
Abstract
Background. Intratumoral (IT) injection of European mistletoe (Viscum album L) preparations might induce local tumor response through combined cytotoxic and immunomodulatory actions of the preparations. Although promising in vitro and in vivo data, along with clinical case studies suggest the need for validation of this hypothesis in prospective trials, the safety of IT mistletoe injections has yet to be thoroughly assessed. Methods. The present study summarizes the practice and safety of off-label IT mistletoe therapy within the Network Oncology, a conjoint clinical registry of German hospitals and outpatients specialized in anthroposophic and integrative medicine. Demographic, diagnosis and treatment data of cancer patients who received IT mistletoe applications between 2007 and 2013 were assessed. Suspected adverse drug reactions (ADRs) were analyzed in terms of type, frequency, severity, seriousness and potential risk factors. Results. A total of 123 cancer patients received 862 IT mistletoe injections (preparations from Abnoba, Helixor and Iscucin). The most commonly applied preparations were Abnoba viscum Fraxini (71 patients) and Helixor Mali (54 patients). Of the total patients, 26 patients (21.1%) experienced 74 ADRs. All ADRs were in response to either Abnoba viscum Fraxini (25.4% of exposed patients) or Helixor Mali (18.5% of exposed patients). ADRs were mostly body temperature or immune related and of mild (83.8%) or moderate (14.9%) intensity. Only one possible ADR was described as severe (hypertension) and no serious ADRs occurred. The frequency of ADRs to IT mistletoe injections was 3 times and 5 times higher than has previously been found for subcutaneous and intravenous applications of mistletoe, respectively. Conclusion. IT injection of mistletoe preparations resulted in a relatively high frequency of ADRs. Nearly all ADRs were mild to moderate however, and no serious ADRs occurred. Furthermore, it is possible that immune-related ADRs such as pyrexia and local inflammatory reactions might be critical for tumor response. In light of these results, IT mistletoe therapy seems to be safe and prospective trials are recommended.
Keywords
Introduction
In efforts to boost the effectiveness of anticancer drugs, the past decade has seen increasing numbers of investigators trialing intratumoral (IT) drug delivery approaches. Procedures range from injections into easily accessible, advanced solid malignancies, such as melanomas, to endoscopic ultrasound (EUS)-guided injections for pancreatic cancer.1,2 Anticancer agents that have been applied via IT injection include chemotherapy agents (eg, vincristine), oncolytic viruses (eg, ONYX-015), immunomodulators (eg, agonistic CD40 monoclonal antibodies), and autologous immune cells (eg, dendritic cells).2-9 Potential advantages of IT delivery of anticancer drugs include better anticancer effectiveness through achievement of high concentrations of anticancer agents within the tumor microenvironment and reduced systemic adverse drug reactions (ADRs) and drug resistance.5,10-12 In general, single-agent efficacy has been less than satisfying to date; however, promising results have been achieved using IT-administered targeted therapies, combined with conventional chemotherapy or radiation.10,13-17
A major challenge of cancer therapy is immune resistance orchestrated by the tumor microenvironment, which promotes tumor survival. 18 European mistletoe (Viscum album L) extracts and constituents, notably lectins and viscotoxins, show anticancer activity as well as immunomodulating properties.19-22 Used in anticancer therapy in central Europe since 1917, anthroposophic mistletoe preparations (ie, Abnoba viscum, Helixor, Iscador, Iscucin, Isorel) are usually injected subcutaneously (SC), as an adjuvant therapy to conventional cancer treatments. The aims of SC-injected mistletoe (also intravenous [IV]), are to boost the immune system, improve patient health-related quality of life, and reduce ADRs associated with conventional therapies.23,24 On the other hand, IT drug delivery represents a more recent and also promising application of mistletoe therapy which might effectively result in tumor shrinkage because of the combined cytotoxic and immunomodulatory properties of mistletoe.22,25,26 In vitro studies have shown induction of apoptosis and necrosis depending on mistletoe extract concentrations in a wide range of tumor cells.19-21,25,27,28 Preclinical in vivo studies have likewise been promising, with IT injection of tumors in a range of mice models and in horses inhibiting tumor growth and inducing partial or complete regressions.25,26,28,29 As for clinical use, several groups have published case studies describing partial or complete tumor remission by IT mistletoe therapy alone or in combination with conventional therapies.30-33 A recent retrospective study by Schad et al, 34 which included 39 pancreatic patients who received a total of 223 IT mistletoe injections in addition to conventional therapies, suggests that IT applied mistletoe might have contributed to an improved overall survival. Prospective clinical studies designed to confirm efficacy for IT or multimodal mistletoe therapy are therefore required. As an off-label use of mistletoe preparations, however, a concise safety profile for IT mistletoe therapy has not yet been established. The present study describes the off-label use of IT mistletoe injections in clinical practice within an integrative oncological setting in Germany and assesses the safety of its use. 35 In addition to describing IT mistletoe–induced ADRs in terms of type, frequency, and severity, these results are compared with data from previous studies regarding the safety of SC and IV applications of mistletoe.36,37
Methods
Study Design and Data Sources
A multicenter, observational study was carried out within the Network Oncology (NO), a conjoint clinical registry of German hospitals and out-patient practitioners specialized in anthroposophic medicine.35,38 As described previously, documentation officers extract patient information, cancer diagnoses, therapies, adverse events, and disease progress from patient files and record data using the QuaDoSta (Quality management, Documentation and Statistics) software that was developed at Havelhoehe Research Institute.36,37,39 The NO documents detailed information about mistletoe therapies received, including preparation types, dosage data, therapy start and end dates, and related adverse events. The NO project has received a positive vote from the ethical committee of the Medical Association Berlin. In the present study, we analyzed all data relating to IT mistletoe use (including intralesional and peritumoral) that were recorded for consenting patients between 2007 and 2013. All analyses were conducted and figures created with R version 2.15.1. 40
Selection and Analysis of Patient Data
All patients with a valid identification number, birth date, gender, cancer diagnosis date, ICD-10 code, and at least a start or end date for IT mistletoe therapy were included in the final analyses. Descriptive statistics were used to describe patient demographics. Disease stages of patients at diagnosis and at the start of IT mistletoe therapy were classified according to the Union for International Cancer Control (UICC) staging. Types and doses of mistletoe applied and conventional therapies received are summarized.
Analysis of Safety Data
All mistletoe-related adverse events reported by physicians were assessed by the investigators. Local reactions <5 cm in size and increased body temperatures <38°C are considered as expected effects of mistletoe therapy and were not recorded as ADRs. In contrast, local reactions >5 cm in size and increased body temperatures >38°C, along with all other adverse events, were considered as suspected mistletoe ADRs if a causal relationship between mistletoe and an event was described by physicians as at least a reasonable possibility. ADRs were classified as MedDRA® 15.0 preferred terms (developed under the auspices of the International Conference on Harmonization [ICH]) and grouped by System Organ Class.41,42 ADRs were evaluated in terms of severity (grades 1 to 5) according to the Common Terminology Criteria for Adverse Events v4.0 43 and designated as serious or nonserious according to ICH guidelines. 41 The numbers of ADRs per person were determined, and the management and outcome of ADRs are summarized. To identify potential risks for experiencing an ADR, doses and preparations to which patients experienced ADRs were considered in relation to the doses and preparations to which patients were exposed. Furthermore, the relative frequency of patients experiencing ADRs in response to IT mistletoe injections was compared with SC and IV mistletoe applications.36,37
Results
Patient Characteristics and Therapies
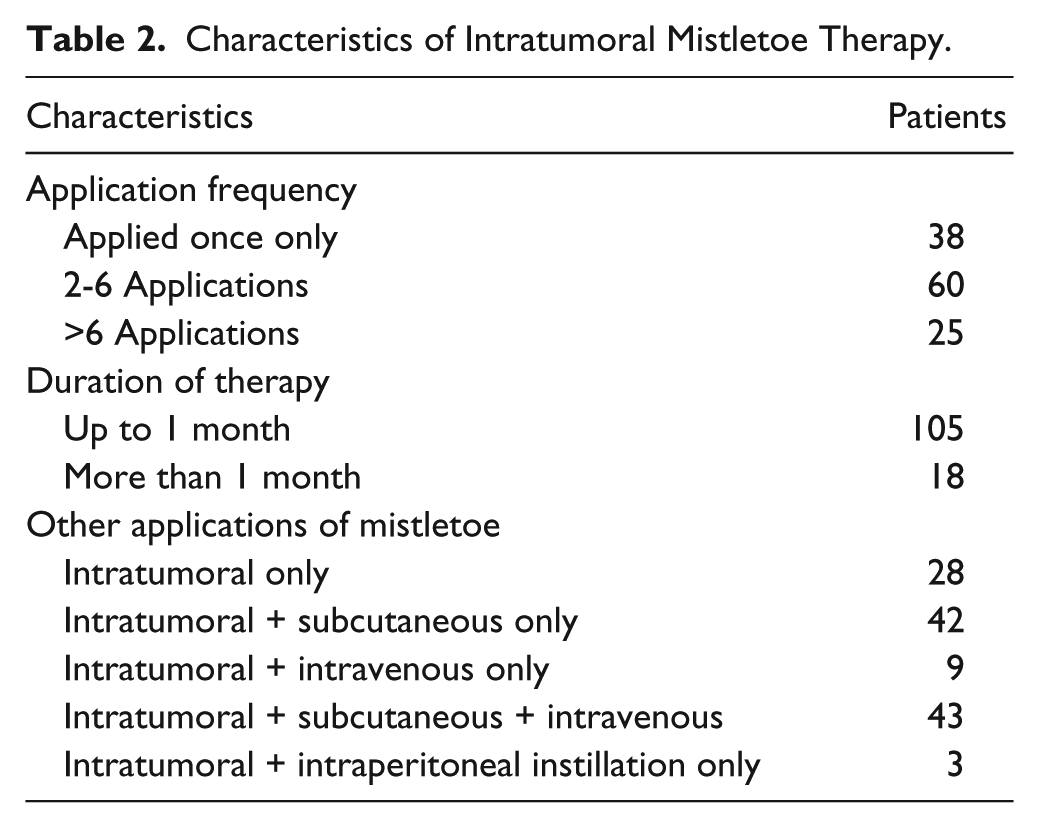
A total of 123 cancer patients who received IT mistletoe injections were analyzed. Patients consisted of 49 men (39.8%) ranging from 27 to 85 years of age and 74 women (60.2%) ranging from 25 to 86 years. The median age for both genders was 61 years, with an interquartile range of 52.3 to 66.0 years for women and 53.0 to 68.0 years for men. Pancreatic cancer patients made up 48.0% of all patients, with lung, breast, colorectal and liver cancer patients making up 13.0%, 12.2%, 8.9%, and 7.3%, respectively (Table 1). Almost half of the patients (47.2%) were found to have stage IV cancer on first documentation of UICC stage (at or within 1 month of first diagnosis). By the commencement of IT mistletoe therapy (median = 7 months after first diagnosis, interquartile range = 1.6 to 21.7 months), 93 out of 112 (83.0%) patients with a documented up-to-date UICC stage had stage IV cancer (Table 1). In addition to receiving IT mistletoe injections, 77.2% of patients also received mistletoe preparations by another form of administration (Table 2). In terms of conventional cancer therapies, 80.5% of patients had a surgery, 75.6% had a systemic therapy (chemotherapy, 68.3%; signal transduction inhibitors, 13.0%; bisphosphonates, 11.4%; immunotherapy, 8.1%; hormonal therapy, 5.7%), and 26.8% received radiation therapy. In contrast to IV mistletoe therapy, IT injections were not applied immediately prior to systemic or radiation therapies. Four patients received IT injections on the same day as surgeries (2 atypical liver resections, 1 diagnostic tracheabronchoscopy, and 1 port implantation).
Patient Cancer Entities and Union for International Cancer Control (UICC) Stages at the Commencement of Intratumoral Mistletoe Therapy.
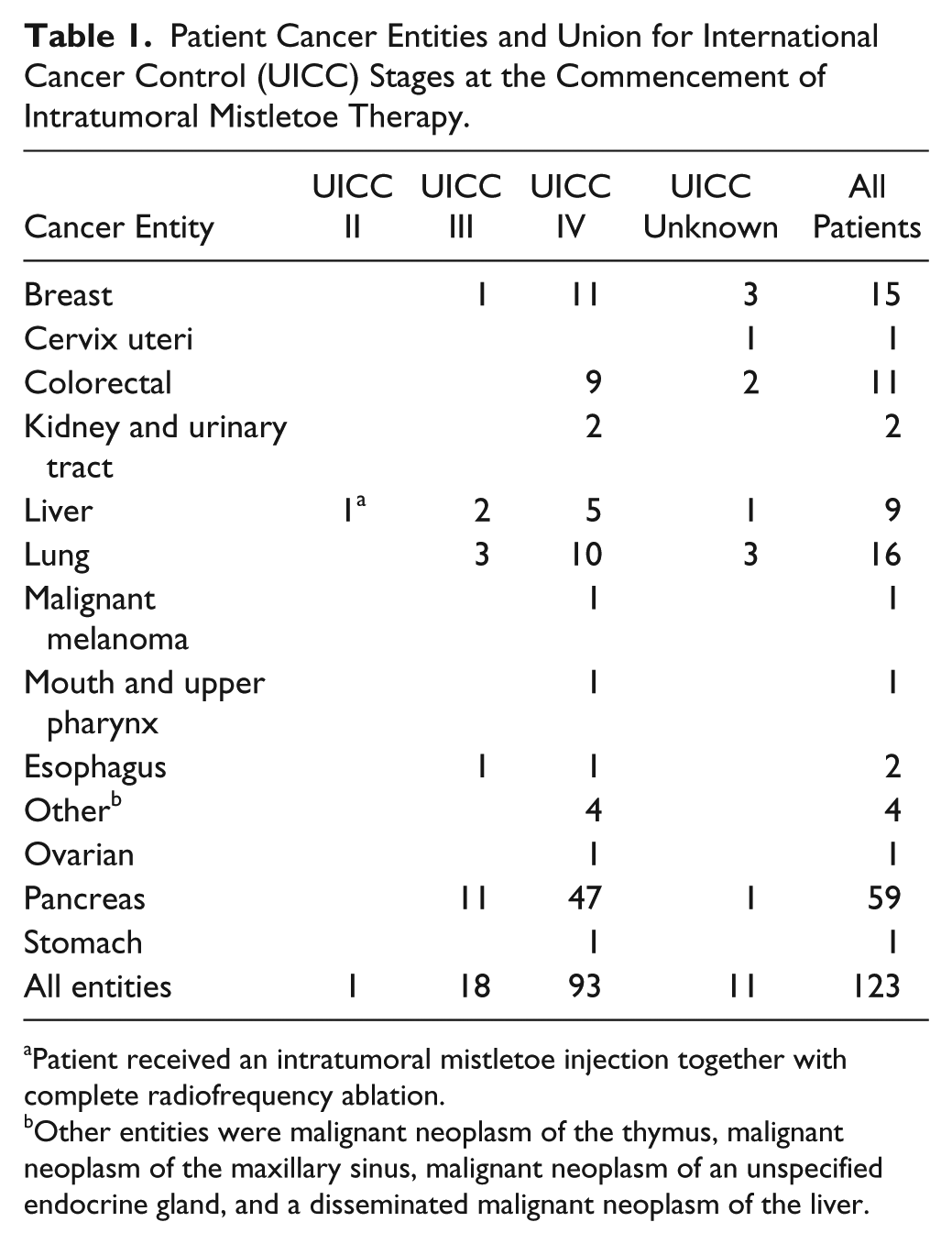
Patient received an intratumoral mistletoe injection together with complete radiofrequency ablation.
Other entities were malignant neoplasm of the thymus, malignant neoplasm of the maxillary sinus, malignant neoplasm of an unspecified endocrine gland, and a disseminated malignant neoplasm of the liver.
Characteristics of Intratumoral Mistletoe Therapy.
IT Mistletoe Therapy
A total of 862 IT mistletoe injections were recorded in 123 patients between 2007 and 2013. Most patients received multiple IT mistletoe applications; however, treatment usually lasted 1 month or less (Table 2). Preparations from Abnoba and Helixor were the most commonly applied, and 1 patient received 3 injections of Iscucin Tiliae (Table 3). IT-injected preparations were almost exclusively preparations of mistletoe that were grown on either Fraxini or Mali host trees. Because of differences in their production, mistletoe dose ranges vary significantly depending on the preparation type. Administered doses of Abnoba viscum preparations ranged from 0.02 to 250 mg, with a median dose of 60 mg (Figure 1). Helixor doses ranged from 50 to 1400 mg with a median of 500 mg (Figure 1). The only patient to receive Iscucin Tiliae received 2, 5, and 6 ampoules of Strength H (concentration 20−1), the most potent Iscucin concentration, on 3 occasions during a 2-week period.
Recorded Applications of Different Mistletoe Preparations.
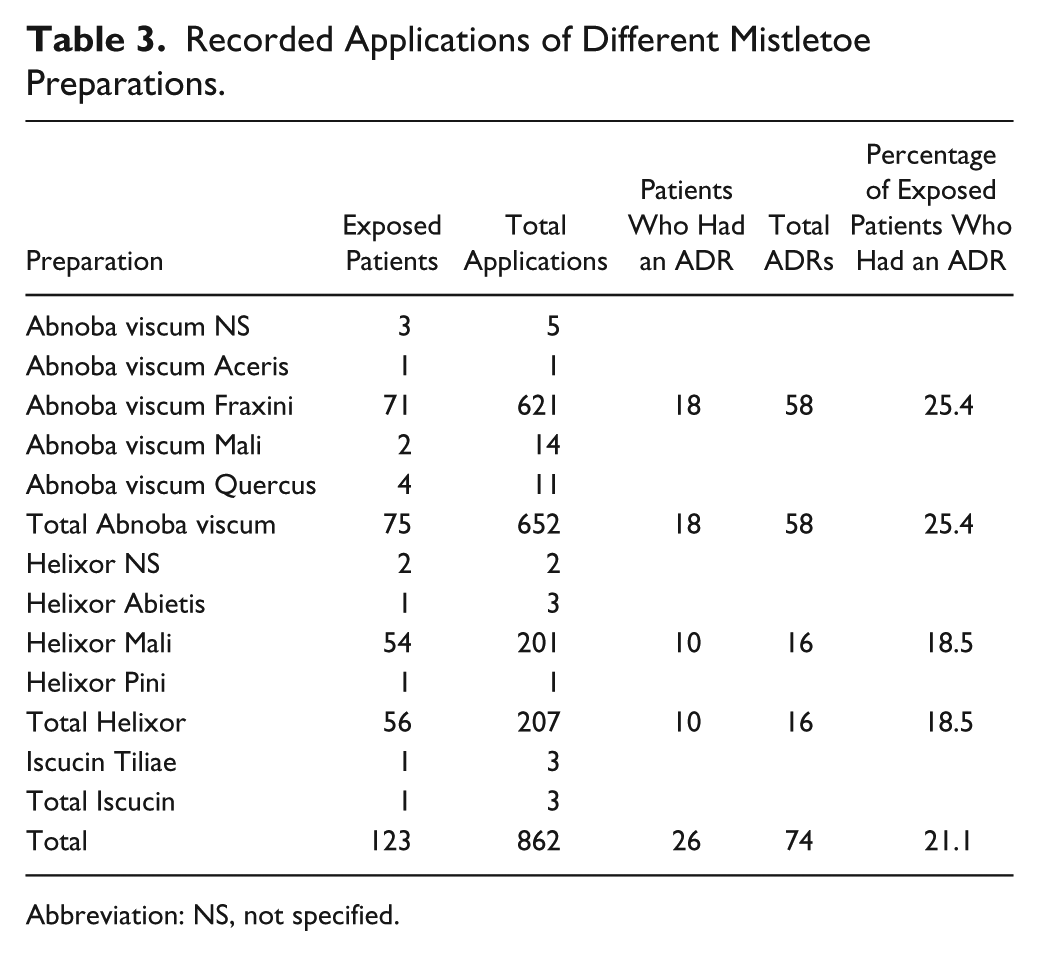
Abbreviation: NS, not specified.
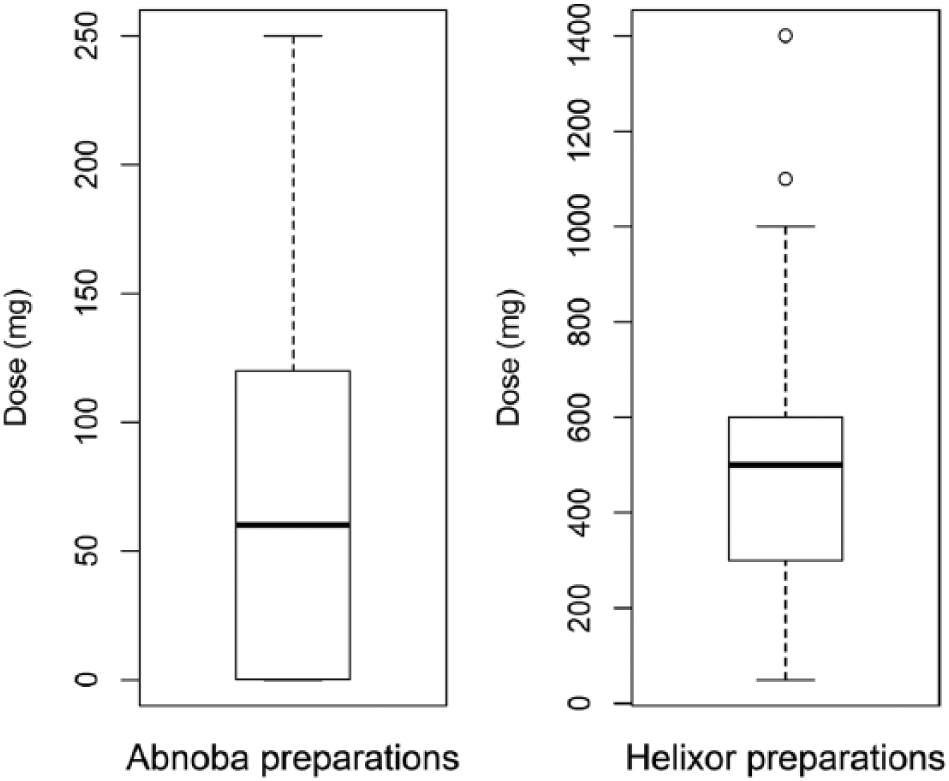
Doses at which intratumoral mistletoe applications were given with respect to preparation type. Horizontal lines within boxes show median values, boxes show 25% to 75% data ranges; the whiskers extend by 1.5 times the interquartile range, and circles represent outliers. Note the large differences in scale of the y-axes.
ADRs Attributed to IT Mistletoe Therapy
Of 123 patients who received IT mistletoe injections, 26 patients (21.1%) experienced a total of 74 ADRs (Table 4). Among them, 10 patients had 1 ADR, 6 had 2 ADRs, 3 had 3 ADRs, 1 had 4 ADRs, 2 had 5 ADRs, 2 had 6 ADRs, 1 had 8 ADRs, and 1 had 9 ADRs. Most ADRs were classified as “general disorders and administration site conditions” (55.4% of ADRs, 17.1% of total patients) or “gastrointestinal disorders” (28.4% of ADRs, 8.9% of total patients). In terms of ADR severity, 83.8% of ADRs (62 patients) were judged to be mild/grade 1, 14.9% (11 patients) to be moderate/grade 2, and 1.4% (1 patient) to be severe/grade 3. The moderately intense ADRs were vomiting, nausea, and pain and 8 cases of pyrexia (>39°C to <40°C). A pancreatic cancer patient received an IT injection of 140 mg Abnoba viscum Fraxini while under sedation with 100 mg propofol, and experienced a short period of postinterventional hypertension up to 240/130 mm Hg, without clinical symptoms. Blood pressure returned to baseline after administration of piritramide, sublingual nitroglycerin, and enalapril. The patient received tramadol as a baseline pain remedy and also had piritramide for pain relief following a previous IT mistletoe application and on other occasions. One week before the hypertensive episode, the patient was admitted for bile duct stent occlusion. Because of low blood pressure, antihypertensive treatment with metoprolol and enalapril was paused. Metoprolol was reintroduced 4 days prior to the IT mistletoe application and enalapril 2 days prior, but at a lower dosage. Although it is not clear whether this event was a reaction to mistletoe, it cannot be ruled out and, therefore, must be considered as a severe suspected ADR. Among all other patients who experienced ADRs, 1 patient with moderate pyrexia had a reduction in mistletoe dose; but no further ADRs required treatment, and no patient stopped IT mistletoe therapy because of an ADR. All patients completely recovered from mistletoe-related ADRs, and there were no life-threatening or serious ADRs.
Adverse Drug Reactions Attributed to Intratumoral Mistletoe Therapy.
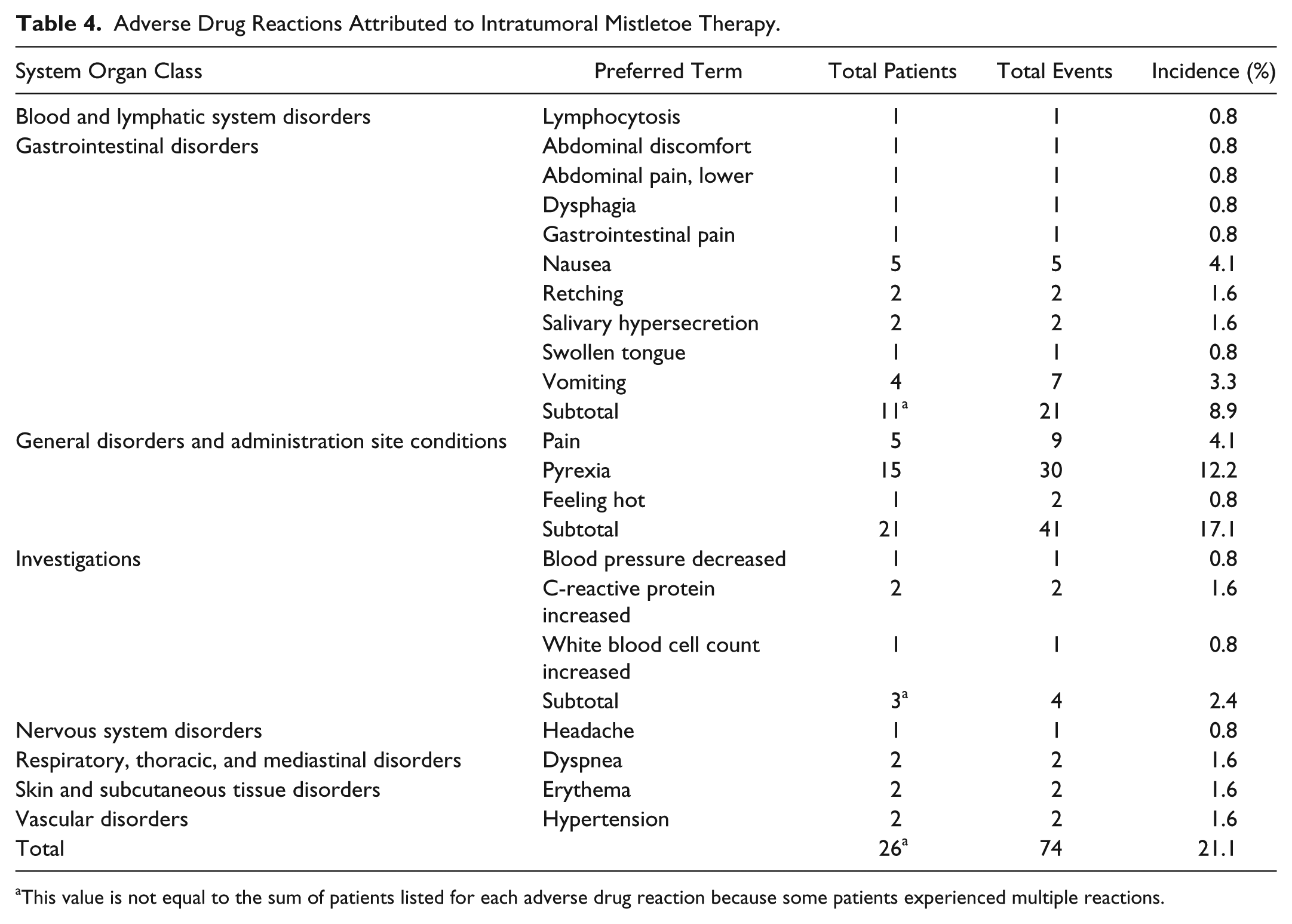
This value is not equal to the sum of patients listed for each adverse drug reaction because some patients experienced multiple reactions.
Investigation of Patients Who Experienced ADRs to IT Mistletoe Therapy
Among the 26 patients who experienced ADRs, there were 21 pancreatic, 2 breast (pyrexia, feeling hot, dyspnea, blood pressure decreased), 1 liver (pyrexia, nausea, vomiting), 1 lung (pyrexia), and 1 esophagus (dysphagia) cancer patients. Of the 4 patients who received an IT mistletoe injection on the same day as having a surgery, none experienced an ADR.
To investigate whether IT application of high mistletoe doses is associated with an increased risk of experiencing an ADR, doses at which ADRs occurred were assessed in relation to doses to which patients were exposed. For Abnoba viscum preparations, ADR doses ranged from 20 to 220 mg, with a median dose of 80 mg (median exposure dose was 60 mg). For Helixor preparations, ADR doses ranged from 100 to 1000 mg, with a median of 450 mg (median exposure dose was 500 mg). No ADRs occurred in response to 3 applications of Iscucin. For 3 out of the 26 patients who experienced an ADR, it was their first-ever exposure to mistletoe, and for 9, it was their first IT mistletoe injection. This means that every 10th patient (12 out of 123) experienced an ADR on their first IT mistletoe injection. Of the 14 patients (out of 26) who did not react to their first IT injection, 9 later experienced an ADR after an increase in mistletoe dose and 1 after a change in mistletoe preparation. Also, 21 patients had more IT mistletoe injections after experiencing an ADR, and of these, 13 experienced 1 or more additional ADRs.
Abnoba viscum Fraxini and Helixor Mali were the only preparation types to which patients reacted (Table 3). Although more patients reacted to Abnoba viscum Fraxini (25.4%) than to Helixor Mali (18.5%), the types of ADRs were similar for both preparations (mostly pyrexia and pain at the administration site, along with nausea and vomiting).
Comparison of IT Mistletoe With Subcutaneous and IV Mistletoe
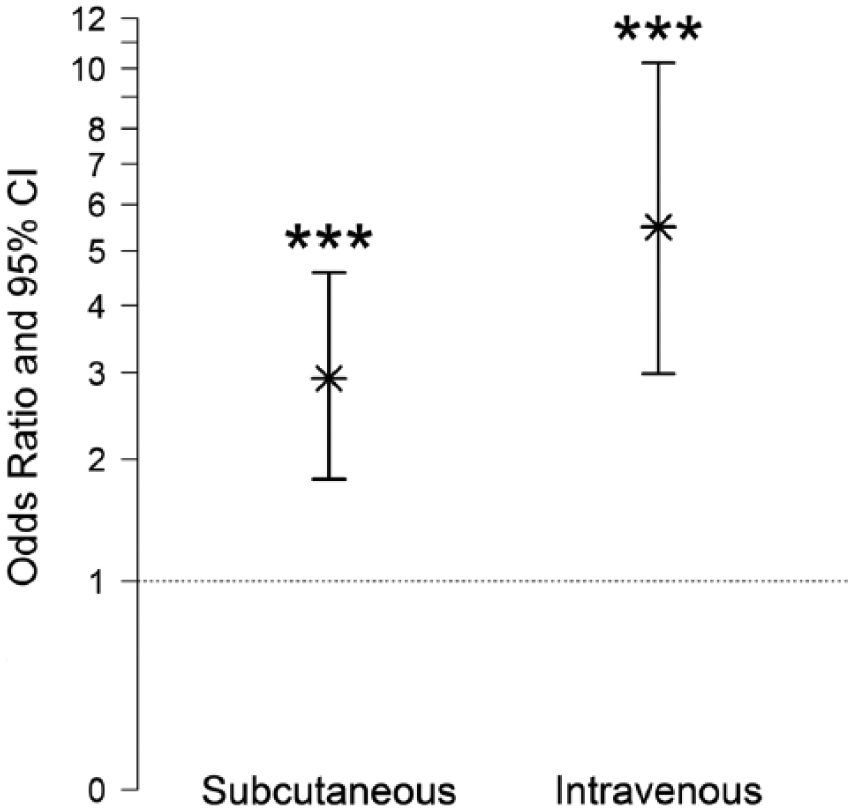
The relative frequency of ADRs in IT mistletoe-treated patients was compared with previously published results on the relative frequencies of ADRs in patients who received SC or IV mistletoe therapies.36,37 It was found that patients were almost 3 times more likely to experience an ADR to IT injections compared with SC injections and 5 times more likely compared with IV infusions (Figure 2).
Discussion
The present study assessed 123 patients who received 862 IT mistletoe applications. Over a fifth of patients (21.1%) experienced at least 1 ADR, and among those patients, the median number of ADRs per patient was 2. Consistent with the literature, “general disorders and administration site conditions,” especially pyrexia, were the most common types of ADRs.34,44-46 This is not surprising because mistletoe preparations contain substances with known immunostimulatory effects, especially mistletoe lectin I. 47 Interestingly, and differing from previous findings regarding ADRs to SC and IV mistletoe applications, “gastrointestinal disorders” were the next most common ADR type (8.9% of patients and 28.0% of ADRs). Of the 10 patients who experienced gastrointestinal disorders such as nausea, vomiting, and abdominal discomfort or pain, 9 were pancreatic cancer patients, and 1 patient had liver cancer. Although it is possible that local IT mistletoe-induced inflammation might have irritated the gastrointestinal tract in some patients, it should be noted that pain, nausea, and vomiting can also be symptoms of advanced-stage pancreatic and liver cancers. Furthermore, the act of piercing the peritoneum can induce nausea and vomiting. It is, therefore, difficult to assess the causality of such ADRs. Similarly, dysphagia (difficulty swallowing) that occurred in a patient diagnosed with stage III esophageal cancer could have been a result of local inflammation induced by IT mistletoe injection or a disease-related event.
In terms of severity, nearly all ADRs were judged to be mild or moderate; however, 1 patient experienced a short period of severe, postinterventional hypertension. Hypertension is not an expected reaction to mistletoe, and we were only able to find 1 similar report in the literature, which was hypertension following SC application of aviscumine, a recombinant form of mistletoe lectin. 48 More commonly, mistletoe is reported to have a hypotensive effect and has even been used in the treatment of hypertension.49-51 Nevertheless, the suspected ADR may have been related to IT injection of a high mistletoe dose or was possibly a result of suboptimal hypertension treatment preintervention or insufficient pain management postintervention.
No strong conclusions could be arrived at with respect to the relationship between mistletoe dose and ADR risk in the current study. ADRs mostly occurred in response to the very first IT mistletoe injection (every 10th patient) or after an increase in dose or change of preparation. Abnoba viscum Fraxini and Helixor Mali preparations, both of which have high lectin contents,52-54 appear to be associated with a higher risk of ADRs. However, these preparations were also the most frequently applied preparations by far, giving rise to a strong bias and preventing an accurate conclusion.
In terms of ADR frequency, we found that patients were almost 3 times more likely to experience an ADR to IT injections compared with SC injections and 5 times more likely compared with IV infusions. Patients were also more likely to experience multiple ADRs to IT injections.36,37 These differences were not likely to be a result of differing demographics because there were no significant differences between the 3 treatment groups in terms of age and gender. The elevated frequency of ADRs in response to IT injections compared with SC injections might be explained by the fact that IT injections typically involve administration of much higher doses of mistletoe. Whereas the IT doses administered were also slightly higher on average than the IV doses, IV dosage involves slow infusion of mistletoe preparations into the bloodstream, allowing rapid dispersal throughout the circulatory system. IT injection on the other hand, involves immediate delivery of high doses of mistletoe preparations into a partially restricted and immune-cell-populated area (the tumor microenvironment). It is, therefore, not surprising that IT injection is frequently accompanied by pyrexia-inducing local inflammation. 46
IT injection of mistletoe preparations has previously been associated with causing a moderately high frequency of ADRs.34,45,46 A retrospective study by Orange 45 found that high-dose IT mistletoe therapy posed a significant treatment burden. It was reported that patients were motivated to tolerate these effects, however, and that apart from hypersensitivities (pruritus, urticaria), most ADRs were appreciated as desirable in the context of the aim of eliciting a significant immune response. Frequently occurring ADRs to “high dose mistletoe febrile induction therapy” were grade-1 to -2 fevers, 12- to 24-hour sickness behavior, fatigue, chills, flu-like symptoms, and inflammatory reactions at the injection sites. 45 In another study in which significant disease responses with IT mistletoe treatment of exophytic bronchial carcinomas were reported, half of the patients developed pyrexia. 46 A common finding among these studies and our own is that although a high frequency of ADRs occurred in response to IT injections, most ADRs were mild to moderate in intensity, with few severe ADRs occurring and no life-threatening (grade 4) or serious ADRs.
An important observed commonality among many studies investigating high-dose mistletoe therapy, whether involving IT injection or other application types, is demonstration of an association between immune response and therapeutic benefit. Orange 45 has suggested that robust febrile responses may be required for breaking tumor escape in the host. He has commented extensively on the importance of application type and initial dose, arguing that the use of high doses of mistletoe for IT administration at the beginning of treatment is critical for achieving tumor response. Furthermore, significant tumor responses were observed with combined regimes of high-dose IT and IV applications, particularly if fever was elicited.45,55,56 Results presented by Büssing et al 57 indicate that the induction of moderate local reactions, compared with no or mild local reactions, in response to SC mistletoe application was associated with improved T-cell function and health-related quality of life. In another study involving 14 patients with inoperable colorectal cancers, an increase in eosinophils after intralesional mistletoe therapy correlated with improved survival. 58 Together, these studies suggest that robust immune responses are required for beneficial therapeutic response to occur, making it possible that mild to moderate ADRs might actually be desired events. This observation has also been made for other anticancer treatments, such as the recently approved immunotherapy ipilimumab. 59 Immune-related adverse events were observed in 62% of patients, and elevated lymphocyte and eosinophil counts following ipilimumab infusions are reported to be early markers associated with better overall survival. 59 Similarly, the presence of a skin rash following treatment with erlotinib in pancreatic cancer patients was associated with a higher likelihood of achieving disease control, and in colorectal cancer patients treated with cetuximab, a rash of grade 2 or higher was strongly associated with improved survival.60-62 Clearly, the relationship between mistletoe therapy, immune response, and therapeutic outcome requires further investigation.
Limitations of this retrospective study include the possibility of missing or erroneous data, a heterogeneous demographic, and highly varying treatment regimes. Additionally, there was no control group for this study, meaning that ADRs may have been overreported because of our inability to calculate the frequency of disease-related or spontaneous adverse events. Strengths of our study are the provision of a detailed summary of the variation that exists in the delivery of IT mistletoe therapy and an accurate assessment of the safety of IT mistletoe therapy under clinical use within an integrative oncological framework.
Conclusions
IT injection of mistletoe preparations appears to be associated with a significantly higher rate of ADRs, compared with SC and IV applications of mistletoe. This seems to be related to the high doses of mistletoe preparations used in IT therapy and to the pharmacokinetics involved with different forms of administration. All patients recovered fully, however, and there were no serious or life-threatening ADRs. Furthermore, it is possible that immune-related ADRs, such as pyrexia and local inflammatory reactions, might actually be critical for tumor response. The key implication of this study is that future prospective studies assessing the efficacy and effectiveness of IT or multimodal mistletoe therapy can be carried out with increased confidence regarding the safety of IT mistletoe injections.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: H. Matthes has been a member of Weleda AG directory board since March 2012. The other authors declare that they have no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Network Oncology was funded by the Software AG Stiftung Darmstadt, Germany; Weleda AG Arlesheim, Switzerland; Abnoba GmbH Pforzheim, Germany; and Helixor GmbH Rosenfeld, Germany. By contract, researchers were independent from the funder.