
Abstract
Purpose. Following surgical lung resection, patients frequently suffer functional decline and reduced activity levels. Despite this exercise interventions are not routinely provided. This study aimed to establish the safety and feasibility of exercise administered following lung resection in an Australian setting. Method. Pilot randomized controlled trial. Fifteen individuals (53% male), mean ± standard deviation age 65.5 ± 16.1 years, undergoing surgery for suspected lung cancer. Randomization occurred postoperatively. Control arm received protocolized inpatient respiratory physiotherapy. Intervention arm additionally received twice daily exercise until discharge home and twice weekly as outpatient for 8 weeks. Outcome measures (safety, feasibility, functional capacity, functional mobility, and health-related quality of life [HRQoL]) were assessed preoperatively and 2 and 12 weeks postoperatively. Results. Fifteen participants (lung cancer n = 10) were assigned to control (n = 8) and intervention (n = 7) groups. Inpatient exercise was delivered on 71% of occasions (35 out of 49 planned sessions). Four participants attended outpatient exercise sessions and these participants attended sessions on 81% of occasions (52 out of 64 planned sessions). No adverse events occurred. There was a significant between group difference in 6-Minute Walk Test (6MWT; P = .024). In both groups the 6MWT declined from baseline to 2 weeks postoperative and then improved up to 12 weeks; improvements were greater in the intervention group. Intervention was associated with positive trends of improvement in some HRQoL domains. Conclusions. Exercise intervention performed in the inpatient and outpatient settings for individuals following lung resection was safe and feasible. The uptake rate for outpatient exercise was 57%, similar to previous trials; however, adherence was excellent within the subgroup of participants who attended. Further research is required to investigate the best setting of exercise delivery and explore ways to improve the uptake rate.
Introduction
Lung cancer is the most prevalent cancer diagnosed worldwide and is associated with the highest mortality. 1 In Australia, cancer is the greatest contributor to the burden of disease and lung cancer specifically is one of the leading causes. 2
Lung cancer is associated with debilitating and distressing symptom clusters that frequently result in individuals electively limiting their participation in physical activity.3-6 Inactivity perpetuates a cycle of deconditioning, loss of muscle mass, worsening exercise tolerance, and functional decline that subsequently affects an individual’s ability to participate in further physical activity, maintain health-related quality of life (HRQoL), and tolerate cancer treatment. 7
Surgical resection is the treatment of choice for stage I to IIIa lung cancer.
8
Lung resection is associated with an immediate reduction in exercise tolerance,
9
with peak oxygen consumption (V
Exercise interventions in the cancer population have been shown to be associated with benefits on cardiorespiratory fitness, HRQoL, mood, symptoms, and treatment side-effects.13-15 Most research to date has included individuals with breast or hematological malignancies. 16 Research investigating the benefit of exercise for individuals with lung cancer is still in its early stage; however, small cohort and case series studies conducted internationally have demonstrated positive benefits associated with exercise. 17
Exercise interventions implemented following lung resection have been shown to be associated with benefits on functional capacity, HRQoL, shoulder pain, and shoulder function; however, most previous trials are of a cohort or case series design and none of them have been performed in an Australian setting.18-22 Despite promising results from these studies, the research has not been disseminated into clinical practice and exercise intervention following lung resection is not routine. 23 The main focus of physiotherapy practice in Australia for individuals following lung resection is respiratory prophylaxis of postoperative pulmonary complications (PPCs) in the immediate postoperative period.23-25 The feasibility of implementing an exercise intervention in Australian inpatient or outpatient settings for individuals following lung resection has not been reported.
The objective of this trial was to establish the safety and feasibility of providing an exercise intervention to individuals following lung resection. Secondary objectives were to explore changes in functional capacity, functional mobility, and HRQoL in participants exposed to standard care compared with an additional exercise intervention. It was hypothesized that (a) administering an exercise intervention following lung resection would be safe and not associated with any adverse events, (b) inpatient and outpatient exercise would have an uptake and adherence rate of greater than 70%, and (c) a trend toward improvements in functional capacity, functional mobility, and HRQoL would be found in the intervention group.
Method
Trial Design
A single-center pilot randomized controlled and assessor blinded trial (RCT) was conducted at a tertiary hospital in Melbourne, Australia, from March 2009 to February 2010. The RCT design was chosen to simulate and test the method to be used in a subsequent phase II trial and to allow a comparison of results with a control group, given the known pattern of functional decline seen immediately postoperatively.
Participants
Eligible participants were English-speaking individuals, aged 18 years or older, undergoing lung resection for suspected or confirmed cancer. Individuals were screened at a general thoracic surgery clinic by a recruitment therapist. All recruited participants provided written informed consent and underwent baseline outcome measurement prior to surgery (Figure 1). Randomization was undertaken using an off-site computer-generated random number table and sequentially numbered sealed opaque envelopes prepared by personnel not involved in the study. Randomization occurred on the first day following surgery. For each consented participant, on the morning after surgery, the next consecutive assignment envelope was opened by personnel not involved in the study and the intervention therapist was notified of allocation. Participants and outcome assessors were blinded to allocation. The study was granted local ethical approval and the protocol was registered with the Australian and New Zealand Clinical Trials Registry (ACTRN12611000431921) (universal trial number U1111-1121-0408).

Consort diagram 26
Treatment
Participants were assigned to receive standard care physiotherapy (control) or exercise intervention (intervention; Figure 1). All participants were provided with standard care from a ward physiotherapist blinded to group allocation.
Standard care
Physiotherapy for individuals following thoracic surgery at the institution followed a clinical pathway commencing day 1 postoperatively. Participants sat out of bed and mobilized away from the bedside at least 20 m and at least 50 m on the first and second postoperative days, respectively. Ambulation with the ward physiotherapist was ceased once it was deemed on assessment that the individual no longer required specific physiotherapy intervention. Participants who developed PPCs amenable to physiotherapy treatment additionally received respiratory physiotherapy, such as airway clearance or continuous positive airway pressure. Thoracic spine and shoulder stretches were taught to participants once intercostal catheters were removed with handouts encouraging performance of these exercises daily for the following 3 weeks. On acute hospital discharge (median length of stay 6 days, range 3-17 days), inpatient rehabilitation or home-based post–acute care physiotherapy was only provided to participants if their mobility at time of discharge had deteriorated to a level preventing safe discharge home. No other follow-up physiotherapy or outpatient exercise was offered to participants after discharge.
Intervention
Participants randomized to the intervention arm received additional exercise intervention, commencing day 1 postoperatively, administered by a second independent blinded physiotherapist. A twice daily structured exercise program involving aerobic, resistance, and stretching exercises was performed until discharge home (Table 1). The length of inpatient hospital stay was determined by the surgical team and medical readiness for discharge. The median length of stay (LOS) for the intervention group was 4 days (range 3-9; Table 3). Participants were monitored during the exercise sessions with portable pulse oximetry (oxygen saturation and heart rate [HR]) and participants did not commence or continue an exercise or testing session if they satisfied any of the safety criteria (Table 2). The safety protocol used had previously been developed, tested, and implemented in similar research trials at the same institution. 27
Intervention Arm Inpatient Exercise Program

Abbreviations: ICCs, intercostal catheters; LL, lower limb; reps, repetitions; RPE, rating of perceived exertion.
Breathlessness = somewhat hard on the modified 10 point BORG scale. 28
Exertion = somewhat hard on the rating of perceived exertion (RPE) scale. 28
Safety Protocol: Discontinuation of Exercise Intervention or Testing Criteria27

Abbreviations: SBP, systolic blood pressure; Sp
Group Demographics

Abbreviations: LOS, length of stay; n, number; BMI, body mass index; SD, standard deviation.
On discharge home, participants in the intervention arm were given a booklet with a home exercise routine to complete from time of hospital discharge until commencement of the outpatient exercise program. Participants were encouraged to walk daily for a total of 30 minutes at a breathlessness intensity of Borg 4 and to continue lower limb resistance exercises and stretches. 28 One phone call per week was made to encourage adherence. Three domiciliary visits from a physiotherapist were provided to assist with exercise progression.
Participants in the intervention arm commenced an 8-week outpatient exercise program supervised by a physiotherapist or exercise physiologist following their 2-week postoperative surgical review. Exercise sessions occurred twice weekly for 1 hour in an outpatient gymnasium and included a combination of stationary cycling, treadmill walking, upper and lower limb resistance exercises, and upper limb and thoracic stretches. Prior to commencing the first outpatient exercise session, participants performed a symptom-limited incremental submaximal cycle ergometer test (CPEX) to assist with exercise prescription. The test was performed on a standardized cycle ergometer in the gymnasium. Participants were monitored with portable pulse oximetry (oxygen saturation and HR) and questioned regarding their Borg breathlessness score each minute. Cycle wattage was increased incrementally each minute according to a standardized protocol. 29 The test was ceased when the participant achieved an HR of 85% maximum predicted, Borg 7, a breach of the safety protocol (Table 2), or the participant requested to stop. The maximum wattage achieved was recorded. During the exercise sessions aerobic exercise was performed for 30 minutes and was a combination of treadmill walking and/or stationary cycling. 28 Initial cycling wattage was prescribed from the pre-outpatient rehabilitation CPEX and training commenced at 70% wattage of initial test. Treadmill walking was initially prescribed at 70% baseline mean walking speed, calculated by multiplying the number of meters walked in their hospital discharge (time point 2) 6-minute walk test (6MWT) by 0.007. The intensity of aerobic exercise was aimed at Borg 4 and exercise was progressed each session using the Borg scale, with cycling wattage and walking speed increased to achieve Borg 4 throughout the 8-week program. Resistance exercises were individually prescribed to participants and included exercises such as resisted leg press, calf raises, wall squats, step ups, chest press, seated row and triceps extension with hand held weights or theraband and aimed at a fatigue intensity of RPE 13. 28 Prior to commencing the first outpatient exercise session, the maximum weight each participant could comfortably, correctly, and safely lift on each machine exercise was assessed. Each exercise was commenced at 80% of the initial weight lifted, and the exercises were performed for 3 sets with repetitions, sets, and weight increased according to standard American College of Sports Medicine strengthening guidelines. 30 No upper limb strength training was performed within 6 weeks of surgery to minimize potential wound complications. Upper limb and thoracic stretches were performed within pain limits. Participants were encouraged to continue their home exercise program on the days they did not attend class.
Outcomes
Primary outcomes of the study were safety and feasibility. Safety was assessed by a number of adverse events occurring during exercise testing, inpatient exercise training, and outpatient exercise training. Adverse events were recorded on a protocolized data collection form. If any of the safety protocol criteria were met during the exercise session (Table 2), an adverse event was documented to have occurred. Participants were questioned at each outpatient exercise session if any identifiable adverse events (such as a fall or severe breathlessness) had occurred while completing the unsupervised home exercise program. Adverse events were not formally monitored in the home setting. Feasibility was assessed by recruitment rate, consent rate, number of inpatient exercise sessions delivered, and participant attendance at outpatient sessions.
Secondary outcomes were change in functional capacity, functional mobility, and HRQoL and were measured by a blinded outcome assessor who was not involved in the intervention exercises. Functional capacity was assessed at 3 time points—baseline (within 2 weeks prior to surgery), 2 weeks postoperatively, and 12 weeks postoperatively—using 6WMT according to standardized guidelines. 31 The 6MWT is a commonly used, valid, and reliable submaximal self-paced test that measures the distance an individual can walk over a flat straight corridor in 6 minutes.31,32 Duplicate tests were performed for reliability and the maximum 6MWT was used. 31 Predicted 6MWT was calculated for all individuals. 33
Functional mobility was assessed at each time point using the timed-up and go test (TUG), a valid and reliable tool for quantifying functional mobility in the elderly, which has documented normal values for individuals aged 60 years and older.34,35 Participants are timed as they stand up from a standardized chair, walk 3 m, turn around, walk back, and sit down. The time taken has been shown to correlate with balance, gait speed, and outdoor walking safety. 34 Three tests were performed for reliability and the best time was used.
HRQoL was assessed at baseline and 12 weeks postoperatively using both general and cancer-specific questionnaires. The Short Form 36 version 2 (SF36) is a widely used health status measure that has been successfully used in healthy and lung cancer populations.17,36,37 The 36-item questionnaire incorporates 8 dimensions (physical function, role physical, bodily pain, general health, vitality, social function, role emotion, and mental health), which can be computed into 2 summary measures estimating overall physical health (physical component summary) and mental health (mental component summary). 37 Most questions are rated according to occurrence in the past 4 weeks.
The European Organization for the Research and Treatment of Cancer HRQoL questionnaire and lung cancer module (EORTC-QLQ-C30-L13) is a widely used, valid, and reliable tool for individuals with lung cancer.17,38 The core 30-item questionnaire incorporates 5 functional domains (physical, role, emotional, cognitive, and social functioning), 3 symptom scales (pain, fatigue, nausea or vomiting), a global health and quality of life (QoL) status score, and a number of single items (appetite loss, dyspnea, diarrhea, constipation, insomnia, and financial impact). The 13-item L13 includes multi- and single-item scales measuring specific symptoms of the disease and treatment-related side effects. 39 Responses to most questions are rated on a 4-point Likert-type scale according to occurrence in the past week. Global health status/QoL is rated on a 7-point numerical analogue scale. Higher scores on functional domains and global health status/QoL scale represent higher functioning and higher HRQoL. Lower scores on symptom domains and single items represent less symptoms.38,40 The MCID for domain scores for change in individuals with lung cancer have been established, 41 as have normative scores for the different tumor streams. 42
Sample Size
The pragmatic sample size chosen was 15. The study was not powered to identify statistically significant changes in secondary outcomes; however, these measures were included in an attempt to describe trends that may assist with development of future phase II trials.
Statistical Methods
Independent samples t tests were conducted to compare equivalence of baseline variables between groups. Data were assessed for normality using the Kolmogorov–Smirnov statistic. For the measures of 6MWT and TUG, a mixed between–within subjects analysis of variance (ANOVA) was conducted to compare difference between groups: a covariate was included if statistically significant differences between groups were identified at baseline. Data were presented as mean ± standard deviation (SD) at each time point.
SF-36 scores were presented as norm-based scores standardized to Australian population mean ± SD of 10 ± 50. 37 Scores below 50 represent poorer health than the general Australian population. EORTC-QLC-C30-LC13 domain and single-item raw scores were linearly transformed to a scale of 0 to 100. 40 A mixed between–within subjects ANOVA was conducted to compare difference between groups for SF36 and EORTC-QLC-C30 domains. HRQoL domain scores were presented as mean ± SD at each time point and mean difference with 95% confidence intervals (95% CI) within groups over time.
Statistical analyses were calculated using SPSS for Windows statistical software package (Version 18.0.2; IBM SPSS Inc, Chicago, IL).
Results
Primary Outcomes
Between March and November 2009, 175 patients were screened at thoracic surgery clinic, 18% (n = 32) were eligible and 13% (n = 22) were approached (Figure 1). The main reasons for ineligibility were participant “not undergoing lung resection” (n = 78) and “not suspected lung cancer” (n = 45). The main reason for eligible patients not being recruited was “missed by recruitment therapist” (n = 10). There was an 82% consent rate (n = 18 out of 22). Reasons for decline were “did not like exercising” (n = 1), “too difficult with young children” (n = 1), and “not specified” (n = 2). Eighteen participants consented to the study and underwent baseline measurement. Two participants did not proceed to surgery, and 1 participant had surgery at another hospital, leaving 15 participants to undergo randomization (on the first day following surgery) to control (n = 8) and intervention (n = 7) arms (Figure 1). Following surgery, 10 participants (67%) had lung cancer diagnosed from histology in control (n = 7) and intervention (n = 3) arms.
Table 3 demonstrates the baseline demographics of participants. There were no statistically significant differences between groups. Of the 15 participants, 53% were male with a mean ± SD age of 65.5 ± 16.1 years.
No adverse events occurred during exercise testing, inpatient exercise training, or outpatient exercise training. In the intervention group, inpatient exercise sessions were delivered on 35 out of 49 occasions (71%). Reasons for missed sessions included hypotension precluding exercise (n = 1), participant having procedure (n = 2), lack of staff resources (n = 1), participant declined due to pain (n = 4), participant declined as had recently walked with ward physiotherapist (n = 4), and no reason specified (n = 2). During the home-based exercise program, adverse events were not formally recorded; however, on questioning at each outpatient session no participant retrospectively reported an adverse event to have occurred while exercising at home.
In the intervention group, 3 of the 7 participants declined to commence the outpatient exercise program following discharge home (57% uptake rate) due to “too many commitments” (n = 2) and “concerned about exercising during chemotherapy” (n = 1). Two of the 3 participants who declined did not have a diagnosis of cancer. The remaining 4 participants (lung cancer n = 2) attended outpatient sessions on 52 out of 64 occasions (81%).
Secondary Outcomes
At baseline there were statistically significant differences in 6MWT (P = .006) but not TUG (P = .061) between groups. When controlling for baseline 6MWT, there was a significant between group difference in 6MWT (P = .024) with the intervention group improving to a greater extent than the control group. In both groups, the 6MWT declined from baseline to 2 weeks postoperative and improved from 2 to 12 weeks postoperative: intervention group mean (SD) 677.0 ± 89.3 m to 647.5 ± 53.1 m to 705.7 ± 65.3 m; control group mean (SD) 435.8 ± 98.2 m to 426.0 ± 64.3 m to 458.2 ± 38.6 m (Table 4). Changes were only greater than the MCID in the intervention group. 43 There was a significant between group difference in TUG (P = .041) with the control group improving to a greater extent than the intervention group. In both groups, the TUG improved from baseline to 2 weeks postoperative and then worsened up to 12 weeks postoperative: intervention group mean seconds (SD) 6.3 ± 1.6 to 4.4 ± 2.6 to 4.9 ± 0.8; control group mean seconds (SD) 9.0 ± 2.6 to 6.0 ± 3.2 to 6.8 ± 1.5 (Table 4).
Change in 6MWT and TUG Across Time Within Groups
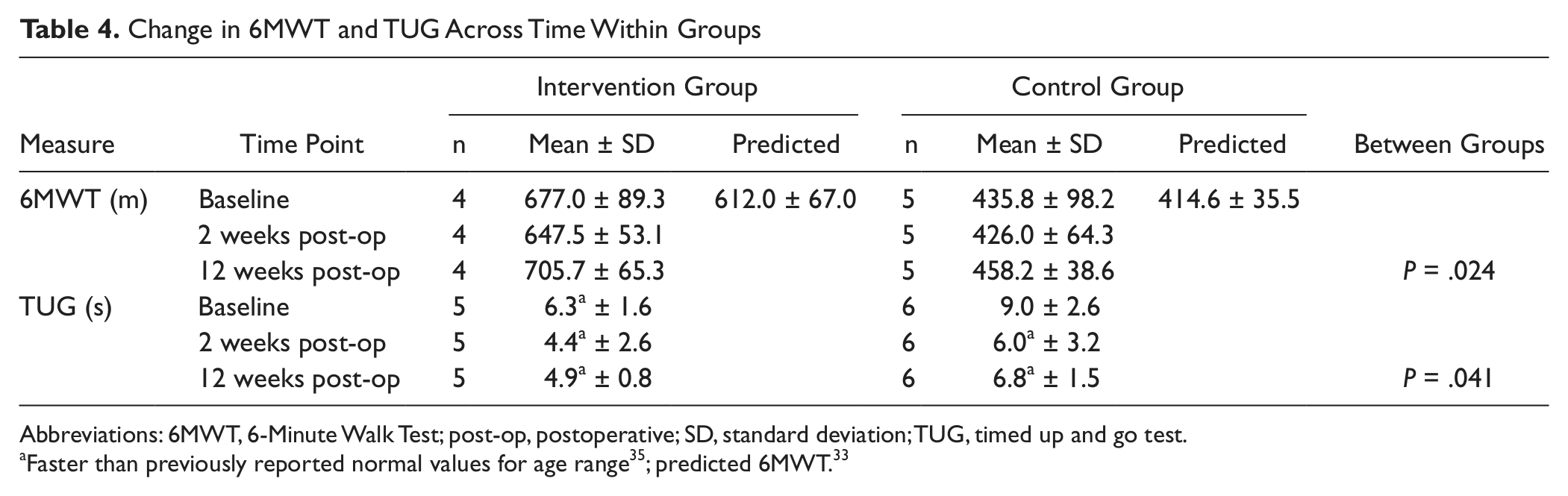
Abbreviations: 6MWT, 6-Minute Walk Test; post-op, postoperative; SD, standard deviation; TUG, timed up and go test.
HRQoL measured with SF-36 and EORTC-QLQ-C30 is displayed in Table 5. In the SF-36, at baseline, there were no statistically significant differences between groups (P > .05); however, the role emotional domain of control group and the social function, role emotional, and mental health domains of the intervention group were outside 1 SD of Australian norm (worse). There were no significant between-groups differences identified using ANOVA; however, at the 12-week follow-up the physical function domain of the control group was outside 1 SD of the Australian norm (worse). Over time, trends noted in the physical function and mental health domains demonstrated worsened scores in the control group compared with improvement in the intervention group, greater than the reported MCID. The general health and vitality domains both declined in the control group and were unchanged in the intervention group over time (Table 5).
Change in HRQoL Norm-Based Scores in the SF-36 and HRQoL Domain Scores in the EORTC-QLQ-C30 Within Groups

Abbreviations: CI, confidence interval; diff, difference; int, intervention group; EORTC-QLQ-C30, European Organization for the Research and Treatment of Cancer; fn, function; MCS, mental component summary; N&V, nausea and vomiting; PCS, physical component summary; prob, problems; SD, standard deviation; SF-36, Short Form 36 Version 2; QoL, quality of life. SF36 MCID = 2 points if norm based score is <40 or 3 points if >40. EORTC QLQ-C30 MCID: global health status = 10 points; physical function = 6 points; social function = 8 points; role function = 11 points; fatigue = 6 points; pain = 15 points. 41
Improvement in domain greater than the MCID.
Decline in domain greater than the MCID.
In the EORTC-QLQ-C30, at baseline, the only statistically significant difference between groups was the “nausea and vomiting” domain (P = .05). Using ANOVA, the only significant between-groups difference was “nausea and vomiting” (P = .03), and no other significant between-groups differences were found. Trends were noted with worsening of the physical function, fatigue, and pain domains greater than the MCID in the control group, which were not seen in the intervention group. A decline in role function was seen in both groups (Table 5).
Discussion
This was the first study to assess the safety and feasibility of implementing an exercise program for individuals following lung resection in an Australian setting. Our results are consistent with previous studies performed internationally that show exercise for individuals following lung resection is safe.19,44 In this trial, according to the safety protocol, exercise was not commenced only once out of 45 inpatient occasions and no sessions were ceased early due to a protocol breach. No adverse events occurred during exercising testing, inpatient exercise sessions, or outpatient exercise sessions, and individuals who participated in the intervention program did so safely in the early postoperative period. While participants were given safety guidelines for unsupervised exercise in the home setting, adverse events were not formally recorded and therefore no conclusions can be drawn with regard to the safety of the home-based exercise component. Although previous research in other patient populations have not reported issues with safety in home-based exercise,45,46 future research needs to explore novel and innovative ways to monitor patients’ safety in the home setting for exercise with this population.
This study included 15 individuals undergoing lung resection for suspected cancer. The mean age in the trial was below the median age reported for Australians diagnosed with lung cancer (70.3 years). 47 Given the younger age of participants and the fact that a third of participants had nonmalignant disease (33.3%), application of our results to individuals with lung cancer undergoing surgery needs to be done with caution. Previous research investigating postoperative changes and impairments following lung resection has been focused on individuals undergoing surgery for lung cancer specifically.10-12 In practice, however, it is inevitable that some individuals who undergo surgery for suspected lung cancer are actually diagnosed with nonmalignant disease intraoperatively; decreasing complications and supporting recovery in these patients is also important because morbidity in the postoperative thoracic surgery population is high. 48 Control and intervention groups also had notable (but not statistically significant) differences in age, gender, respiratory function, and cancer diagnosis at baseline, which is most likely due to the small sample size, and therefore results need to be read with caution when comparing the groups. Although we have reported P values in this study, due to the small sample size, statistically significant results in secondary measures must be interpreted with caution.
Agreement to participate at time of recruitment was encouraging, with only 4 individuals declining inclusion into the trial. The consent rate (82%) is greater than previously documented uptake rates for exercise programs offered to individuals following lung resection (12% to 50%)19,22 or individuals with cancer (67%). 49 However, after hospital discharge only 57% of participants agreed to participate in the outpatient component of the intervention, and the time commitment to travel and complete outpatient sessions appeared, on questioning, to be the main barrier. This is consistent with a recent systematic review identifying “too busy/no time” as the most frequent reason for individuals with cancer refusing exercise interventions. 49 Despite the uptake rate for outpatient exercise being less than the 70% hypothesized, we still conclude the intervention to be feasible, on the basis that the uptake rate is similar to uptake rates previously reported for similar outpatient-based exercise programs such as pulmonary rehabilitation (8.3% to 64%).50-53 Further research is required to investigate the best setting and method of exercise delivery (e.g., home-based training, supervised vs unsupervised) to achieve the greatest uptake rates in a population following lung resection. Our trial did not measure adherence to the unsupervised home exercise program, but home exercise seems a logical alternative for participants unwilling or unable to commit the time to exercise in an outpatient setting. Adherence to unsupervised exercise has not been reported for a population following lung resection. This was not measured in our study and is an important evidence gap that requires further investigation. 17 Participants who did take up the outpatient intervention achieved an attendance rate of 81%, which is consistent with previous studies in this population (72% to 85%).17,19,54
Results from this trial did confirm the hypothesis that there would be a trend of improvement in functional capacity favoring the intervention group. However, it is important to note that the sample size was not powered to detect statistical differences, standard deviations were large, and groups commenced with differences (worse functional capacity in the control group). This may have been a result of the variability in age between the groups and/or the small sample size. The high functional capacity level of the intervention group may have also resulted in a ceiling effect on the change in 6MWT seen over time. It is interesting to note that despite no decline in the 6MWT by the control group, the control group did have a decline in physical function measured by the SF36. This is likely due to the fact that the SF36 measures physical function more broadly than just walking. However, the suitability of the 6MWT as an outcome measure in this population needs to be reconsidered. Future trials could consider the use of the endurance shuttle walk test,
55
the incremental shuttle walk test,56,57 or the CPEX
58
as potentially more appropriate tests to detect changes in functional capacity and/or V
Our study was the first RCT to provide structured outpatient exercise for people following lung resection and had some notable differences to previous studies in this area. Other comparative and case series trials have reported improvements in 6MWT and V
The suitability of the use of the TUG as an outcome measure of functional mobility in this trial needs to be questioned. Regardless of group allocation, the trend of improvement seen in the TUG from baseline to 2 weeks postoperative and then deterioration from 2 to 12 weeks contradicts the trend seen in the 6MWT. This may be due to the fact the TUG has been designed for use in the elderly (60 years and older) and our trial included a significantly younger cohort. 34
Our results did support the hypothesis that improvement in HRQoL would be favored in the intervention group. At baseline, our cohort’s HRQoL was slightly worse than the SF-36 normative data for Australians with some domains being outside 1 SD of the norm. On the EORTC-QLQ-C30, our cohorts’ global HRQoL and physical function were better than the EORTC-QLQ-C30 normative data for individuals with lung cancer. 42 At the 12-week follow-up, the trend in physical function measured by SF36 and EORTC-QLQ-C30 was a decline in the control group and maintenance/improvement in the intervention group. Fatigue and pain were also noted to worsen in the control group over time. The different trends observed in HRQoL between groups may not only be due to the intervention provided, but also due to the cancer disease, with a higher proportion of individuals with malignant disease in the control group. Controlling for nonmalignant diagnoses between groups in future trials is vital and this may be achieved by using stratified randomization designs. The improvement in HRQoL in the intervention group is consistent with the findings by Jones and colleagues who reported improvements in global HRQoL, fatigue, and functional well-being following the implementation of an exercise program after surgery. 19
Limitations
This study was limited by the fact that 33% of participants (n = 5) did not have a diagnosis of lung cancer. This occurred because recruitment and randomization occurred prior to histological confirmation of cancer. This is difficult to avoid in surgical patients if baseline testing is to take place prior to surgery. Baseline testing if undertaken immediately postoperatively would not be truly representative. Allowing for nonmalignant diagnoses in recruitment numbers in future trials is therefore important.
The second limitation to the study was that the intervention group was significantly fitter than the control group at baseline. This may have had an impact on the change observed in functional capacity and/or HRQoL over time between groups.
The third limitation to this study was that adherence and safety to home-based exercise was not measured and therefore it is impossible to conclude how much exercise participants in the intervention group actually performed and the safety of such a program. Future trials should include measurement of home-based exercise adherence and safety.
Conclusion
Exercise intervention performed in the inpatient and outpatient settings for individuals following lung resection was safe and feasible. The uptake rate for outpatient exercise was 57%, similar to previous trials; however, adherence was excellent in the subgroup of participants who attended. Further research is required to investigate the best setting for exercise delivery and explore ways to improve uptake rates. Large RCTs are required to substantiate the benefit of exercise for individuals following lung resection. This pilot trial has identified several important points to consider in future trials.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors wish to acknowledge the support of the Physiotherapy Department, Austin Hospital, Australia. This study was supported by a Jill Nosworthy Bequest, Physiotherapy Research Foundation.