
Abstract
Background. Flax is a food and dietary supplement commonly used for menopausal symptoms. Flax is known for its lignan, α-linolenic acid, and fiber content, components that may possess phytogestrogenic, anti-inflammatory, and hormone modulating effects, respectively. We conducted a systematic review of flax for efficacy in improving menopausal symptoms in women living with breast cancer and for potential impact on risk of breast cancer incidence or recurrence. Methods. We searched MEDLINE, Embase, the Cochrane Library, and AMED from inception to January 2013 for human interventional or observational data pertaining to flax and breast cancer. Results. Of 1892 records, we included a total of 10 studies: 2 randomized controlled trials, 2 uncontrolled trials, 1 biomarker study, and 5 observational studies. Nonsignificant (NS) decreases in hot flash symptomatology were seen with flax ingestion (7.5 g/d). Flax (25 g/d) increased tumor apoptotic index (P < .05) and decreased HER2 expression (P < .05) and cell proliferation (Ki-67 index; NS) among newly diagnosed breast cancer patients when compared with placebo. Uncontrolled and biomarker studies suggest beneficial effects on hot flashes, cell proliferation, atypical cytomorphology, and mammographic density, as well as possible anti-angiogenic activity at doses of 25 g ground flax or 50 mg secoisolariciresinol diglycoside daily. Observational data suggests associations between flax and decreased risk of primary breast cancer (adjusted odds ratio [AOR] = 0.82; 95% confidence interval [CI] = 0.69-0.97), better mental health (AOR = 1.76; 95% CI = 1.05-2.94), and lower mortality (multivariate hazard ratio = 0.69; 95% CI = 0.50-0.95) among breast cancer patients. Conclusions. Current evidence suggests that flax may be associated with decreased risk of breast cancer. Flax demonstrates antiproliferative effects in breast tissue of women at risk of breast cancer and may protect against primary breast cancer. Mortality risk may also be reduced among those living with breast cancer.
Keywords
Introduction
Breast cancer is one of the most common cancers affecting Canadian women, with almost 23 000 new diagnoses expected in 2012. 1 Many women elect to use natural therapies in addition to conventional treatments in the management of their condition, in order to reduce the adverse effects of treatment or to influence the progression of the disease. 2
Flaxseed (Linum usitatissimum), also known as linseed, is widely cultivated throughout the northern hemisphere for both human and animal consumption. The seeds of the flax plant are the best-known plant-based source of the ω-3 fatty acid, α-linolenic acid, 3 as well as a source of fiber. Flaxseed has been studied for its potentially beneficial physiologic effects, including proposed anticancer effects, since the early 1980s. 4 A recent survey of breast cancer patients in Ontario, Canada, found that 33% reported consuming flaxseed regularly since diagnosis. 5
α-Linolenic acid has been shown to exert anti-inflammatory activity,6,7 and in animal models of premenopausal (high estrogen) breast cancer, it has been shown to have antiproliferative effects. 8 Fiber intake has been inversely associated with breast cancer risk 7 ; and in the Women’s Healthy Eating and Living Study, a large intervention trial, a dietary pattern high in fiber was shown to reduce risk of breast cancer recurrence, 9 likely through effects on hormone metabolism and elimination.9,10
Flaxseed is also one of the most important sources of the lignan precursor secoisolariciresinol (SECO), which occurs as secoisolariciresinol diglycoside (SDG) oligomers bound to hydroxymethylglutaric acid in the flax seed coat.4,11 It has also been suggested that SECO itself may act as a lignan in the body.4,12 Plant lignans as a group consist of phenolic compounds including enterolactone (ENL) and enterodiol (ED) (as well as others that are classified as phytoestrogens) alongside isoflavones, coumestanes, mycotoxins, and stilbenes. Although many foods contain lignans, flaxseed is unique in that it is the densest source of the lignan SDG, with between 60 and 300 mg lignans per 100 g serving.13-16 This diverse class of constituents is thought to possess varying degrees of both estrogenic and anti-estrogenic effects in vivo,17-21 in conjunction with more direct antitumor effects.22-24 Through metabolism by intestinal microbes, plant lignans are converted into their active mammalian forms, ENL and ED. 25 These metabolites appear to be responsible for some of the anticancer effects that have been attributed to lignans. 26
The potential therapeutic effects of phytoestrogen-containing plants continue to be explored in the literature. These compounds may have particular benefit in hormone-dependent conditions such as menopausal hot flashes. 27 However, for women with breast cancer, the decision to consume phytoestrogen-containing foods or supplements may be difficult, owing to concerns that these agents may be cancer promoting. The objectives of this systematic review are to assess the efficacy of flaxseed or its constituents, including flaxseed oil and flax lignans, in the management of hot flashes in women at risk of breast cancer incidence or recurrence and to determine the effect of this intervention on risk of breast cancer development, recurrence, or mortality.
Methods
Search Strategy
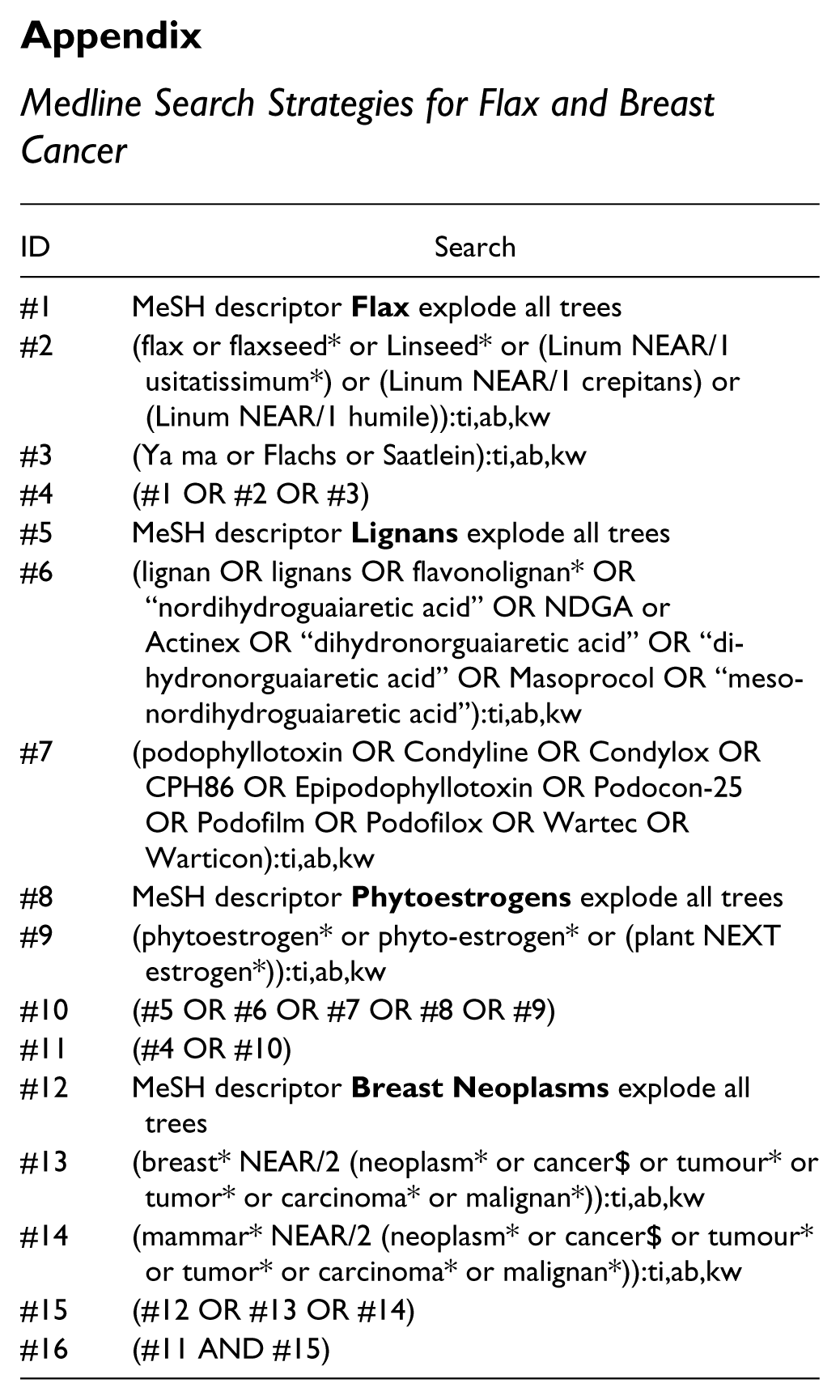
Electronic search strategies were designed through an iterative process and peer-reviewed prior to execution using the PRESS Checklist. 28 Using the OVID platform, we searched Ovid MEDLINE, Ovid MEDLINE In-Process & Other Non-Indexed Citations, EmbaseClassic + Embase, and Allied and Complementary Medicine (AMED) from inception to December 2, 2011, with an update of all databases conducted on January 19, 2013. We also searched the Cochrane Library on Wiley. MEDLINE was updated again prior to publication, on April 5, 2013. Strategies used a combination of controlled vocabulary (eg, Flax, Lignans, Breast Neoplasms) and keywords (eg, flaxseed, linseed, breast cancer). No language restrictions were applied. Specific details regarding the strategies appear in the appendix. Grey literature was identified using selected sites, including clinical trial registries, from CADTH’s Grey Matters: A Practical Tool for Evidence-Based Medicine 29 in December 2011.
Study Design
All published human intervention trials meeting our criteria for population characteristics, interventions, and outcomes were included. Both controlled and uncontrolled trials were considered. Observational data were also included, provided that appropriate markers of intake were used, as described below. No preclinical data were included in this review given the potential difficulty of extrapolating in vitro and animal data to humans. 30
Study Population
For inclusion, intervention studies had to include women who were at risk of breast cancer or who had a past or present diagnosis of breast cancer. Retrospective observational studies were required to include cases with breast cancer, while prospective studies were required to report on cancer-related risk outcomes, as described below. No limitations were imposed by menopausal status, tumor characteristics, cancer staging, or type of breast cancer.
Interventions and Measures of Exposure
All trials using flaxseed, flaxseed-derived SDG, or other flax-derived products such as flaxseed oil, as an intervention, as well as those evaluating dietary intake of flaxseed were included. Observational studies assessing overall lignan intake or measuring serum levels of flaxseed metabolites such as ED, ENL, or SECO were not included, as these compounds may be derived from many different sources16,31 and are not specific to flaxseed. Sources of these compounds include beverages, nuts, seeds, grains, fruits, and vegetables in the average diet. 32
Outcomes of Interest
Studies were included if they evaluated the effect of flax on menopausal symptoms and hot flashes using either of the following 2 conditions:
A generalized menopausal symptom score (Kupperman Index, Greene Climacteric Scale, Menopause Rating Scale)
Any measure of hot flashes (subscore of generalized scale, daily record of frequency and/or severity)
Studies reporting on one or more of the following outcomes relating to breast cancer risk or disease progression were also included:
Risk of breast cancer incidence, recurrence, or survival
Tumor characteristics (receptor status)
Surrogate markers of risk (tissue proliferation index, serum and urinary estrogen levels)
Evidence of changes in other hormonally responsive tissue (breast density, vaginal maturation index, endometrial thickness)
Data pertaining to adverse events occurring within identified studies were also extracted.
Screening of Records and Data Extraction
Titles and abstracts (where available) of all search results were reviewed by one researcher (RF), and a second reviewer (GF) conducted a quality control of a selection of excluded results. A third reviewer (HF) was consulted in cases of disagreement. Full-text copies of all included records were obtained, and a second pass screening was conducted.
Data were extracted by GF using a piloted extraction sheet, 33 and HF performed quality control on 50% of extracted records. No notable differences were seen between reviewers. Quality assessment fields were based on the Consolidated Standards of Reporting Trials (CONSORT) statement for clinical trials and the Newcastle-Ottawa Scale (NOS) for observational studies.34,35 Risk of bias assessments were conducted using the Cochrane Collaboration’s tool for assessing risk of bias in randomized trials 36 and the NOS for observational studies. Data pertaining to patient demographics, interventions, and outcomes as described above were also collected.
Results
A total of 1892 records were screened from all sources. A total of 10 studies met the predefined inclusion criteria,37-46 and these studies were included for full analysis. Figure 1 shows the literature flowchart depicting the process of article assessment and selection that was undertaken for this review. Tables 1 and 2 summarize the methods and results of included randomized controlled trial (RCTs) and uncontrolled trials.39-42

Literature flowchart.
Methods of Human Trials of Flax and Breast Cancer.

Abbreviations: abst, abstract; AI, aromatase inhibitor; Br Ca, breast cancer; HF, hot flashes; I, intervention; n, number of participants; n/a, not applicable; NR, not reported; Pre, premenopausal; Post, postmenopausal; P, placebo; SDG, secoisolariciresinol diglycoside; Tamox, tamoxifen.
Five-year Gail model risk of ≥1.7%—3-fold higher-than-average risk.
Seventeen participants had biopsy showing lobular carcinoma in situ or atypical ductal hyperplasia.
Six participants were also involved in a blinded study and may also have been taking tamoxifen (5) or an aromatase inhibitor (1).
Outcomes of Human Trials of Flax and Breast Cancer.

Abbreviations: BL, baseline; E2, estradiol; GI, gastrointestinal; HF, hot flashes; NR, not reported; NS, nonsignificant; QOL, quality of life.
Randomized Controlled Trials
One of the 2 RCTs assessed the effect of 7.5 g of ground flaxseed on hot flashes compared with placebo. 40 The study population included 44 women taking tamoxifen and 91 with a history of breast cancer. Following 6 weeks of treatment with flax-containing bars (410 mg lignans), a nonsignificant decrease in hot flash composite scores (−4.9 points and −3.5 points in the flax and placebo groups, respectively, P = .29) and hot flash frequency (−29% and −28%, respectively, P = .90) was observed. A total of 36% of participants reported a 50% decrease in their hot flashes over the course of the study. No between-group differences were reported, and no difference in response was observed between women experiencing treatment-induced and natural menopausal symptoms. The intervention and placebo bars were well matched for other factors, with both containing approximately 200 calories, a small amount of protein, and 20 g fiber.
In the second RCT, muffins containing 25 g of flaxseed (50 mg SDG) were consumed by 32 women with primary breast cancer for a mean of 32 days prior to surgery. 42 Core tumor biopsies were obtained before and after flax treatment. Flaxseed significantly (P < .05) increased tumor apoptotic index (+30.7%) and decreased c-erbB2 (HER2) expression (−71.0%) compared with placebo (+8.0% and +55.0%, respectively). In addition, total intake of flax was significantly correlated with a change in c-erbB2 score (r = −.373, P = .036) and apoptotic index (r = .495, P < .004). The Ki-67 labeling index, a marker of cell proliferation 47 associated with poor disease-free survival and overall survival in women with breast cancer, 47 decreased significantly in tumor tissue compared to baseline in the flax group (−34.2%, P < .01), but not in the control group; however, this was not statistically significant when the 2 groups were compared (P value not reported).
Uncontrolled Trials
Two uncontrolled trials were included for analysis.39,41 The first reported that 40 g (4 tablespoons) of crushed flaxseed containing 400 mg of SDG led to a highly significant (P < .001) median decrease in hot flash scores of 50% compared to baseline following 6 weeks of flax administration. 41 Women in the study experienced a minimum of 14 hot flashes per day at baseline; 1 participant was taking an aromatase inhibitor and 5 were receiving tamoxifen therapy. Participants also reported a highly significant (P < .001) improvement on the impact of hot flashes for overall quality of life (mean score increased by 23 points on a 100-point scale).
In a second uncontrolled trial, 50 mg of SDG in capsule form was administered over a 12-month period to women at increased risk of breast cancer incidence or recurrence. 39 SDG was shown to decrease Ki-67 nonsignificantly in benign breast tissue compared to baseline. In a subgroup analysis of responders (80% of sample), a significant decrease in median Ki-67 was demonstrated (4%; [range = 2% to 16.8%] at baseline; 2% [0% to 15.2%] at 12 months, P < .001). In addition, the percentage of women with atypical cytomorphology was significantly higher at the beginning of the study (62%) than at its conclusion (42%; P < .035). Median mammographic density decreased nonsignificantly by 6.3%, and serum estradiol levels were unchanged by the intervention.
Biomarker Study
A nonrandomized, open-label, ex vivo study investigated the potential anti-angiogenic effects of flaxseed in normal breast tissue of healthy women, compared to tamoxifen, in normal breast tissue of women who had been treated for early breast cancer. 45 Nine healthy women consumed 25 g ground flaxseed containing 44.32 mg SECO daily for 6 weeks, and 11 women who were treated for breast cancer took tamoxifen 20 mg daily. Markers of angiogenesis in normal breast tissue and subcutaneous fat tissue were measured before and after 6 weeks of treatment. The following markers were assessed: vascular endothelial growth factor (VEGF), angiogenin, and endostatin. There was a differential effect of tamoxifen and flax on VEGF and angiogenin, where tamoxifen significantly decreased levels of both markers, but flax did not. Both tamoxifen and flax increased levels of endostatin by approximately 33%, flax in breast tissue but not subcutaneous fat, and tamoxifen in both compartments. Since endostatin is an anti-angiogenic factor in breast tissue, the authors concluded that that flax may exert its antitumor effects in part through effects on endostatin.
Observational Evidence
Five observational studies, consisting of 3 case–control studies and 2 cohort studies, were included in the final analysis. A number of observational studies were identified that reported on associations between ENL levels and breast cancer risk, but the majority of these were excluded since the specific effect of flax could not be isolated. The studies discussed below identify flax as a major contributor to the classes of foods investigated in each report.
An initial case control study by Cotterchio et al investigated lignan intake and breast cancer risk, stating that flaxseed accounted for 88% of total lignan intake among participants. 38 In this analysis, a daily intake of ≥5.35 mg lignans was associated with a 19% reduction in risk of breast cancer incidence (multivariate [MV] odds ratio [OR] = 0.81; 95% confidence interval [CI] = 0.65-0.99). Subgroup analysis by body mass index (BMI) found increased benefit in women with a BMI ≥25 (0.70; 0.53-0.93), compared to those with a BMI <25 (0.92; 0.67-1.25). No differentiation of risk by menopausal status was found.
In 2013, Cotterchio’s group reported a second study looking specifically at flaxseed intake. 13 Compared to never-use, those women who consumed ¼ cup flaxseed (163 mg lignans) on a daily or weekly basis had an approximate 20% decreased risk of breast cancer, adjusted OR [AOR] = 0.82 (95% CI = 0.69-0.97). Similarly, consumption of 1 piece of flax bread (3.6 mg lignans) on a weekly or daily basis was associated with an approximate 30% decreased risk of breast cancer, AOR = 0.77 (95% CI = 0.67-0.89). In both cases, these relationships remained significant for postmenopausal women, but not among premenopausal women.
A German case–control study assessed the effect of combined flax and sesame seed intake on postmenopausal breast cancer risk. 46 The study found no significant association between “high” flax consumption (not quantified) and nonconsumption, AOR = 0.93 (95% CI = 0.83-1.04); however, median intake among the study population as a whole was low, 1.42 g per day. Similarly, there was no significant association between intake of SECO and risk of breast cancer, AOR = 1.05 (95% CI = 0.90-1.21). There was no significant modification by ER+ or ER− status.
One prospective cohort study evaluated the combined effect of sesame and flaxseed intake on mortality. 37 No linear association between sesame/flax intake and either overall mortality or breast cancer mortality could be identified. Although women in the study consuming 0.3 to 3.5 g/day of sesame/flaxseed had a 31% reduction in overall mortality (multivariate [MV] hazard ratio [HR] = 0.69; 95% CI = 0.50-0.95), those ingesting ≥3.6 g/day had no survival advantage (MVHR = 0.90; 95% CI = 0.68-1.19).
A second cohort study assessing phytoestrogen-supplement usage found an association between flaxseed oil use and better mental health scores on health-related quality-of-life questionnaires, AOR = 1.76 (95% CI = 1.05-2.94). 43 Flaxseed oil use was defined as ever-use since being diagnosed with breast cancer. However, there was no association between flax oil and fatigue or report of hormone related symptoms.
Adverse Events
Adverse events were reported in all RCTs and uncontrolled trials. The 2 RCTs described increased frequency of abdominal fullness, flatulence, nausea, and bowel movements in the group consuming flax, but the difference from placebo was not statistically significant.40,42 Gastrointestinal complaints and instances of irregular menses are recorded by Fabian et al, 39 but the authors of this uncontrolled trial concluded that these were unlikely to be treatment related. Bloating was reported in 50% of participants in another uncontrolled trial, and gastrointestinal effects were cited as the cause of treatment discontinuation in 3 study participants. 41
Discussion
Investigations into the potential role of flax in breast cancer management are limited at present. Only 2 studies examine the use of flax in the management of hot flashes in women with cancer.40,41 Both trials report some benefit from the intervention, but in the RCT, this effect was not different from placebo. Given that the placebo effect accounts for up to 60% of improvements in hot flashes in other intervention studies, 48 this should not necessarily be discounted. In addition, the large difference in dose of gross flaxseed between the 2 studies should be considered, with one study using a small dose of 7.5 g flaxseed (410 mg lignans) per day, while the uncontrolled trial showing seemingly greater benefit used a dose of 40 g ground flaxseed (400 mg SDG). Further well-designed clinical trials are needed before a definitive statement can be made as to the specific effects of flaxseed on hot flash frequency or severity.
Observational studies reviewed suggest that flax or flax-derived lignan consumption may decrease risk of breast cancer when adequate amounts are consumed (¼ cup ground flax, equivalent to 32 g ground flax or 163 mg lignans daily or weekly in one study, respectively).13,38 However, in some studies, the dose of flax consumption was in the low range, such as 1.42 g per day, 46 limiting the likelihood of observing any therapeutic effects. Notably, only 1 study isolated the contribution of flax per se 13 to breast cancer risk: one study considered total lignan consumption while citing flax as a major contributor, 38 and 2 studies investigated the combined intake of flax and sesame seeds. 37 Nonetheless, if these are confirmed by subsequent studies, flax could emerge as an important agent in the chemoprevention of breast cancer.
Flax appears to also possess antitumor activity. Studies by Thompson and Fabian indicate that flax increases tumor apoptotic index, decreases HER2 expression, and decreases tumor cell proliferation (Ki-67 labeling index) in breast cancer patients,39,42 while a biomarker study suggests that flax may have anti-angiogenic activity in breast tissue. 45 These biomarker studies suggest that consumption of flaxseed at 25 g per day, containing 50 mg SDG, may contribute to overall antitumor effects.39,42,45 These actions may also explain the observations reported by Lowcock et al regarding chemoprotective effects of flax consumption at higher doses. 13 This question deserves further study in large, well-designed trials.
Population Studies: Lignans and Breast Cancer Risk
As discussed above, flaxseed is an important source of the plant lignan SDG, a precursor to the mammalian lignans ENL and ED. 25 Other sources of dietary lignans include fruits and vegetables, tea, grains, and alcoholic beverages. 49 While results of studies measuring overall lignan intake and serum ENL levels should not be extrapolated directly to flax, results from these studies do encourage further research into the potential risk-attenuating effects of flaxseed consumption. 13
Population studies point to a potential role of dietary plant lignans in the prevention of cancer. One meta-analysis of dietary lignan consumption reported no association with breast cancer risk (pooled risk estimate [RE] = 0.92; 95% CI = 0.81-1.02). 50 However, when a subgroup analysis by menopausal status was conducted, a significant reduction in risk was observed among postmenopausal women (RE = 0.86; 95% CI = 0.78-0.94). An earlier meta-analysis parallels these results: no association was identified until postmenopausal women were considered in isolation (OR = 0.85; 95% CI = 0.78-0.93; P < .001). 51 Similar findings were reported by 2 studies in our review.13,38 These findings may lead to the speculation that a low-estrogen environment is required for the protective effects of plant lignans, such as those found in flax, to become clinically relevant. Alternatively, preclinical studies indicate that flax may possess aromatase inhibitory effects that have more impact on postmenopausal populations. 52 The potentially protective effects of flax merit further investigation to identify the populations that may benefit most from this intervention.
As animal studies suggest that SDG requires conversion to ENL in order to initiate its anticancer activity, 26 associations between serum ENL levels and cancer risk should be investigated. While recent studies associate decreased breast cancer mortality with higher serum ENL levels,53,54 others assessing risk of breast cancer incidence and ENL show no association.50,51 This lack of observed effect does not necessarily rule out an association between ENL and cancer risk, since ENL is a good marker of short-term intake only 50 and may not be the most appropriate marker of long-term SDG exposure. Additionally, antibiotics, 55 smoking, and poor digestive function affect ENL production, reducing its levels by up to 30%, and this may confound possible correlations with cancer risk.56,57
Flax Estrogenic Effects
In vitro, flaxseed metabolites such as ENL have been shown to interact with estrogen receptors, 58 behaving as weak estrogen agonists.59,60 While this action may be of concern to women with breast cancer, flaxseed administration appears to have no significant effect on endogenous estrogen levels in the majority of human trials, either in women with cancer 39 or in healthy women.61-65 Conversely, studies that do report significant changes cite decreases in serum estrogen levels, suggesting reduced exposure to endogenous estrogen over time19,66 with flaxseed consumption. Fabian et al assessed the effect of 50 mg of SDG on breast density over a 12-month period. Mammographic assessment found no significant change from baseline in breast tissue density following this intervention. These results lend further support to the notion that flaxseed does not appear to have a significant estrogenic effect in vivo.
A high ratio of 2-hydroxyestrone (2OH) to 16-α-hydroxyestrone (16αOH) has been put forth by some authors as being protective against breast cancer risk. 67 Flax seed ingestion significantly increased the ratio of these urinary estrogen metabolites from baseline in 4 studies,21,68-70 while a fifth reported a significant decrease in 2OH:16αOH. 62 The predictive value of this ratio is under investigation. Although a lower 2OH:16αOH ratio has been reported in women with breast cancer compared to healthy controls, 71 a recent systematic review of 1871 breast cancer cases and 2915 controls failed to find significant association with cancer incidence. 72 Subsequent epidemiological studies suggest instead that excretion ratio of estrogen metabolites to parent compounds is a more significant marker of risk.73,74 Further research is needed to determine any potential significance of this ratio, but the potential effect of flax on urinary metabolites is not associated with increased harm.
Effect by ER Status
To date, studies assessing the effect of flax on risk of breast cancer have not identified a clearly differential effect according to ER status. Lowcock reported protective effects overall associated with flax consumption, and when stratified by hormone status, the effect was nonsignificant, but similar in both groups: ER+/PR+, OR = 0.81, 95% CI = 0.66-1.01, and ER−/PR−, OR = 0.75, 95% CI = 0.53-1.06. 13 A German case–control study reported no significant overall effects associated with high flax consumption (quantity not specified) or SECO consumption and the risk of breast cancer; on subanalyses, there was no modification of effect by ER+ or ER− status. 46 Buck et al found no difference in the effect of flax on breast cancer mortality according to ER status. 37 In the biomarker study by Thompson et al, baseline tumor characteristics including ER status did not affect the antiproliferative effects of flaxseed in vivo. 42 In addition, given the apparent anti-estrogenic effects of flax in vivo as discussed above, it seems unlikely that flax consumption would have tumor-promoting effects in ER+ breast cancer, and this appears to be supported by human evidence to date.
Mechanism of Action
Animal studies provide some insight into the potential, multifaceted anticarcinogenic actions of flaxseed and its metabolites. Flaxseed and SDG have been shown to possess antiproliferative, 23 anti-angiogenic, 22 and pro-apoptotic 75 effects in vivo, resulting in decreased tumor size,76,77 multiplicity, 78 and a reduction in metastases. 24 Markers of disease progression including VEGF 79 and CRP 80 are also attenuated by this intervention. Preliminary human studies appear to support these results, demonstrating that 50 mg of SDG significantly reduces HER2 expression and cell proliferation while increasing apoptosis.39,42
In addition to its direct antitumor effects, flaxseed may be chemoprotective through its influence on endogenous estrogen activity. As weak aromatase inhibitors, 52 flaxseed metabolites may in theory decrease serum estrogen levels, although this action has not been demonstrated in the literature. This effect may be enhanced by the association of lignan-containing foods with higher levels of sex hormone-binding globulin. 81 As a weak estrogen agonist, ENL may competitively inhibit and decrease the effect of endogenous estrogen on the estrogen receptor and target tissues, in theory providing some protection against breast cancer.
Drug Interactions
No human-level data describe interactions between flaxseed and selective estrogen receptor modulators such as tamoxifen or aromatase inhibitors such as anastozole. Animal models investigating the effects of a combination of flax or flax-derived interventions with tamoxifen suggest an additionally protective effect of the combination of these treatments. Flaxseed, flax oil, or SDG in combination with tamoxifen appears to reduce tumor size by a greater margin than through tamoxifen treatment alone.23,82-84 Flax appears to increase apoptosis and decrease cell proliferation,23,83 without any negative skeletal effects. 85
Strengths and Limitations
The primary limitation of this review is the lack of high-quality evidence on the subject of flaxseed use in women at risk of breast cancer, as well as lack of data on risk of recurrence in women with breast cancer. Of 5 included clinical trials, only 2 were RCTs. Existing trials of flaxseed are hampered by considerable differences in the type and dose of intervention used (ranging from 7.5 to 40 g of flaxseed vs isolated SDG), as well as frequently poor description of the agent and constituents (sometimes described in terms of SDG content or unspecified lignans). Unfortunately, studies examining ground flaxseed as a whole agent do not allow for easy attribution of effects to a single bioactive constituent, for instance, lignans or more specifically SDG, fatty acid content, or fiber content. More complex study designs comparing ground flaxseed to equivalent dosages of isolated SDG and/or flaxseed oil are necessary to tease apart these details.
In addition, 3 observational studies included in our review assessed the effect of flax in combination with that of other foods, limiting our ability to attribute any association directly to flax.37,38,46 Observational studies of flax consumption are generally limited by the low dosages commonly consumed, although the study by Lowcock was able to assess more sizable dosages. 13 This is the first systematic review of the safety and efficacy of flax with respect to breast cancer and includes data from both interventional and observational studies.
Conclusion
The available evidence does not support the use of flaxseed for the management of hot flashes in women at risk of or surviving breast cancer; however, there is a need for further investigations assessing higher dosages of flax or flax lignans in a controlled manner. Although improvements in hot flash scores were seen in the 2 trials included for review,40,41 effects could not be distinguished from that of placebo. Observational data suggest that flaxseed may be protective against breast cancer, with intakes of ¼ cup (~32 g ground flaxseed) or approximately 160 mg SDG demonstrating the strongest cancer protective effects thus far. Biomarker studies in breast cancer patients indicate increased tumor cell apoptosis, decreased HER-2 expression, decreased tumor cell proliferation, and anti-angiogenic activity in vivo at doses between 25 g ground flax or 50 mg SDG per day. Additional studies specifically assessing flaxseed consumption are needed to accurately ascertain potential effects. Evidence pertaining to the metabolites that may be derived from flaxseed implies a protective effect, particularly in postmenopausal women. Animal data point to broad, anticancer effects of flaxseed as an intervention, but should be interpreted with caution until they can be corroborated by evidence in humans. Information pertaining to potential drug interactions is incomplete but current literature does not suggest negative effects. Current evidence suggests that flax consumption may decrease risk of breast cancer development and may exert antitumor effects in women with breast cancer when used at doses of 25 g ground flaxseed or 50 mg SDG per day.
Footnotes
Appendix
Medline Search Strategies for Flax and Breast Cancer
| ID | Search |
|---|---|
| #1 | MeSH descriptor |
| #2 | (flax or flaxseed* or Linseed* or (Linum NEAR/1 usitatissimum*) or (Linum NEAR/1 crepitans) or (Linum NEAR/1 humile)):ti,ab,kw |
| #3 | (Ya ma or Flachs or Saatlein):ti,ab,kw |
| #4 | (#1 OR #2 OR #3) |
| #5 | MeSH descriptor |
| #6 | (lignan OR lignans OR flavonolignan* OR “nordihydroguaiaretic acid” OR NDGA or Actinex OR “dihydronorguaiaretic acid” OR “di-hydronorguaiaretic acid” OR Masoprocol OR “meso-nordihydroguaiaretic acid”):ti,ab,kw |
| #7 | (podophyllotoxin OR Condyline OR Condylox OR CPH86 OR Epipodophyllotoxin OR Podocon-25 OR Podofilm OR Podofilox OR Wartec OR Warticon):ti,ab,kw |
| #8 | MeSH descriptor |
| #9 | (phytoestrogen* or phyto-estrogen* or (plant NEXT estrogen*)):ti,ab,kw |
| #10 | (#5 OR #6 OR #7 OR #8 OR #9) |
| #11 | (#4 OR #10) |
| #12 | MeSH descriptor |
| #13 | (breast* NEAR/2 (neoplasm* or cancer$ or tumour* or tumor* or carcinoma* or malignan*)):ti,ab,kw |
| #14 | (mammar* NEAR/2 (neoplasm* or cancer$ or tumour* or tumor* or carcinoma* or malignan*)):ti,ab,kw |
| #15 | (#12 OR #13 OR #14) |
| #16 | (#11 AND #15) |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a knowledge synthesis grant from the Canadian Institutes of Health Research (CIHR). Deborah Kennedy is supported by a career development grant from the Sickkids Foundation.