
Abstract
Resistance exercise has great potential to aid in the management of breast cancer–related lymphedema (BCRL), but little is known regarding the acute response of performing resistance exercises with the affected limb. Purpose. To examine the acute impact of upper body resistance exercise on the amount of swelling and severity of symptoms in women with BCRL and to compare these effects between resistance exercise involving high and low loads (heavier vs lighter weights). Methods. Seventeen women aged 61 ± 9 years with mild to severe BCRL participated in this study. Participants completed a high load (6-8 repetition maximum) and low load (15-20 repetition maximum) exercise session consisting of 2 sets of 5 upper body resistance exercises in a randomized order separated by a 10- to 12-day wash-out period. The extent of swelling was assessed using bioimpedance spectroscopy, dual-energy x-ray absorptiometry, and arm circumference measurements. The severity symptoms were assessed using the visual analogue scale (pain, heaviness, and tightness) and a modified Brief Pain Inventory. Measurements were taken pre-exercise, immediately post-exercise, 24 hours post-exercise, and 72 hours post-exercise. Results. No changes in the extent of swelling or the severity of symptoms were observed between pre-exercise and immediately post-exercise, 24 hours post-exercise, or 72 hours post-exercise. No differences in the response to the high or low load exercise were observed. Conclusions. Upper body resistance exercise does not acutely increase swelling or feelings of discomfort/pain, heaviness tightness in the affected limb of BCRL patients when performed at either high or low loads.
Introduction
Breast cancer–related lymphedema (BCRL) is the chronic swelling of the hand, arm, shoulder, and/or breast that occurs after treatment for breast cancer and is estimated to affect at least 20% of breast cancer survivors.1,2 Although the complex pathophysiology of BCRL remains unexplained, axillary lymph node removal and radiotherapy are considered the primary initiating factors.1,3 Damage to the lymphatic system in turn results in edema, chronic inflammation, and accumulation of tissue protein in the affected limb.1,3 BCRL has a significant impact on quality of life.4,5 Significant physical function impairment has been reported in both gross and fine motor tasks,1,6 as well as increased feelings of discomfort, pain, heaviness, and aching. 7 Additionally, women with BCRL exhibit significantly increased psychosocial morbidity, including depression, anxiety, and distress as well as displaying maladjustment to illness.8,9 These factors permeate all aspects of life, affecting work, home, and recreational activities as well as social relationships.4,10
Traditionally, clinical guidelines recommend that women with BCRL avoid vigorous, repetitive, or excessive upper body exercise to prevent exacerbation of lymphedema. 11 The conservative advice, aimed at minimizing risk of injury or harm to the involved side, indirectly encourages women to protect their limb, which in turn may lead them to limit their physical activity and in particular, the use of the affected side. However, such limitation of activity is theorized to hinder rehabilitation and in the longer term result in muscle atrophy, increased adiposity, and declining function. 12 There is the potential that such conservative advice is actually counterproductive as a significant factor associated with the decline in functional activity and quality of life in those with BCRL appears to be a considerable loss of muscle strength in the affected limb.13,14 Women with BCRL have significantly lower perceived and clinically measured upper body function and are more likely to report symptoms, such as pain, numbness, and stiffness, when compared with those without BCRL.13,14
The overwhelming consensus throughout the literature indicates that exercise is very beneficial for cancer patients, resulting in clinically meaningful improvements in quality of life, physical function, and structure as well as mental health.15-17 A growing body of literature provides evidence that these findings extend to patients with BCRL. A consistent finding of this research is that exercise, including exercise specifically involving the affected limb, does not appear to initiate or exacerbate BCRL.1,11,18-24 The risk of developing BCRL has been observed to be lower for patients who engage in regular physical activity compared with those who are sedentary (odds ratio = 1.9; 95% confidence interval = 0.5-2.9). 1 Furthermore, the incidence of BCRL was observed to be lower in a group of breast cancer survivors involved in regular resistance exercise compared with a usual care control group (11% vs 17%, respectively). 20 The largest randomized controlled trial involving BCRL patients to date reported no difference over 12 months in interlimb volume difference between women involved in resistance exercise and usual care. 21 Furthermore, the resistance exercise intervention had beneficial effects on the incidence of exacerbations, severity of lymphedema symptoms, and muscle strength. 21
Upper body resistance exercise is emerging as a particularly important therapy for survivors with BCRL as it is likely to support improved clearance of lymph through the effect of the muscle pump on venous and lymphatic clearance.25-27 Increases in lean muscle mass, muscle strength, and endurance are also expected—changes that have significant positive effects on physical functional ability.28-31 Furthermore, these changes result in an elevated maximal work capacity, meaning that everyday tasks would require less effort. Importantly, the increased work capacity is theorized to translate into reduced risk for lymphedema incidence and exacerbation from everyday use of the affected arm. 12 The clinical trials conducted to date provide strong evidence that maintaining or increasing strength of the upper body through resistance exercise aids in the management of BCRL.11,12,18-22 Despite this, a paucity of research has examined the acute response of performing resistance exercises with the affected limb of women with BCRL and, most importantly, if exercise response would differ between common prescribed resistance training loads (ie, heavier vs lighter weights). In this study, we examined for the first time the acute (immediately after exercise bout) impact of upper body resistance exercise on the amount of swelling and severity of symptoms in women with BCRL and compared these effects between resistance exercise involving high and low loads (ie, heavier vs lighter weights).
Methods
Participants
Sixty women with BCRL who were referred by oncologists and physiotherapists or who responded to advertisements via a local newspaper in the city of Perth, Western Australia from June through August 2010, were initially screened for participation in the study (Figure 1). Forty-three women were excluded from participation due to declining involvement in the trial (n = 24); not meeting the criteria for clinical diagnosis of lymphedema (n = 7); physician decline (n = 1); and other reasons (n = 11), such as travel constraints. Seventeen women were enrolled to participate in this study. Participants had a histological diagnosis of breast cancer at least 1 year prior to the study, a clinical diagnosis of BCRL, and obtained medical clearance from their physician. Clinical diagnosis of lymphedema was defined as having (a) an impedance ratio of at least 3 standard deviations greater than normative data,32,33 (b) a volume difference between affected and unaffected limbs of 5% or more,33,34 and (c) a difference in circumference between affected and unaffected limbs of 5% or more.21,33,34 Participants were excluded if they had (a) unstable lymphedema, defined as receiving intensive therapy (ie, decongestive therapy or antibiotics for infection) within the previous 3 months, or (b) musculoskeletal, cardiovascular, and/or neurological disorders that could inhibit them from exercising. This protocol was approved by the university’s human research ethics committee, and all participants provided written informed consent.
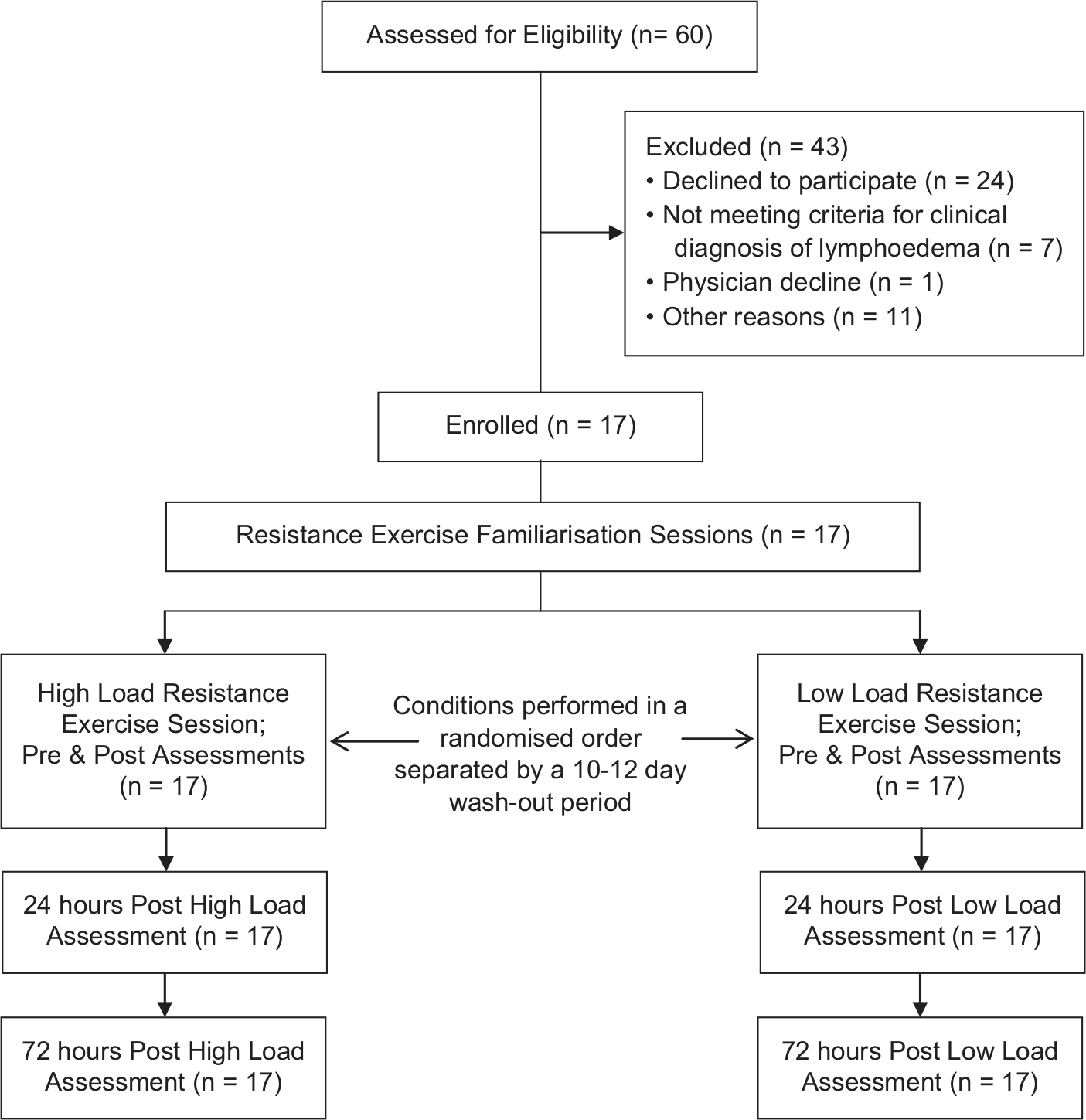
Flow of participants throughout trial.
Sample size calculations were based on change in lymphedema as indicated by volume and circumference (ie, extent of swelling). Whereas a 5% change over time is considered clinically significant, 21 no evidence exists regarding the threshold for a clinically significant acute change in volume or circumference. Therefore, we aimed to detect a medium standardized effect (d = 0.3). With an α level of .05 and a final sample of 17 patients, we achieved 80% statistical power to detect such an effect.
Experimental Design
This study involved a crossover design in which participants completed a high load and low load upper body resistance exercise session separated by a 10- to 12-day wash-out period (Figure 1). Following comprehensive familiarization, participants completed the exercise sessions in a randomized order. Participants were randomized in an allocation ratio of 1:1 using a random assignment computer program. A research methods consultant with no patient contact was responsible for the randomization, and the exercise physiologists involved in supervising and assessing participants were blinded to the allocation sequence. The extent of swelling was assessed using bioimpedance spectroscopy (BIS), dual-energy x-ray absorptiometry (DXA; limb volume), and arm circumference measurements. The severity symptoms were assessed using the visual analogue scale (VAS; pain, heaviness, and tightness) and a modified Brief Pain Inventory (BPI). Measurements were taken on both the affected and non-affected arms pre-exercise, immediately post-exercise, 24 hours post-exercise, and 72 hours post-exercise. Participants were instructed to maintain their usual lymphedema self-care management regimen, physical activity levels, and diet throughout the intervention period.
Exercise Intervention
Prior to completing experimental sessions, all participants completed a series of 4 familiarization sessions over a 2-week period. The familiarization sessions involved 1 to 2 sets of 6 to 20 repetitions of 5 upper body resistance exercises. The resistance exercises—chest press, lateral pull-down, biceps curl, triceps extension, and lateral raise—focused on the major muscle groups in the upper body. Symptom response was monitored using VAS for pain, heaviness, and tightness before and after each session. 35 Load was prescribed and progressed individually. Both the high load and low load experimental exercise sessions involved moderate- to high-intensity resistance exercise. Participants were required to complete 2 sets of the 5 upper body resistance exercises. The high load session involved lifting as much weight as possible for 6 to 8 repetitions (ie, 6-8 repetition maximum [RM]), whereas the low load session involved lifting as much weight as possible for 15 to 20 repetitions (ie, 15-20 RM) of each exercise. 31 Similar to previous research, participants choose whether or not they wore a compression garment during the exercise sessions, 22 and this choice was held consistent across both high and low load conditions. All sessions were performed in an exercise clinic in individual sessions supervised by an exercise physiologist.
Outcome Measures
The extent of swelling and the severity of symptoms were assessed pre-exercise, immediately post-exercise, 24 hours post-exercise, and 72 hours post-exercise for both the high load and low load conditions. The length of time that participants wore their compression garment prior to each assessment was recorded for all participants and held consistent for each individual across all the time points examined. Participants were asked to report any deviations from their standard lymphedema self-care management regimen, physical activity levels, and diet at all assessment time points.
Extent of swelling
The severity of swelling associated with BCRL was assessed using standard objective measures: (a) BIS, (b) DXA, and (c) arm circumference measurements. These 3 methods were used as there is no gold standard for the assessment of lymphedema and the method used to quantify the extent of swelling may influence the results.33,36-38 Impedance of the extracellular fluid in the affected and non-affected arms was assessed and compared using a range of frequencies according to guidelines of the BIS device manufacturer (ImpediMed IMPTM DF50; ImpediMed, San Diego, CA). 32 The impedance values of the affected and unaffected arms were compared and the ratio reported (L-Dex score). DXA (Hologic Discovery A, Waltham, MA) was used to assess tissue composition of the limbs using a 3-compartment model sensitive to changes in fluid retention.39,40 Measurements were converted into volume using known densities of adipose tissue (0.9167 g/mL ≈ 0.92 g/cm3), lean tissue (1.0615 g/mL ≈ 1.06 g/cm3), and bone (3.15 g/cm3), a method shown to correlate very highly (r = .996, P < .0001) with total arm volume measurement by plethysmography. 41 Absolute values of the total volume for the affected arm as well as the volume difference between the affected and non-affected arms were reported. A constant tension tape was used to assess regional circumferences of the affected and non-affected arms. Measurements were started just distal to the metacarpal-phalangeal joints and were taken at 4-cm intervals up the arm until the base of the axilla. 42 Participants were seated with their arm positioned at 90° abduction resting on a massage table while arm circumference was assessed. 33 Absolute values of the sum of all circumference measurements for the affected arm as well as the difference in the sum of all circumference measurements between the affected and the non-affected arms were reported. Circumference measurements at the point of greatest difference between the limbs was also assessed but not reported as the trends were consistent with the sum of circumference measurements.
Symptom severity
The severity of BCRL symptoms was assessed using: (a) VAS for pain, heaviness, and tightness and (b) the BPI questionnaire. VAS were used to quantify the severity of perceived pain, heaviness, and tightness in both the affected and non-affected arms. 35 Participants rated their symptom severity from no pain/no discomfort (VAS score = 0) to very severe pain/worst imaginable discomfort (VAS score = 10). The BPI assessed any feelings of pain, the area of pain, the sensation (ie, discomfort, heaviness, aching, throbbing, etc.), and the extent to which the symptoms interfered with aspects of daily life over the previous 24 hours. 43 The BPI was modified so that each item was assessed with respect to the affected and non-affected limbs separately.21,42
Tolerance of the exercise sessions
Session rating of perceived exertion was recorded immediately after the completion of each exercise session. Participants were asked to rate the overall difficulty of the session (ie, how hard/how much exertion was involved) on a scale of 6 (no exertion at all) to 20 (maximal exertion). A 7-point Likert-type scale was also administered after the completion of each exercise session to assess the perception of tolerance of the exercise session (1 = intolerable, 7 = very tolerable).
Statistical Analyses
Data were analyzed using SPSS Statistics for Windows, Version 19.0 (IBM SPSS, Chicago, IL). Analyses included standard descriptive statistics, paired sample t tests, and repeated measures analysis of variance. All tests were 2-tailed with statistical significance set at an α level of .05. Results are presented as mean ± standard deviation or number of participants (percentage of participants) for frequency data.
Results
Participants
All participants enrolled completed the study. Participants had been diagnosed with lymphedema an average of 5.4 years prior to involvement in this study (Table 1). Approximately 47% of the participants were diagnosed within the previous 3 years. All participants had surgical treatment (100%), with an average of 13 lymph nodes removed during the procedure. The majority of participants had received radiotherapy previously (88%), 65% had previous chemotherapy, and 47% previous/current hormone therapy. Participants were generally overweight or obese (percentage fat = 39.2 ± 5.6; body mass index = 31.5 ± 5.6 kg/m2). According to common toxicity criteria grading, 34 30%, 35%, and 35% of participants had mild, moderate, and severe lymphedema, respectively. Approximately 18% of participants (3 of 17) chose to wear their compression garment during the resistance exercise sessions. No deviations in standard lymphedema self-care management, physical activity, and diet behaviors were reported throughout the study.
Baseline Characteristics of Participants. a

Results are presented as mean ± standard deviation (SD) or number of participants (percentage of participants).
Comorbidity classified as cardiovascular disease, hypertension, diabetes, osteoporosis, and dyslipidemia.
At the point of greatest difference between limbs.
Extent of Swelling
No significant differences were observed in volume or circumference of the affected arm across most of the time points examined (ie, pre-exercise, immediately post-exercise, 24 hours post-exercise, and 72 hours post-exercise; Table 2). Arm circumference at 72 hours post-high load exercise was significantly lower that pre-exercise. When comparing the affected and non-affected arms, no significant differences were observed in the BIS ratio, arm volume difference, and arm circumference difference across any of the time points examined (Table 2). No significant changes were observed from pre-exercise to immediately post-exercise, 24 hours post-exercise, and 72 hours post-exercise in the BIS ratio, arm volume, or arm circumference (Figure 2A-C). No significant differences were observed between the high load and low load exercise conditions across all of the time points examined (Table 2 and Figure 2A-C). There were no clear trends in terms of the impact of the resistance exercise on the extent of swelling, with individual responses varying from no change to decreased and/or increased swelling (Figure 3).
Extent of Swelling and Severity of Symptoms Throughout All Conditions. a

Visual analogue scale (VAS) and Brief Pain Inventory (BPI) scores are from the affected arm. No post-exercise measure for BPI—Interference (it assesses interference with activities of daily living in the past 24 hours).
Significantly different from pre-exercise.
Significantly different from post-exercise.

Change in the extent of swelling (A-C) and severity of symptoms (D-F) from pre-exercise to immediately post-exercise, 24 hours post-exercise, and 72 hours post-exercise for both high and low load conditions.

Individual response in the extent of swelling from pre-exercise to immediately post-exercise, 24 hours post-exercise and 72 hours post-exercise for both high (A-C) and low (D-F) load conditions.
Symptom Severity
Visual analogue scale and BPI results were reported for the affected arm only, as the difference in symptom severity between the affected and non-affected arms did not change throughout all time points assessed (ie, affected arm scores were consistently significantly higher than the non-affected arm scores across all time points for both exercise conditions). No significant differences in the severity of pain, heaviness, or tightness were observed across all time points examined (Table 2). Furthermore, no significant differences in extent to which the symptoms interfered with aspects of daily life were reported across most time points examined (Table 2). The interference score of the BPI was significantly lower than pre-exercise at 24 hours post-exercise, and 72 hours post–low load exercise (Table 2). No significant changes were observed from pre-exercise to immediately post-exercise, 24 hours post-exercise, and 72 hours post-exercise in the severity of pain, heaviness, or tightness (Figures 2D-F). No significant differences were observed between the high load and low load exercise conditions across all of the time points examined (Table 2, Figure 2D-F). No clear trends existed in the symptom response to the exercise conditions as individual responses varied from no change to decreased and/or increased severity of pain, heaviness, and tightness following the exercise sessions (Figure 4).
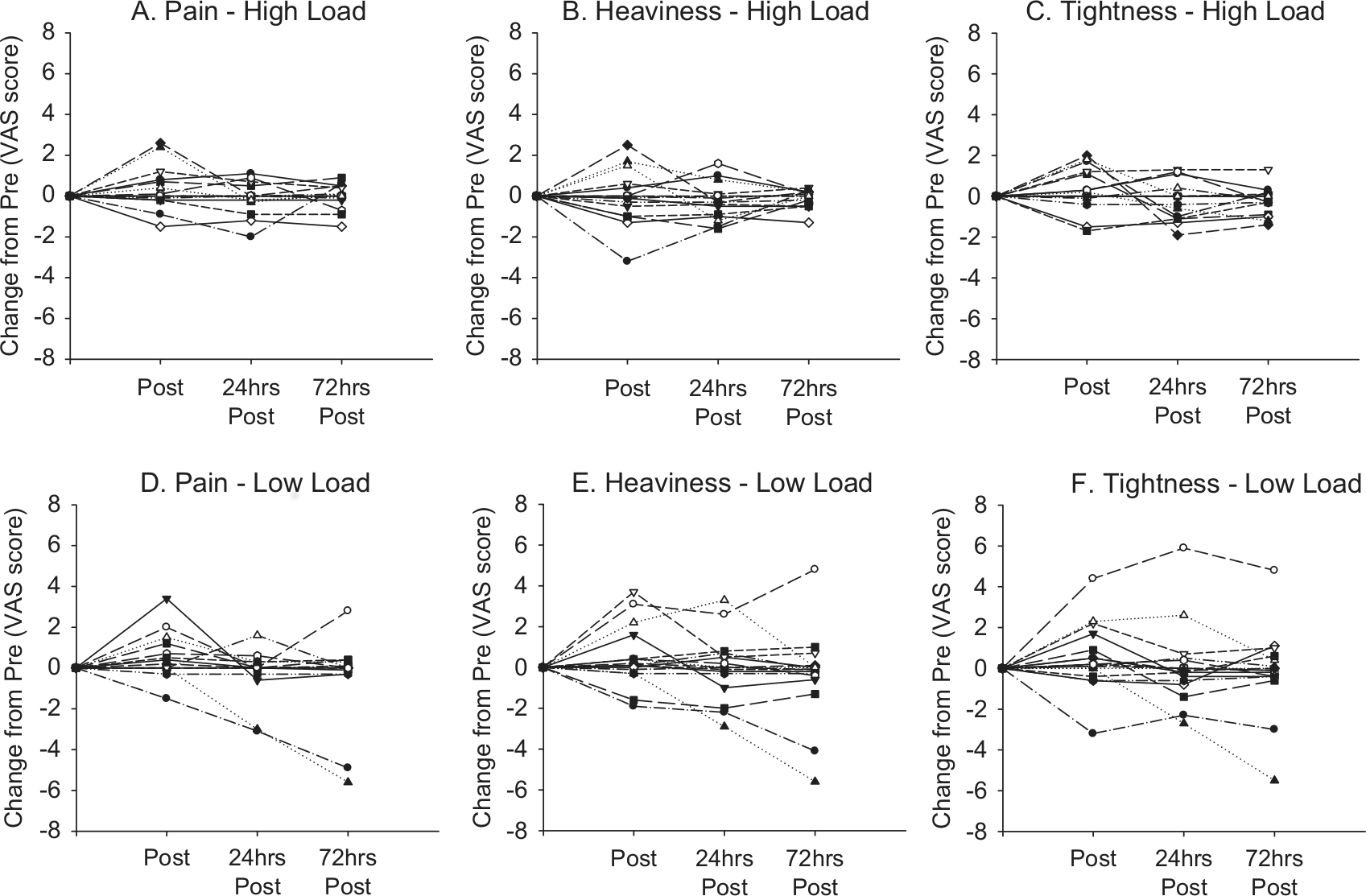
Individual response in the severity of symptoms from pre-exercise to immediately post-exercise, 24 hours post-exercise, and 72 hours post-exercise for both high (A-C) and low (D-F) load conditions.
Tolerance of the Exercise Sessions
Compliance was high with all participants completing all required exercise and assessment sessions (100% compliance). No adverse events were recorded. The moderate- to high-intensity resistance exercise resulted in a rating of perceived exertion of approximately 12.5 ± 1.3, which is equivalent to a rating of “somewhat hard” (high load =12.6 ± 1.3; low load =12.3 ± 1.2). The exercise sessions were well tolerated with an average tolerance score of 6.7 ± 0.6 out of a possible 7 (high load = 6.8 ± 0.4; low load =6.7 ± 0.6). No differences in the rating of perceived exertion or tolerance existed between the high and low load resistance exercise sessions. The weight lifted differed significantly between the high load and low load conditions (high load =33.3 ± 4.7 kg; low load =21.5 ± 3.1 kg; P = .000).
Discussion
The primary findings of this small, exploratory study includes the following: (a) upper body resistance exercise performed in a controlled setting (ie, correct instruction and highly supervised) did not acutely increase the extent of swelling or the severity of symptoms in women with BCRL; (b) there was no difference in the acute response to upper body resistance exercise involving either high loads (6-8 RM) or low loads (15-20 RM); and (c) the moderate- to high-intensity upper body resistance exercise sessions involving high (6-8 RM) and low (15-20 RM) loads were well tolerated by women with BCRL.
Despite the common advice for women with BCRL to avoid lifting with their affected limb to prevent an exacerbation, the upper body resistance exercise performed in a controlled setting during this study did not acutely increase the extent of swelling or the severity of lymphedema symptoms. This is the first investigation to examine the impact of moderate- to high-intensity upper body resistance exercise on the affected limb of women with BCRL immediately after and in the days following an exercise session. The methodologies involved with the assessment of swelling were among the most comprehensive used to date, 33 with changes in extracellular fluid, arm volume, and arm circumference measured both in absolute terms as well as the difference between affected and non-affected arms. The lack of significant change in any of these measures, coupled with the observation that pain, heaviness, tightness, and the degree to which BCRL symptoms interfered with aspects of daily life did not worsen following the exercise suggests that appropriately prescribed and supervised resistance exercise is safe for women with BCRL. These findings support previous research examining the acute impact of low intensity resistance exercises targeting arm muscles in patients with mild to moderate BCRL. 44 Furthermore, the current findings add to an emerging body of evidence indicating that regular upper body resistance exercise is safe and does not cause exacerbations in women with BCRL.19-23
The current results provide initial evidence indicating that the load (high 6-8 RM or low 15-20 RM) used during upper body resistance exercise performed in a controlled setting did not affect the acute response in swelling or symptom severity in this sample of women with BCRL. It is well established that both high (generally ≥80% of 1 RM) and low (generally ≤60% 1 RM) load resistance exercise are effective at eliciting physiological adaptations that translate into improved muscle size, strength, and physical function (provided the intensity of the resistance exercise is moderate-high).28,30,31,45,46 However, a strong dose-response relationship exists between the load of resistance training and the magnitude of muscle size and strength gains.30,31,46,47 For example, a meta-analysis of 140 trials indicates maximal gains in strength are observed with high load resistance exercise (80% of 1 RM effect size = 1.80 ± 1.30) compared with lower loads (eg, 70% of 1 RM effect size = 0.70 ± 0.65). 46 Importantly, a strong dose-response relationship exists between strength gains and improvements in physical function following resistance training, 30 and high load resistance exercise has also been reported to result in significantly greater improvements in health-related quality of life when compared with low load resistance exercise. 48 Despite the evidence for superior efficacy of high load resistance exercise, clinical experience indicates that women with BCRL are very apprehensive about using heavier weights, and allied health professionals who advise patients to exercise typically stipulate low intensity exercise using very light loads. 44 Results from the current study indicate that there was no difference in the acute response in swelling or symptom severity between high and low loads. Although continued study is required to determine the long-term effect, this initial evidence indicates that an appropriately designed and supervised upper body resistance exercise program involving the prescription of high loads was safe for women with BCRL and may lead to superior long-term improvements in physical structure and function.
Moderate- to high-intensity upper body resistance exercise was well tolerated by women with BCRL. Additionally, there was no difference in the perceived difficulty or tolerability of the resistance exercise sessions involving either the low or high loads. This is an important outcome to highlight, given the apprehension commonly experience by women with BCRL to participate in an exercise program involving upper body resistance exercise and the distribution of patients with mild, moderate, and severe lymphedema within this study. There is theoretical rationale 12 and evidence19-23 that resistance exercise is an effective adjunct therapy for the management of BCRL. Our current study extends these findings indicating that both low and high loads are well tolerated by this patient population when appropriately prescribed and supervised.
There are limitations associated with this investigation worthy of comment. Although the sample size provided adequate power to detect a medium standardized effect (d = 0.3), the relatively small number of participants limited the ability to detect changes of a small standardized effect (d = 0.1-0.29). It is unclear what magnitude of effect is clinically significant when examining acute changes in lymphedema severity, so the results should be interpreted with caution. Due to the fact that assessments were taken up to 72 hours after the exercise sessions, the results at both 24 hours post-exercise and 72 hours post-exercise may have been confounded by the other activities participants were involved in after the exercise bout (eg, mopping, gardening, etc.). However, participants were instructed to maintain normal daily activities throughout the duration of the study. Although every effort was made to ensure consistency in the length of time, participants wore their compression garment prior to each assessment point; self-report may have differed from actual behavior. The relatively small sample size prevents any subgroup analysis required to examine if the response to the exercise bouts differed according to lymphedema severity. However, this was the first exploratory study examining different exercise loads, and we employed a comprehensive battery of measures to assess lymphedema swelling and symptom severity including BIS, DXA, arm circumference, VAS (pain, heaviness, and tightness), and the BPI questionnaire. Finally, our subjects were well-functioning individuals who were mostly motivated to undertake the exercise study, and they may not be representative of all women with BCRL.
Conclusions
This exploratory, acute study suggests that when appropriately prescribed and supervised, women with BCRL can perform moderate- to high-intensity upper body resistance exercise with both low and high loads without fear of exacerbating their lymphedema. Furthermore, this type of exercise was well tolerated by a sample of women with BCRL, and we report no adverse events. These initial findings have important clinical significance, given the clear potential for resistance exercise to aid in the long-term management of BCRL through enhanced muscular strength and endurance as well as improved functional ability. Prospective trials examining the chronic response of upper body resistance exercise using low and high loads are warranted.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funding from Edith Cowan University. Prue Cormie is supported by the Cancer Council Western Australia Postdoctoral Research Fellowship.