
Abstract
Purpose. This is a pilot study investigating the effect of healing touch (HT) on fatigue in breast cancer patients undergoing radiation therapy (RT). Methods/Design. This study presents the results of a within-subjects design randomized clinical trial where the treatment group was treated with HT, whereas the control group experienced sham therapy. The setting was a university RT clinic. The participants were breast cancer patients treated with lumpectomy or mastectomy, 21 to 75 years old with an Eastern Cooperative Oncology Group (ECOG) score of 0 to 2. The intervention was a 45-minute session of HT or sham therapy once a week during RT. Outcome measures included fatigue, quality of life (QOL), and anxiety/depression. Results. A total of 70 patients were approached, with 41 completing the study. At completion, the HT participants tended to report higher levels of fatigue, statistically significant for interference (P = .010) and usual fatigue (P = .024). The control group tended to report greater reductions in fatigue relative to their own means than the HT group (Cohen’s d = 0.30 to 0.49 vs 0.06 to 0.18, respectively). There were no statistically significant differences between the groups for QOL. Conclusions. Our enrollment and retention indicate that HT is feasible for women during RT. Our pilot findings do not support a beneficial effect of HT on fatigue or QOL. Future research may explore increasing dose and teasing out therapist effect.
Introduction
Fatigue is a pervasive symptom of cancer therapy affecting the patient’s quality of life (QOL). It may be easier to recognize than define, but Hardy and Studenski 1 found that participants equated fatigue with tiredness, sleepiness, and trouble concentrating. At the time of diagnosis, 50% to 75% of cancer patients report fatigue. 2 The number of patients experiencing fatigue rises to 80% to 96% for patients undergoing chemotherapy and 60% to 93% for patients undergoing radiation therapy (RT).2-4 The causal mechanism of cancer treatment–related fatigue is not well understood, but rest and sleep alone do not relieve it.2,5 In addition, cancer-related fatigue is disproportionately negatively related to the level of exertion; that is, the greater the level of activity, the lower the fatigue. 5 Higher levels of fatigue are associated with the presence of multiple chronic conditions and a poorer QOL.1,6 In patients with cancer, a positive relationship also has been reported between fatigue, and anxiety 7 and depression.8-10 Few therapies are available that treat cancer-related fatigue.
Complementary and alternative medicine includes a domain of energy medicine therapies whose use seems promising in reducing fatigue in cancer patients. Healing touch (HT) is one of the energy therapies with a potential to reduce fatigue. However, it is also a putative energy therapy (effects are yet to be measured). In theory, HT may be used to restore and rebalance an energy field disruption, such as those that could be caused by RT. The mechanism of action for energy therapies is unknown at this time. There have been few measurable physiological changes associated with HT therapies. One study found an increase in secretory immunoglobulin A in clients treated by experienced HT practitioners. 11 In another related energy therapy (therapeutic touch), researchers found a significant increase in hemoglobin and hematocrit among anemic female students receiving therapeutic touch. 12 In cervical cancer patients undergoing chemo-RT, HT was found to increase natural killer cell cytotoxicity when compared with control groups. 13 There is some evidence that HT can enhance energy in patients undergoing treatment for cancer.6,14,15
Because prior studies reported positive albeit nonsignificant results, the current study was designed as a randomized clinical trial to provide pilot data on the effectiveness of HT on fatigue experienced by breast cancer patients receiving RT. Fatigue and QOL were the primary indicators of effectiveness in this research. We hypothesized that women receiving HT therapy would report lower levels of fatigue over the course of RT and improved QOL at the end of RT compared with women receiving sham (placebo) therapy.
Methods
This was a randomized clinical trial with 2 factors. The between-subjects factor was group assignment where the intervention group was treated with HT, whereas the control group received sham therapy as a placebo. All patients were blinded to group assignment. The within-group factor was time because fatigue was measured weekly over the course of RT.
Participants
Participants were recruited from a single radiation oncology clinic in an academic medical center. Eligibility criteria for the study included histologically proven breast cancer surgically treated with lumpectomy or mastectomy. Also, patients were limited to English-speaking adults aged 21 to 75 years old, with an Eastern Cooperative Oncology Group (ECOG) performance status of 0, 1, or 2. Patients with stage IV cancer were excluded because of the poorer prognosis with this stage of cancer. In addition, patients with active psychiatric illness were excluded. The study was approved by the institutional review board. Patients provided informed consent, with the understanding that they would receive active or placebo treatment and would be unaware of group assignment. Participants were recruited and enrolled prior to their first radiation treatment.
Randomization and Blinding
Enrolled patients were randomly assigned to control or HT intervention using a block randomization scheme developed by the statistician. Both the patient and researcher administering the surveys were blinded to group assignment. The control and intervention therapists could not be blinded to group assignment.
Intervention
As in the Cook et al 14 study, HT and sham treatments were given once a week during the participants’ RT experience. Although unproven, the theory was that RT created holes in the energy fields, which could result in energy leaks and other distortions in the patient’s energy field. A weekly treatment schedule was chosen because of the belief that harmful effects of a week of RT could be relieved in 1 HT treatment session. In addition, this weekly schedule is consistent with previous trials of HT in patients with cancer. 14
In this study, neither HT nor sham practitioners physically touched or spoke to the participant (other than to request or assist in repositioning). In actual practice, many HT practitioners seldom physically touch the body. The belief is that the work on the energy field does not require physical touch, but the results still affect the recipient’s physical and emotional states. Even with the chakra connection, in which hands are placed on or over adjacent joints, it is believed that it is not necessary to touch the joint to produce the desired effect. During this study, HT providers were instructed to not touch the body but to work no closer than 6 inches above the body; touching would suggest to the participant that she was in the HT group and interfere with the attempt to blind the participant to group assignment.
Each participant had a drape at the neck (ie, an anesthesia-type drape) or was blindfolded to ensure that she could not see how the treatment was being delivered. Each session was 45 minutes long.
Healing Touch Providers
The HT Certificate Program is an education program in energy-based therapy that moves from beginner to advanced practitioner and instructor levels. The program of study incorporates a variety of healing techniques that include both didactic and experiential learning. Level 3 is the last of the 3 technique workshops of the 6 levels of training. Registered nurses who had completed a minimum of level 3 certificate training were recruited to provide the HT treatments. Each practitioner was widely known in the local HT community as an excellent healer. Of the 5 providers for this research, 3 had completed level 3 training, and 2 had completed level 4. Each had a minimum of 1 year of an active HT practice. Two had been in practice for 10 to 15 years. To eliminate the effect of individual practitioner traits, each patient received therapy from at least 3 HT practitioners. None of the authors participated in providing HT therapy.
Healing Touch Intervention
The HT protocol was taken from the study by Cook et al 14 of HT and QOL in RT patients. The HT providers were instructed to begin the session by centering, which is a light meditative state leading to a slowing of respirations and a lowered heart rate. The HT provider remained in this centered state throughout the treatment. The HT provider scanned the participant’s field from neck to below the toes to discover any aberrations in the energy field. Once the practitioner had an impression of the participant’s field, the practitioner would use the standard HT techniques of magnetic passes, chakra connection, and wound sealing to attempt to return the participant’s energy field to a more uniform state.
Magnetic passes are believed to align the energy field, promote relaxation, decrease anxiety, and promote a sense of well-being. Magnetic passes involve the HT provider making gentle sweeping motions from head to foot. The HT providers kept their hands no closer than 6 inches above the body. HT protocol does not describe a minimum or maximum space above the client in which to work 16 ; practitioners use ongoing evaluations of the energy field to determine where to work.
The chakra connection, like magnetic passes, is used to promote relaxation and general well-being, but it is also a specific HT technique for use after chemotherapy and RT. 16 The chakra connection involves the provider holding his/her hands above the sole of the feet, ankles, knees, hips, tail bone, sacral plexus, solar plexus, sternum, throat, brow, and crown in turn until the provider senses that the energy movement beneath each hand is similar. Because some of the participants were draped at the throat area in this study, the connections to the brow and to the crown were modified; the HT providers connected the chakras in order up to the heart/throat connection then with intention connected the throat to the brow and the brow to the crown. If the participant had selected a blindfold (vs draping), the HT provider was able to do the complete chakra connection unmodified.
When the chakra connection was completed, the provider did magnetic passes with the prescribed gentle repetitive sweeping movements from neck to toe. During magnetic passes, a HT provider simultaneously evaluates the field while providing the treatment. Energy leaks may be obvious from the first pass or may be revealed after several passes. When and if the provider identified a leak in the energy field, the practitioner did wound sealing at that area. If there was no sense of an energy leak, wound sealing was not necessary. Wound sealing is a folding of the energy field into itself, as if closing a wound. It is not uncommon for a series of magnetic passes/wound sealing sequences to occur in a single treatment session. The treatment closed with as many magnetic passes as time permitted.
Sham Providers
The practitioners for sham interventions had no training in HT therapy or any other energy modality; each had an active nursing license. Each patient assigned to the control group received a session from at least 2 sham providers over the course of RT.
Sham Intervention
The sham practitioners walked around the participant but did not place their hands or arms over the participant’s body. They were instructed not to allow their hands or arms to come within 12 inches of the sides of the participant but to hold their arms still or move them randomly. Sham practitioners were given no directions on what to think or any mental activities—they were merely required to not speak to the participant during the treatment.
Instruments
Participants completed the Hospital Anxiety and Depression Scale (HAD), the Brief Fatigue Inventory (BFI), the Functional Assessment of Cancer Therapy-Breast (FACT-B), and a demographic form at baseline. Measures of anxiety, depression, hemoglobin, and albumin were included because of the potential relationship of these variables with fatigue. Fatigue was measured on a weekly basis throughout RT with the BFI. The HAD and FACT-B were readministered at the end of RT.
Hospital Anxiety and Depression Scale
The HAD 17 is a 14-item self-report instrument that has been used to measure anxiety and depression in patients with physical illness. The anxiety and depression subscales have demonstrated adequate internal consistency 18 and validity.17,19 The depression subscale has been moderately correlated with multiple domains of QOL as well as fatigue (r = 0.29). 20 The Cronbach α values for the observed HAD depression scale scores in this study were .81 and .87 for the first and final assessments, respectively. The α for the observed anxiety scores were .76 and .84 for the first and final assessments.
Brief Fatigue Inventory
The BFI measured 2 aspects of fatigue—its intensity (3 items) and the degree to which fatigue interferes with daily life (6 items). 21 An 11-point numerical rating scale (0-10) is used to rate each item. The BFI has demonstrated validity.21,22 Cronbach’s α for the observed BFI interference scores in this study ranged from .95 to .98 across the weekly surveys.
Functional Assessment of Cancer Therapy–Breast
The FACT-B includes the 27-item FACT-G (FACT–General; version 4) and the 9-item breast-specific subscale.23,24 Higher values reflect better QOL. Psychometric properties of the FACT-G have been examined in a variety of oncology populations with α coefficients ranging from .65 to .89. 25 Sensitivity to change and validity of the breast subscale also have been reported. 24 Cronbach’s α for the observed FACT-G total scores in this study were .77 (first) and .81 (last) and .75 (first) and .70 (last) for the breast module.
Demographic and Clinical Variables
Data were collected on demographic variables (age, race/ethnicity, marital status, and employment) through self-report. Clinical variables (date of cancer diagnosis, treatment received/planned, stage, performance status, hemoglobin, and albumin) were obtained from the participants’ medical records.
Procedure
Women were enrolled in this trial prior to initiating radiation. Baseline data were collected on all study measures and demographic and clinical data at this time. HT or sham therapy was scheduled following RT each Friday for the duration of treatment. Length of RT varied from 5 to 7 weeks; therefore, the number of HT sessions varied proportionally to the length of RT. The BFI was administered each Friday following RT but before HT or sham therapy by a research assistant who was blinded to group assignment. On completion of RT, the research assistant administered the HAD and FACT-B and conducted the end-of-treatment interview.
Statistical Analysis
Frequency distributions were used to summarize the nominal and ordinal demographic and clinical characteristics of the study participants; means and standard deviations (SDs) summarized the continuous demographic and lab values. Likelihood χ2 and independent t tests were used to compare the demographic and clinical characteristics of the study groups. A Mann-Whitney test was used to compare believability of treatment between the 2 groups. Pearson’s correlations measured the strength of the associations of anxiety, depression, hemoglobin, and albumin with the key study outcomes (fatigue and QOL). Subsequently, tests of the hypothesized differences in the changes in outcome variables were conducted using analysis of covariance adjusting for the observed associations of anxiety, depression, hemoglobin, and albumin with the respective outcome variable. Because the meaningful descriptive statistics resulting from such analyses are baseline and end-of-study values were adjusted for covariates (not the observed values), means and standard errors of those estimates are reported rather than observed SD values. Statistical powering indicated that group sizes of 20 would require large differences in the amount of change in a given measure (eg, fatigue) between the groups to be statistically significant (specifically, 0.8 of a SD for 80% power and α = .05). Therefore, additional analyses were done to quantify findings in terms of clinically meaningful changes (not just statistical significance); the amount of change observed within the groups was standardized using their own respective baseline values. These Cohen’s d statistics summaries were calculated for the HT and sham therapy effects on the key outcome variables. A maximum α of .05 (P < .05) was used to determine statistical significance.
Results
From July 2007 to March 2009, 70 patients were approached to participate with 44 enrolling into the study (62.9%). Lack of interest was the most frequent reason given for not participating, but time/schedule issues and travel distance were also mentioned. After enrollment, there was 93% retention. Two intervention and 1 control participants withdrew from the study before completion.
Description of the Sample
A total of 41 women completed the trial; 20 received sham therapy, and 21 received HT therapy, maintaining the original assigned groups to the end of the trial. The demographic and clinical characteristics of the participants in the 2 study groups are summarized in Table 1. The mean age of the sample was 51.5 (SD = 9.2) years. There were no statistically significant differences between the groups for any of the demographic and clinical variables. Although not statistically significant, there was a difference in employment status; 61.9% of women in the HT group were employed full- or part-time, whereas 85% of the sham group members were employed.
Demographic and Clinical Characteristics, by Study Group. a

Abbreviations: HT, healing touch; SD, standard deviation.
Independent t tests compared continuous data; χ2 tests of independence compared nominal data.
The remainder also had received chemotherapy.
Hemoglobin and albumin during the early phase of RT were in the normal range; only 1 participant in the control group was treated with erythropoietin for anemia during the trial (data not shown). A majority of participants were undergoing surgery and RT only. There were no statistically significant differences between the control and HT groups on any of these variables (Table 1). Also, t tests revealed no statistically significant differences at baseline between groups on any of the fatigue, QOL, anxiety, or depression variables (see Table 2).
Outcome Variables, by Study Group at Baseline. a
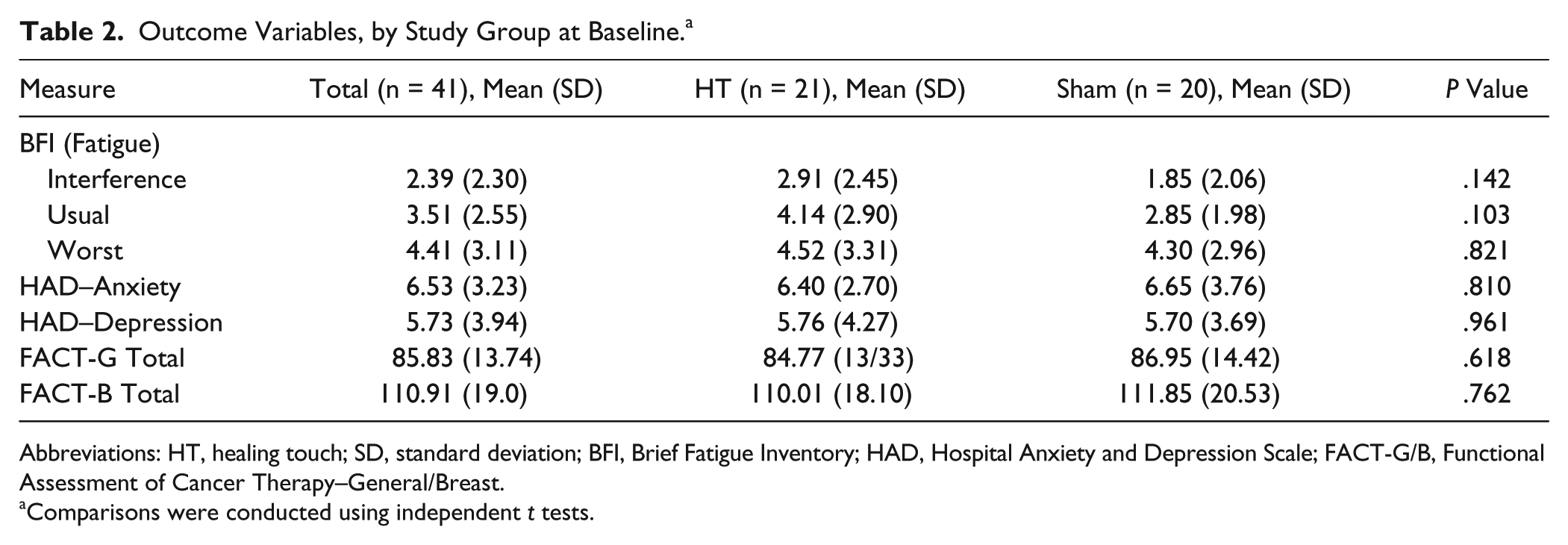
Abbreviations: HT, healing touch; SD, standard deviation; BFI, Brief Fatigue Inventory; HAD, Hospital Anxiety and Depression Scale; FACT-G/B, Functional Assessment of Cancer Therapy–General/Breast.
Comparisons were conducted using independent t tests.
Integrity of Blinding to Group Assignment
Each participant was interviewed at the end of the treatment to determine the integrity of the blinding procedure. The interview took place before the participant was informed of group assignment. Questions on the credibility of treatment included the following: (a) What type of therapy do you think you received and (b) On a scale from 0 (low) to 10 (high), how believable was the therapy you received?
Associations of Depression, Anxiety, and Laboratory Values With Fatigue and QOL
Correlations of depression, anxiety, and laboratory values with fatigue and QOL measures are presented in Table 3. Only usual, worst, and interference fatigue values are reported, but other results from the BFI are available on request. As expected, there were statistically significant positive correlations between depression and each of the fatigue measures, with values ranging from r = 0.36 (usual, P = .020) to r = 0.47 (interference, P = .002). Anxiety also was statistically significantly associated with fatigue interference (r = 0.34; P = .032). Depression and anxiety demonstrated even stronger and inverse associations with the measures of QOL (FACT-G total: r = −0.72 and −0.79, respectively, P < .001). Lower levels of hemoglobin and albumin tended to be associated with more fatigue and lower reported QOL. A statistically significant association of level of hemoglobin with overall QOL (FACT-G total: r = 0.46; P = .005) was observed (see Table 3).
Correlations of Fatigue and QOL with Anxiety, Depression, and Laboratory Values at Baseline. a

Abbreviations: QOL, quality of life; FACT-G/B, Functional Assessment of Cancer Therapy–General/Breast.
Values in cells are r (P value); *P < .05; **P < .01; ***P < .001.
Changes in Fatigue
Baseline and end-of study BFI scores adjusted for associated baseline depression, anxiety, and hemoglobin values are summarized in Table 4. After adjusting for depression and anxiety where necessary, the HT participants tended to report higher levels of fatigue throughout the study than the control participants. Those differences were statistically significant for interference (P = .010) and usual fatigue (P = .024). There were neither statistically significant changes in the adjusted fatigue values over the course of the study nor interaction between group and time for fatigue (P > .05). Thus, the hypothesized effect of HT on fatigue was not supported.
Adjusted Values of Fatigue and QOL at Baseline and at the End of the Study (n = 41).

Abbreviations: QOL, quality of life; HT, healing touch; SE, standard error; FACT-G/B, Functional Assessment of Cancer Therapy–General/Breast.
Adjusted for depression and anxiety.
Adjusted for depression.
Adjusted for depression, anxiety, and hemoglobin values.
Adjusted for anxiety.
Given the generally higher adjusted fatigue values for the HT than for the sham participants, standardized (adjusting for the higher means) changes in the fatigue scores for the 2 groups were generated (also presented in Table 4). As can be seen in Table 4, the control group, who received sham therapy, tended to report greater reductions in fatigue relative to their own means than did the HT group (Cohen’s d = 0.30 to 0.49 vs 0.06 to 0.18, respectively). The control groups’ difference scores for fatigue relative to their own means exceeded a minimally important clinical significance threshold of 1.3. 26
Changes in QOL
After adjusting for anxiety, depression, and hemoglobin values found to be associated with the QOL (FACT) scores, a similar pattern to that found for fatigue was observed in the QOL scores. There were no statistically significant differences between the groups in terms of global QOL or breast cancer–specific QOL, nor were there statistically significant differences in the patterns of change in those measures between the 2 groups over the course of this study (see Table 4). For overall QOL (FACT-G Total), a similar difference to that seen for fatigue between the adjusted effect sizes was observed (Cohen’s d: control = 0.32, HT = 0.11). Effect sizes for changes in the breast-specific QOL measure were minimal and nearly identical.
Integrity of Blinding to Group Assignment
Because participants were blinded to group assignment, credibility of the intervention ensured integrity of the blinding procedure. At the end-of-treatment interview, similar proportions of participants in the HT and sham therapy groups thought they had received the active (HT) treatment. There were no statistically significant differences in the ratings of believability of the therapy between the participants assigned to HT and sham therapy groups. Thus, the blinding procedure was effective.
End-of-Study Interview With HT Providers
Following the close of the study, all 5 HT providers were invited to share their experiences (3/5 participated). All had detected energy leaks in every participant’s energy field and used the wound-sealing technique. The HT therapists who participated reported feeling negative sensations from the physical setting (an examination room within radiation oncology), such as noise, humming, or “struck with how it felt.” All HT providers reported that their patients usually fell asleep during the 45-minute session.
Discussion
This study demonstrated that accruing women to a complementary and alternative medicine study where they were blinded to group assignment was feasible; indeed, we were able to retain all but 3 participants throughout the 5 to 7 weeks of treatment. This study used a believable sham intervention and a well-validated fatigue instrument. Nevertheless, the study did not demonstrate significant improvements in fatigue or QOL for women receiving HT when compared with a sham therapy.
There are several studies with HT interventions that included breast cancer patients and had findings different from the outcomes of this study. First, Post-White et al 27 did a 3-group study with crossover (total of 230 patients) comparing massage therapy and HT therapy with no treatment controls. The HT group reported significantly greater reductions in fatigue compared with the control group. In the Post-White et al study, the patients were not blinded to group assignment, and a larger proportion of the controls dropped out because they did not want to be assigned to the presence group. In fact, the withdrawal rate from the control group was almost twice the withdrawal rate from the combined intervention groups (30/75 or 23% vs 36/155 or 40%). Fatigue was measured with the Profile of Mood States as opposed to the BFI used in the current study. Although the majority of patients had breast cancer (52%), other cancers were represented, and cancer stage/treatment was not limited. The second study, Cook et al, 14 randomized 62 patients to HT versus mock (sham) treatment, with the patients blinded to group assignment. They found that the HT group reported less fatigue but the differences were not statistically significant. As with the previous study, a different instrument was used to measure fatigue. Also, in Cook et al, 14 the participants were a mix of patients with breast and gynecological cancer. In the third study, Schnepper 6 enrolled 40 patients with early-stage breast cancer and found that the HT group did significantly better on the FACT physical well-being subscale but did not explicitly measure fatigue. The intervention and study periods were shorter (20-30 minutes weekly and 4 weeks, respectively). Although information was incomplete, the 3 studies also may have differed in Cochrane criteria for judging bias in intervention studies. 28 The risk of bias for the current study was relatively low (ie, less biased) compared with the previous studies.
The results of the current study, in contrast to these 3 studies, were that the participants who received sham therapy had a greater reduction in fatigue compared with those who were randomized to HT. One possible explanation is the disruption to provider-patient relationship imposed by the protocol.
Several patients spoke of a period of enforced rest as soothing and something they would not necessarily have scheduled had they not participated in the study. Although rest is not a recommended intervention to relieve cancer-related fatigue, 5 it is interesting to note that more women in the control group were working full- or part-time. Perhaps the enforced rest for those who had little opportunity to rest during the workday benefitted them to a greater extent than the participants who received HT. A period of rest with or without a therapeutic intervention may be worth considering as a supportive care component for breast cancer patients.
In this study, effect sizes were examined to determine the differential change from baseline to end of study in a standard format. The effect sizes found in this study are similar to the range of 0.17 to 1.0 found for psychosocial interventions reported in a Cochrane review. 29 The effect size for the sham therapy in this study was larger than that for HT, representing a moderate effect size. In the Cochrane review, interventions specific to fatigue were found to be more effective than nonspecific interventions (80% vs 14%). HT therapy is not considered specific to fatigue, so the effect may have been too small to detect in the sample size recruited for this study. In a review of bio-field therapies, Jain and Mills 30 noted the inconsistent findings regarding the effect of HT on fatigue in randomized controlled trials and suggested more comparisons with mock healing groups and focused outcomes on fatigue. Our study addressed these 2 design issues, and the findings do not support a therapeutic benefit of HT.
Considering interventions for fatigue at a broad level, a meta-analysis of psychosocial intervention studies with aims and/or outcomes to decrease cancer-related fatigue found lower effect sizes in studies limited to breast cancer patients (0.22) versus mixed samples that included other cancers (0.55). 5 Exercise interventions, however, had larger effect sizes for reducing fatigue in both breast cancer (0.60) and non–breast cancer patients (0.92). 5 Although the meta-analysis did not include an energy therapy, the effect sizes for psychosocial interventions tended to be smaller than the effect sizes for exercise interventions. 5 This differs from findings of an earlier meta-analysis, 31 but the 2 meta-analyses differed in how they separated the concept of fatigue from that of vigor/vitality, treatment of outcome scores, and number of studies included.
Limitations
This study was designed as a pilot study; the trial was not adequately powered to detect differences between groups on the key outcome variables. In addition to small sample size, the “dose” was limited to a single session each week. Finally, the effect of the intervention may have been weakened by the disruption of the patient-provider relationship. The fact that each HT participant saw a minimum of 3 providers, whereas the sham participants typically only saw 2 providers may have introduced bias into the intervention.
Conclusions and Implications
HT, an energy-based therapy, was tested to determine its effect on fatigue and QOL in women with breast cancer undergoing RT. Our enrollment to and retention in the trial indicate that it is feasible and acceptable to women during RT. Our findings do not support a beneficial effect of HT on fatigue or QOL when compared with a sham intervention, which controlled for attention. This raises the issue of 1 possible mechanism of action: Is it the presence of an empathetic individual or enforced rest at the end of the week? Future research may explore the therapeutic effect of the therapist and rest on fatigue in patients with cancer undergoing therapy. Future research may also consider several protocol modifications, including the following: (a) increasing the “dose” of HT to perhaps 45-minute sessions twice a week and (b) controlling for baseline fatigue—that is, beginning sessions only after there is measurable fatigue. As a means of teasing out therapist effect, we recommend using the same therapist for the sham and HT therapies, with the sham intervention designed to remove intention to heal (occupy therapist mind with multiplication tables as done by Schnepper 6 ), and remove intentional manipulation of energy fields.
Footnotes
Authors’ Note
Clinical Trial Registry: NCT00574145. The ClinicalTrails.gov site erroneously lists the trial as supported by NCI—the work was only supported by a Vanderbilt University discovery grant.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Discovery Grant from Vanderbilt University.