
Abstract
The development of nontoxic agents that can selectively enhance the cytotoxicity of chemotherapy is an important aim in oncology. This study evaluates the ability of infrasound exposure to sensitize glioblastoma cells to cisplatin-induced apoptosis. The infrasound was delivered using a device designed to replicate the unique infrasound emissions measured during external Qigong treatments. Human glioblastoma cell lines harboring wild-type p53 (U87) or mutant p53 (U251, SF210, and SF188) were treated in culture with cisplatin, infrasound emissions, or the combination of the 2 agents. Induction of apoptosis was quantified after 24 hours by flow cytometry following annexin V/propidium iodide staining. Infrasound emissions alone, delivered at moderate levels (~10 mPa) with dynamic frequency content (7-13 Hz), did not induce apoptosis, yet combining infrasound with cisplatin augmented the induction of apoptosis by cisplatin in all the 4 cell lines (P < .05). Increased cellular uptake of the fluorophore calcein associated with infrasound exposure was quantified by fluorescence microscopy as well as flow cytometry, demonstrating increased cell membrane permeability. The 4 cell lines differed in the degree to which infrasound exposure increased calcein uptake, and these differences were predictive of the extent to which infrasound enhanced cisplatin-induced apoptosis. When exposed to specific frequencies, membrane permeabilization also appeared to be differentially responsive for each cell line, suggesting the potential for selective targeting of tissue types using isolated infrasonic frequencies. Additionally, the pressure amplitudes used in this study were several orders of magnitude less than those used in similar studies involving ultrasound and shock waves. The results of this study provide support for using infrasound to enhance the chemotherapeutic effects of cisplatin in a clinical setting.
Introduction
The development of nontoxic chemosensitizers is especially urgent in the case of malignant gliomas, which are generally treated with postoperative radiotherapy in combination with 1 or more chemotherapies. 1 Gliomas are the most common intracranial tumors, comprising about 60% of all primary central nervous system tumors. The most malignant form, glioblastoma, is also the most common, representing approximately half of gliomas diagnosed. 2 Despite aggressive therapies, recurrence of glioblastoma within a year is not uncommon. An important factor contributing to this dismal prognosis is the expression of multiple anti-apoptotic signals by glioblastoma cells, often including deficient p53 function. 3 The tumor-suppressor protein p53 accumulates when DNA is damaged, and wild-type p53 will induce apoptosis if damage is extensive and repair efforts fail. DNA damage from anticancer agents is often repaired by endogenous preventative pathways, such as base excision repair, resulting in decreased chemotherapeutic efficacy. Thus, the pharmacological inhibition of DNA damage repair pathways is one strategy for enhancing the cytotoxicity of chemotherapy. 4 Other strategies include inhibition of cellular anti-apoptotic factors 5 and enhancement of drug transport into cells.
Chemosensitization by enhanced drug transport has been achieved by both chemical methods, such as delivery via cationic lipids, 6 as well as methods to increase cell membrane permeability, such as electroporation, 7 shock wave exposure, 8 and ultrasound application (inaudible acoustical energy above 20 kHz).9,10 Ultrasound in particular has been found to be effective as an agent to temporarily permeabilize the cell membrane, thus allowing for increased transport of drugs and other therapeutic compounds from the extracellular environment into the cell. This increased uptake has been largely attributed to the formation of transient pores in the cell membrane because of microbubble oscillations near the cell membrane, 11 that is, so-called sonoporation 12 ; however, the permeabilizing effects are not completely understood. 13 Numerous studies have demonstrated the chemosensitizing potential of ultrasound. Ultrasound sensitizes HeLa cells to the chemotherapeutic agent camptothecin, for example, resulting in a reduction in the median lethal dose from 58 to 18 nM. 14 Likewise, Yu et al reported that exposure to ultrasound appeared to lower thresholds for apoptosis in chemoresistant ovarian cancer cells. 15 Iwanaga et al investigated the ability of ultrasound to chemosensitize the human gingival squamous carcinoma cell line, Ca9-22, to bleomycin. They found that the delivery of bleomycin was enhanced by ultrasound exposure in vitro and that the combination treatment was significantly more effective than drug alone against Ca9-22 tumors implanted in nude mice in vivo. 16 Studies with Chinese hamster ovary cells showed ultrasound to markedly enhance the cytotoxicity of Adriamycin but not of cisplatin and etoposide. 17 Similarly, tone-burst ultrasound was shown to increase the cytotoxicity of Adriamycin but not cisplatin in Chinese hamster ovary cells. 18 In contrast, cisplatin cytotoxicity in HeLa cells was found to be augmented by ultrasound. 19 Additional investigations of the chemosensitizing effects of ultrasound exist and are also seemingly on the rise as this technology gains more attention.
Though not as extensive as the research on ultrasound, there is support for the efficacy of shock waves in augmenting drug delivery. A study evaluating high-energy shock waves demonstrated that treatment in conjunction with paclitaxel was significantly more effective against rat breast cancer cells in vitro and in vivo than treatment with paclitaxel alone. 20 Another study demonstrated marginal yet measurable synergistic effects of bleomycin and shock waves on human colon cancer tumors implanted in nude mice: cell proliferation decreased and apoptosis increased with combined treatments relative to control conditions and either treatment type alone. 21 Using just single shock waves, Kodama et al delivered molecules of fluorescently labeled dextran with mean molecular weights of up to 2 000 000 (12 345 glucose units) to human ovarian cancer cells, 8 thus demonstrating the potential for transport of relatively large molecular complexes using this technique.
Given the usefulness of ultrasound and shock waves as a sensitizer, we were interested in evaluating the potential of sound waves in the infrasonic range (inaudible acoustical energy below 20 Hz) to be similarly efficacious. This interest was triggered by anecdotal reports that cancer patients were using an infrasound generator as a complement to chemotherapy regimens. The infrasound generator was designed to replicate the infrasonic emissions measured during external Qigong treatments. 22 The potential for infrasound to enhance cellular drug delivery is supported by a small number of studies indicating that exposure can influence cell membrane permeability. Svidovyi and colleagues, for example, studied the effects of infrasound on human erythrocytes in vitro as well as the organs of rats in vivo and reported increased membrane permeability.23,24 Interestingly, studies of rabbit ocular tissue revealed that increased tissue permeability induced by infrasound is associated with elevated concentrations of hyaluronidase and a temporary reduction in the viscosity of hyaluronic acid. 25 This is of particular relevance for cancer treatment since elevated levels of hyaluronic acid are found in many types of human cancers and manipulations of hyaluronic acid expression or interactions have been shown to influence tumor progression. 26 Our group reported preliminary findings indicating that infrasonic emissions can sensitize human glioblastoma cells to the chemotherapeutic agent 5-fluorouracil. 27 Here, we extend these findings by evaluating the potential for infrasonic emissions to sensitize glioblastoma cells to cisplatin.
Cisplatin is a DNA-damaging chemotherapeutic drug that may have a role in the adjuvant chemotherapy of several solid tumors, including glioblastoma.28,29 Since one of the major modes of action of cisplatin and other chemotherapeutic drugs may be via the activation of apoptosis,15,30 we measured induction of apoptosis in cultures exposed to 3 experimental conditions: infrasound exposure alone, cisplatin alone, or the combination of infrasound and cisplatin.
Materials and Methods
Cell Culture
We evaluated 4 established and widely studied glioblastoma cell lines to capture a range of responsiveness that recapitulates the genetic heterogeneity inherent in this disease. Three harbor mutations in the tumor suppressor gene p53 (U251, SF210, and SF188), which renders cells generally more resistant to chemotherapeutic agents, whereas one harbors wild-type p53 (U-87 MG). The U87 and U251 lines were obtained from the American Type Culture Collection (ATCC, Manassas, VA), and SF210 and SF188 were obtained from the Brain Tumor Research Center at the University of California at San Francisco. Cell lines were maintained as exponentially growing monolayer cultures in RPMI-1640 media, supplemented with 10% fetal bovine serum, and 1% antibiotics/antimycotics in a humidified incubator at 37°C and 5% CO2. Prior to the start of each experiment, approximately 80 000 cells/well were plated onto untreated BD Falcon 6-well cell culture plates (BD Biosciences, Bedford, MA) with 3 mL of media in each well and allowed to adhere and grow overnight to 80% to 90% confluence.
Infrasound Delivery
A commercially available infrasound generator (Infratonic QGM 4.0; China Healthways Institute, San Clemente, CA) was used to deliver dynamic frequency infrasound to cells inside an environmental chamber. The infrasound generator is listed with the US Food and Drug Administration as a 501(k) therapeutic massager and is designed to emit infrasound at varying frequencies. Another generator was designed and developed in our laboratory consisting of a function generator (4011A; BK Precision, Yorba Linda, CA) and power amplifier (VM100; Velleman, Gavere, Belgium) to investigate the potential effects of single-frequency infrasound in a subset of the experiments in this study. Samples not receiving infrasound exposure were incubated in the same environmental chamber to ensure identical handling except for infrasound exposure. The environmental chamber maintained the cells at 37°C and 5% CO2 during the infrasound treatments after which the cells were returned to an incubator until subsequent processing was required.
Infrasound was delivered during initial incubation with cisplatin or calcein, depending on experiment type, with the infrasonic transducer mounted inside an environmental chamber approximately 3 cm from the target cells. This was the closest, practical distance that prevented any mechanical coupling although effects were detected at distances as great as 10 cm. The exposure protocol was determined through preliminary experiments that measured reliable chemosensitizing effects of infrasound with exposures as brief as 30 minutes, marginal increased effectiveness between 1 and 2 hours, and negligible differences between 2 and 4 hours of exposure (data not shown). Unlike the design of most published studies of ultrasound and shock waves that evaluate direct transduction via solid or liquid, our experimental design evaluated indirect conduction where infrasound transmissions first traveled through air, then a thin layer of plastic, followed by another layer of air, and then the liquid media before reaching the target cells (see Figure 1). Indirect conduction more closely models the application of external qigong from which the infrasonic generator is based on and is also a much easier method to employ in an experimental as well as clinical setting.

Schematic diagram of experimental set up.
Infrasound Measurement
Prior to the setup, a spatial dispersion analysis was performed by sampling the output at various radial displacements about the transducer head to ensure that a uniform distribution of energy was being applied to the cell culture wells. A measurement apparatus was constructed to characterize infrasonic emissions and ensure that a uniform and consistent application of infrasound was delivered to target cells. The system consisted of a high fidelity microphone (AT2020; Audio Technica, Tokyo, Japan) using a Phantom power supply and MP3 amplifier (Rolls, Salt Lake City, UT) for sound transduction and amplification and an analog to digital converter (PicoScope ADC212/3; Pico Technologies, Cambridgeshire, England) to convert to digital data. An independent, certified measurement system consisting of a high-sensitivity Model 2570 microphone, dual-channel 2200C power supply, and ultra low noise PRM900C preamp (Larson Davis, Depew, NY) enabled validation of the primary measurement system. Time series and spectral analysis were performed with programs developed in MATLAB using Signal Processing and Statistical Toolkits (Mathworks, Natick, MA).
Assessment of Cisplatin-Induced Apoptosis
Cells were exposed to cisplatin (cis-Platinum(II) diamine dichloride; Sigma Chemical, St Louis, MO) dissolved in ethanol at indicated concentrations for 4 hours with and without exposure to infrasound during the drug treatment. Apoptosis was measurable up to 96 hours after treatments in pilot studies (data not shown). The 24-hour time point was determined to be optimal for measuring changes in apoptosis across all 4 cell lines and was therefore used for the experiments reported here. After treatment, adherent cells were collected by trypsinization, pooled with nonadherent cells, washed with RPMI-1640 media, and subsequently stained with annexin V-FITC (fluorescein isothiocyanate) and propidium iodide (PI) using an apoptosis detection kit (Medical & Biological Laboratories, Woburn, MA). The cells were then centrifuged, resuspended in 200 µL of phosphate buffered saline, and analyzed by flow cytometry using a fluorescence-activated cell analyzer with CellQuest software (BD Immunocytometry Systems, San Jose, CA). Sample runs consisted of 10 000 cells excited with a 488 nm argon laser and gated on appropriate forward-scatter and side-scatter criteria to filter out cell fragments and other detritus. Annexin V and PI signals were collected through 530/30 nm and 585/42 nm band pass filters, respectively, using log settings. Compensation was performed to remove bleed over into the 585 nm channel. Partitions were established that separated the cell events into quadrants according to staining with annexin V and/or PI. Average increases in apoptosis relative to vehicle-treated controls were calculated for combined effects, |Ap(Cis + IS)|, and for the individual effects of cisplatin and infrasound alone, |ApCis| and |ApIS|, respectively. A paired t test was performed between the combined effects and the sum of the individual effects to determine significance. Additionally, apoptosis augmentation through chemosensitization was quantified by the ratio: (|Ap(Cis + IS)| − |ApCis|)/|ApCis|, yielding a relative increase compared with cisplatin alone.
Calcein Measurement
Fluorescence microscopy was used to monitor increased uptake of the relatively impermeable molecule calcein (C481; Molecular Probes, Eugene, OR) following previously published methods.8,31,32 Four independent wells in each of the 2 culture plates were seeded with 80 000 cells/well in phenol-red-free RPMI-1640 media, and calcein (100 µM) was added to each well immediately prior to treatment. Both were maintained at routine incubation settings and optimum humidity inside the aforementioned environmental chamber enclosing an Axiovert 200M microscope (Carl Zeiss, Gottingen, Germany). One culture plate received infrasound, whereas the other was acoustically isolated on the other side of the environmental chamber. After 2 hours of treatment the cells were washed twice with media before images (both phase contrast and fluorescent) were obtained using Volocity Acquisition software (Improvision, Lexington, MA). The images were acquired at a magnification of 10× using a high resolution digital camera (ORCA C4742-80-12AG; Hamamatsu, Hamamatsu City, Japan). Each well yielded a total of 4 areas consisting of 9 adjacent fields (3 × 3) from each of the 2 plates. Approximately 50 cells were in each field (measuring 840 by 640 µm) providing a robust statistical population. Mean fluorescence was calculated as the averaged intensity over all image pixels after background intensity was subtracted and outliers (detritus) removed.
Evaluation of calcein uptake by flow cytometry followed a similar protocol with cells collected after treatment by trypsinization. Flow cytometry was conducted using the same equipment and software described above for apoptosis analysis. The calcein signal was collected in log mode for sample runs of 10 000 gated cells and mean fluorescence was measured for cells treated with infrasound and compared with those not receiving infrasound. Average mean fluorescence for microscopy and cytometry data were calculated relative to background noise for control cells, |FlC|, and for cells treated with infrasound, |FlIS|. A paired t test was performed to determine significance and the normalized increase was calculated by the formula, (|FlIS| − |FlC|)/|FlC|, and used as a comparative statistic.
Results
Infrasound Enhancement of Cisplatin-Induced Apoptosis
We examined a group of 4 human glioblastoma cell lines to assess the ability of infrasound treatment to influence responsiveness to cisplatin. To accommodate the sensitivity of individual cell lines, cisplatin concentrations were varied such that drug treatment alone resulted in less than a 50% decrease in the number of observed viable cells. Results from each experimental condition were compared with those from untreated cultures (control condition). Induction of apoptosis was assessed by flow cytometry based on staining with annexin V in conjunction with PI, allowing cells to be identified as viable, in early apoptosis, or in late apoptosis/necrosis. Figure 2A depicts flow cytometry results from a representative experiment with U87 cells evaluated 24 hours after treatments. Figure 2B plots the percentages of cells undergoing apoptosis following treatments in 4 glioblastoma cell lines, and Table 1 summarizes these data. A paired t test on the apoptosis data for all 4 cell lines determined that the combined effect of cisplatin and infrasound was significantly greater than what would be expected of the additive effects of the individual treatments (P < .05 for 3 cell lines and P < .01 for 1 cell line). This determination holds true despite relatively large standard deviations within treatment conditions due to differences in sensitivities of cultures within each experiment. Thus, cisplatin treatment is rendered more efficacious when combined with infrasound. The average relative increases in the apoptotic fractions observed following combination treatment for U87, U251, SF210, and SF188 cells were 20.5%, 32.5%, 45.2%, and 22.2%, respectively. These values represent the percent increase in the apoptotic fraction of the combination treatment relative to those observed following cisplatin treatment alone, subtracting baseline control conditions, that is, the increase in effectiveness of cisplatin with the addition of infrasound. It should be noted that infrasound alone produced no discernible apoptotic effects compared with control conditions in all 4 cell lines when assessed at 48, 72, and 96 hours (data not shown).
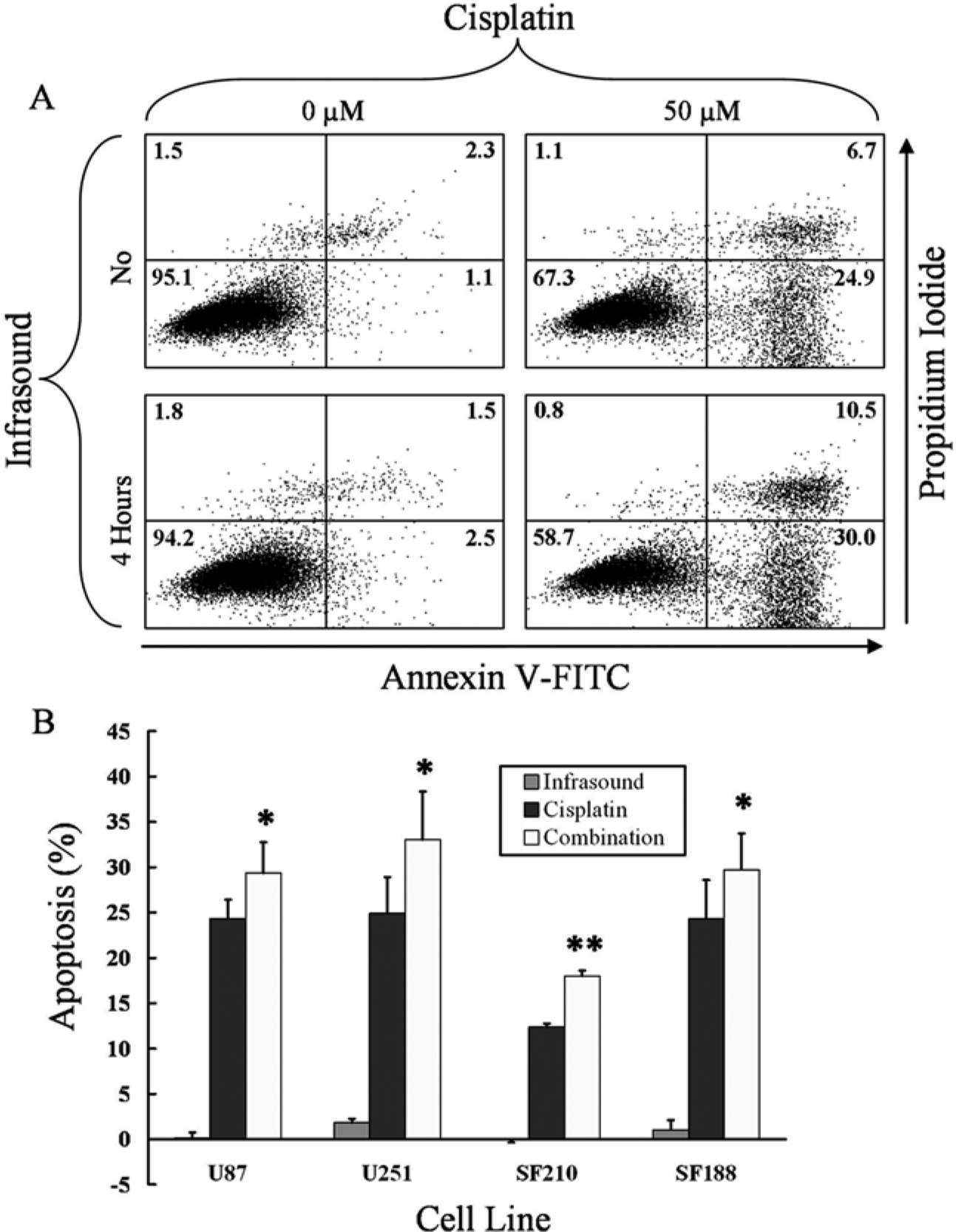
Enhancement of cisplatin-induced apoptosis by infrasound exposure.
Summary Showing Relative Changes of Viable, Early Apoptosis, and Late Apoptosis/Necrosis Quadrant Cell Populations Compared With Control Conditions. a

Specifically, the outcomes from the control conditions were subtracted from the other conditions for all quadrants.
It is interesting to note that the U87 cell line differs from the other 3 cell lines in that it expresses wild-type p53, whereas the others harbor mutations in this tumor suppressor gene. The comparable responses to infrasound treatment among the 4 cell lines indicate that wild-type p53 function is not required for the enhancement of cisplatin-induced apoptosis, possibly implicating the involvement of a sphingolipid-mediated cytolytic pathway. Comparing U87 and U251, the concentration of cisplatin resulting in approximately the same apoptotic response was a factor of 3 times greater for U251 than for U87 (150 µM vs 50 µM), yet infrasound exposure in conjunction with those cisplatin concentrations produced roughly equivalent relative increases in apoptotic response (29.3% and 33.0%).
Increased Cellular Uptake of Calcein by Infrasound
Given the key role of membrane permeability in chemosensitization by ultrasound, we evaluated this parameter in our infrasound model using the cellular uptake of the fluorophore calcein as a surrogate marker for drug uptake. Calcein has a molar mass that is approximately double that of cisplatin and can be introduced into cells via incubation. Increased cellular uptake of calcein following exposure to infrasound was clearly evident by fluorescence microscopy and consistent with the experiments depicted above in Figure 2, and infrasound exposure did not cause any apparent adverse effects as assessed by phase contrast imaging (10×) of morphological characteristics (data not shown). Calculation of mean fluorescence from images containing approximately 8000 SF210 cells from 4 independent runs yielded a significant increase from infrasound compared with control (P < .005). In a separate experiment, we quantified cellular uptake of calcein with and without infrasound exposure using flow cytometry (see Figure 3). A relative increase of 69% in mean calcein fluorescence intensity was observed in cells receiving infrasound (932 vs 550 arbitrary units). Control experiments following the same experimental protocol with the infrasound generator turned off were also performed to ensure that any observed effects resulted from infrasound emissions rather than from other elements of the apparatus or setup. Calcein uptake was analyzed, and no significant differences in mean fluorescence were observed between the infrasound setup and the standard controls. Taken together, these data provide strong support for the notion that the enhanced cisplatin-induced apoptosis observed following infrasound exposure is contributed to by increased cellular uptake of the drug and are thus consistent with findings evaluating chemosensitization with ultrasound and shock waves.

(A-D) Increased cellular uptake of calcein with infrasound. (E) Histogram of fluorescent intensities obtained by flow cytometry of SF210 cells incubated with 100 µM of calcein. One sample received 4 hours of infrasound exposure, whereas the other (control) received none.
Spectral Characterization of Infrasound Generator
The output of the infrasound device at 3 cm was determined to be approximately 75 dB sound pressure level (reference pressure 20 µPa) or equivalently 10 mPa, which is considered moderate. This measurement distance was chosen to be consistent with the spacing of the transducer head to the monolayer of cells in the experimental setup. We characterized the frequency content and manner of distribution of the dynamic frequency infrasound generator. Amplified microphone voltage output was sampled every 341 µs to ensure adequate resolution of frequencies well below the ascertained output spectrum of the generator. A 50-second sample of output was measured and analyzed by Fourier analysis. The subsequent periodogram was smoothed to visualize the average power spectral density (see Figure 4). Frequencies ranged from 6 to 15 Hz with apparent subpeaks around 7.5, 8.5, 10, and 11.6 Hz. Consistent with the manufacturer’s specifications, the output of the infrasound generator is random, and although the output of the spectral analysis varied slightly from trial to trial, the overall characterization is consistent. The dynamic, random component is purported to prevent biological adaptation that could diminish therapeutic applications.
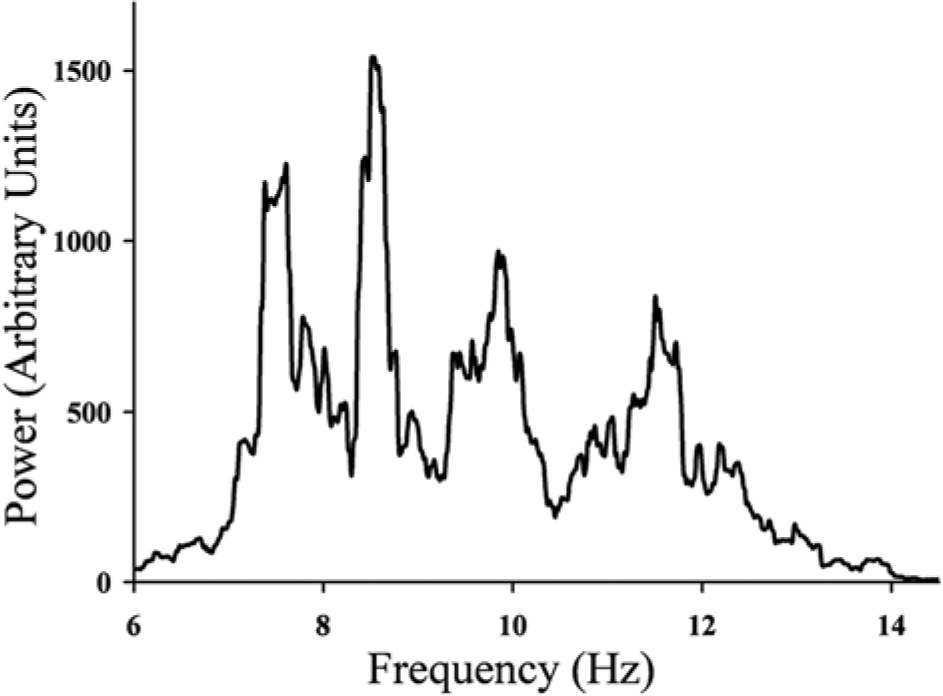
Spectral analysis of infrasound emissions.
Frequency and Cell Line Dependence of Permeabilization by Infrasound
To test whether the dynamic frequency component of the infrasound exposure in our model is required for the observed cell permeabilization effects, a series of calcein uptake experiments was conducted to compare glioblastoma cells exposed to either dynamic frequency infrasound from the commercial device or to a specific, constant frequency of infrasound driven by a generator constructed in our laboratory. Two constant frequencies were chosen from within the range emitted by the dynamic frequency infrasonic generator corresponding to 2 of the subpeaks (8.5 Hz and 11.6 Hz). One constant frequency was chosen just outside the upper bound (15 Hz) to determine if effective subsonic frequencies might exist outside the spectrum of the dynamic frequency infrasonic generator. The duration of infrasound exposure was set at 2 hours and the calcein concentration at 50 µM. Results were analyzed using a linear mixed effects model to determine how cell line and infrasound frequency influenced relative increases in calcein uptake. The model included fixed effect terms for 4 cell lines (U87, U251, SF210, and SF188), 4 frequencies (dynamic, 8.5, 11.6, and 15 Hz), and interactions between cell lines and frequencies. Two random effect terms were added to allow for variation among cell line intercepts and for measurement variation within each combination of cell line and frequency. The model was fit to the data using the statistical program nlme written in the R statistical language. The program tests the statistical significance of each fixed effect term in the model using a t statistic.
Differences were observed among the different cell lines regarding the degree to which infrasound increased calcein uptake (see Figure 5). The SF210 and SF188 cell lines displayed significantly higher infrasound-induced increases in calcein uptake compared with the other 2 lines (approximately 2-fold; P < .001). Within cell lines, the analysis found that most of the responses were independent of frequency, whether consisting of dynamic frequencies or at specific frequencies. However, there were several pairings that did yield statistically significant differences in frequency response. There was a relative increase at 15 Hz for U87 (P = .03) and SF210 (P = .06) and relative decrease at 8.5 Hz for U251 (P = .04) and SF210 (P = .06). Although these differences were not as pronounced as the differential responses between cell lines, they indicate potential for frequency-dependent permeabilization unique to each cell line.

Relative increases in calcein concentration with infrasound.
Correlation of Enhanced Cisplatin-Induced Apoptosis and Permeabilization by Infrasound
If membrane permeabilization is a factor underlying the ability of infrasound to chemosensitize glioblastoma cells, differences between the cell lines in relative increases of calcein uptake with infrasound exposure should correlate with the extent of chemosensitization achieved in each cell line. To test this, 3 of the glioblastoma cell lines were treated with cisplatin at the same concentration of calcein (100 µM) and the same infrasound duration (4 hours). The degree to which infrasound exposure increased apoptosis was then compared with infrasound-induced increases in calcein uptake (see Figure 6). The SF188 cell line was not included in this set of experiments because 100 µM cisplatin resulted in greater than 50% cytotoxicity (data not shown). The relative increases in apoptosis associated with infrasound along with cisplatin and the infrasound-induced increases in calcein uptake were tightly correlated so that prediction of enhanced apoptosis from increased calcein uptake is highly accurate. In fact, greater than 99% of the variation in enhancement of cisplatin-induced apoptosis by infrasound is explained by the increase in calcein uptake. This correlation reinforces the notion that increased membrane permeability is a key mechanism contributing to enhanced apoptosis observed with infrasound exposure combined with cisplatin. Increased intracellular concentrations of cisplatin may trigger apoptosis in the glioblastoma cells through increased drug levels within the nucleus and mitochondria as well as by damage to cytoplasmic proteins and RNA.33,34

Linear regression of effects of infrasound on calcein uptake and increased sensitivity to 100 µM cisplatin.
Discussion
The results of this study demonstrate that infrasound chemosensitizes U87, U251, SF210, and SF188 glioblastoma cells to cisplatin and that these effects are contributed to in large part by increased membrane permeability. Similar to ultrasound and shock wave techniques, local application of infrasound in clinical applications would combine the enhancement of drug transfer with the capability of restricting this effect to the desired area. Specifically in the case of treating brain tumors, infrasound may prove superior to ultrasound as its relatively longer wavelength can penetrate solids 35 (ie, delivery through the skull bone) more easily yet remain less disruptive to brain tissue than shock waves. Although all these vibrational techniques are extracorporeal, the potential thermal damage to tissues that can be associated with certain uses of ultrasound36,37 and cellular disruption connected to shock waves 38 are unlikely in the case of this particular application of infrasound owing to lower intensity and mechanical decoupling.
The precise mechanisms underlying infrasound-mediated permeabilization are not identified in this study, and research on the effects of infrasound at the cellular level is scant, especially in comparison with those investigating similar applications of ultrasound. The mechanisms underlying ultrasound-mediated permeabilization have been largely attributed to microbubble formation, oscillation, and collapse due to acoustic cavitation. These effects have been implicated directly with membrane augmentation through lipid disordering and/or sonoporation from microstreaming, 39 as well as indirectly by way of cell damage from free radicals generated from the breakdown of water molecules. 40 Although infrasound and ultrasound are similar in that they are both vibrational energy modalities, it is unlikely that acoustic cavitation is involved in this particular application of infrasound. The intensities associated with cavitation for ultrasound-mediated chemosensitization range from 0.2 to 400 W/cm2 with associated pressure amplitudes of 170 to 340 000 MPa. 41 The pressure amplitudes generated by the infrasound device used in this study measure approximately 10 mPa, which are 6 orders of magnitude smaller—mPa versus MPa—and are far below the theoretically determined cavitation threshold needed to induce such phenomenon. 42 It should be noted that although the chemosensitization effects measured in this study are modest, there is potential for significantly larger effects to be observed with equipment that can deliver higher output.
Although research on the biological effects of infrasound is limited, relevant studies do exist. A computational analysis of the response of bilayer lipid membranes to pressure waves using molecular dynamics modeling demonstrate that transient permeabilization can be achieved and that membrane thickness and area per lipid are reduced in this instance. 43 One early study investigating the responses of artificial bilayer membranes to infrasonic vibrations found that capacitive response decreased with increasing frequency over a narrow range (~0.2 Hz to ~10 Hz). 44 Interestingly, the parameters identified in the aforementioned permeability study are also determining factors of membrane capacitance. This supports the notion that cellular membrane permeabilization is mediated by infrasound and perhaps even differentially responsive to specific frequency ranges and suggests that the alteration of membrane thickness and area per lipid are potential underlying mechanisms. Such findings are consistent with the results of this study, which showed frequency dependence as well as differential responses among cell lines. In summary, the outcomes of this study provide encouraging data for enhancing the chemotherapeutic effects of cisplatin using infrasound and that there is potential for optimizing chemosensitization among tissue types using specific infrasonic frequencies. Since no adverse effects were observed among the tested cell lines from infrasound alone, we are optimistic that localized application of infrasound would be an innocuous method of lowering the effective dosages of toxic chemotherapies.
Study Limitations
Although it is reasonable to assume that infrasound exposure at the levels applied in this study will not be disruptive to normal cells and tissue, explicit experimentation should be performed to verify this. Indeed, when discussing the optimization of chemosensitization using infrasound, the reduction of harmful effects from toxic chemotherapies to normal tissue can and should also be considered. As noted above, given the observed differential responses between cell lines and frequency dependence, it is quite possible that specific frequencies may be identified that render tumor tissue more permeable to chemotherapies than normal tissue.
Footnotes
Acknowledgements
The authors wish to thank Tri Luu, Rob Silfvast, and Brian Wong for technical assistance, Dr. Richard Lee for review of the manuscript, and Dr. Michael Degtyarev for translation of key references.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Grant Number NIH R21 AT003312-01A1 from the National Center for Complementary and Alternative Medicine (NCCAM). The contents of the manuscript are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.