
Abstract
Introduction. The purpose of this study was to determine the influence of Chinese medicine in a Chinese medicine ward (CMW) on weight loss and quality of life in patients with head and neck (HN) cancers during radiotherapy (RT). Methods. From 2006 to 2010, patients with HN cancers hospitalized in the CMW for ≥10 days during RT were included. Outpatients with HN cancers from the Department of Radio-oncology were also enrolled. Body weight was evaluated near the beginning and the end of RT. Quality of life was assessed near the end of RT. Results. Sixty-nine inpatients and 74 outpatients with radiation doses ≥60 Gy were included. Inpatients had significantly lesser weight loss than outpatients (P = .016) during RT or chemoradiation. Patients hospitalized for ≥40 days had lesser weight reduction than those hospitalized for a shorter period (P = .025). In the quality-of-life assessment, inpatients had significantly lower score for the item “lack of appetite” on the M.D. Anderson Symptom Inventory than outpatients (P = .002). Conclusions. Patients with HN cancers receiving hospitalization and Chinese medicine in the CMW had lesser weight loss than outpatients. By monitoring the patient’s condition to adjust the prescription of Chinese medicine, this treatment minimized the weight loss resulting from RT or chemoradiation potentially because of a better functioning of appetite. Patients receiving integrated medicine early showed better results than those starting this treatment later.
Introduction
In 2009, the crude death rate of oral cancer ranked sixth among all cancers reported by the Department of Health in Taiwan. From 1975 to 2001, the incidence of head and neck (HN) cancers at sites such as the tongue, tonsil, nose, salivary glands, thyroid, bone, and soft tissue increased in the United States. 1 In the European community, squamous cell carcinoma of the upper digestive tract is the fourth most common cancer type among men. 2 Treatment plans for patients with HN cancers largely depend on tumor stage, location, and general health condition, and the most common treatment modalities are surgery, radiotherapy (RT), combined surgery and RT, and concomitant radiochemotherapy (CCRT) for more advanced cancers. Despite new techniques in treatment, therapies for HN cancers still have profound effects on the facial appearance of patients, their capacity to communicate, and their ability to eat. Patients who receive RT typically experience acute toxicity, such as mucositis, xerostomia, dysphagia, and alteration of taste or smell, and these adverse effects often lead to poor nutritional intake and malnutrition. Moreover, the influence of a preceding operation often adds to the acute morbidity induced by RT. Concurrent chemotherapy and radiation, in most cases cisplatin based, is associated with increased acute toxicity and higher prevalence of weight loss during therapy. 3 According to a previous study, patients with HN cancers often lose a significant percentage of weight, which correlates with the complication rate. 4 Malnutrition is a common problem in patients with HN squamous cell carcinoma and is present in about 50% of these patients. 5 Since weight loss has been reported to be an important prognostic indicator of malnutrition in most cancers in the Western world, many researchers have focused on how to maintain or prevent weight loss in patients with HN cancers.4,6,7
Complementary and alternative medicine (CAM) has gained popularity among cancer patients in the past years, 8 and its use dramatically increases after a diagnosis of HN cancer (ie, 8-fold increase in the use of herbs). 9 However, only limited information is available at the moment about the use of CAM, especially traditional Chinese medicine, to prevent weight loss in patients with HN cancers during oncological treatment. Therefore, it was the aim of this study to compare the weight loss and quality of life during RT between patients with HN cancers who did and did not receive individualized treatment with traditional Chinese medicine in a Chinese medicine ward (CMW).
Methods
A retrospective cohort study on weight changes and quality of life during RT in patients with HN cancers was carried out.
Study Population
In Taiwan, the first CMW was established at the Chang Gung Memorial Hospital, Taoyuan, in 2006. The inpatient services of the CMW are mainly for patients undergoing RT with/without chemotherapy for HN cancer, breast cancer, and colon cancer. The treatment plan during hospitalization was to relieve the side effects of RT or chemotherapy by Chinese medicine. All patients in this study had been informed the availability of self-paid hospitalization in the CMW, and they chose to be hospitalized or not by themselves. From June 2006 to May 2010, patients with HN cancers who were hospitalized in the CMW for ≥10 days at their own request and expense during RT at Chang Gung Memorial Hospital, Linkou, were included in this study as an intervention group. Patients were transported by bus between these 2 branches (about 15 minutes) on weekdays for RT with/without chemotherapy. Since RT is an important modality in the treatment of HN malignancies, we also included outpatients with HN cancers from the Department of Radio-oncology of the Chang Gung Memorial Hospital, Linkou, as a control group. Radiation doses for all patients included in this study were ≥60 gray (Gy), and patients were treated by different methods such as RT, combined surgery and RT, or CCRT according to their stage, tumor location, and general health condition. Data on weight changes before and after radiation were recorded, and the number of tube feedings and quality of life at the end of RT was also evaluated. Inpatients who were hospitalized in the CMW for ≤10 days and outpatients in the control group who took herbal medicine during this study were excluded, and patients who could not have their body weights measured and those who were younger than 18 years or older than 80 years were also excluded.
Chinese Medicine Intervention
Inpatients who were hospitalized in the CMW received integrated and individualized Chinese medicine intervention; that is, each was given a diagnosis according to the presenting pattern(s), and an individualized herbal treatment, oral or topical, was given for that pattern according to the theory of traditional Chinese medicine. Since RT or CCRT is an intense treatment, it affects each patient’s constitution nearly the same way, giving rise to intense Fire that wears qi and damages yin. For intense Fire, manifesting in dermatitis, stomatitis, or other mucomembranous reaction, herbs to clear Heat and drain Fire were prescribed. For example, we used Dahurian Angelica (bai zhi), Aloe (lu hui), Rhubarb (da huang), Phellodendron (huang bai), Coptis (huang lian), and Scutellaria (huang qin). For qi vacuity, manifesting in anorexia, poor digestion, or fatigue, we gave inpatients Astragalus (huang qi), American Ginseng (xi yang shen), Xiang-sha-liu-jun-zi-tang (Costusroot and Amomum Six Gentlemen Decoction), Shen-ling-bai-zhu-san (Ginseng, Poria, and White Atractylodes Powder), or Bu-zhong-yi-qi-tang (TJ-41: Center-Supplementing Qi-Boosting Decoction). For insufficiency of yin, with xerostomia or dysphagia, we prescribed formulae such as Zeng-ye-tang (Humor-Increasing Decoction) or Sha-shen-mai-dong-tang (Adenophora/Glehnia and Ophiopogon Decoction). We list some common patterns with clinical symptoms and choice of herbal medicine and its dosage in Table 1. In addition, doctors occasionally used acupuncture to adjust qi in the channels or network vessels of patients.
Correlation Among Patterns, Clinical Presentations, and Prescribing Examples

All oral herbal medicines are concentrated extract powders, which are made by the pharmaceutical companies Sun Ten, Sheng Chang, Chuang Song Zong, and Ko Da in Taiwan. The powder is divided into 3 packages for giving 3 times a day after meal.
Baizhi Luhui gel, composed of Dahurian Angelica and Aloe, is made by the Formosa Biomedical Technology Corporation in Taiwan. The gel is usually applied topically 2 or 3 times a day.
Nutrition Intervention
Both inpatients and outpatients received the usual care of clinical practice in the Chang Gung Memorial Hospital, that is, education by the nurses of the Department of Radio-oncology, provision of commercial liquid nutrition supplement samples, and basic nutritional knowledge. There was no nutrition assessment, no individualized nutrition advice, and only occasionally dietetic consultations if patients requested. In this retrospective cohort study, we simplified by monitoring the body weight changes of both inpatients and outpatients with HN cancers instead of monitoring the nutritional status and food intake, since such data were not collected in the usual clinical practice.
Body Weight Measurement
Body weights of both inpatients and outpatients were recorded near the beginning and end of RT on the same electronic weigh scales. The percentage of weight change was calculated by subtracting the pretreatment weight from the posttreatment weight and divided by the pretreatment weight. Age, gender, and height were recorded at the first visit. A nasogastric tube was inserted whenever clinically indicated, such as when patients had severe difficulty in swallowing, and the number of tube feedings was recorded at the end of the study.
M.D. Anderson Symptom Inventory Core Assessment
The M.D. Anderson Symptom Inventory (MDASI) is a brief measure of the severity and impact of symptoms produced by the cancer itself or the disease treatment, which includes items that report the “sensory” dimension of symptoms (intensity, or severity) and the “reactive” dimension of symptoms (interference with daily function). Severity is assessed for 13 core MDASI symptom items (pain, fatigue, nausea, disturbed sleep, emotional distress, shortness of breath, lack of appetite, drowsiness, dry mouth, sadness, vomiting, difficulty remembering, and numbness or tingling) and for 6 interference items (general activity, mood, walking ability, normal work, relations with other people, and enjoyment of life). 10 The MDASI has proved to be a useful tool for symptom surveys, clinical trials, and patient monitoring, and its core items account for the majority of symptom distress reported by cancer patients in active treatment and those who are followed-up after treatment. 11 Higher scores on the MDASI reflect worse functioning. Authorization to use the traditional Chinese character version of the MDASI Core was obtained from the M.D. Anderson Cancer Center, University of Texas. Therefore, this version was used to assess patients with HN cancers near the end of RT.
Statistical Analysis
The percentage of change in body weight was expressed as mean ± standard deviation. The paired t test was used to examine the weight changes of patients during RT with/without chemotherapy in the same group. Changes in body weight and MDASI were compared by independent t test between inpatient and outpatient groups. Statistical significance was assumed at P < .05. The Statistical Package for the Social Sciences (SPSS, Chicago, IL), version 17.0 for Windows, was used for data analysis. The χ2 test was used to compare differences in tumor staging and location, mode of treatment, and number of tube feedings between groups.
Ethical Considerations
The Committee on Research Ethics of the Chang Gung Memorial Hospital in Taiwan approved the study (No: 98-3179B, 99-2107C).
Results
Characteristics of Inpatients and Outpatients
Between June 2006 and May 2010, 69 inpatients from the CMW and 74 outpatients from the Department of Radio-oncology who met the criteria were included in this study. All patients received oncology treatment with RT with/without chemotherapy at the Chang Gung Memorial Hospital. The tumor locations were classified as nasopharyngeal carcinoma (NPC), cancers of the larynx and pharynx, and other HN cancers. Tumors of the HN were staged according to the staging rules laid down by the American Joint Committee on Cancer in 2002. Baseline characteristics of the study population, including parameters such as tumor stage, location, modes of treatment, and mean dose and duration of RT are shown in Table 2 with no significant differences between groups. Initially, mean body weights of outpatients and inpatients of CMW were 66.06 and 63.69 kg, respectively, which was not significantly different.
Baseline Characteristics of Study Participants a
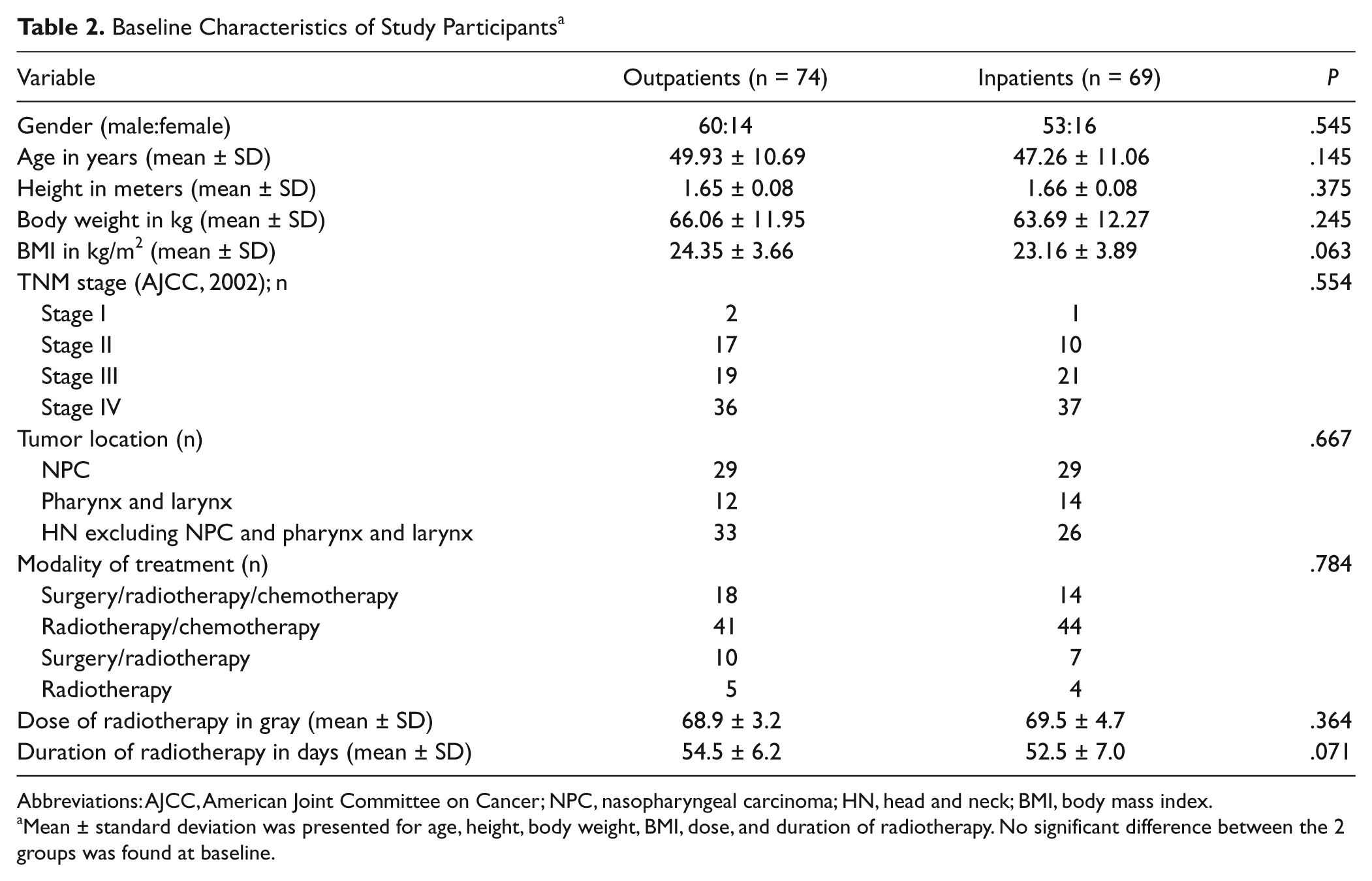
Abbreviations: AJCC, American Joint Committee on Cancer; NPC, nasopharyngeal carcinoma; HN, head and neck; BMI, body mass index.
Mean ± standard deviation was presented for age, height, body weight, BMI, dose, and duration of radiotherapy. No significant difference between the 2 groups was found at baseline.
Weight Changes and Tube Feedings
Generally, both groups of patients had significant weight loss during RT with/without chemotherapy (P = .000), but inpatients in the CMW had significantly lesser body weight loss than the outpatients (P = .016) as shown in Table 3. The mean weight change was −7.63% in the outpatients and −5.43% in the inpatients. For patients with HN cancer excluding NPC, the mean body weight change was −6.86% for outpatients and −3.76% for inpatients, which is a statistically significant difference (P = .015). However, there were no significant differences between the 2 groups for any of the 3 tumor locations individually. Nevertheless, there were trends toward lesser weight loss in the inpatients group with cancer of the pharynx and larynx and for other HN cancers excluding NPC. Both groups had 28 patients with tube feedings at the end of RT, with no statistical difference. For patients with and without tube feeding, the mean weight loss was −7.80% versus −7.53% in outpatients, and −5.10% versus −5.65% in patients in the CMW, respectively, which was not statistically significant. Moreover, one outpatient, but no inpatients of the CMW, in the study had a body weight loss of >20%. The largest decline in body weight was −23.21% in the outpatient group and −17.21% in the inpatient group. There were 25 outpatients (33.78%), but only 13 inpatients (18.84%) lost more than 10% of their pretherapy body weight.
Percentage of Weight Change and Number of Tube Feeding a

Both groups of patients had weight loss during radiotherapy with/without chemotherapy, but inpatients in the Chinese medicine ward had significantly lesser body weight loss than the outpatients.
P < .05.
There were 36 outpatients and 37 inpatients with stage IV cancers, and their mean weight changes were −7.90% and −4.09%, respectively, which was a statistically significant difference (P = .004). However, this difference was not found between subgroups with stage II or III disease. In addition, the correlation between changes in body weight and length of hospitalization was analyzed for the inpatient group. A significant correlation was found for patients hospitalized ≥40 days who had lesser body weight loss during RT compared with inpatients hospitalized for a shorter period (P = .025). The weight change of inpatients hospitalized ≥40 days was significantly lesser than that of the outpatients group as seen in Table 4 (P = .001). No drug interaction between Chinese and Western medicine was recorded in this study.
Outpatients Versus Inpatients With ≥40 Days of Hospitalization a
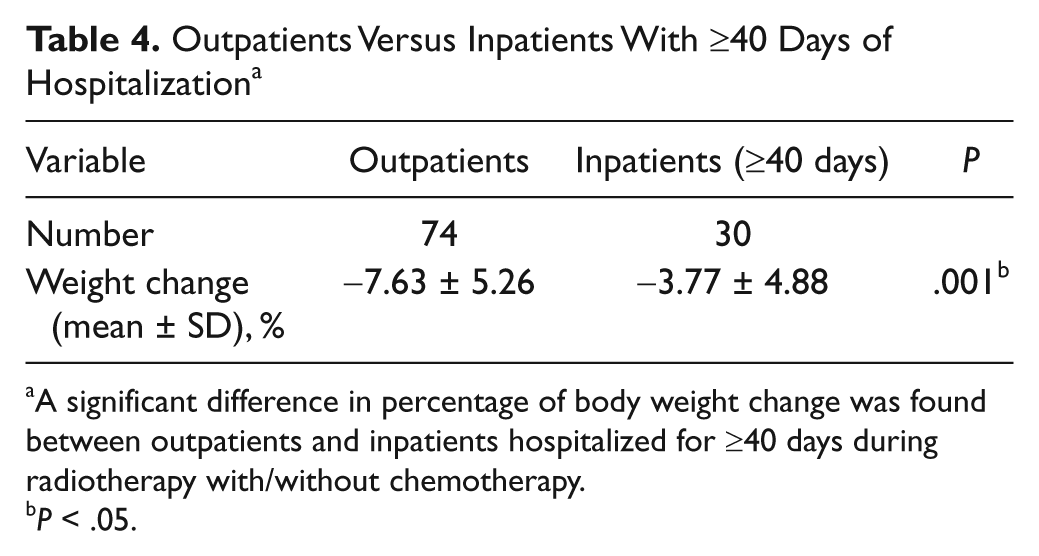
A significant difference in percentage of body weight change was found between outpatients and inpatients hospitalized for ≥40 days during radiotherapy with/without chemotherapy.
P < .05.
Quality of Life—MDASI Assessment
In this study, 61 outpatients and 29 inpatients who received ≥60 Gy of RT completed the MDASI core assessment (Table 5), and their mean doses of radiation were 63.6 and 68.0 Gy, respectively, which was a statistically significant difference (P = .000)—but only with around 3 days difference in average according to 180 to 200 cGy of RT per day. When MDASI questionnaires were completed, the mean dose of RT was lower in the outpatient group because they filled in the questionnaires at the time of outpatient service once per week, which did not guarantee inclusion of the time that the maximum dose of radiation was given. However, inpatients who were hospitalized in CMW could complete the MDASI core assessment closer to the end of RT. Since there was no reward for completing this questionnaire, more than half of inpatients did not return it, especially because some patients were being prepared for discharge around the end of RT. There were no significant differences in baseline characteristics, dose and duration of radiation, or percentage of weight change between inpatients in the CMW who completed the questionnaire (n = 29) and those who did not (n = 40). No significance differences were found in the scores for severity and interference of symptoms on the MDASI between inpatients and outpatients. However, inpatients had significantly lower scores, indicating better functioning, for the items “lack of appetite,” “normal work,” and “walking ability” on the MDASI than outpatients (P = .002, P = .033, P = .012, respectively). Hence, quality of life was improved in patients receiving hospitalization and CAM.

Abbreviations: SD, standard deviation; MDASI, M.D. Anderson Symptom Inventory.
Sixty-one outpatients and 29 inpatients with ≥60 Gy of radiotherapy completed the MDASI core assessment, and mean doses of radiation at the time of completion of the questionnaire were 63.6 and 68.0 Gy, respectively, with a statistically significant difference (P < .05). No statistical differences were presented in 2 dimensions of MDASI between the 2 groups. However, for the items “lack of appetite,” “normal work,” and ”walking ability,” inpatients had significantly lower scores (P < .05) than outpatients.
Outpatients generally completed the questionnaire earlier in the course of treatment than inpatients.
P < .05.
Discussion
Complementary and alternative medicine has become popular among cancer patients. One previous study reported that the use of CAM is unlikely to interfere with the administration of standard cancer therapy during a period of cancer diagnosis and treatment. 12 Another study mentioned that 1 in 5 HN cancer patients use CAM, and the most common therapies are herbal medicines (47%) to counteract ill effects arising from cancer and its treatment. 9 Although many patients with HN cancers use CAM, its effects on maintenance of body weight and quality of life during RT has rarely been reported. Therefore, our retrospective study is the first to discuss these issues.
According to the theory of traditional Chinese medicine, most patients with cancer have a pattern of both a lack of right qi and an excess of evil qi. Surgery, RT, and chemotherapy are similar to the attacking method in Chinese medicine theory. Attacking evil often harms the right qi, which worsens the lack of right qi. One study reported that yin deficiency might reflect a status of long-term malnutrition, which often occurs in patients with chronic wasting disease, especially in patients in the late stage of cancer. 13 Moreover, radiation belongs to Fire evil, which is 1 of the 6 excesses causing disease. The Fire or Heat damages yin, and depletion of yin humor represents a lack of fluid and nutrition in the body. Since a balanced status of yin and yang is considered important for health, a yin deficiency leads to yin–yang imbalance and clinical symptoms appear. Chemotherapy is considered a drug toxin resulting in a lack of qi and essence, which determines the strength of the constitution. Therefore, patients with HN cancers hospitalized in the CMW during RT or CCRT usually have a pattern wherein both qi and yin are lacking. Internal use of Chinese herbal medicines, such as Sha-shen-mai-dong-tang, 14 mainly supplements qi and nourishes yin to relieve symptoms such as stomatitis, xerostomia, and dysphagia. Drugs to harmonize the stomach and intestines are also used for anorexia and nausea if needed. External use of herbs locally to the radiation site principally clears Heat and resolves toxins to minimize dermatitis. Doctors occasionally use acupuncture to adjust the qi in the channels or network vessels of patients. Hence, inpatients in the CMW with HN cancers included in this study received the integrated therapies mentioned above. Patients hospitalized for ≤10 days were not included in this study because intervention in the CMW was incomplete, and we were not able to determine if these patients received Chinese medicine at the outpatient service after discharge. In rare cases, intravenous hydration was given for a few days if the patient requested. No parenteral nutrition was offered during hospitalization since enteral nutrition is still considered the gold standard for the nutritional support of patients with HN cancers.
Patients with HN cancers often have malnutrition and weight loss because of local problems or systemic issues. Not only is there involvement of symptoms related to the cancer itself, such as tumor obstruction, tumor cachexia, and anorexia, but also symptoms related to the side effects of anticancer modalities, including mucositis, dermatitis, reduced salivary secretion, taste alteration, and trismus arising from radiation, as well as psychological reactions such as depression. Beaver et al 15 also found that patients treated by CCRT had a risk of severe body weight loss. However, there are still no mature guidelines to prevent weight loss in patients with HN cancers during RT with/without chemotherapy. It has been reported that weight loss >20% significantly increases CCRT-induced toxicity, which is correlated with an increase in infections, hospital readmission rate, and early mortality risk within 30 days after the completion of CCRT. 16 One outpatient in our study had a body weight loss of >20%, but no inpatients in the CMW lost this much weight. In addition, patients with weight reduction of >10% during cisplatin-containing CCRT have been found to be at high risk of declining kidney function. 3 In our survey, 33.78% of outpatients lost more than 10% of their pretherapy body weight, but only 18.84% of inpatients lost this much weight.
Parenteral nutrition is rarely used because it is less efficient in delivering nutritional requirements but more expensive than enteral nutrition, and there are risks of leukopenia-related infections and fluid overload.16,17 Early or intensive nutritional intervention and tube feeding, either from a nasogastric tube or a percutaneous endoscopic gastrostomy in selected patients have been suggested,6,7,15,16 but the benefits in preventing weight loss are equivocal. 18 For patients with cancer, an increased metabolic rate or elevated resting energy expenditure is a significant component behind weight loss. Weight loss may occur because of altered responses of body functions and may not be related to energy intake.19-21 Cancer patients with stage IV disease have even higher resting energy expenditure compared with those at other stages. 21 In this study, the mean weight reduction was significantly lower in HN cancer patients in the CMW than outpatients during RT, and this difference was more prominent between groups for patients with stage IV disease. However, the rates of tube feeding were similar between the 2 groups. Radio-oncologists suggested inserting a feeding tube when patients with HN cancers had about >5% kg weight loss from the commencement of treatment. However, insertion of feeding tube or not depended on patients’ preference, and it was difficult to persuade patients to agree to tube feeding in Taiwan. In the Chinese tradition, some patients considered that tube feeding seemed equivalent to future death, so only those patients who could not swallow water would agree to tube insertion. Therefore, it was difficult to increase patients’ body weight by tube feeding, and the aim was rather to maintain their body weight. There were no recognizable differences between inpatients and outpatients who had tube feedings because of dysphagia resulting from postoperative structure change or painful swallowing. Tube feeding had no effect on weight change in either group. These findings imply that integrated medicine in the CMW might reduce the weight loss of patients with HN cancers during RT, either by improving local or systemic problems or correcting imbalances in metabolism, which could lead to a so-called harmonized yin and yang. Inpatients hospitalized for ≥40 days had an even more distinct alleviation of weight loss. Since most patients with HN cancers develop RT or CCRT related mucositis and dysphagia within 15 days of beginning oncological treatment, earlier intervention with integrated medical care in the CMW might have more benefits in preventing the side effects of anticancer modalities, and thereby avoid weight loss. Furthermore, there were trends toward less decrease of weight in those with cancer of the pharynx and larynx and other HN cancers excluding NPC. This might imply that larger case numbers are needed to see statistical differences.
According to previous reports, numerous quality-of-life dimensions significantly correspond to body weight loss, 22 and scores of global quality of life are lower in patients with more than 10% weight loss. 23 In addition, there is deterioration of physical function and role function 3 months after surgery for oral cancers, which correlates with reduced body image because of a significant decrease in oral function. 24 For patients with advanced stage oral cancers, such as stages III and IV, lower quality of life scores have been reported for pain- and site-specific effects such as swallowing and nutritional aspects. 24 Although more than a half of inpatients did not fill the MDASI questionnaire in this study, there were no significant differences in percentage of weight change between inpatients in the CMW who completed the questionnaire and those who did not. Therefore, we assumed that patients in the inpatient group who did not fail to complete the MDASI questionnaire because of their poor response to treatment. The sample size was too small to show a significant difference in the 2 dimensions of the MDASI core assessment between groups, but statistically significant lower scores were found for the items “lack of appetite,” “normal work,” and “walking ability” in inpatients. Loss of appetite and weight have been reported to be predictors of poor prognosis for cancer patients, 18 and intervention with integrated medicine in the CMW seemed to improve both aspects for inpatients with HN cancers. The items “working” and “walking ability,” assessed by the MDASI, seemed to have less influence on inpatients since most inpatients had health insurance, which covered hospitalization or could afford to pay for care, and they did not have much daily activity and/or a long commute for treatment because they were staying in the CMW.
In this retrospective study, several limitations deserve discussion. The most distinguishing feature of this study is the individualized Chinese medicine intervention without standardized prescription. Inpatients in the CMW were offered an integrated medicine program every day, which included internal and external use of herbs and acupuncture. Prescriptions of herbal medicine were changed by doctors if clinically indicated, which could not be done in the outpatients service of Chinese internal medicine. On one hand, individualized treatment based on pattern identification (bian zheng lun zhi in Chinese) is the characteristic of Chinese medicine. On the other hand, it makes randomization and reproduction difficult. In addition, inpatients were treated individually by 8 different attending physicians in this study, who were all licensed. Some studies25,26 have already reviewed the potential of Chinese herbal medicines or Asian botanicals for diminishing the side effects and complications caused by chemo- or radiotherapy. Our study accurately reflects clinical practice and also implies that CAM minimized patient’s weight loss from RT or chemoradiation potentially because of improved appetite. However, hospitalization is a confounding factor in this study. Since patients with HN cancers are not routinely admitted to a ward in the Western internal medicine department during oncological treatment, and all subjects in our study receiving Chinese medical treatment were hospitalized, it is impossible to exclude the impact of hospitalization itself on the results. In fact, most subjects were willing to be hospitalized because they lived too far to bear the long commutes for RT on weekdays or because they had health insurance that covered hospitalization. They were not necessarily wealthier patients of high social status who could afford better care. Outpatients who stayed at home might have felt more comfortable and eaten better because of family care. We could not avoid the bias in patients’ selection for the CAM group. However, this novel study lays a foundation for better designed clinical trials in the future. In addition, for patients with HN cancers who intend to be admitted to the CMW of the Chang Gung Memorial Hospital, our study provides evidence based medicine on minimizing weight loss and improving appetite during RT with/without chemotherapy. The weight changes were not compared between groups during regular follow-up after RT since some of the outpatients started using Chinese medicine after standard oncological therapy. In the future, the tumor recurrence rate or 5-year survival rate might be investigated to see if there is any difference between outpatients and inpatients in the CMW.
Conclusion
In this retrospective but novel study, we concluded that patients with HN cancers who were hospitalized in the CMW with individualized treatment of traditional Chinese medicine had lesser weight loss during RT with/without chemotherapy. There were no reports of drug interactions, and patients with early admission for Chinese medicine care during RT had better results than those with a shorter stay. Moreover, integrated medicine in the CMW was suggested to minimize lack of appetite, which might be correlated with the reduction of weight loss. Based on this preliminary study, a prospective and well designed clinical study in the outpatient service of Chinese Internal Medicine Department might be warranted to investigate the effects of Chinese medicine during RT without hospitalization. Further evaluation is also needed to find the mechanism of Chinese medicine that prevents weight loss during oncological treatment, and its influence on the metabolism of cancer patients.
Footnotes
Acknowledgements
We are grateful to the doctors, nurses and assistants of the Radio-oncology Department of the Chang Gung Memorial Hospital, Linkou, and the Department of Chinese Internal Medicine of the Chang Gung Memorial Hospital, Taoyuan, in Taiwan for their excellent and kind help in collecting data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.