
Abstract
Background:
With an increasing number of non-small cell lung cancer (NSCLC) patients being offered surgical treatment, postoperative rehabilitation is also being increasingly emphasized. Traditional Chinese medicine (TCM) holds promise for enhancing postoperative recovery, with treatment methods still in refinement. This study aims to evaluate the efficacy of Chinese herbal decoction and Liuzijue exercises in NSCLC patients during the rapid postoperative recovery period.
Methods:
A randomized, parallel-group clinical trial assigned 50 patients to receive Chinese herbal medicine and Liuzijue exercise plus symptomatic treatment, and 49 to symptomatic treatment alone. Treatment continued until postoperative complications resolved, chest tubes were removed, and no abnormal examination findings were reported. The primary outcome was Quality of Life Questionnare-Core 30 (QLQ-C30) score. Secondary outcomes included MOS item short form 36-Item Short Form Health Survey (SF-36) score, rate of complications, six-minute walk test (6MWT) distance, Leicester Cough Questionnaire (LCQ) score, numerical rating scale (NRS) score, and functional activity score (FAS).
Results:
Significant improvements in role (MD: 12.15, 95%CI: 2.99-21.32, P < .05) and social functioning (MD: 10.25, 95%CI: 1.72-18.78, P < .05) were observed in the intervention group vs. controls, as measured by QLQ-C30. The intervention group showed better post-treatment SF-36 scores in Role-Physical (RP), Social Function (SF), Role-Emotional (RE), and Mental Health Summary (MCS) (P < .05). The complication rate was lower in the intervention (20.00%) than the control group (44.44%) (P < .05). The intervention group also had a significant increase in FAS scores (P < .05) and covered a better 6MWT distance (P < .05).
Conclusion:
Chinese herbal decoction and Liuzijue exercises during the rapid recovery period after lung cancer surgery enhanced patients’ QoL and physical endurance, and mitigated complications.
Introduction
Lung cancer is one of the most common malignancies. With the advancement of CT diagnosis technology, lung cancer screening has been promoted. 1 Early stage lung cancer with ground glass nodules as the main imaging manifestation is referred to surgery, 2 and the recurrence-free survival rate after radical surgery for lung cancer patients with lesions less than 2 cm can reach 99.7%. 3 However, surgery also poses health risks to patients. Postoperative lung cancer patients have a high symptom burden. Postoperative patients with lung cancer commonly experience shortness of breath and cough within 4 weeks, and coughing negatively affects patients’ quality of life (QoL). 4 Symptoms such as fatigue, pain, sleep disturbances, and anxiety are also frequent and affect the lives of patients. 5 These discomfort symptoms are most severe in the first week after surgery and gradually decrease from 2 to 8 weeks after surgery, but even then they do not reach the preoperative level.4 -7 Furthermore, 53% of patients who underwent lobectomy and sublobar resection experienced varying degrees of postoperative complications within 90 days after surgery. 8 In the most severe cases, patients are even at risk of death. The mortality rate within 90 days after surgery is 5.9%. 9
The health risks associated with lung cancer surgery make postoperative rehabilitation valuable. In this context, attention has also been paid to the standardized management of the perioperative period. The ERAS (enhanced recovery after surgery) concept was introduced into the perioperative management of thoracic surgery. Related guidelines describe the systematic management of the perioperative period for lung cancer surgery, while emphasizing the importance of preoperative pulmonary rehabilitation exercises and early postoperative activity. There are clear recommendations for preoperative pulmonary rehabilitation exercises and intraoperative management,10,11 but there is still less consensus on the specific protocol for postoperative rehabilitation, and there are still shortcomings in the current studies.12,13
There is potential for traditional Chinese medicine (TCM) therapy for postoperative pulmonary recovery. Pneumonia is one of the common complications affecting recovery after lung cancer surgery. Combined use of Chinese herbs may provide symptomatic relief and promote lung recovery in patients with pneumonia. 14 Traditional mind-body exercise therapy has a positive impact on exercise capacity and QoL in patients with pulmonary disease, with similar or even better results than exercise-based cardiopulmonary rehabilitation (EBCR). 15 Among them, Qigong can improve patients’ lung function, exercise capacity, and QoL. 16 However, the studies applying TCM to the rehabilitation of postoperative patients with lung cancer are insufficient.
Therefore, a randomized controlled trial was conducted to assess the efficacy of TCM combined with conventional postoperative lung therapy in patients in the early perioperative period (within 1 week postoperatively) after lung cancer surgery. We hypothesized that the combination regimen would result in a more improved QoL than patients treated conventionally.
Material and methods
Study design
A randomized, parallel-group, clinical trial was adopted. The study was approved by the Ethics Committee of Yueyang Hospital of Integrated Traditional Chinese Medicine and Western Medicine, Shanghai University of Traditional Chinese Medicine (No. 2020-038), and registered with chictr.org.cn (Registration number: ChiCTR2100044776) on March 27, 2021. Participants provided written informed consent.
Participants
Eligible participants were recruited between April 2021 and September 2022 at Yueyang Hospital and Shanghai Pulmonary Hospital. Patients were eligible if they were between the ages of 18 and 80, underwent video-assisted thoracoscopic surgery (VATS) for resection of localized lung lesions, had postoperative pathological confirmation of lung cancer, and were capable of understanding and signing an informed consent form. To ensure the safety of participants undergoing postoperative rehabilitation exercises, patients who have undergone total lung resection, those transferred to the ICU postoperatively, those with intraoperative blood loss greater than 1000 ml or still experiencing active bleeding requiring surgical hemostasis, as well as those who have already developed postoperative complications, were excluded. Additionally, patients who were more than one week post-operatively were also excluded.
Randomization
Participants were randomly assigned to the intervention or control group in a 1:1 ratio. Patients included in this study were randomized using a dynamic minimization randomization approach. The randomized grouping was output by the randomization system of the Shanghai Medical Clinical Research Center. The above procedures are performed by independent clinicians.
Interventions
The eligible participants were randomly assigned to two groups. In addition to the standard treatment, the intervention group received TCM therapy.
The TCM therapy included the Chinese herbal decoction and Liuzijue exercise. The Chinese herbal decoction was prescribed by Dr. Xu Ling, chief physician of Yueyang Hospital. If the patient has cough, sputum and dyspnea as the main symptoms, use the modified prescription of Banxiahoupotang combined with Sangjuyin. (If the patient is accompanied by fever and spitting yellow sputum, add Sanbaipi and Digupi.) Patients with abdominal distension, poor appetite and constipation as the main symptoms use the modified prescription of Baohewan combined with Pingweisan. The components are shown in Table 1. If a patient has both types of symptoms both formulas can be prescribed at the same time. Each patient took Chinese herbal decoction orally twice a day, with each dose of 200ml, until the patient was discharged from the hospital. Liuzijue exercise is a traditional Chinese exercise. The exercise requires the patient to pronounce the different sounds of the six characters xu, he, hu, si, chui, and xi, while making specific body movements. Patients were led by a specialized physical therapist to perform Liuzijue exercise every other day until the patient was discharged. Each exercise includes 3 min warm-up and stretching exercises, 12 to 15 min six-character exercise, which is required to be completed at a slow speed, 5 to 10 min breathing adjustment and muscle relaxation after the exercise. The whole process did not over-emphasize the normality of the movements and the amount of exercise. If patients felt weak, they could pause and rest immediately. If patients were unable to perform limb extensions due to indwelling chest drains and other reasons, they could only perform breathing and vocal exercises.
Composition of Chinese Herbal Decoction.

All eligible participants received postoperative rehabilitation treatment and education based on the Chinese expert consensus on perioperative lung protection in thoracic surgery (2019). 17 (1) Anti-infection treatment: Antibiotics were given for the first 3 days postoperatively to prevent infection and were discontinued on the fourth day. When the patients suffered an infection, they were treated with appropriate antibiotics according to the bacteriological findings until they recovered from the infection. (2) Respiratory management: After the operation, ambroxol injection (40 mg) and doxofylline (200 mg) were given once daily intravenously, and budesonide (1mg) nebulized inhalation was given once daily until the patient was discharged. (3) Pain management: Patients were treated for pain when they presented with a numerical rating scale (NRS) score of 4 or more. The use of analgesic medications follows the three-step analgesic ladder principle. The use of opioids should be minimized. (4) Education: Patient was educated about the hazards of prolonged postoperative bed rest, mobilized for mobility out of bed as early as possible, encouraged active coughing and sputum excretion, instructed a postoperative high-protein diet, taught abdominal breathing, lip reduction breathing, use of respiratory training apparatus and other breathing exercises. Patients were asked to practice independently for at least 20 minutes a day.
The treatment lasted for a week. Patients should meet the following criteria before being discharged from the hospital: removal of the chest drainage tube, no postoperative complications, no abnormalities in laboratory tests and imaging examinations, and both the surgeon at Shanghai Pulmonary Hospital and the clinician at Yueyang Hospital assessed that the patient could be discharged.
Outcomes
Primary outcome
The primary outcome is QoL. The Quality of Life Questionnaire-Core 30 (QLQ-C30) was used to assess the QoL of patients. The QLQ-C30 consists of three components: functional scales, symptom scales, and general QoL. Functional scales include physical functioning, role functioning, emotional functioning, cognitive functioning, and social functioning. Symptom scales include fatigue, nausea and vomiting, pain, dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties. Higher scores in functional and general QoL indicate better health conditions. However, higher scores in symptom scores indicate more severe symptoms. Measurements were taken at baseline (after randomization) and after discharge conditions were met.
Secondary outcomes
Secondary outcomes included the following: 36-Item Short Form Health Survey (SF-36) scores (including patients’ Physical Functioning (PF), Role-Physical (RP), Bodily Pain (BP), General Health (GH), Vitality (VT), Social Functioning (SF), Role-Emotional (RE), Mental Health (MH), Health Transition (HT), physical and mental health summary measures (PCS&MCS) 18 ), occurrence of postoperative complications (referring to the definition and classification in the relevant consensus19 -21), coughing status (using the Leicester Cough Questionnaire (LCQ) 22 ), pain levels (using numerical rating scale (NRS) and functional activity score (FAS) for pain severity and its impact on function), and cardiopulmonary function (using 6-minute walk test (6MWT)).
6MWT was performed in accordance with guideline. 23 Patients walked for 6 minutes through a 50m long corridor at a speed they could tolerate. Patients were evaluated with Borg (Borg scale for shortness of breath) before and after the test. Patients’ walking distance before and after treatment and the difference between pre- and post-treatment distance were compared, and a positive difference was considered an improvement. Borg scores ranged from 0 to 10, with higher scores indicating more severe dyspnea and fatigue. The pre-test and post-test Borg scores of the patients were compared before and after treatment, and a negative difference was considered an improvement.
Safety assessment
Trial Safety is measured by monitoring laboratory test results and the occurrence of adverse events. Adverse events are assessed using the Common Terminology Criteria for Adverse Events (CTC AE5.0). Diagnosed postoperative complications in this trial were not considered adverse events.
Sample size
Referring to our previous research results on postoperative rehabilitation of lung cancer, with a α level of 0.05 and 0.80 power, the overall QoL score of patients at baseline after surgery was assumed to be 65.40 ± 18.37, and the post-treatment score of the intervention group was 76.64 ± 16.57, allowing for a 10% dropout rate, yielding 43 patients needed in each group, for a total of 86 patients.
Statistical analysis
The data were analyzed using SPSS 26.0. The Pearson x 2 test or Fisher’s exactness test will be used for the number of postoperative complications, the number of coughs, and the count and percentage information in the baseline data. The t-test will be used for measurement data such as SF-36, LCQ, and NRS scores. The Shapiro-Wilk test and histogram were used to assess the normality of the data before the t-test. For comparisons within groups, paired t-tests were used. The Mann-Whitney U test was used if the data did not conform to normality.
Result
Participants Enrollment
A total of 166 patients were assessed for eligibility between March 29, 2021 and September 7, 2022. 67 patients were excluded, including 63 who were not eligible for enrollment, 3 who declined to participate, and 1 who could not provide informed consent. A total of 99 patients were randomized, with 50 patients entering the intervention group and 49 patients entering the control group. Three patients in each of the two groups did not comply with the postoperative pathology, two patients in the intervention group had poor compliance with the intervention, and one patient in the control group had difficulty cooperating with the examination. Nine were eventually removed (Figure 1). Finally, 45 cases each in the intervention and control groups (48 [53.33%] males; 42 [46.67%] females; average age 60.79 [10.40] years) were included in the analysis. Table 2 shows no significant differences in demographic and clinical characteristics between the two groups of patients.

Flowchart of patient enrollment.
Demographic and Clinical Characteristics.

Note: FEV1: Forced Expiratory Volume in 1 second.
The preoperative examination of these patients revealed that only the lungs had space-occupying lesions, and the size of the lesions was within 2 cm, so the surgeon proceeded with the operation. Postoperative pathological examination indicated small cell lung cancer.
Quality of life
The results of QLQ-C30 showed that both groups of patients exhibited improvements in physical functioning, emotional functioning, and cognitive functioning after treatment. Additionally, the intervention group showed increased scores in role functioning and social functioning. The general QoL scores also increased in both groups. In terms of symptom scales, both groups showed a decrease in scores for fatigue, nausea and vomiting, pain, insomnia, constipation, and financial difficulties. The scores for dyspnea showed little change in both groups. The intervention group had a slight increase in scores for appetite loss, but the change was not significant. When comparing the two groups, significant differences were observed only in the functioning scales. The intervention group showed a significant improvement in role functioning compared to the control group (69.70 vs. 81.85; MD = 12.15, 95%CI: 2.99 to 21.32, P = .010). The intervention group also exhibited better scores in social functioning compared to the control group (71.97 vs. 82.22; MD = 10.25, 95%CI: 1.72 to 18.78, P = .019) (Table 3).
Results of QLQ-C30 Before and After Treatment Mean (SD).
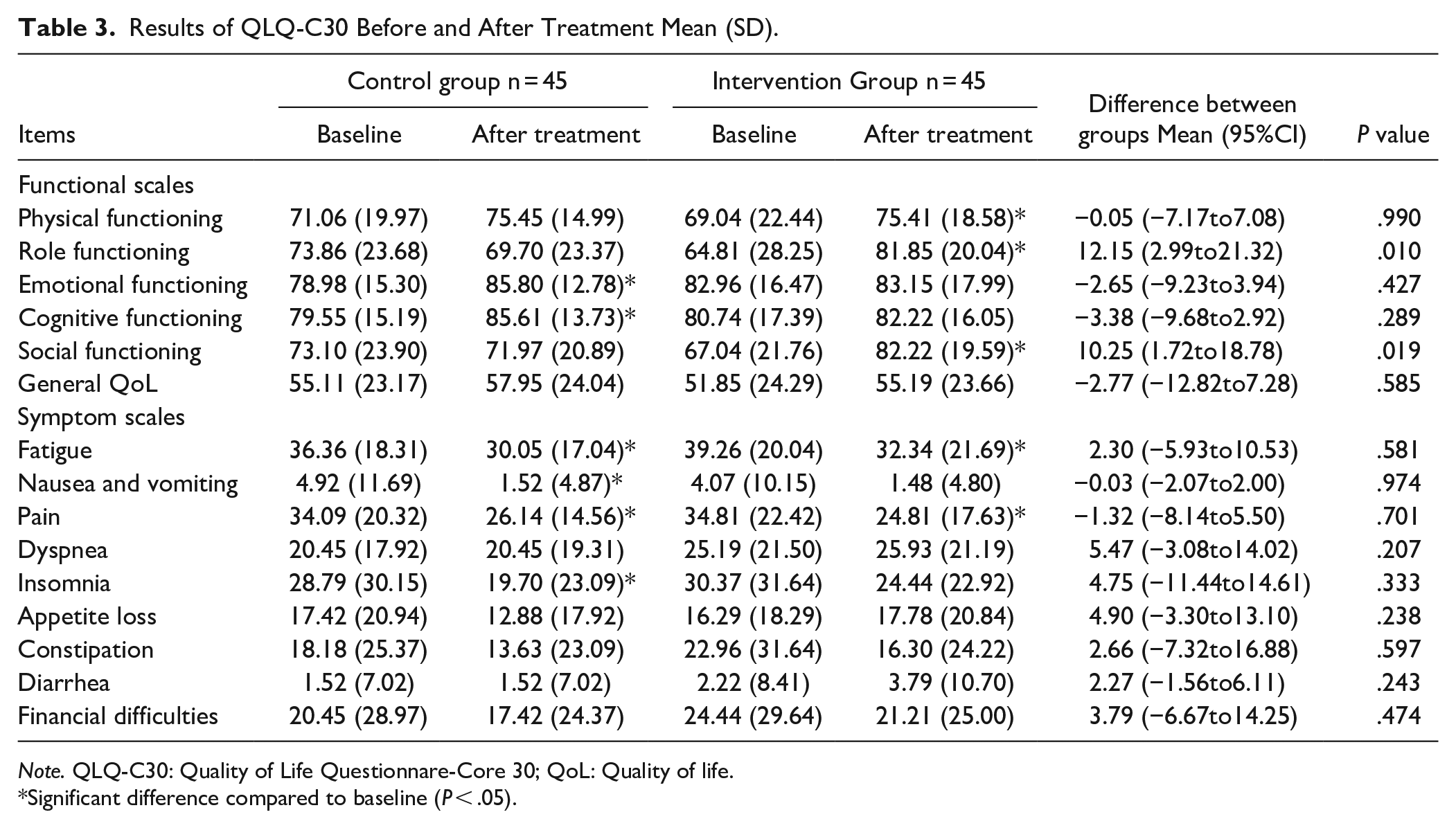
Note. QLQ-C30: Quality of Life Questionnare-Core 30; QoL: Quality of life.
Significant difference compared to baseline (P < .05).
The intervention group showed improvements in the scores of the 6 domains and PCS in SF-36 questionnaire compared to baseline. The control group also showed improvements in the scores of 3 domains compared to baseline (Table 4). VT and PCS scores improved significantly after treatment in the intervention group (P < .05), while the differences in 9 domains, PCS and MCS were not significant in the control group. After treatment, RP (19.38 vs. 44.89; MD = 25.51, 95%CI: 8.32 to 42.71, P = .004), SF (59.17 vs. 74.63; MD = 15.46, 95%CI: 5.83 to 25.09, P = .002), RE (35.00 vs. 59.63; MD = 24.63, 95%CI = 4.93 to 44.33, P = .015) and MCS (39.48 vs. 46.16; MD = 6.69, 95%CI: 0.19 to 13.18, P = .044) scores were significantly better in the intervention group than in the control group. In addition, the differences in RP (−13.12 vs. 5.44; MD = 18.57, 95%CI: 0.68 to 36.72, P = .041), VT (−3.37 vs. 4.22; MD = 7.60, 95%CI: 1.37 to 13.82, P = 0.016), and SF (−6.60 vs. 4.38; MD = 10.98, 95%CI: 0.88 to 21.08, P = .033) before and after treatment in the intervention group were significantly different from those in the control group.
Results of SF-36 and 6MWT Before and After Treatment Mean (SD).

Abbreviation: SF-36:36-Item Short Form Health Survey; PH:Physical Functioning;
RP: Role-Physical; BP: Bodily Pain; GH: General Health; VT: Vitality; SF: Social Functioning;
RE: Role-Emotional; MH: Mental Health; HT: Health Transition; PCS: Physical Health Summary Measures; MCS: Mental Health Summary Measures; 6MWT:6-minute Walk Test;
Borg: Borg scale for shortness of breath.
Δ Value after treatment-value in baseline.
Significant difference compared to baseline (P < .05).
Postoperative complication
After treatment, the postoperative complication rate in the treatment group decreased significantly (20.00%vs.44.44%; P = .013) (Table 5). Especially in terms of lung infections, the incidence rate is significantly lower than that of the control group (15.56% vs. 37.78%; P = .017).
Incidence of Postoperative Complications n (%).
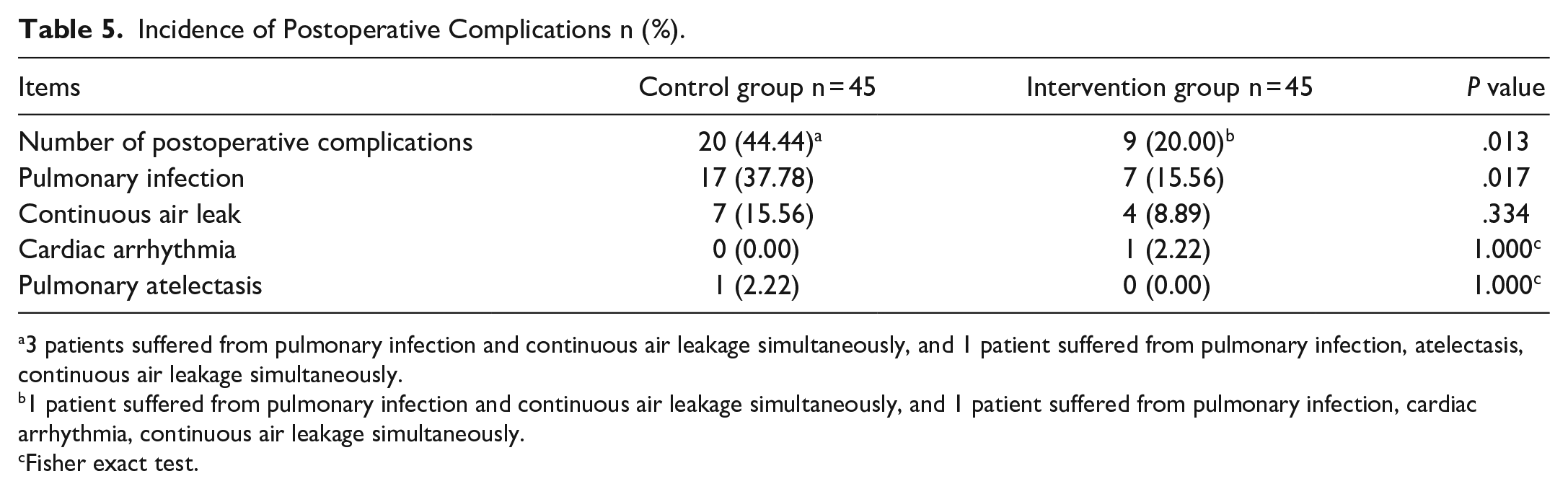
3 patients suffered from pulmonary infection and continuous air leakage simultaneously, and 1 patient suffered from pulmonary infection, atelectasis, continuous air leakage simultaneously.
1 patient suffered from pulmonary infection and continuous air leakage simultaneously, and 1 patient suffered from pulmonary infection, cardiac arrhythmia, continuous air leakage simultaneously.
Fisher exact test.
Postoperative Cough and Pain
The postoperative cough in the treatment group showed significant relief, while the control group had the opposite effect (Table 6). The psychological scores in the LCQ improved significantly in the intervention group compared with the pre-treatment scores (5.31 vs. 4.89; P < .05), while the control group showed no benefit.
Preoperative Cough Incidence and Results of LCQ before and after treatment.

Note. LCQ: Leicester Cough Questionnaire.
Δ Value after treatment-value in baseline.
Significant difference compared to baseline (P < .05).
The intervention group showed significant improvement in NRS after treatment compared with baseline (3.24 vs. 4.22; P < .05) (Table 7), but there was no significant difference between groups. In terms of pain severity, the number with severe pain decreased in both groups after treatment, but no difference was seen in the overall distribution. The number of FAS grade III-IV decreased and the number of grade I increased in both groups after treatment. The overall distribution of the comparison between groups was significantly better in the intervention group than in the control group (P = .024).
Results of NRS and FAS Before and After Treatment.

Note. NRS: Numerical Rating Scale; FAS: Functional Activity Score.
Significant difference compared to baseline (P < .05).
Cardiopulmonary Function
The 6MWT improved significantly in both groups before and after treatment (P < .05) (Table 4). After treatment, walking distance was significantly better in the intervention group than in the control group (441.80 vs. 391.18; MD = 50.62, 95%CI: 9.05-92.20, P = .018), and the difference in walking distance also improved more significantly in the intervention group before and after treatment (97.42 vs. 40.87; MD = 56.56, 95%CI: 23.39 to 89.72, P = .029). The intervention group had better Borg scores than the control group after treatment both before (0.91 vs. 1.46; MD = −0.54, 95%CI: −1.05 to 0.73, P = .029) and after (1.72 vs. 2.62; MD = −0.90, 95%CI: −1.60 to −0.20 P = .018) the 6MWT.
Safety
Forty-five of the 47 patients (95.74%) in the control group (excluding those proven not to have lung cancer) completed rehabilitation. 45 of the 46 patients (97.82%) in the test group completed treatment. The reason for failure to cooperate with rehabilitation for two patients in the control group was a request for early discharge. The reason for the patients in the intervention group was the inability to understand the exercises and the questionnaire. No patients withdrew from the trial due to inability to tolerate the treatment. No treatment-related adverse events occurred, except for diagnosed postoperative complications.
Discussion
In this randomized clinical trial, patients who received Chinese herbal decoction and Liuzijue exercises within week after lung cancer surgery recovered better than those who received conventional postoperative rehabilitation. The efficacy was mainly reflected in the improvement of some QoL indicators, the reduction of complication rate and the improvement of 6MWT results. No treatment-related adverse events or serious adverse events were experienced by patients in either group in this study. Most patients were able to complete the rehabilitation of this program. Therefore, the results of this study also support the safety of Chinese herbal decoction and Liuzijue exercises in patients with lung cancer one week after surgery.
To our knowledge, this is the first randomized controlled trial to apply TCM therapy to patients within one week of lung cancer surgery. Our study showed that the involvement of TCM in early postoperative rehabilitation can improve the QoL of patients to some extent without increasing their additional health risks and speed up their postoperative recovery. This allows post-operative lung cancer patients to return to social life and restore productivity more quickly.
In this trial, we found significant differences in QLQ-C30 scores between patients who received Chinese herbal decoction and Liuzijue exercises and those who did not. These differences were mainly observed in the role functioning and social functioning scores. Furthermore, we found that the most significant improvements in the SF-36 scores of the patients treated with TCM compared to the control group were in the RP, SF, RE and MCS. Through linear regression analysis, it was found that our treatment protocol has a significant impact on role functioning (b = 12.16, P = .01), and social functioning (b = 10.25, P = .02) in the QLQ-C30, and on the domains of RP (b = 25.51, P = .01), SF (b = 15.46, P = .00), RE (b = 24.63, P = .02), and MCS (b = 6.69, P = .04) in the SF-36. In the QLQ-C30, the scores for role functioning and social functioning primarily reflect the extent to which physical symptoms interfere with daily life. In the SF-36, the domains of RP, SF, and RE focus more on the patient's functional status and the impact of health on daily life and social adaptation, rather than just the improvement of physical health. The MCS is a reflection of the patient’s overall mental health. In previous studies, the improvement in QoL after conventional postoperative exercise (including treadmill, power bicycle, etc.) therapy was mostly physical health, but not significant for psychological aspects.24 -26 In a study of patients at 5 to 7 weeks postoperatively using a high-intensity training intervention that was maintained for 20 weeks, patients showed better improvements in functional fitness and physical and psychological scores. 27 This seems to indicate that within 1 week after lung cancer surgery, the advantages of TCM treatment are reflected in the improvement of patients’ functional fitness and social adjustment. Functional fitness and social adjustment reflect a patient’s ability to manage their daily life and work. 28 The results of this study seem to indicate that compared to traditional rehabilitation exercises, the addition of TCM treatment allows patients to return to normal life more quickly, which suggests that such a rehabilitation treatment plan not only leads to numerical improvements but also makes patients more likely to experience the effects of treatment in their daily lives.
In terms of postoperative complications, we found that the previously reported rate of postoperative complications was about 28.7% to 33.5% in lung surgery.29 -31 This is consistent with the total complication rate in this trial. However, we found that the complication rate in the control group was higher than the data in previous reports. After communicating with clinicians, we found that this may be related to the fact that patients who were at high risk for complications were more inclined to participate in this trial to gain access to postoperative rehabilitation. In other current findings, preoperative exercise has been shown to reduce the risk of postoperative complications in lung surgery. 32 The full range of ERAS procedure interventions, including postoperative respiratory training, aerobic exercise, and effective coughing, can also be effective in reducing complication rates. 33 It is worth mentioning that the results of studies that only observe the effectiveness of postoperative rehabilitation exercises in reducing postoperative pulmonary complications are still insufficient. In this trial, pulmonary infection was the most frequent of the postoperative complications that occurred. The overall complication rate and the incidence of pulmonary infections in the intervention group decreased by approximately 50% after the intervention compared to the control group. Logistic regression analysis also demonstrates that our treatment protocol can significantly impact the occurrence of pulmonary infections (OR = 0.30, P = .02) and overall complication rates (OR = 0.31, P = .02). This can inform treatment strategies for early interventions to reduce postoperative complications after lung cancer surgery. The reduction of postoperative complications means that patients can recover more quickly. For patients who need adjuvant therapy after surgery, this can help them receive subsequent treatment as soon as possible for a better prognosis. For those who do not require adjuvant therapy, it allows them to quickly move beyond the impact of surgery and achieve a higher QoL.
Previous studies have shown that cough in postoperative lung cancer patients usually occurs on the 7th day after surgery and lasts for about 5 months. 34 As for the effect of cough on QoL, LCQ scores were found to be significantly higher in the group of patients who underwent VATS sublobar resection 1 month after surgery, but there was no significant difference at months 3 and 6. 35 In this trial, the subjects were patients within 1 week after surgery. Therefore, the incidence of cough generally increased after treatment, which is consistent with previous results. From the results of this study, it appeared that cough symptoms were still in the process of developing within 1 week after surgery. Therefore, no significant differences were seen between the two groups after treatment. According to the results of this study, the cough was not effectively relieved in patients within 1 week after surgery. Perhaps the efficacy will be demonstrated after a few months, which is subject to follow-up studies.
Most patients will experience pain after lung cancer surgery. Current rehabilitation or exercise within 1 week after surgery is still ineffective for patients with pain. 36 In our study, we also found no significant differences in NRS scores and pain levels between the two groups after treatment. However, the results of FAS in the intervention group after treatment reflected the advantage. The results of the logistic regression analysis also indicate that the treatment significantly affects FAS (OR = 0.36, P = .02). FAS focuses more on the impact of pain on functional activities, so this suggested that rehabilitation within 1 week postoperatively could reduce the impact of pain on patient activity more quickly. And it may take longer for the pain severity to ease. Reducing the impact of pain on patients’ functional activities means that they can also engage in rehabilitation exercises more effectively. This also implies that daily life will not be overwhelmed by pain. Therefore, the improvement in pain control demonstrated in this study has clinical value.
The current 6MWT distance in postoperative lung cancer patients is mostly evaluated at 3 to 6 months postoperatively. Patients who underwent rehabilitation exercises for more than 1 month after surgery usually had a significant improvement in their 6-minute walking distance.36,37 However, no significant improvement in 6MWT compared to the control group was observed after 3 months postoperatively in patients who remained hospitalized with in-hospital physical therapy and rehabilitation exercises. 38 We used postoperative in-hospital rehabilitation, and the time points for evaluating the 6MWT distance were chosen before the start of rehabilitation and before discharge from the hospital. We found a significant improvement in the difference between the pre- and post-treatment 6-minute walking distance in the intervention group, as well as in the pre- and post-treatment Borg scores (both pre- and post-test). Linear regression analysis also shows that the treatment significantly improves the 6-minute walking distance (b = 50.62, P = .02). Therefore, we hypothesize that there was a short-term effect of rehabilitation within 1 week postoperatively on the improvement of 6MWT outcomes in patients. Whether the efficacy persists for several months after surgery requires further investigation. The improvement in patients’ 6MWT results indicates that they have higher expectations of gaining sufficient physical strength for daily life. Patients can also intuitively feel their own improvement during the pre- and post-treatment testing process, which gives them more confidence in their recovery and return to daily life.
In this study, a combination of herbal medicine and Liuzijue exercise were used in the treatment to explore the efficacy of integrated treatment. However, there are some limitations. Firstly, a herbal medicine placebo was not used for control in this study. Since the intervention included rehabilitation exercises, implementing blinding and placebo controls was challenging, which could not rule out potential biases. Secondly, the study design focused on the short-term effects of early rehabilitation treatment after lung cancer surgery, and it is unclear whether the treatment effects are sustainable. Therefore, further observation of patients is needed to determine long-term effects and to design additional rehabilitation plans for continued patient benefit. Additionally, the treatment plan in this study included two parts: herbal medicine and Liuzijue exercises. The study could not discern the differential effects produced by each. Future study designs should explore the separate therapeutic effects of the two treatment methods.
Conclusion
This study demonstrated that the administration of a Chinese herbal decoction and Liuzijue exercises within 1 week after lung cancer surgery significantly improved patients’ QoL, reduced the incidence of postoperative complications, and enhanced their exercise capacity. Patients treated were better able to restore social functioning and productivity.
List of abbreviations
Definition Abbreviation
Non-small cell lung cancer NSCLC
Traditional Chinese medicine TCM
Quality of Life QoL
Quality of Life Questionnare-Core 30 QLQ-C30
36-Item Short Form Health Survey SF-36
Six-minute walk test 6MWT
Leicester Cough Questionnaire LCQ
Numerical rating scale NRS
Functional activity score FAS
Enhanced recovery after surgery ERAS
Exercise-based cardiopulmonaryrehabilitation EBCR
Video-assisted thoracoscopic surgery VATS
Physical Functioning PF
Role-Physical RP
Bodily Pain BP
General Health GH
Vitality VT
Social Functioning SF
Role-Emotional RE
Mental Health MH
Health Transition HT
Physical health summary measures PCS
Mental health summary measures MCS
Borg scale for shortness of breath Borg
Footnotes
Acknowledgements
The authors thank all the trial participants and their families for their contributions. They also appreciate the medical staff of the Department of Thoracic Surgery at Shanghai Pulmonary Hospital for their assistance in the design and implementation of the treatment program for this study.
Author Contributions
Yifeng Gu, Yichao Wang, Lijing Jiao,Ling Xu contributed to the conception and design of the study. Yifeng Gu, Ao Qi, Jiaqi Li, Congmeng Zhang, Yichao Wang, Yi Liu, XueQi Tian, Jiajun Song participated in data acquisition, analysis, and interpretation. Yichao Wang, Huiling Zhou, Yong Yang, Jialin Yao, Wenxiao Yang, Lingzi Su,Xiong Qin was responsible for patient recruitment. Yifeng Gu, Yichao Wang, drafted the manuscript. Yifeng Gu, Guanjin Wu, participated in data statistical analysis. Yabin Gong, Xiong Qin, Ling Xu provided administrative, technical, and material support. All authors have reviewed and approved the manuscript.
Availability of data and materials
The data that support the findings are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author (s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author (s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Important Research and Development Program of China “Modernization of Traditional Chinese Medicine” Special Project (2023YFC3503302 ; 2023YFC3503300); Shanghai Science and Technology Commission “Science and Technology Innovation Action Plan” medical innovation research special project (No. 22Y31920400);Clinical Collaboration Pilot Project of Traditional Chinese and Western Medicine from Shanghai Municipal Health Commission (ZXYXZ-201901).
Ethical approval and patient consent
The study was approved by the Ethics Committee of Yueyang Hospital of Integrative Medicine, Shanghai University of Traditional Chinese Medicine (Yueyang Hospital), Grant No. 2020-038, and registered with chictr.org.cn (Registration number:ChiCTR2100044776) on March 27, 2021. All participants gave informed consent. They were informed that their participation in this study is entirely voluntary and they have the right to withdraw at any time without affecting their subsequent treatment. Their personal information will be kept confidential, and all published data will not include their names, residential addresses, etc