
Abstract
Background. The goal of this pilot study was to determine the magnitude and direction of intervention effect sizes for inflammatory-related serum markers and relevant health outcomes among breast cancer survivors (BCSs) receiving a physical activity behavior change intervention compared with usual care. Methods. This randomized controlled trial enrolled 28 stage I, II, or IIIA BCSs who were post–primary treatment and not regular exercisers. Participants were assigned to either a 3-month physical activity behavior change intervention group (ING) or usual care group (UCG). Intervention included supervised aerobic (150 weekly minutes, moderate-intensity) and resistance (2 sessions per week) exercise that gradually shifted to home-based exercise. Outcomes were assessed at baseline and 3 months. Results. Cardiorespiratory fitness significantly improved in the ING versus the UCG (between-group difference = 3.8 mL/kg/min; d = 1.1; P = .015). Self-reported sleep latency was significantly reduced in the ING versus the UCG (between group difference = −0.5; d = −1.2; P = .02) as was serum leptin (between-group difference = −9.0 ng/mL; d = −1.0; P = .031). Small to medium nonsignificant negative effect sizes were noted for interleukin (IL)-10 and tumor necrosis factor (TNF)-α and ratios of IL-6 to IL-10, IL-8 to IL-10, and TNF-α to IL-10, whereas nonsignificant positive effect sizes were noted for IL-6 and high-molecular-weight adiponectin. Conclusions. Physical activity behavior change interventions in BCSs can achieve large effect size changes for several health outcomes. Although effect sizes for inflammatory markers were often small and not significant, changes were in the hypothesized direction for all except IL-6 and IL-10.
Introduction
Physical activity provides multiple psychological and physiological benefits after a breast cancer diagnosis and is associated with a reduced risk of breast cancer mortality.1-4 Inflammation has been linked to health problems that may improve with physical activity and are particularly troublesome for cancer survivors; these problems include fatigue and sleep dysfunction, which have both been associated with proinflammatory cytokines.5-10 Proinflammatory cytokines have also been associated with reduced physical functioning in survivors of head and neck cancer 11 and are associated with reduced physical functioning, muscle strength, and/or muscle mass in some cancer-free groups, notably elderly people.12-15 Cytokines may also be markers for risk of breast cancer recurrence as exemplified by an association between chronic elevations of interleukin (IL)-6 and poorer prognosis in breast cancer survivors (BCSs). 16 Thus, inflammation may be a common denominator underlying both the risk of cancer recurrence and the symptoms of fatigue, sleep patterns, and reduced physical functioning.17-19
Proinflammatory cytokines could also link exercise and body composition to health outcomes such as cancer risk via the modulatory effects of adipokines. 20 Adipokines are adipocyte-derived chemokines that are overexpressed in obesity and promote the recruitment of macrophages, which in turn release proinflammatory cytokines such as tumor necrosis factor (TNF)-α, IL-6, and IL-1β. 21 Obesity is also characterized by increased production of the proinflammatory adipokine leptin and by reduced secretion of adiponectin, which has anti-inflammatory effects on macrophages. 22 Exercise interventions have been shown to cause beneficial changes in adipokines in some but not all studies of populations both with and without cancer.23-26
Physical activity behavior change interventions that focus on increasing physical activity behavior in general, as opposed to achieving a specific exercise dose, 27 result in improved health outcomes.28-35 We hypothesize that the beneficial effects of these interventions may, in part, be the result of a reduction in chronic inflammation. 36 Contracting skeletal muscle transiently releases IL-6 during acute exercise, increasing systemic levels of IL-6 up to 100-fold; this marked but transient increase in IL-6, which occurs with each bout of exercise, is theorized to trigger increased IL-10 and IL-1 receptor antagonists, resulting in a greater anti-inflammatory response.37-39
Although the effect of exercise on systemic markers of inflammation has been studied in a number of populations, few studies have specifically focused on cancer survivors. The inflammatory responses of cancer survivors to exercise may differ from those of other populations because baseline inflammation may be qualitatively or quantitatively different among individuals with chronic disease. 40 Furthermore, only a minority of the few studies in cancer survivors have used randomized exercise trials, which provide more rigorous assessment of exercise effects on health outcomes and markers of inflammation in a prospective manner. For example, a randomized controlled trial of 53 BCSs assigned to a 15-week vigorous exercise intervention or no exercise found no difference between the groups in terms of proinflammatory and anti-inflammatory cytokine production by unstimulated or phytohemagglutinin-stimulated peripheral blood mononuclear cells. 41 In another study, 28 BCSs receiving 6 months of resistance training and vigorous aerobic exercise showed no difference in lymphocytic cytokine production or plasma IL-6 as compared with 21 nonexercisers but did show a significant reduction in plasma interferon-γ at the midpoint of the exercise intervention. 42
Physical activity behavior change studies focus on creating sustained increases in regular exercise behavior, whereas exercise efficacy studies focus on health benefits in optimal settings in response to a specific exercise “dose.” 27 This difference is important because (1) behavior change studies more closely reflect the translation of exercise efficacy studies into clinical practice and (2) exercise efficacy demonstrated in an optimal setting may not occur in behavior change interventions.
Only a few physical activity behavior change studies have assessed cytokines in cancer survivors. In 1 study, for example, changes in IL-6 were not detected after participation in a behavior change intervention involving a mail-delivered diet and physical activity plan; however, this intervention achieved essentially no change in physical activity (<3 minutes per week on average). 43 Similarly, IL-6 failed to change after a 12-week program of walking for 80 minutes per week in 20 BCSs receiving hormonal therapy. 44 Another study in which BCSs on adjuvant chemotherapy were randomized to receive diet counseling with and without recommendations for home-based exercise found no change in physical activity or the proinflammatory and anti-inflammatory serum markers IL-1β and TNF receptor II. 45 However, the amount of exercise may be crucial to the development of changes in inflammation, such that the lack of increase in physical activity in these studies make results inconclusive. For example, C-reactive protein and physical activity were negatively correlated in 741 BCSs only when patients self-reported more than 6 metabolic equivalent hours per week (ie, about 90 minutes per week of moderate-intensity physical activity) in the year prior to the study assessment. 46
In one of the few studies of resistance training effects on inflammation, 38 breast and prostate cancer survivors were randomized to receive a 4-week home-based physical activity behavior change intervention using pedometers and resistance bands versus the control condition. This study reported a significant negative effect of the intervention on serum IL-6 with no significant difference between the study conditions with regard to TNF-α. 47 In non–cancer populations, C-reactive protein significantly declined after a 1-year resistance training intervention in 28 overweight women. 48
In summary, exercise efficacy and behavior change studies in cancer survivors are consistent with prior studies in healthy adults,38,39 in that exercise may change serum cytokines without changing cytokine release from blood mononuclear cells in vitro. However, none of the cancer survivor exercise studies has detected an increase in systemic IL-6 caused by muscle release of IL-6, as has been reported for healthy adults.38,39 This discrepancy could be related to the focus of cancer studies on chronic training rather than on acute exercise bouts, which transiently increases IL-6 primarily in the first 24 hours after the acute exercise bout. 49 In addition, previous physical activity behavior change studies often may not have achieved exercise levels sufficient to alter inflammatory markers. These issues highlight our need for a better understanding of how physical activity behavior change interventions affect the complex patterns of proinflammatory and anti-inflammatory cytokines and adipokines in BCSs and how this modulation of systemic inflammation contributes to health concerns such as fatigue and sleep dysfunction.
In preparation for a larger prospective study evaluating the potential inflammatory mechanisms of physical activity behavior change intervention effects, we chose study outcomes based on the biological framework described in Figure 1. We hypothesized that exercise reduces chronic systemic inflammation (eg, proinflammatory serum cytokines) directly and indirectly through changes in body composition, in turn attenuating fatigue, improving sleep quality, and reducing risk of cancer recurrence. The primary goal of the current study was to obtain preliminary estimates of the magnitude and direction of the exercise intervention effects on serum markers of inflammation (cytokines and adipokines) and relevant health outcomes (cardiorespiratory fitness, muscle strength, body composition, fatigue, and sleep dysfunction) in preparation for a subsequent trial that will be powered to detect changes in serum cytokines and adipokines with the intervention. In particular, we determined preliminary effect sizes to identify those outcomes that are most sensitive to modulation by the intervention and to estimate sample size requirements for subsequent use of these outcome measures. Our intervention goal was 150 minutes of moderate-intensity physical activity per week (ie, equivalent to 7.5 to 12.5 metabolic equivalent hours per week), which we hypothesized would be sufficient to affect systemic inflammation, as assessed using serum markers associated with cancer risk, fatigue, and/or sleep dysfunction (see Table 1). Specifically, we hypothesized that as compared with the usual care group (UCG), the physical activity behavior change intervention group (ING) would have (1) lower serum concentrations of proinflammatory cytokines (eg, TNF-α, IL-1β, IL-6, and IL-8) and inflammatory-related markers associated with excess adiposity (eg, leptin) and (2) higher levels of anti-inflammatory cytokines (eg, IL-10) and markers associated with lower body weight or fat (eg, adiponectin). In addition, we expected improvements in all health outcome measures in the ING as compared with the UCG.

Chronic exercise training, inflammation, and related outcomes: theoretical biological framework.
Inflammatory Markers: Health Outcome Associated With Higher Serum Levels and Expected Change With Chronic Physical Activity.

Abbreviations: IL, interleukin; TNF, tumor necrosis factor; HMW, high molecular weight.
Certain cytokines may have both proinflammatory and anti-inflammatory effects (eg, IL-6), 60 but only outcomes associated with the primary action are listed.
Does not include muscle cytokine levels in response to acute exercise bouts, which may differ from serum levels after exercise training.
Contrary to the other cytokines listed, IL-10 reduces non–rapid-eye-movement sleep possibly improving sleep quality. 50
Methods
Setting, Participants, and Study Design
The local institutional review board approved the study, and all participants provided informed consent before beginning the study. Eligible participants were women who were stage I, II, or IIIA BCSs between the ages of 18 and 70 years. Other eligibility criteria included the following: not currently receiving (and not planning to receive during the study duration) chemotherapy or radiation therapy, ≥8 weeks postsurgery, English speaking, and medical clearance for participation provided by physician. Exclusion criteria were as follows: dementia or organic brain syndrome; medical, psychological, or social characteristic that would interfere with ability to fully participate in study activities (eg, psychosis and schizophrenia); contraindication to participation in a regular physical activity program; metastatic or recurrent disease; unable to ambulate; engaged in ≥60 weekly minutes of vigorous physical activity or ≥150 weekly minutes of moderate plus vigorous activity during the past month (based on self-report); anticipated undergoing elective surgery during the intervention that would interfere with participation (eg, breast reconstructive surgery); and did not live or work within 50 miles of the study site.
This 2-arm, randomized controlled pilot study compared an ING with a UCG. Measurements were obtained at baseline (preintervention, M0) and 3 months (postintervention, M3). Randomization was based on computer-generated numbers, performed in blocks of 4, and revealed in the order in which participants completed baseline testing.
Intervention and Usual Care
The physical activity behavior change intervention was adapted from the previously reported BEAT Cancer program61-63 by adding strength training using resistance bands. The intervention goal was to gradually increase each participant’s physical activity to 150 weekly minutes of exercise that was of or more than moderate intensity and 2 sessions per week on nonconsecutive days of resistance training (ie, up to 20 repetitions of 8 different exercises using each of the major muscle groups). Participants were tapered from supervised exercise sessions with an exercise specialist to home-based, unsupervised exercise over the first 6 weeks of the intervention. They were given personal heart rate monitors to facilitate achieving target exercise intensity. For behavioral support, participants attended 6 discussion group sessions with a clinical psychologist over the first 9 weeks of the intervention and met with the exercise specialists for a face-to-face “update” counseling session every 2 weeks in the final 6 weeks of the intervention.
Because the focus of the intervention was behavior change rather than exercise efficacy, 27 the UCG received written materials from the American Cancer Society, which included general information about physical activity and nutrition after a cancer diagnosis but did not include specific recommendations regarding exercise behavior. Participants were told that they could receive the intervention at the end of the study, free of charge.
Measures
A self-administered survey was used to assess age, race/ethnicity, marital status, smoking history, alcohol consumption, and medical history. Bilateral arm circumferences were measured on all participants at the midpoint between the shoulder and the elbow (an average of 3 measurements) to monitor for potential increases related to lymphedema. Because carbohydrate ingestion may influence cytokine response to exercise, 36 a 3-day diet record was done prior to the blood draw to determine if between-group differences requiring statistical adjustment existed.
Adherence to the intervention physical activity recommendations was measured with 7-day MTI/ActiGraph accelerometer monitoring (aerobic) and exercise logs (resistance). Physical activity intensity cut-points were as follows: light activity = 0 to 1952, moderate activity = 1953 to 5724, hard activity = 5725 to 9468, and very hard activity >9468.64,65 Resistance training adherence was recorded by exercise specialists during supervised sessions. Home-based sessions were recorded by the participants; study staff reviewed the log sheets with participants during supervised and follow-up sessions.
A submaximal treadmill test using the Naughton protocol estimated fitness. 66 Muscle strength was measured using a back/leg dynamometer. Body mass index (BMI) was calculated from height and weight measured by trained staff. Waist-to-hip ratio was measured using a nonstretching tape measure with the participant standing with abdomen relaxed and arms at the sides with no clothing at the waist and only undergarments at the hip. Percentage body fat was measured by bioelectric impedance (ie, Quantum X by RJL Systems) in a standardized fashion (ie, same time of day for each measurement after a ≥4 hour fast). Fatigue intensity and interference experienced during the past week was measured with the multidimensional fatigue scale (ie, Fatigue Symptom Inventory; a higher score indicates greater fatigue). 67 The following 2 subscales are reported: (1) fatigue intensity (mean of 4 items, 1-10 scale) and (2) fatigue interference (mean of 6 items, 1-10 scale). Self-reported sleep dysfunction was measured using the Pittsburgh Sleep Quality Index (PSQI), which was scored according to published protocol (ie, higher score indicates greater sleep dysfunction). 68 Sleep latency and efficiency were measured objectively using the same accelerometer used for measuring physical activity by transferring it to the wrist when in bed. The participant recorded time in and out of bed on a record sheet.
Blood Sampling Rationale, Methods, and Assays
The Luminex methodology was chosen because it allows for simultaneous measurement of multiple analytes, thereby reducing sample volume requirements and cost related to labor and reagents compared with other single-analyte methods such as enzyme-linked immunosorbent assays (ELISAs). Serum rather than plasma was assayed based on prior comparisons of Luminex cytokine assays with ELISA measurements, which showed good correlation in serum69,70 but not in plasma. 71 In addition, cytokine levels have been reported to be higher in serum compared with plasma samples among breast and prostate cancer patients. 47
Participants were instructed to abstain from physical activity, smoking, and alcohol; take all medications prescribed for regular daily use; and not take sporadic or “as needed” medications for 24 hours before the blood draw. Participants were asked to fast for 12 hours before the blood draw, which was performed by an experienced phlebotomist between 7:45 and 10:00
Data Analysis
The intervention and UCGs were compared on demographic, medical, and carbohydrate ingestion outcomes at baseline with independent t test or χ2, depending on the nature of the variable. For magnitude and direction of the intervention effect, M0 was subtracted from M3 for a difference score with the ING and UCG compared with the independent t test. An intent-to-treat analysis was performed. The following ratios were calculated to examine the relative proinflammatory to anti-inflammatory patterns: IL-6:IL-10, IL-8:IL-10, and TNF-α:IL-10. The level of significance was set at a P < .05. Because of the pilot nature of the study and limited available data related to cytokine response to a physical activity behavior change intervention for BCSs, we report the effect sizes regardless of statistical significance. Effect sizes were calculated by dividing the between-group difference by the standard deviation of the between-group difference. Effect sizes were defined as small (0.2), medium (0.5), or large (0.8). 74
Results
Participant Flow and Characteristics
Participants were recruited from June 2008 through April 2009. Figure 2 provides the participant flow through the study. Complete M0 assessments were obtained on all 15 intervention participants. Although all usual care participants provided baseline data, the serum sample from one of the usual care participants was not usable because of excessive hemolysis. This participant refused to have repeat phlebotomy done and withdrew from the study. At M3, 1 participant in the ING did not wear the accelerometer long enough to collect 4 valid days of data, and 1 participant in the UCG did not return a completed survey.

Participant recruitment, allocation, and retention by study group (M0 = month 0, M3 = month 3).
Baseline characteristics for all participants combined and stratified by group assignment are provided in Table 2. No statistically significant differences between the study groups at baseline were noted for demographic, medical, and carbohydrate ingestion outcomes with the exception of the UCG, who had more mean years of education as compared with the ING at baseline (16.3 ± 2.5 vs 14.1 ± 2.9, P = .047; Table 2).
Baseline Characteristics for Participants (Overall and by Group Allocation) a .
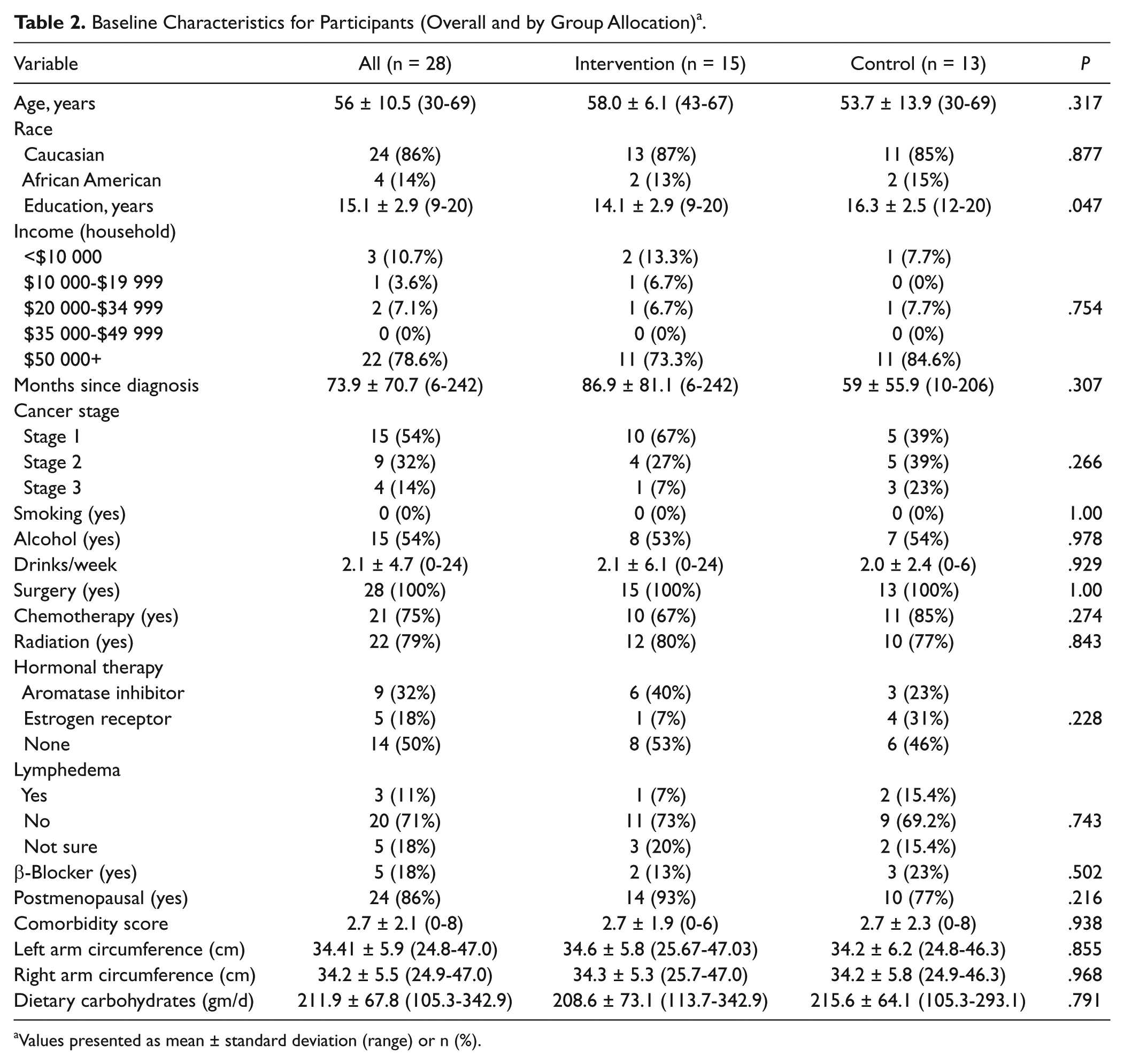
Values presented as mean ± standard deviation (range) or n (%).
Exercise Adherence, Protocol Deviations, and Adverse Events
The 14 participants completing the intervention attended 100% of the supervised exercise sessions (168/168), 100% of the update sessions (42/42), and 73% of the group sessions (61/84). With regard to adherence to aerobic physical activity (based on accelerometers), improvement was noted in the weekly minutes of physical activity that was greater than moderate intensity for the ING versus the UCG (ie, +45.4 vs −37.7; mean between-group difference = +83.1; effect size, d, = 0.76; P = .097). At M3, the mean for physical activity greater than moderate intensity in the ING was 198.4 ± 111.7 minutes per week. With regard to resistance training, the 12 participants in the ING providing M3 data completed 21 of the 24 possible resistance exercise sessions over the 12-week period (87.5%) and reported a weekly average of 1.8 sessions per week. During the final 4 weeks of the intervention, the intervention participants completed 5 of the 8 sessions (63%; weekly average = 1.3 sessions).
No protocol deviations occurred. In all, 3 adverse events were identified (2 related and nonserious in the ING and 1 unrelated and serious in the control group). No significant change in arm circumference for the ING versus UCG was noted (left arm: intervention = −0.3 cm vs usual care = +0.7 cm, between-group difference = −1.0 cm, d = −0.7, P = .145; right arm: intervention = −0.1 cm vs usual care = +0.2 cm, between-group difference = −0.3 cm; d = −0.2; P = .691).
Health Outcomes
The magnitude and direction of the effect sizes for the health outcomes are provided in Table 3. Fitness and PSQI (self-reported) sleep latency demonstrated statistically significant effect sizes, all in a beneficial direction (ie, fitness increased and self-reported sleep latency decreased). Although not statistically significant, a large positive effect size was noted for muscle strength, with medium to large negative effect sizes noted for BMI, percentage fat mass, PSQI daytime dysfunction subscale, and global PSQI score. Only small effect sizes were found for fatigue and sleep efficiency.
Physical Activity, Muscle Strength, Body Composition, Fatigue, and Sleep Dysfunction for Intervention Versus Usual Care Group a .

Abbreviations: M0, month 0 (baseline); M3, month 3; SD, standard deviation; d, effect size.
Data based on study participants completing both baseline and 3-month follow-up.
Possible range = 1 to 10.
A higher score indicates greater sleep dysfunction; possible range for subscales = 0 to 3 and global dysfunction = 0 to 21.
Inflammatory-Related Serum Markers (Cytokines and Adipokines)
Except for IL-1β, all cytokines evaluated were detectable in ≥95% of M0 and M3 samples (Table 4). Because of the high percentage of samples with concentrations below the level of detection for IL-1β, statistical comparisons were not performed. For the remaining cytokines, samples with concentrations below the level of detection were assigned a concentration of one half the detection limit. This approach is unbiased when the percentage of measurements below the level of detection is less than 10%. 75 Leptin, high-molecular-weight adiponectin, and total adiponectin were detectable in 100% of samples.
Number (Percentage) of Samples With Detectable Cytokine Levels Stratified by Assessment Time Point.

Abbreviations: IL, interleukin; TNF, tumor necrosis factor.
One participant’s month 0 sample was not useable as a result of hemolysis. Therefore, the total number for month 0 assays was 27.
The magnitude and direction of the effect sizes for the inflammatory-related serum markers are provided in Table 5. The intervention was associated with a large effect size reduction in leptin as compared with the UCG and with a medium to large effect size increase in IL-6. Small to medium effect size changes occurred as follows: decrease in IL-10, increase in high-molecular-weight adiponectin, decrease in total adiponectin, and decreases in the IL-6 to IL-10, IL-8 to IL-10, and TNF-α to IL-10 ratios.
Inflammatory-Related Serum Markers for the Intervention Versus Control Group a .

Abbreviations: M0, month 0 (baseline); M3, month 3; SD, standard deviation; d, effect size; IL, interleukin; TNF, tumor necrosis factor; HMW, high molecular weight.
Data based on study participants completing both baseline and 3-month follow-up.
Discussion
Our physical activity behavior change intervention in BCSs increased physical activity to a level that was sufficient to cause significant improvements in fitness, sleep latency, and serum leptin concentrations as compared with usual care. Although not statistically significant, medium to large effect sizes in a beneficial direction occurred for muscle strength, BMI, and percentage body fat for the ING compared with the UCG; smaller effect sizes were noted for some but not all dimensions of fatigue and sleep dysfunction. The magnitude of intervention effects on inflammatory markers and ratios of proinflammatory to anti-inflammatory cytokines were generally small, although changes in IL-6 and leptin were relatively large. The directions of these effect sizes were as hypothesized with the exception of an increase in IL-6 and decreases in IL-10 and adiponectin in the ING compared with the UCG.
The changes we detected in serum markers of inflammation suggest hypotheses and patterns that merit assessment in trials that are powered to detect small effect size changes (eg, 400 study participants in each study group allocation would be required to detect an effect size of 0.2 with a power of 80 and P < .05 74 ). Given that 800 participants would require a costly, multicenter study, a future trial could use a number of strategies to increase effect sizes and improve study power. For example, enrolling a more homogeneous sample (eg, similar levels of fatigue, amount of sleep dysfunction, time since cancer diagnosis, and age) would reduce variability in response to the intervention, resulting in greater study power. Also, limiting future trials to survivors with higher levels of fatigue and sleep dysfunction at baseline would avoid the chance of smaller effect sizes caused by a floor effect. Related to the hypothesized pathways in Figure 1, our intervention may have influenced inflammation, fatigue, and sleep primarily through the direct effect of exercise on chronic systemic inflammation rather than through an indirect effect through a change in body composition (ie, we found minimal changes in body composition in the ING). However, lengthening the intervention beyond 3 months would facilitate greater changes in body composition and possibly increase the effect size changes related to inflammation.
Our high percentage of samples with IL-1β concentrations below the level of detection is consistent with other studies. For example, IL-1β was not detectable in 79% of breast cancer patients on active treatment (ie, chemotherapy) 76 or in 91% of breast cancer patients with metastatic disease, 77 suggesting that IL-1β may not increase as a function of therapy or disease severity. The high percentage of individuals with nondetectable IL-1β in our study population could also reflect relatively good physical functioning in our participants (ie, they were capable of engaging in moderate-intensity exercise). Consistent with this possibility, others detected IL-1β in only 0% to 36% of “healthy” participants when samples were analyzed with multiple different multiplex and ELISA kits, including the same high-sensitivity Luminex assay used for the current study. 78 Finally, we opted to measure IL-1β based on its association with poor physical functioning and sleep regulation.11,50 However, poor sleep quality was not an inclusion criterion for this study.
Our effect size increase of 0.76 in weekly minutes of physical activity is consistent with the significant improvement in fitness with the intervention. With regard to resistance exercises, adherence declined during the later weeks of the intervention, which may explain, in part, the lack of significant increase in muscle strength. The significant effect size decrease in leptin was the result of both a decrease in the ING and an increase in the UCG. This may be explained, in part, by the patterns of change in physical activity in the study groups (ie, increased in the ING and decreased in the UCG) and the trends noted for BMI, waist-to-hip ratio, and percentage body fat. These results are consistent with a previously reported association between lower leptin and higher self-reported physical activity in a cross-sectional study of BCSs. 25 However, we found a significant change in leptin in our behavior change intervention study, whereas an exercise efficacy intervention did not, perhaps because the latter study had an exercise target of 90 minutes per week compared with our target of 150 weekly minutes. 26 Consistent with this, 2 recent randomized exercise efficacy studies in postmenopausal women found significant reductions in leptin after 12 months of 225 weekly minutes of exercise.23,24 The decrease in leptin represents a valuable health outcome because of its association with lessened risk of breast cancer recurrence and its potential as a therapeutic target. 57
The measured cytokines did not change in a consistently proinflammatory or anti-inflammatory manner, perhaps because some cytokines (eg, IL-6) 79 have both proinflammatory and anti-inflammatory properties. The proposed mechanism of exercise effects on cytokines is through a transient increase in IL-6, which is consistent with our effect size of +0.7. We did not expect to find an increase in IL-6 because such changes occur primarily within 24 hours of an acute exercise bout, and our participants did not exercise for at least 24 hours before the blood draw. Perhaps over time, adequate, repeated, and consistent bouts of exercise result in a higher steady-state level of serum IL-6 that contributes to a reduction in chronic inflammation via the anti-inflammatory properties of IL-6. Our positive effect on IL-6 differs from a negative effect reported in an intervention study using a home-based pedometer and resistance bands. 47 This inconsistency may be a result of the fact that cytokine response to exercise may vary based on gender and/or treatment status (ie, on or off primary cancer treatment). Moreover, the exercise intensity and amount achieved in the previous study may have been lower than that of our study because of minimal contact time with study staff (only 1 instructional session) and use of perceived exertion rather than target heart rate to ensure adequate exercise intensity. However, our ratios of proinflammatory to anti-inflammatory cytokines showed negative effect sizes, suggesting that the exercise intervention may change the cytokine balance in favor of an overall reduction in inflammatory tone. Such a change in the balance of proinflammatory and anti-inflammatory cytokines could account for the inconsistency in the epidemiological evidence regarding reduced breast cancer recurrence and mortality with exercise, 1 despite a poorer prognosis in patients with chronic elevations of IL-6. 16
Although the intervention showed little effect on fatigue, a small to medium effect size reduction (ie, d = −0.4) in the PSQI daytime dysfunction subscale is similar to the weighted mean effect size change in fatigue with exercise of −0.54 reported in a recent review. 4 This suggests that the intervention may improve daytime somnolence not detected by the fatigue measure used. Also, the significant improvement in self-reported sleep latency coupled with the small to medium effect size improvements in the self-reported global sleep score and accelerometer latency suggest that a future, larger trial has the potential to examine the role of the ratio of proinflammatory to anti-inflammatory effects in mediating changes in sleep dysfunction that may occur with a physical activity behavior change intervention for BCSs.
Although exercise efficacy studies have reported reductions in leptin with exercise training in postmenopausal women, 24 our study is unique in reporting that BCSs show beneficial changes in response to an overall increase in physical activity, as opposed to achieving a specific exercise dose. Our findings are reassuring, given the real-world challenges of achieving specific exercise amounts in broader populations after rigorous randomized exercise efficacy trials identify benefits of specific exercise regimens. Our study is also one of few that describe cytokine responses to a physical activity behavior change intervention in BCSs. As reviewed in the introduction, behavior change intervention studies have been inconsistent with regard to changes in cytokine markers of inflammation, possibly because of insufficient increases in physical activity. The magnitude and direction of our effect size changes support the possibility that a physical activity behavior change intervention can affect inflammation and related health outcomes. Our study also provides valuable effect size data for power calculations for future trials that may use similar physical activity interventions, inclusion/exclusion criteria, and assay methods. A recent review of exercise and immune function concluded that future studies are needed to identify those inflammatory mediators that are most sensitive to exercise. 80 Our study suggests that adipokines may be the most sensitive markers. With regard to serum cytokines other than adipokines, IL-6 may be the most sensitive, but its complex effects (ie, proinflammatory vs anti-inflammatory properties) may complicate the interpretation of changes.
Because of its small sample size and lack of study power, our study does not allow definitive conclusions about specific intervention effects. Also, budgetary constraints prevented the measurement of percentage body fat with dual X ray absorptiometry, which is considered the gold standard. Finally, the 2 study groups differed significantly with regard to education, but the small sample size prevented us from addressing this difference statistically. However, we expect that the effect of education differences on the study outcomes would be minimal, with the potential bias being toward a smaller effect size change, given that higher education may be associated with greater physical activity adherence. 81 If that were the case, the adjusted effect size changes would be larger than those we report.
In conclusion, our data show that physical activity behavior change interventions aimed at improving exercise adherence without reaching a specified exercise dose (as in an exercise efficacy study) can have statistically significant beneficial effects on cardiorespiratory fitness, sleep latency, and serum leptin concentrations. The direction and magnitude of changes in serum markers in our study suggest patterns relevant to the interactions of physical activity, inflammation, and fatigue and sleep dysfunction and warrant assessment in larger trials. Further delineating the effects of a physical activity behavior change intervention on individual inflammatory markers and their patterns of change in BCSs has the potential to increase our understanding of how such interventions might contribute to symptom management.
Footnotes
Authors’ Note
Clinical trial registration: ClinicalTrials.gov NCT00640666.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by the Simmons Cancer Institute at Southern Illinois University School of Medicine Translational Research Award. Drs Rogers, Hopkins-Price, Vicari, Rao, and Verhulst receive salary support from National Cancer Institute Grant 1R21CA135017. Drs Rogers, Hopkins-Price, Vicari, and Verhulst also receive salary support from National Cancer Institute Grant 5R01CA136859. Dr Courneya is supported by the Canada Research Chairs Program and National Cancer Institute Grant 5R01CA136859.