
Abstract
Acupuncture is being adopted by cancer patients for a wide range of cancer-related symptoms including highly prevalent psychological symptoms like depression, anxiety, insomnia, and impairment in quality of life. Pharmacological treatment of prevalent symptoms like anxiety, depression, and sleep disturbance can contribute to the high chemical burden already carried by cancer patients, creating additional side effects. As a result, patients and providers alike are interested in evidence-based nonpharmacologic alternatives like acupuncture for these symptoms. This article reviews the current literature (January 2000 through April 2013) for acupuncture in cancer-related psychological symptoms with attention to both efficacy and acupuncture-specific methodology. All published studies that met our review criteria demonstrate a positive signal for acupuncture for the treatment of depression, anxiety, sleep disturbance, and for improving quality of life with most results showing statistical significance. However, there are only a handful of acupuncture studies that were specifically designed to evaluate depression, sleep disturbance, and quality of life as primary outcomes, and no studies were found that looked at anxiety as a primary outcome in this population. Published studies in cancer patients and survivors show that acupuncture treatment is not only safe but also more acceptable with fewer side effects than standard of care pharmacological treatments like antidepressants. Finally, there is wide variability in both the implementation and reporting of acupuncture methods in the literature, with only 2 of 12 studies reporting full details of acupuncture methods as outlined in the revised Standards for Reporting Interventions in Clinical Trials of Acupuncture guidelines, published in 2010 and providing an essential framework for the reporting of acupuncture methodology. This lack of methodological detail affects outcomes, generalizability, and validity of research involving acupuncture. Reasons for ongoing challenges in the development of high-quality acupuncture trials are discussed. In conclusion, results are encouraging for the development of randomized trials to directly evaluate the therapeutic impact of acupuncture in cancer-related psychological symptoms, including depression, anxiety, sleep disturbance, and quality of life, but attention to acupuncture methodological specific challenges in the development of high-quality research is necessary.
Keywords
Introduction
Acupuncture is a therapeutic intervention originating in China thousands of years ago involving the insertion of thin, solid metallic needles into specific anatomic locations on the skin. Although acupuncture is well known for the treatment of pain, it was designed to treat the full range of physical and emotional disorders as an extension of an independent, complex medical system known as Chinese medicine. 1 The general public has increasingly adopted the use of acupuncture for a wide range of ailments, but its use has been particularly prevalent among cancer patients and survivors.2-4 As a result, there has been increasing attention to the study of acupuncture for various cancer-associated symptoms in the oncology patient. 5 Currently, evidence supports the use of acupuncture in cancer therapy-related nausea and vomiting, and is promising for treatment of hot flashes, chemotherapy-induced leukopenia, postchemotherapy fatigue, and radiation-induced xerostomia in both cancer patients and survivors.5,6 In addition, emerging research5,7-10 suggests that acupuncture might also be useful for treatment of commonly occurring cancer-related psychological symptoms. Pharmacological treatment of prevalent symptoms like anxiety, depression, and sleep disturbance can contribute to the high chemical burden already carried by cancer patients, creating additional side effects. As a result, patients and providers alike are interested in evidence-based nonpharmacologic alternatives like acupuncture for these symptoms.
Although acupuncture use is prevalent among cancer patients and survivors,2-4 evaluation of the efficacy of acupuncture is hindered by methodological issues in acupuncture research. For example, it is difficult to develop an effective control condition (sham acupuncture) because of the invasive nature of inserting a needle into the skin. Sham acupuncture is a control condition used by some studies, generally involving placing needles that do not puncture the skin, or needling at locations not considered true acupuncture points. However, given its invasive nature, acupuncture is difficult to blind and thus, it is challenging to conduct randomized clinical trials with an adequate placebo arm. Likewise, compromises to the applicability and reproducibility of the data are often required to maintain fidelity to the Chinese medicine framework in which acupuncture is commonly practiced. Finally, the frequent incomplete reporting of acupuncture methods makes the interpretation of the research more problematic.
The purpose of this review is to summarize existing research for acupuncture in cancer patients and survivors in the treatment of psychological symptoms such as anxiety, depression, sleep disturbance, and quality of life. In addition, this review will provide interpretation of acupuncture findings and further elucidate the challenges of acupuncture research in order to make recommendations for future studies.
Methods
A Pubmed search was conducted by the authors with the aid of a medical librarian using the terms “acupuncture” and either “cancer” or “neoplasm,” combined with “depression” or “anxiety” or “sleep” or “insomnia” or “quality of life.” Criteria for selected articles were use of acupuncture as treatment modality and (1) English language, (2) adults, and (3) at least one measure of anxiety, depression, quality of life, or sleep disruption as primary or secondary outcome. We included only primary studies (not reviews) in which full articles were available. The titles and abstracts of all articles that met review criteria were reviewed by both researchers to determine whether the articles met selection criteria. If relevant, full text article was systematically reviewed, and data was extracted on study design, number and characteristics of participants, outcome measures used, and data specific to the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) guidelines as outlined below. We excluded studies that focused exclusively on pediatric populations, were available only in non-English language, or were otherwise not relevant.
Given the wide variability in the administration of acupuncture, we used the recently published revised STRICTA guidelines in describing existing research. The STRICTA guidelines, originally published in 2001 11 and revised in 2010, 12 identify a 6-item checklist for the reporting of methodology in acupuncture trials to improve interpretation and replication. These 6 areas include (1) specifics of acupuncture rationale (including style of acupuncture and reasoning for treatment), (2) details of needling, (3) treatment regimen, (4) other components of treatment (ie, additional modalities such as moxabustion that involves burning a prepared herb over skin), (5) practitioner background, and (6) specifics of control or comparator interventions. 12 An analysis of STRICTA guideline “other components of treatment” was excluded in order to focus more exclusively on the reporting of acupuncture. All studies dealing with acupuncture and psychological symptoms in cancer are listed in Table 1.
All Studies in Psychological Symptoms in Cancer.

Abbreviations: ∅, not described; √, present; 5E, Five Element style; Acu, acupuncture; BDI-PC, Beck Depression Inventory–Primary Care; Ca, cancer; CCM, Cancer Coping Methods; CES-D, Center for Epidemiological Studies–Depression score; CMD, Chinese medicine differential; CRFDS, Cancer-Related Fatigue Distress Scale; EA, electro-acupuncture; f/u Q, follow-up questionnaire; FACT-QOL, Functional Assessment of Cancer Therapy–Quality of Life scale; flex, flexible protocol; HADS, Hospital Anxiety and Depression Scale; HAMD, Hamilton Anxiety and Depression questionnaire; HDRS, Hamilton Depression Rating Scale; HRQOL, health-related quality of life; HT, hormone therapy; LAc, licensed acupuncturist (master’s level training); Med, medical acupuncture; MenQOL, Menopause-Specific Quality of Life Questionnaire; No dx, no differential diagnosis described despite stating style; N/A, not applicable; PGWB, Psychological and General Well-Being Index; POMS, Profile of Mood States; POMS-SF, Profile of Mood States–Short Form; PSQI, Pittsburgh Sleep Quality Index; Pt, patients; RCT, randomized controlled trial; RSCL, Rotterdam Symptom Checklist (QOL); SCL, Symptom Check List; SDS, Self-Rating Depression Scale; SF-12 mental, Short Form 12, mental subscale; SF-36 = Short Form–36 (HRQOL); SLDS-c, Satisfaction With Life Domains Scale–Cancer; STRICTA, Standards for Reporting Interventions in Clinical Trials of Acupuncture; sx, symptoms; TCM, Traditional Chinese medicine style; tx, treatment; WHQ, Women’s Health Questionnaire (QOL measure, subscale measures sleep).
Overview of Acupuncture for Psychiatric Side Effects of Cancer
Sleep Disturbance
Sleep disturbance is prevalent in cancer patients and survivors, as nearly 80% of cancer patients experience sleep disturbance, and about 60% of survivors complain of poor sleep.25-27 In a recent review of cancer-related symptoms, sleep disturbance was the second most prevalent symptom reported by cancer patients after fatigue. 28 Four clinical trials14,16,17,23 met criteria for this review and were conducted using acupuncture for sleep disturbance in cancer. Only 1 of them chose sleep as a primary outcome, 23 while others focused on sleep disturbance secondary to either hot flashes14,17 or depression. 16
Otte et al 23 conducted a study that focused on sleep disturbance as the primary symptom in cancer patients. In this study, 10 women with breast cancer who were experiencing sleep disturbance and hot flashes received 3 acupuncture sessions in a single arm design. Otte et al 23 reported significant improvements in sleep parameters, specifically in percentage of time awake after sleep onset and decreased sleep latency as measured by actigraphy. Of note, the study by Otte et al 23 was the only one to use objective sleep measurement. Two randomized clinical trials evaluated acupuncture for sleep disturbance associated with other symptoms in cancer patients. Feng et al 16 evaluated sleep comorbid to depression. A second study by Frisk et al 17 evaluated sleep as secondary to hot flashes.
Feng et al 16 studied 80 cancer patients randomized to either acupuncture or antidepressant (fluoxetine) using the Pittsburgh Sleep Quality Index. Frisk et al 17 evaluated 45 breast cancer patients treated with electro-acupuncture or hormone therapy using a sleep log. It should be noted that Frisk et al 17 conducted this study when hormone therapy was still an acceptable treatment for this population, which it is no longer. 6 Sleep parameters improved significantly in both studies, with acupuncture superior to fluoxetine and equivalent to hormone therapy.16,17 Although both were positive trials for sleep improvements, neither was designed to treat sleep disturbance. In the study by Frisk et al, 17 sleep improvements appeared largely related to reduction in hot flash symptoms. As a result, it is unclear from the study by Frisk et al 17 whether acupuncture had a direct impact on sleep disturbance. Of note, Feng et al 16 was the only study evaluating sleep to use a Chinese medicine differential diagnosis (phlegm stasis binding) as diagnostic criteria.
de Valois et al 14 designed an open arm trial with once weekly acupuncture treating 50 breast cancer survivors who suffered from tamoxifen-induced hot flashes that secondarily dysregulated sleep. The study by de Valois et al 14 also reported significant improvements in sleep parameters.
These 4 studies demonstrate a positive signal for the impact of acupuncture on sleep disturbance. However, 2 of the 4 studies were designed to treat hot flashes, and the only one (Otte et al 23 ) designed to treat sleep had 10 participants. Additionally, half used a nonrandomized design and half (Feng et al 16 and de Valois et al 14 ) lacked explanation of essential details of the acupuncture protocol, as outlined in Table 2. Given positive findings for the impact of acupuncture on sleep problems in the general population,29,30 there is a need for well-designed, adequately powered randomized clinical trials that focus on the impact of acupuncture on sleep in cancer patients using standardized sleep assessments and appropriate control groups.
Sleep and Acupuncture in Cancer. a
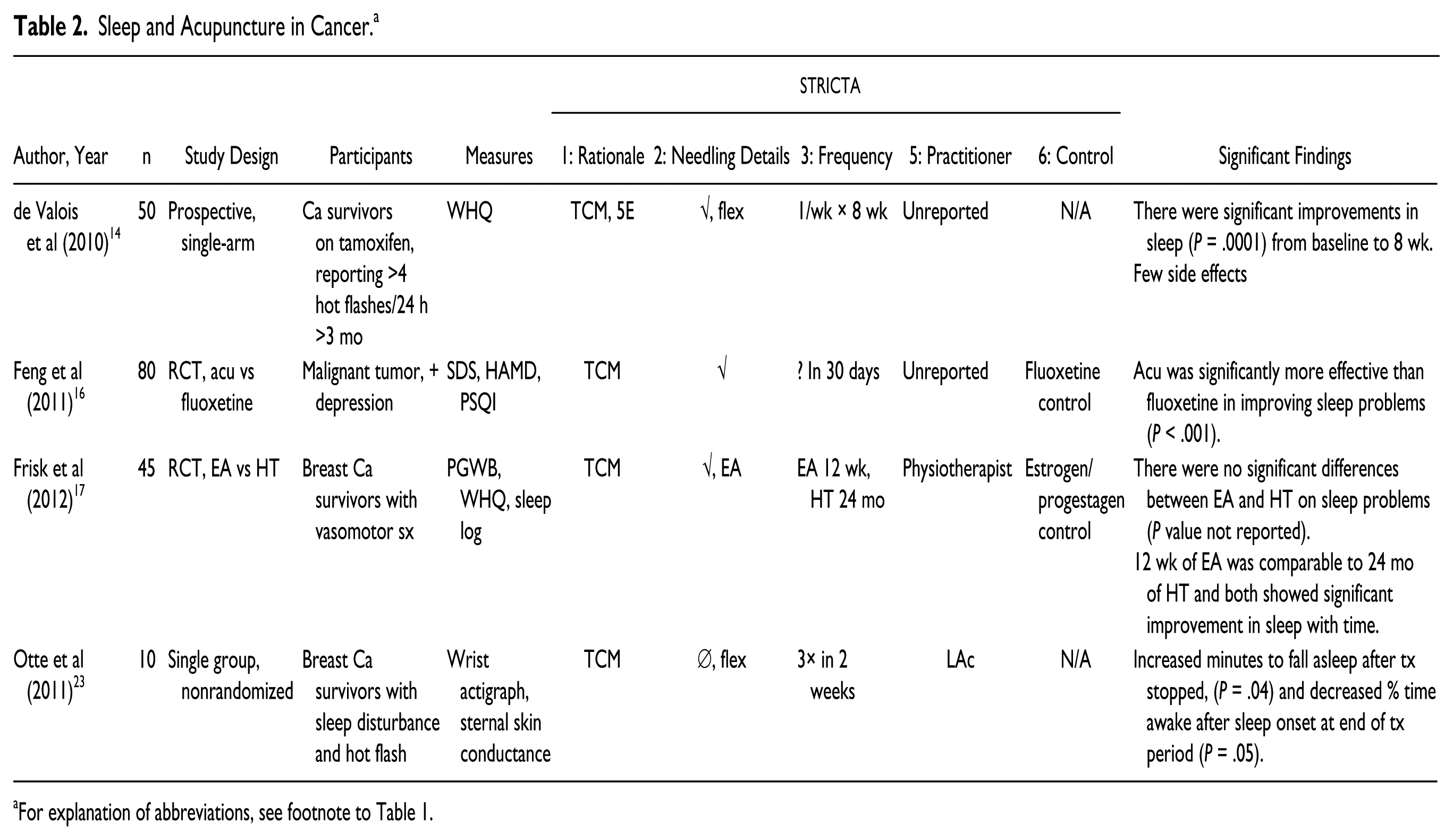
For explanation of abbreviations, see footnote to Table 1.
Depression
While studies vary on the exact prevalence of depression in cancer, a recent review suggests that up to 15% of cancer patients and survivors and 50% of those in palliative care suffer from depression. 31 We found 6 trials that met review criteria for the evaluation of acupuncture and depression in cancer patients. Five of these studies were randomized clinical trials, but only one used depression as a primary outcome measure, 16 and one, 20 which will be discussed last, used acupuncture in addition to massage as the intervention.
Feng et al 16 conducted the only randomized clinical trial designed to evaluate acupuncture for depression in cancer patients. Treatment was acupuncture versus antidepressant (fluoxetine) in 80 patients diagnosed with malignant tumor who met criteria for depression and a Chinese Medicine differential diagnosis called phlegm stasis binding, which is one Chinese diagnosis consistent with cancer. Results showed that both acupuncture and fluoxetine were effective in relieving depression based on Hamilton Anxiety and Depression questionnaire score, but that acupuncture was significantly more effective than fluoxetine.
Three randomized clinical trials13,21,24 evaluated depression as a secondary outcome, with primary outcome measures of fatigue in 2 studies13,21 and vasomotor symptoms in 1 study. 24 Molassiotis et al 21 randomized 302 breast cancer patients with fatigue to acupuncture versus usual care, a fatigue information booklet. In a different design, Balk et al 13 treated 27 cancer patients with fatigue via real versus sham acupuncture. Here, sham acupuncture consisted of telescoping blunt-edged needles that did not puncture the skin placed at the same locations as the real acupuncture. Both studies13,21 had positive findings, with Molassiotis et al 21 reporting significant improvement in depression as compared with fatigue information booklet (usual care) using the Hospital Anxiety and Depression Scale. Although Balk et al 13 report improvement in depression in their abstract, depression outcome is listed as a “confounder measurement,” and so does not appear to be evaluated as primary or secondary outcome in this statistically underpowered study with failed blinding. Walker et al 24 performed a randomized trial to compare acupuncture and standard of care, venlafaxine treatment, in 50 breast cancer patients on anti-estrogen hormone treatment who had vasomotor symptoms. Beck Depression Inventory scores improved significantly in both groups, concluding that acupuncture was at least as effective as venlafaxine in decreasing depressive symptoms. In addition, Walker et al 24 reported that acupuncture was significantly better tolerated and accepted than venlafaxine, with 18 reports of adverse events in the venlafaxine group and a third of eligible patients declining to participate because they were unwilling to take venlafaxine as compared with none in the acupuncture group.
Dean-Clower et al 15 performed a pilot single-armed prospective trial designed to evaluate quality of life in 40 advanced ovarian and breast cancer patients, using the Profile of Mood States–Short Form as secondary outcome measure. Results demonstrated a significant decrease in severity score for anxiety and depression, and these were sustained at 12 weeks. No significant adverse events attributable to acupuncture were observed.
Finally, Mehling et al 20 (n = 138) performed a randomized controlled trial of acupuncture and massage or usual care alone on postoperative days 1 and 2 for cancer patients receiving surgery. Given the combination of acupuncture plus massage, it is not possible to draw conclusions about the effectiveness of acupuncture; however, improvement in depression was significant for the treatment group.
In summary, treatment of depression in cancer patients with acupuncture is promising, however these findings need to be interpreted cautiously given the limitations in study design and the limited details on acupuncture study protocol, as noted in Table 3. Nonetheless, acupuncture does appear to be a well-tolerated and acceptable intervention, as in 2 trials above (Walker et al 24 and Feng et al 16 ), acupuncture was compared with standard of care, antidepressant medication, and in both cases performed as well or better than medication with fewer side effects.
Depression and Acupuncture in Cancer. a

For explanation of abbreviations, see footnote to Table 1.
Anxiety
A recent review found that the prevalence of clinical anxiety in cancer patients was 19%, with women almost twice as likely to report anxiety (24% vs 12.9%). 32 There were no studies that met review criteria that had anxiety as a primary outcome measure. Of the following 4 studies,14,15,19,21 one was a randomized clinical trial designed to treat fatigue, 21 two were single-arm studies, evaluating quality of life 15 or hot flashes, 14 and the final study 19 was a retrospective chart review of acupuncture in a hospice program.
The largest (n = 302) study of acupuncture in cancer patients measuring anxiety was the 2012 study by Molassiotis et al. 21 In a trial of acupuncture for fatigue in breast cancer patients utilizing a randomized controlled design, the study found significant improvement in anxiety as measured by the Hospital Anxiety and Depression scale compared with usual care.
The subsequent 3 studies14,15,19 were either prospective single arm or retrospective chart review studies. In the 2010 single-arm study by Dean-Clower et al, 15 12 acupuncture treatments were given to 40 advanced ovarian and breast cancer patients with results demonstrating significant decrease in anxiety scores. This improvement continued at 1 month after acupuncture was completed. de Valois et al 14 enrolled 50 patients with early breast cancer to a single-arm trial of 8 acupuncture treatments for hot flashes. Anxiety was measured through Women’s Health Questionnaire anxiety subscale, and improvement reached significance. Finally, Kaufman and Salkeld, 19 through retrospective chart review and acupuncturist interview of Kaiser Northwest Hospice acupuncture program, determined that 63% of patients treated with acupuncture had a cancer diagnosis and 45% had an anxiety diagnosis. It is unclear, however, in what proportion these 2 groups overlapped. Results indicated that 31% of patients who were treated for anxiety had “excellent” or “good” results as noted in the charts.
In summary, currently no definitive conclusions can be drawn regarding the efficacy of acupuncture for anxiety in cancer patients given limited data, and also because no trials evaluated anxiety as a primary outcome measure as outlined in Table 4. Studies that did use anxiety as secondary outcome measure were generally positive with significant results, paving the way for the pursuit of higher quality studies with anxiety as primary outcome measure.
Anxiety and Acupuncture in Cancer. a

For explanation of abbreviations, see footnote to Table 1.
Quality of Life
Quality-of-life measures attempt to evaluate the impact of cancer on a person’s activities of daily living. The measures used in the acupuncture literature are varied, but generally include a combination of psychological, psychosocial, and symptom-specific questions. 33 Several studies looked at the impact of acupuncture on quality of life; however, similar to research for other cancer-related psychiatric symptoms (as described above), only one was specifically designed to evaluate quality of life, 15 and this trial was a single-arm pilot study. An additional 5 randomized clinical trials met criteria in the evaluation of acupuncture for quality of life, 3 for hot flashes17,22,24 and 2 for fatigue.13,21
Dean-Clower et al 15 performed the only study to primarily evaluate quality of life, in an 8-week single-arm trial of acupuncture for 40 advanced ovarian and breast cancer patients. In addition to showing significant improvement in quality of life (P = .0004), 97% of participants reported that acupuncture “helped their overall sense of well-being.” Quality-of-life measures continued to show improvement one month after acupuncture was completed (at week 12). No significant side effects or adverse events attributable to acupuncture were observed.
There are 3 randomized controlled trials that evaluated quality of life as secondary to hot flashes in breast cancer patients via 12-week acupuncture versus control. Control condition differed among the 3 studies, and was hormone therapy in Frisk et al, 17 venlafaxine in Walker et al, 24 and applied relaxation in Nedstrand et al. 22 All 3 demonstrated significant improvement for acupuncture in quality-of-life measures, with Frisk et al 17 (n = 45) demonstrating significant improvement in quality of life in both electro-acupuncture and hormone therapy group using the Psychological and General Well-Being Index and Women’s Health Questionnaire, but no significant difference between the groups. Nedstrand et al 22 (n = 38) also used electro-acupuncture and found significant improvement in “psychological well-being” in both electro-acupuncture and applied relaxation groups using Symptom Checklist and Mood Scale. Walker et al 24 evaluated 50 breast cancer patients receiving anti-estrogen hormone treatment and found significant improvement in quality of life for both acupuncture and venlafaxine groups using the Menopause-Specific Quality of Life Questionnaire and concluded that acupuncture was at least as effective as venlafaxine in improving quality of life associated with hot flashes. As previously noted, Walker et al 24 reported that acupuncture was significantly better tolerated than venlafaxine, as there were zero adverse events in acupuncture group compared with 18 in venlafaxine. Out of 94 eligible patients who declined to participate, one third did so because they were unwilling to take venlafaxine, but none declined because of acupuncture, an indication of acceptability and tolerability.
The following 2 randomized controlled trials were designed to evaluate fatigue in cancer patients, with Molassiotis et al 21 randomizing 302 breast cancer patients to acupuncture or fatigue pamphlet. They found a significant improvement in quality of life in the acupuncture-treated patients as compared with control using the Functional Assessment of Cancer Therapy scale. In a different design, Balk et al 13 performed a sham-controlled trial of acupuncture in 27 participants using the Short Form 36, with both sham (nonpenetrating, blunt, telescoping needles) and true acupuncture groups showing improvement in quality of life.
Finally, a subjective approach was sought by Hervik and Mjåland 18 in their questionnaire research of 82 women who had previously participated in a randomized controlled trial investigating the effects of acupuncture versus sham acupuncture on hot flashes in breast cancer patients. A nonspecific, broad, and open question was posed and qualitative data were then analyzed. Sham acupuncture participants complained that hot flashes were still problematic, and those treated with true acupuncture found them “less of a problem and generally had a more positive outlook on life.” Although intentionally subjective, a limitation of this study was the open-ended subjective question and associated challenges inherent to analysis and interpretation of qualitative research.
In spite of the limitations described above, acupuncture appears to have positive effects on quality of life in cancer patients. It was well tolerated and better tolerated than medication. 24 In addition, some participants expressed strong preference for acupuncture over medication. 24 When quality of life is examined in association with symptoms such as hot flashes, acupuncture appears to work as well as medication. However, once again, these findings are limited by study design, with only one trial evaluating quality of life as the primary outcome measure, 15 and another trial underpowered to detect a difference between acupuncture and sham. 13 Incomplete reporting of acupuncture practices was common, as outlined in Table 5, and this limits the interpretation of results. Clinical trials with adequate power, objective and validated outcome measures, and adequately described acupuncture protocol are needed to specifically evaluate the role of acupuncture for psychological well-being and quality of life.
Quality of Life and Acupuncture in Cancer. a

For explanation of abbreviations, see footnote to Table 1.
Summary
In reviewing this literature on acupuncture in the treatment of cancer-related psychological symptoms, common themes have emerged. There appears to be a positive effect for acupuncture in all published articles that met review criteria for cancer-related psychological symptoms, including sleep disturbance, depression, anxiety, and quality of life. However, there are only a few studies that directly address the question of whether acupuncture is effective in managing these psychological symptoms, since the majority evaluated these symptoms secondary to other cancer-related symptoms such as fatigue and hot flashes. There is strong evidence for acupuncture safety and tolerability in this population, as well as its higher acceptability and tolerability than standard of care pharmacological treatments like antidepressants. The statistically significant findings for the beneficial effect of acupuncture on cancer-related psychological symptoms in a limited number of studies are encouraging and suggest the need for conducting randomized clinical trials to directly evaluate the therapeutic impact of acupuncture in this setting.
Possible Biologic Mechanisms for Acupuncture Effects
There are diverse theories that attempt to explain the potential effect of acupuncture on psychiatric symptoms. Animal studies have suggested that acupuncture may have many different mechanisms of action that act both locally and systemically. 34 One theory involves acupuncture’s apparent effect on neuropeptide Y, a neuromodulator produced primarily by the sympathetic nervous system. Neuropeptide Y is thought to be pivotal in the stress response, with functions that include increasing food intake and fat storage, reducing anxiety, stress, and the perception of pain, and affecting circadian rhythms. 35 One immunohistochemical study demonstrated an increase in neuropeptide Y immunoreactive cells in the hippocampus, associated with increase in locomotion and weight as compared with control in maternally separated rats treated with a single acupuncture point. 36
Additional potential mechanisms of action stem from evidence that acupuncture can increase adrenocorticotropic hormone, a substance integral to the stress response, β-endorphins—the neurotransmitters associated with pain relief and a sense of well-being—as well as the neurotransmitters serotonin, dopamine and norepinephrine, all important targets in the psychiatric treatment of depression and anxiety.34,37
In addition to neurotransmitters, acupuncture appears to have diverse effects on other signaling molecules, decreasing the expression of 3 cytokines, interleukin-6, β-nerve growth factor, and tissue inhibitors of metalloproteinase-1, 38 potentially reducing the inflammatory response. Emerging research has begun to describe how pro-inflammatory cytokines can influence a vast array of brain function relevant to behavior, including neurocircuits relating to mood, anxiety, and motivation. 39
Evidence also supports the potential role of connective tissue and fibroblasts in the signaling mechanism of acupuncture, in potentially dose-dependent response,40,41 raising the question of whether “De Qi,” or the sensation of heaviness or tingling associated with needle manipulation is an important modulator of acupuncture effect. One theory suggests that acupuncture meridians may actually relate to connective tissue planes, as one study found an 80% correspondence between connective tissue planes and the sites of acupuncture points. 42 The search for potential mechanisms for acupuncture is still in the early stages.
Overview of Challenges
Chinese Medicine and Modern Allopathic Medicine
As a result of the different theoretical frameworks governing Chinese medicine and modern medicine, there are many hidden challenges in conducting acupuncture research. One of the most fundamental and often overlooked challenges is the lack of one-to-one correlation between modern allopathic and Chinese medicine diagnoses. In Chinese medicine, no individual symptom equals a diagnosis, and no symptom or sign can be considered in isolation from all others.43(pp143-144) As an example, a symptom like “anxiety,” has no fewer than 5 possible diagnoses in Chinese medicine, and therefore theoretically requires a different point prescription44(p93) making it difficult to standardize the acupuncture treatment protocol.
Acupuncture is an extension of Chinese medicine, a system that developed thousands of years ago, before the advent of modern science and modern scientific instruments. As such, Chinese medicine uses a functional paradigm to explain and treat human disease that is based on patterns of illness and clusters of symptoms. Practitioners of Chinese medicine are taught to identify patterns based on physical examination and symptom clusters, and then develop an acupuncture point prescription to address this pattern, which generally describes the entirety of a person’s symptoms (symptom cluster), and not solely one symptom. 43 Additionally, acupuncture points often have multiple functions. For instance, a commonly used point for cancer-related nausea is PC 6 (Pericardium 6), which is also an important and widely used point for the management of insomnia and anxiety. Because of this holistic approach, generally only a small percentage of points are symptom-driven points.
Chinese medicine uses a poetic, nonrepresentational language that has roots in Taoism to describe patterns of symptoms and their progression, with disease conceptualized as imbalances in two opposing fundamental forces, Yin and Yang. Yin and Yang are not easily defined, but can be understood by the following “everything in the phenomenal universe has yin and yang aspect . . . (which are) mutually opposed but also mutually united.” Additionally, “yang represents activity, function, warmth and movement, while yin represents matter, form, cold and stillness.”45(p5)
This is a fundamentally different approach than that of modern allopathic medicine, which is based on biological and molecular science, and utilizes a reductionist scientific model. Chinese medicine is an emergent system requiring attention to the totality of symptoms and is different from modern allopathic medicine, which uses a reductionist approach designed to analyze each part of the whole. Thus, designing a trial that adequately addresses these translational issues can be an exercise in compromises. However, because cancer patients share common risk factors, exposures, and thus symptom clusters, they may be a patient population uniquely suited for studying acupuncture, allowing closer fidelity to the Chinese medicine framework while preserving a more rigorous scientific model of inquiry.
Acupuncture Modalities
An additional reality is the variability in the practice of acupuncture. The selection of acupuncture points, as classically practiced, is governed by many factors. Acupuncture point selection includes consideration of the presenting symptoms, but also a determination of the current constitution of a patient, described by the Chinese medicine pattern of imbalance in Yin and Yang called the “differential diagnosis.” However, theoretical differences exist in the modern practice of acupuncture, exemplified by the practices of Traditional Chinese medicine (TCM), taught by many master’s degree programs in the United States, versus Five Element style, another popular branch of Chinese medicine. Although these styles share a fundamental theoretical framework, point selection and diagnosis vary between these 2 schools.
A more recent addition to the practice of acupuncture is auricular acupuncture, developed in France during the 1950s. 46 Auricular acupuncture is a method that forgoes Chinese medicine’s theoretical framework and diagnosis, and chooses points on the ear that correspond to a theoretical homunculus. Perhaps the most widely recognized use of auricular acupuncture in the United States is the National Acupuncture Detoxification Association protocol, a fixed set of points used in the treatment of substance abuse. Additionally, certain adjuncts and variants to acupuncture make a notable appearance in the literature, particularly electro-acupuncture, a method of acupuncture in which electrodes are attached to select acupuncture needles and current is applied for the duration of the session, and acupressure, a heterogeneous group of methods meant to stimulate acupuncture points without the use of a needle puncturing the skin.
Training of Acupuncture Practitioners
There is significant variability in the training of the practitioners performing acupuncture. In the United States, practitioners can range from state licensed individuals with 3 or more years of master’s level training in the theory and practice of Chinese medicine at a nationally accredited institution, to those trained in other health care fields who practice acupuncture with variable levels of training and no standard accreditation. Although state laws vary, most states require licensed acupuncture providers to be trained at schools accredited by the Accreditation Commission for Acupuncture and Oriental Medicine and to seek certification from the national acupuncture board, the National Certification Commission for Acupuncture and Oriental Medicine, which involves successfully passing a comprehensive examination.47,48 Physicians, chiropractors, and physical therapists are among those eligible in some states to take abbreviated courses, often 100 to 300 hours of training, and practice acupuncture without standardized licensure or accreditation.49,50
STRICTA Guidelines
Although the revised STRICTA guidelines 12 provide an essential framework for reporting acupuncture trial methodology, it is not clear if the addition of this information alone allows the average reader to better interpret this varied and complex data. Many readers do not have the basic knowledge in the practice of acupuncture necessary to evaluate the acupuncture-specific methodological strengths and weaknesses of a study. In addition, STRICTA guidelines are still not widely used even in trials published since STRICTA guidelines inception in 2001.
Limitations
Throughout this review, we noted the presence of significant limitations because of an overall small number of trials designed to look at the impact of acupuncture on psychological symptoms in cancer, nonrandomized designs, small sample sizes, and lack of objective outcome measures. Most studies did not evaluate psychological symptoms as primary outcomes. It should be noted that although most articles that met our review criteria had a positive signal for acupuncture, it is possible that there may be a publication bias, since negative trials are less likely to be published particularly in debatable areas of medicine where strong evidence is limited.51-54 Finally, as described above, blinding in acupuncture studies is difficult, and thus studies without control or with failed blinding are common.
One theme that emerged is the inconsistent reporting of acupuncture methodology, as outlined in Table 1. Only 2 (Frisk et al 17 and Mehling et al 20 ) of the 12 trials reported all essential details of acupuncture administration as outlined in the STRICTA guidelines. The most commonly omitted information was lack of details of acupuncture needling (such as the number of needles inserted, location of needling, depth of insertion, and response sought) and the training of the practitioner providing the acupuncture. These omissions have a significant impact on interpretation of acupuncture clinical trial for the following reasons. First, administration of acupuncture has significant variability. Acupuncture needling details are necessary for evaluating an acupuncture trial, similar to providing the name, dosage, and administration form in a medication trial. Leaving out this essential information would render an allopathic medicine trial nearly uninterpretable. Second, the skill level of a practitioner providing an intervention is likely to affect the consistency and efficacy of an intervention. The fact that the vast majority of trials did not describe certain aspects of the acupuncture specific methodological details is a cause of concern.
It should also be noted when reviewing Table 1 that there is wide variability between trials, both in the level of detail with which acupuncture is reported, and in the actual administration of acupuncture. There is little consistency between trials on how the acupuncture points are chosen, whether there is a flexible or fixed protocol, how many sessions are given and how often, or the training of the provider (when these details are reported). These aspects could potentially have significant effects on the outcome of a trial, so greater attention to the reporting of these details could improve reproducibility, aid interpretation, and facilitate the translation of this body of work into clinical practice.
The STRICTA guidelines have been designed to help researchers in reporting of crucial acupuncture methodological details including the specifics of acupuncture methods, rationale (including style of acupuncture and reasoning for treatment), details of needling, treatment regimen, practitioner background, and specifics of control or comparator interventions. However, it is apparent that these guidelines are not yet in widespread use. Furthermore, the question remains whether the inclusion of this information alone is enough to address the interpretive challenges of acupuncture research. Many who consult the literature may not have sufficient knowledge about acupuncture to make sense of this complex data.
In addition to the incomplete reporting of methodologies, there is also a pattern of incomplete reporting of important statistical details such as standard deviations and mean change scores. These were reported in our tables when reported by study authors.
This review has several limitations. First, although this review is novel in analyzing included studies according to the STRICTA guidelines, 12 we did not use a method for ranking the quality of the acupuncture studies and the data that they produce. Thus, it was not in the scope of this review to provide detailed commentary on issues related to choice of outcome measure, duration of treatment, use of appropriate statistical analysis or adherence to Chinese medicine best practices. Instead, the focus of this review was on summarizing the current state of the literature and highlighting the heterogeneity in current acupuncture research methodology and reporting. Second, our conclusions for this review are based on a small number of available published studies on acupuncture in psychological outcomes, few of which examined psychological symptoms as primary outcome. As such, conclusions drawn from this review are useful in suggesting future directions for research, since interpretability of the findings is limited.
Future Directions
In addition to the need for higher quality studies with more rigorous methodology and methodological reporting, further evaluation of each aspect of the variable practice of acupuncture is needed to clarify acupuncture efficacy and best practices. For example, future studies should determine whether Chinese medical differential diagnosis is essential for using acupuncture in treatment of psychological disorders, as is suggested in Liu et al 55 since many current studies appear to forgo this traditionally integral aspect of acupuncture point selection. More research is needed to determine whether substantial training in the theory and practice of Chinese medicine (master’s level state licensed providers) leads to better outcomes. Another unanswered question is whether there are moderators of acupuncture treatment responsiveness such as obtaining De Qi (a specific sensation of heaviness or tingling), as needling technique is taught as an essential component of achieving treatment response in some schools of acupuncture training. Many of the studies evaluated in this review had no discussion of needle manipulation, and the study by Molassiotis et al 21 specifically avoided manipulation of needles. Preliminary evidence for the importance of needling technique is supported by Xiong et al 56 as well as basic science research as outlined in the mechanism of action section.41,57 Furthermore, an issue that appears absent from the current acupuncture literature is the question of whether there are acupuncture responders and nonresponders and their characteristics to guide potential referrals for acupuncture. These issues will help clarify how and whom acupuncture can effectively treat. As higher quality studies emerge, acupuncture has the potential to improve psychological outcomes of cancer patients in clinical practice.
Footnotes
Acknowledgements
We are grateful to the anonymous reviewers for their thoughtful comments and suggestions and to Dr. Smita Das, MD, PhD, MPH who graciously gave of her time proofreading and reviewing statistics.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Nadia Haddad, MD, MS, L.Ac received no financial support for the research, authorship, and/or publication of this article. For Dr. Oxana Palesh, PhD, MPH, the work was supported in part by NCI K07CA132916 and NCCAM 5P30AT005886 grants.