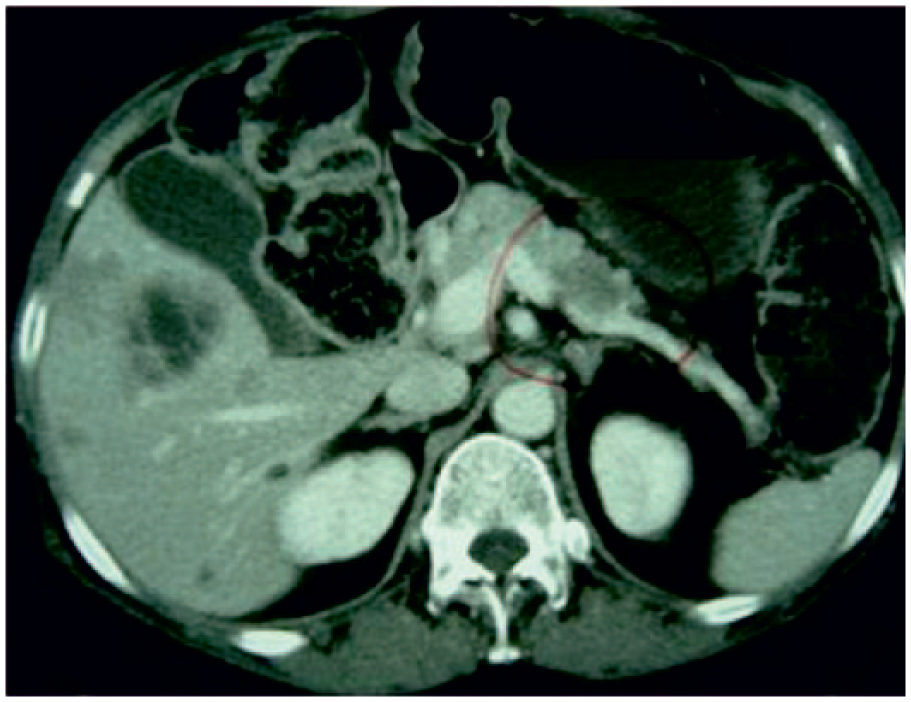
Case 2 (female, age 30 years) presented with jaundice and diarrhea in October 2005. Her blood test revealed anemia, total bilirubin 278 µmol/L, and poor liver function. CT examination confirmed pancreatic head carcinoma (Figure 2). She underwent surgery in November 2005; pathology revealed neuroendocrine carcinoma with liver metastasis. In 2006, she underwent a second surgery for liver metastasis. She did not undergo chemotherapy or radiotherapy and began TCM therapy on February 22, 2006. She presented with abdominal pain, 34-pound weight loss, pallor, fatigue, insomnia, and diarrhea 5 to 6 times/day, including at night. Blood tests revealed alkaline phosphatase 199 U/L, alanine aminotransferase 60 U/L, and aspartate aminotransferase 41 U/L. CHM treatment consisted of Smilax glabra Roxb., Agrimonia pilosa Ledeb, Hedyotis diffusa Willd, Forsythia suspensa (Thunb.) Vahl, Curcuma phaeocaulis Valeton, Vaccaria segetalis (Caryophyllaceae), Salvia miltiorrhiza Bunge, Artemisia capillaris Thunb., Trionyx sinensis Wiegmann, Panax ginseng C.A. Mey., Atractylodes macrocephala Koidz, and Wolfiporia extensa (Peck) Ginns. After 6 months of treatment, liver function tests normalized. The diarrhea and abdominal pain stopped, and the patient had a twice-daily normal defecation pattern and no sleep interruption. With good energy and normal complexion, she regained weight. In October 2009, the patient stopped CHM treatment for a little over 1 year. By December 2010, imaging studies indicated another liver metastasis. She resumed CHM treatment until April 2014, when chemotherapy and targeted therapy were recommended, which did not prolong her survival; she died on June 29, 2015. Despite 2 surgeries and liver metastasis, she survived for almost 10 years in good health with CHM treatment. The last observable medical record on March 8, 2014, noted that she had good appetite, a stable body weight of 115 pounds (net weight gain 24 pounds), and normal bowel movements. She could resume daily work without symptoms of abdominal pain, ascites, or jaundice. With only CHM treatment, she survived for 8 years in good health. She died 1 year after discontinuing CHM treatment and commencing chemotherapy and targeted therapy. The total survival time was 10 years.

Computed tomography (CT) scan image of Case No. 0000942 (Case 2), with liver metastasis, who survived 8 years with only Chinese herbal medicine (CHM) treatment after surgery.
Case 3 (Case No. 0001021)
CT scan of Case 3 (female, age 67 years) revealed pancreatic body carcinoma with multiple liver metastases (Figure 3). Biopsy confirmed neuroendocrine carcinoma. Her first consultation was on August 24, 2006. The patient was thin, fatigued, and constipated, without abdominal pain and jaundice. The TCM diagnosis indicated a pale-purplish tongue, yellow tongue fur, and a thin and weak pulse. Using TCM theory, the syndrome differentiation was (1) deficiency of Qi and blood, (2) phlegm and blood stasis, and (3) dampness heat with Qi stagnation. The treatment prescribed followed the principles of anticancer, body resistance strengthening, and syndrome differentiation. Without surgery, chemotherapy, or radiotherapy, the patient maintained a stable condition with the following CHM treatments: Smilax glabra Roxb, Agrimonia pilosa Ledeb, Salvia chinensis Benth, Hedyotis diffusa Willd, Forsythia suspensa (Thunb.) Vahl, Curcuma phaeocaulis Valeton, Salvia miltiorrhiza Bunge, Rheum officinale Baill, Panax ginseng C.A. Mey., Atractylodes macrocephala Koidz, Wolfiporia extensa (Peck) Ginns, Massa Medicata Fermentata, Trionyx sinensis Wiegmann, Taraxacum mongolicum Hand-Mazz., and Artemisia capillaris Thunb. After learning that neuroendocrine carcinoma usually develops slowly, she discontinued CHM treatment for over a year and her situation deteriorated. She died on January 1, 2011. Her OS was approximately 5 years.
Computed tomography (CT) scan image of Case No. 0001021 (Case 3), with a low-density carcinoma block in the pancreatic body, and liver metastasis. The patient survived for 3 years with Chinese herbal medicine (CHM) treatment alone. Death occurred 1 year after stopping CHM treatment.
Case 4 (Case No. 0004384)
In May 2011, Case 4 (female, age 58 years) sought medical consultation due to anemia and lack of appetite, and she was diagnosed with pancreatic head cancer. During surgery in June 2011, the tumor was deemed too large for removal. Within the same month, she developed obstructive jaundice. From August to October 2011, she received 6 cycles of chemotherapy. The tumor shrank and was surgically removed. Pathological cytology confirmed neuroendocrine carcinoma. Multiple brain metastases were found in May 2012, and she received 10 courses of radiotherapy and oral chemotherapy. She started CHM treatment on July 12, 2012, following presentation of headache, nausea and vomiting, staggering, deafness in the left ear, hand tremor, lower limb weakness, constipation, and insomnia. The TCM diagnosis indicated reddened tongue with white tongue fur and weak pulse. The prescription included Salvia chinensis Benth., Smilax glabra Roxb., Scutellaria barbata D. Don, Agrimonia pilosa Ledeb., Hedyotis diffusa Willd., Polygonum cuspidatum Sieb. Et Zucc., Curcuma longa L., Pinellia ternate (Thunb.) Breit., Acorus tatarinowii Schott., Angelica dahurica (Fisch. Ex Hoffm.) Benth. Ex Hook.f, Ligusticum chuanxiong Hort., Codonopsis pilosula (Franch.) Nannf., Atractylodes macrocephala Koidz., Poria cocos (Schw.) Wolf, Crataegus pinnatifida Bunge, Massa Medicata Fermentata, Hordeum vulgare L., Taraxacum mongolicum Hand.-Mazz., Astragalus membranaceus (Fisch.) Bunge, Angelica sinensis (Oliv.) Diels, Ziziphus jujuba Mill. Var. spinosa (Bunge) Hu ex H.F., Ostrea gigas Thunberg, and Glycyrrhiza uralensis Fisch. She continued with both Western and Chinese treatments for 2 years. CHM followed the principles of anticancer, regulating and nourishing, and syndrome differentiation approach to adjust the prescription. She died on May 2, 2014. The total survival time was 3 years.
Case 5 (Case No. 0004684)
In November 2012, Case 5 (male, age 54 years) presented with right leg pain. On examination, multiple vertebrae, including cervical, were found to be damaged. Further examination confirmed the diagnosis of pancreatic head cancer with liver and bone metastasis. Pathology of tumor was not available. He was at high risk of developing paraplegia and commenced radiotherapy immediately. He started CHM treatment on January 3, 2013. The initial prescription included Salvia chinensis Benth., Chinemys reevesii (Gray), Drynaria fortunei (Kunze) J.Sm., Lycium barbarum L., Dipsacus asperoides C.Y. Cheng et T.M. Ai, Scutellaria barbata D. Don, Agrimonia pilosa Ledeb., Smilax glabra Roxb., Hedyotis diffusa Willd., Forsythia suspensa (Thunb.) Vahl, Curcuma phaeocaulis Valeton, Lycopus lucidus Turcz. var. hirtus Regel, Trionyx sinensis Wiegmann, Astragalus membranaceus (Fisch.) Bunge, Angelica sinensis (Oliv.) Diels, Codonopsis pilosula (Franch.) Nannf., Atractylodes macrocephala Koidz., Poria cocos (Schw.) Wolf, Massa Medicata Fermentata, Uncaria rhynchophylla (Miq.) Jacks., Prunella vulgaris L., and Glycyrrhiza uralensis Fisch. The principles of anticancer, regulating and nourishing, and syndrome differentiation approach were used to subsequently adjust the prescription. During CHM, he continued chemotherapy. After 1 year, 4 months of both Chinese and conventional medicine, he died in October 2014. The total survival time was close to 2 years.
Discussion
Conventional medicine continues to have a progressive role in treating pancreatic cancer.8,20 Surgery and chemotherapy are conventional treatments for pancreatic cancer. Although surgery was feasible and performed for Case 2, no chemotherapy was performed. This enabled an improved quality of life, and the patient could resume normal work without painful symptoms and with a good appetite and steady weight for 8 years. The patient survived 10 years and died within 1 year of CHM termination and commencement of targeted therapy. This suggests the superior potential of TCM in treating pancreatic cancer, not only in combatting disease but also in alleviating symptoms and improving the quality of life and survival. Only the continuous intake of CHM seems to be able to prolong survival.
Ninety percent of pancreatic cancers are adenocarcinomas; less than 5% are neuroendocrine carcinomas. Neuroendocrine carcinoma progresses more slowly and has a higher survival rate 21 than pancreatic adenocarcinoma. The National Cancer Institute’s SEER survival monograph showed that the 5-year survival rate for 411 cases of neuroendocrine carcinoma was 32.2%. 7 The survival rate for pancreatic neuroendocrine carcinoma is still worse than that of breast, colon, and nasopharyngeal carcinomas, which have 5-year survival rates of 73%, 47%, and 34%, respectively. 22 Therefore, the treatment for pancreatic neuroendocrine carcinoma should be carefully managed. The condition of Case 3 was stable for approximately 3 years during CHM treatment and deteriorated after discontinuing CHM treatment for over 1 year; her survival time was 5 years. This patient might have had a longer survival if she had continued CHM treatment.
An in vitro study confirmed the effectiveness of Chinese herbs, including Salvia chinensis (Labiatae), Rheum palmatum (Polygonaceae), Anemarrhena asphodeloides (Lilaceae), Artemisia argyi (Compositae), Commiphora myrrha (Burseraceae), Vaccaria segetalis (Caryophyllaceae), and Uncaria rhynchophylla (Rubiaceae), against pancreatic adenocarcinoma. 23 Additionally, the Chinese herb curcumin has synergistic effects with celecoxib for inhibiting the growth of pancreatic adenocarcinoma, and combination therapy allows for lowering the celecoxib dosage (and therefore its side effects and related toxicities). 24 The Chinese herbs SPES and PC-SPES exhibit significant effect on pancreatic adenocarcinoma compared with gemcitabine in vitro. 25 The 8 major ingredients are Dendranthema morifolium Tzvel, Ganoderma lucidum Karst, Glycyrrhiza glabra L., Isatis indigotica Fort, Panax pseudoginseng Wall, Rabdosia rubescens Hart, Scutellaria baicalensis Georgi, and Serenoa repens Small. Any treatment that is safe and effective is appropriate. It is obvious from this case series and other studies that TCM can provide safe and effective treatment for pancreatic cancer.12,26 Taiwan national data showed a consistent result with this case series although we did not know which exact types of pancreatic cancers were included and treated. This case series provide an illustration of the types of pancreatic cancers being managed in Hong Kong and the direct projection of average survival duration that may align with clinical practice from a bottom-up approach. Chinese and conventional medicine each have their merits and weaknesses and have a high potential when integrated. Cross-discipline research and communication should be pursued to improve mutual understanding so evidence-based medical decisions can be made.27-29
An explorative and open-minded attitude is paramount to enhance scientific advancement, which must respect facts and be unconstrained by bias. The philosophy behind TCM is very complex and may not comply perfectly with modern scientific guidelines, but methods have been developed for TCM researchers to satisfy these guidelines.30-32 Many years of wisdom have accumulated in the practice of TCM, which has been practiced, reflected upon, and analyzed repeatedly. Alternative approaches to improving patient outcomes, besides WM, must be explored.
This study reports a case series only, and these clinical cases are limited by the scale of the clinic; a limited number of cases can be recruited by one CMP. In most cases, patients received both conventional medicine and CHM, as conventional medicine is the standard treatment for pancreatic cancer and very few patients refuse conventional treatment. This case series was a single-arm study in pancreatic cancer patients who received CHM; a comparison group that received only conventional care is worth investigating. We recognize the study design’s limitation, which does not allow an RCT, since conducting RCTs for pancreatic cancer is difficult, 20 particularly considering most patients’ short life expectancy. The generalizability of the study was considered; patients from different sex and age groups were recruited, and the age distribution was similar to that of pancreatic cancer patients in Hong Kong. We also endeavored to recruit a large group of patients. We propose that, in the future, case series be considered an alternative approach for evaluating the effectiveness of CHM for pancreatic cancer treatment. This is the first case series to reflect with open-mindedness the successful use of CHM to manage cases of this life-threatening disease that could not be otherwise treated or targeted.
Conclusion
This retrospective case series illustrates the health outcomes (prolonged survival) following CHM treatment in pancreatic cancer patients in compliance with TCM theory. The survival of patients who received CHM ranged from 4 months to 10 years, with a mean 29.6 months and median 15.2 months. Seventy-six percent survived at least 1 year. The results support a better prognosis for pancreatic cancer patients who receive CHM treatment compared with conventional treatment alone. This study can facilitate discussion on the role of CHM in treating pancreatic cancer. Further investigation should be conducted to identify which specific herbs are beneficial for these patients.
Supplemental Material
Supplementary_Figure_1 – Supplemental material for Chinese Herbal Medicine Effectively Prolongs the Overall Survival of Pancreatic Cancer Patients: A Case Series
Supplemental material, Supplementary_Figure_1 for Chinese Herbal Medicine Effectively Prolongs the Overall Survival of Pancreatic Cancer Patients: A Case Series by Wendy Wong, Bing Zhong Chen, Allyson Kin Yan Lee, Adrian Ho Cheung Chan, Justin Che Yuen Wu and Zhixiu Lin in Integrative Cancer Therapies
Supplemental Material
Supplementary_Table_1_20181219_final – Supplemental material for Chinese Herbal Medicine Effectively Prolongs the Overall Survival of Pancreatic Cancer Patients: A Case Series
Supplemental material, Supplementary_Table_1_20181219_final for Chinese Herbal Medicine Effectively Prolongs the Overall Survival of Pancreatic Cancer Patients: A Case Series by Wendy Wong, Bing Zhong Chen, Allyson Kin Yan Lee, Adrian Ho Cheung Chan, Justin Che Yuen Wu and Zhixiu Lin in Integrative Cancer Therapies
Supplemental Material
Supplementary_Table_2_and_3_pancreatic_cancer_herbs_tonic_20181219_final – Supplemental material for Chinese Herbal Medicine Effectively Prolongs the Overall Survival of Pancreatic Cancer Patients: A Case Series
Supplemental material, Supplementary_Table_2_and_3_pancreatic_cancer_herbs_tonic_20181219_final for Chinese Herbal Medicine Effectively Prolongs the Overall Survival of Pancreatic Cancer Patients: A Case Series by Wendy Wong, Bing Zhong Chen, Allyson Kin Yan Lee, Adrian Ho Cheung Chan, Justin Che Yuen Wu and Zhixiu Lin in Integrative Cancer Therapies
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.