
Abstract
Radiation-induced skin damage is one of the most common complications of radiotherapy. In order to combat these side effects, patients often turn to alternative therapies, which often include antioxidants. Antioxidants such as those in the polyphenol chemical class, xanthine derivatives, tocepherol, sucralfate, and ascorbate have been studied for their use in either preventing or treating radiotherapy-induced skin damage. Apart from their known role as free radical scavengers, some of these antioxidants appear to alter cytokine release affecting cutaneous and systemic changes. We review the role of antioxidants in treating and preventing radiation-induced skin damage as well as the possible complications of using such therapy.
Keywords
Introduction
Skin complications secondary to radiation therapy occur in a majority 1 of patients and may often necessitate alterations in radiation therapy. 2 Though more recent radiation protocols that decrease dose delivery and improve precision have led to a decrease in skin reactions, radiation-induced skin damage still represents a common side effect of radiotherapy.3,4
Radiation-induced skin damage comes in many forms ranging from acute radiodermatitis to chronic skin fibrosis. Acute radiodermatitis is a generalized erythema that becomes visible within 90 days of radiation therapy, often between 2 and 4 weeks following radiotherapy, presenting as a blanchable sustained erythema.5-7 The National Cancer Institute grades the severity of this dermatitis from 1 to 4. 8 Grade 1 presents as a faint erythema that may demonstrate dry desquamation, epilation, or decreased sweating. Pigmentary alteration and pruritus are also common findings in grade 1 radiodermatitis. Grade 2 presents as a brighter or tender erythema that demonstrates moist desquamation within skin folds and also moderate edema. This level of damage typically occurs after 4 to 5 weeks of radiotherapy when greater than 40 Gy is given. 9 One to 2 weeks following the cessation of radiotherapy, this dermatitis begins to subside with an increased expression of epidermal growth factor receptors.10,11 Complete resolution may occur within 1 to 3 months. The formation of bullae and the damage to the barrier function of the skin make patients more susceptible to infections 2 , especially by Staphylococcus aureus. 12 Infection is, however, a rare consequence of radiodermatitis. Grade 3 involves moist desquamation outside of skin folds with pitting edema. Grade 4 is characterized by ulcerated tissue with necrosis or bleeding. When any of these acute reactions fail to resolve, progression to chronic radiodermatitis or skin fibrosis can occur. This grading system is summarized in Table 1.
Summary of the National Cancer Institute Grading System for Radiodermatitis.

Chronic radiodermatitis is histopathologically demonstrated by telangiectasia, fibrosis, loss of hair follicles as well as sebaceous and sweat gland atrophy 13 . Postinflammatory pigmentary alteration is also commonly seen. Additionally, atypical fibroblasts appear in the dermis with associated fibrosis leading to loss of adipose tissue. Microvascular changes and the decrease in normal dermal fibroblasts and stem cells can predispose the patient to ulcers and poor healing.9,14,15
Radiation-induced skin changes can cause significant distress and a decreased quality of life. 16 Patients often seek out various alternative therapies to combat these skin changes and other radiotherapy-induced side effects. 17 Although many of these alternative therapies have not been fully evaluated, 18 antioxidants appear to be a promising therapy for the prevention and treatment of some of the radiation-induced skin damage.18,19 An understanding of the pathophysiology of radiation-induced skin changes is essential to appreciating antioxidants’ role in this process. We review this physiology and also the current body of knowledge regarding the use of antioxidants for both the prevention and treatment of radiation-induced skin damage, including acute radiodermatitis and skin fibrosis.
Pathophysiology of Radiodermatitis
A multitude of cytokine irregularities have been demonstrated to play a role in radiation induced skin toxicity. 20 Transforming growth factor-β (TGF-β) is the principal cytokine involved in the development of chronic radiodermatitis and skin fibrosis 5 through its effect on dermal fibroblasts.21-23 TGF-β levels appear to rise in part because of the formation of thrombin mediated by radiation-induced vascular damage resulting inactivation of the coagulation cascade.24,25 Increased levels of interleukin-1 and tumor necrosis factor-α (TNF-α) have been shown to stimulate the production of metalloproteases causing degradation of dermal components and disruption of the basal cell layer.26,27 Upregulation of adhesion factors such as intercellular adhesion molecule-1, in conjunction with TNF-α production, also contributes to the inflammatory process.13,28
Bone marrow–derived cells appear to play a role in the healing of radiodermatitis. Mesenchymal stem cells, endothelial progenitor cells, and myelomonocytic cells have been shown to migrate toward areas of radiation damage, likely because of the chemotactic effects of stromal derived factor-1 and CXCR4 overexpression.29,30 Myelomonocytic cells appear to be the most important of these bone marrow–derived cells in the postradiation healing process by expressing angiogenic factors. These cells have, however, also been linked to initiating the inflammatory cascade and ischemia reperfusion injury.31,32
Radiotherapy additionally causes damage to Langerhans cells, basal cells, and vascular endothelium.33-35 The decreased number of Langerhans cells and the depletion of basal layer stem cells lead to impaired barrier and immune function, increasing the risk of wound infection. Damage to vasculature can induce hypoxia and TGF-β production, further driving fibrosis. 36 Tissue hypoxia with associated necrosis and inflammation can lead to the generation of significant amounts of reactive oxygen species (ROS). 13
Several endogenous physiologic substances are present to control the effects of ROS, including the superoxide dismutase, catalase, and glutathione peroxidase system. 37 Following radiotherapy, however, ROS overwhelm these systems, leading to excess ROS causing cellular damage. 38 Additionally, these ROS can drive the production of cytokines, perpetuating the cycle of inflammatory changes. 39 Targeting these ROS has been a goal in the development of therapies to prevent and treat radiodermatitis. A summary of the various pathways in radiotherapy-induced skin toxicity is provided in Figure 1.
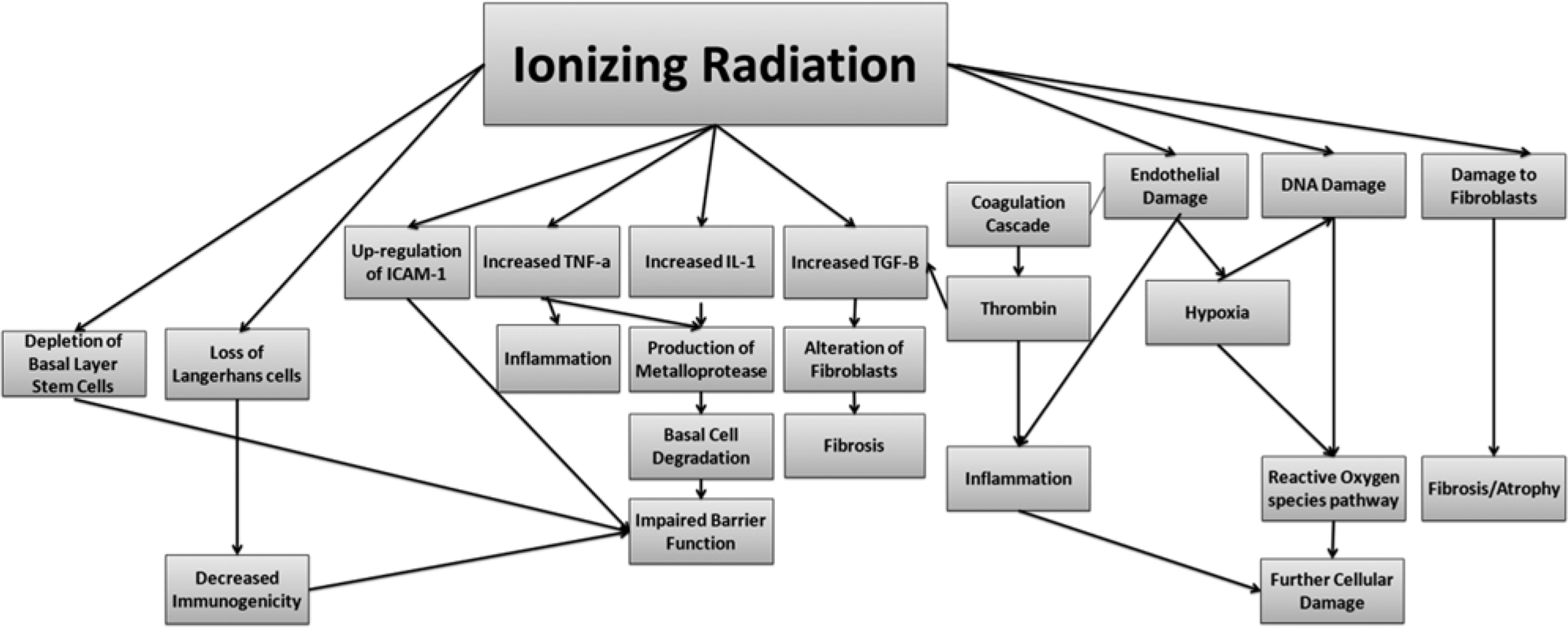
Simplified flowchart of the pathophysiology of the development of radiation-induced skin damage.
Antioxidants Studied in Radiodermatitis
One of the most studied therapies targeting the oxidative pathway is topical superoxide dismutase. Superoxide dismutase scavenges ROS in addition to acting as an anti-inflammatory. 40
Numerous studies, both in vitro and in vivo, have shown success with the use of topical superoxide dismutase for the regression of skin fibrosis and mitigation of acute radiodermatitis with little to no side effects, though there is a need for placebo-controlled trials.41-47 Limitations to its application have, however, included its short half-life time and its high cost. Modifications made to the structure of the enzyme, as well as its delivery vehicle have improved its applicability as a therapy by increasing the duration of action and increasing the availability of the enzyme.48-50 The clinical success achieved with this potent antioxidant has stimulated interest in exploring natural occurring and more affordable antioxidant substances.
Polyphenols
Polyphenols are bioactive substances that include numerous chemical structures, most notably flavones. They are often found in edible plants and additionally are used as food preservatives. 51 An example of the molecular backbone structure of a flavone is provided in Figure 2. These substances exhibit strong antioxidant properties and have been studied for various applications. Silymarin, an extract of milk thistle, has been shown to delay the development of radiodermatitis from 29 to 45 days, as well as curb the severity of cutaneous toxicity in patients receiving radiotherapy, with 10% of patients demonstrating grade II radiodermatitis versus 52% in the placebo group 5 weeks following the development of radiodermatitis. 52 In vitro studies have demonstrated silymarin’s ability to scavenge free radicals as well as serve as an anti-inflammatory.53-54 Other polyphenols such as catechins, genistein, proanthocyanidins, and resveratrol have been shown to act in a similar manner when studied as a photoprotective agent. 55 Polyphenols have also been implicated in accelerated wound healing56,57 and inducing physiologic antioxidant regulatory systems by stimulating nuclear-factor (erythroid derived 2) like-2.58,59 Trials with topical aloe vera, known to contain polyphenols have, however, varied in their demonstration of clinical efficacy in preventing radiotherapy induced skin toxicity.60,61While 2 earlier studies demonstrated no improvement in radiodermatitis with the use of aloe vera, a recent study of aloe vera by Di Franco et al 62 noted improvements in radiodermatitis, determined by using corneometry to measure the barrier function of the skin. This study, however, demonstrated that the moisturization of the skin primarily lead to the improvements in barrier function, not necessarily the aloe vera. Results from studies of Calendula extract, have additionally been inconclusive, with the effect of moisturization seemingly more effective than added extracts.63,64 Determining the efficacy of plant extracts is challenging as these extracts such as aloe vera and Calendula often contain numerous polyphenols, not isolated and concentrated polyphenols. Polyphenols have many chemical structures that could alter their biologic activities. Studies of mixed polyphenols derived from complex plant extracts thus make it challenging to evaluate any one particular polyphenol’s clinical success or failure compared with other members of the family of phytochemicals. A clinical trial comparing the efficacy of using the topical vehicle versus the vehicle plus extract could contribute meaningful data.

Chemical backbone structure of a flavone.
Additional factors also must be considered before applying topical polyphenols. Care must be taken as patients may experience contact dermatitis from certain polyphenols such as that found in aloe or many other plants.65,66 Though there is a concern that antioxidants may interfere with treatment, an issue discussed later, certain antioxidants have demonstrated improved treatment. For example, soy isoflavones have been found to sensitize prostate cells, and also nonsmall lung cells to radiotherapy, while reducing collateral toxicity.67-72 Hydroxychalcone, another type of polyphenol was found to cause radiosensitization in colon and pancreatic cells by causing activation of heat shock protein-1. 73 Resveratrol additionally has demonstrated radiosensitizing behavior in other cancer cells. 74 Therefore, polyphenols could potentially augment traditional cancer therapy while minimizing radiation-induced skin toxicity. In addition to requiring further studies regarding their interaction with tumor cells, more rigorous standardization of polyphenol processing is needed to demonstrate which particular molecules will have the greatest efficacy.
Pentoxifylline and Tocepherol
Pentoxifylline is a xanthine derivative, which, in addition to acting as an antioxidant, was found to increase the flexibility of erythrocytes improving blood flow within the microvasculature. 75 This increase in blood flow has been demonstrated to improve tumor radiosensitivity.76,77 and may reduce hypoxia secondary to vascular damage following radiation. Pentoxifylline has been demonstrated to inhibit interleukin-1 and TNF-α release curbing inflammation and inhibiting fibroblast proliferation.78,79 Studies on pentoxifylline have demonstrated success at preventing chronic radiation-induced fibrosis and soft tissue necrosis compared with control groups, with a 28% reduction in the incidence of soft tissue injury.80,81 Acute radiodermatitis does not appear to improve with the use of pentoxifylline.82,83 Pentoxifylline has often been studied in combination with another antioxidant: tocepherol (vitamin E).
Tocepherol, a free radical scavenger, on its own was not found effective in preventing acute skin fibrosis, 84 but in combination with pentoxifylline it did cause a significant regression of skin fibrosis versus placebo. 85 Tocepherol has also been found to modulate matrix metalloproteinase and collagenase transcription in addition to inhibiting platelet aggregation. 86 The effect that these non-antioxidant properties have on radiodermatitis is unclear. Similarly to flavones, topical application of these antioxidants potentially carries the risk of contact allergy. 87
Sucralfate
Sucralfate is a weak free radical scavenger, significantly less potent than tocepherol. 88 Its ability to prevent skin toxicity is unclear. Maiche et al 89 demonstrated a significantly decreased severity in acute radiodermatitis with a faster recovery period compared with placebo. In this study, however, different topical vehicles were used possibly affecting the study’s finding. Delaney et al 90 compared sucralfate in a cream with the same delivery vehicle without sucralfate. They demonstrated no significant improvements in healing, calling into question whether sucralfate or the vehicle accounted for the change noted in the study by Maiche et al. Later studies of sucralfate demonstrated no improvements in acute radiodermatitis when compared with patients applying aqueous solution or no solution at all.88,91 Sucralfate thus far appears to be ineffective at preventing radiation-induced skin damage.
Ascorbate
Ascorbate is a strong antioxidant that acts as a scavenger of peroxyl radicals. 92 Though previous in vitro studies on ascorbate demonstrated minimal protection of normal tissue during radiotherapy, 93 a clinical trial of topical ascorbate found no advantage to its use in preventing or treating radiodermatitis. 94
Other Antioxidants
As research in the field of cosmeceuticals continues to grow, more emphasis is being placed on naturally occurring antioxidants. 95 Much of the interest in these antioxidants has primarily been in exploring their photoprotective properties. Gingko biloba, for example, once explored for its photoprotective effects, has demonstrated effectiveness in experimental models of radiodermatitis.62,96,97 Many other antioxidants coming from the cosmeceutical industry and other resources are being explored for their prevention of various radiotherapy-induced side effects. The usage of antioxidants during cancer therapy, however, still remains controversial.
Discussion
Though some antioxidants appear promising in the prevention of radiation-induced skin toxicity, longitudinal studies assessing their effect on the malignancies being treated are essential. 98 Though antioxidants appear to have a chemopreventive effect in the development of cancer, 99 antioxidants may interfere with tumor apoptosis following therapy on an already existing cancer.100,101 Studies assessing the comparative risk of tumor recurrence with antioxidants have been inconclusive. 98 These studies were, however, conducted on patients who were given systemic antioxidants as a part of their cancer therapy and would not necessarily translate well to topical therapy given following radiotherapy. Thus, topical antioxidants causing interference with cancer therapy has not yet been demonstrated, though it remains a theoretical concern.
The formation of ROS is a rapid process that can immediately cause apoptosis and cell death within the treated tumor. Systemically delivered antioxidants could disrupt radiation treatment therapy by preventing the formation of ROS within the tumor. 98 Topical antioxidant therapies, given after radiation treatment has been administered, could then avoid interfering with tumor apoptosis. Additionally, the topical application of antioxidants allows for concentrated therapy to the skin, minimizing systemic levels. Topical antioxidant therapy would likely not, however, be appropriate in the case of primary cutaneous malignancies treated with radiotherapy.
As more becomes known about each type of antioxidant and its interaction with different primary tumors, preventing and treating radiation-induced skin toxicity may become more standardized and incorporated into different treatment protocols. Nevertheless, though there remains much uncertainty as to the function of certain antioxidants and their effect on different primary tumor types, many patients will choose to use these alternative therapies on their own to reduce the side effects of radiotherapy. 17 Thus, a clinician’s understanding of the role of antioxidants in the different physiologic pathways of radiation-induced skin injury is essential to properly advising his or her patient.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.