
Abstract
Introduction
Use of complementary and alternative medicine (CAM) has increased in the oncology population.1-3 For prostate cancer, use of CAM ranged from 19% to 47%.4-12 Chinese medicine (CM), also known as traditional Chinese medicine, is one of the most popular types of CAM worldwide. In East Asia and particularly among Chinese populations, CM remains popular and continues to play an active role in the modern health system.13-17 In Western countries, acupuncture and Chinese herbal medicine have increasingly gained accceptance.18-21
Taiwan implemented the universal National Health Insurance (NHI) system in 1995. Coverage of NHI expanded to more than 99% of the population. The NHI provided a full range of care, from ambulatory and inpatient care to traditional Chinese medicine, dental services, child delivery, rehabilitation, home care, and chronic psychiatric rehabilitation. NHI-covered CM services include Chinese herbal medicine, acupuncture, and traumatology manipulative therapies. Beneficiaries are free to choose medical services. Chen et al 22 reported that CM was popular in the general population under NHI in Taiwan. Our previous study found that 2.6% prostate cancer patients used CM services (1.6% visits of ambulatory services) under NHI in Taiwan. 23 To compare the medical utilization of CM and Western medicine related to prostate cancer directly, our previous study only accounted for CM visits with diagnosis code of prostate cancer. With the low prevalence of CM use for prostate cancer, use of CM among prostate cancer patients for noncancer diseases needs to be considered. Besides, our previous study is cross-sectional. Yet little information exists about CAM use among prostate cancer patients in the long-term trends.
We conducted a study to explore long-term trends of CM use among prostate cancer patients under NHI. The National Health Insurance Research Database (NHIRD) provides registration and claim data sets of NHI for research. All CM visits of prostate cancer patients from 1996 to 2008 were accounted and divided into visits for prostate cancer and those for other diseases for comparison. Demographics of users, visit frequency, medical institutes, patterns of therapies, and cost of CM were examined.
Materials and Methods
Data Sources
This is a retrospective study using registration and claim data sets of the NHIRD. Files of registry for beneficiaries and claims of ambulatory care of cancer and Chinese medicine from 1996 to 2008 were obtained for analysis. Because of massive file size and protection of privacy, the complete claim data of ambulatory care of all 23 million beneficiaries were not provided by the NHIRD. Claims of ambulatory care of cancer were extracted from the complete claims of ambulatory care data file. Data that matched cancer diagnosis codes were selected to construct this data set. However, claims of cancer patients without cancer diagnosis codes were not included. The claims of ambulatory care of Chinese medicine were extracted from the complete claims of ambulatory care data file by matching procedure codes of Chinese medicine.
Although NHI was launched since 1995, data of the first year was not available in the NHIRD. NHI covers CM outpatient services but not inpatient services. Therefore, only claims of outpatient services were analyzed. Institutional review board approval was exempted because all personal data were de-identified by the NHI and NHIRD.
Study Samples
Prostate cancer patients were identified in claims of ambulatory care of cancer with diagnosis of prostate cancer (International Classification of Diseases, Ninth Revision, Clinical modification (ICD-9-CM) code 185 and A code A214) in each year. Before 2002, A code and ICD-9-CM were both acceptable. Since May 2002, CM physicians are requested to encode with ICD-9-CM coding system. All patient-based CM visits of prostate cancer were then retrieved from the data sets of claims of ambulatory care of CM. To obtain demographic data, claim data of ambulatory care were linked with files of registry for beneficiaries by their identifications and dates of birth. To compare the prevalence on the same basis, data extraction, linkage, and analysis were performed cross-sectionally year by year from 1996 to 2008. All cross-sectional data sets were combined to constitute this study.
To compare CM visits for prostate cancer and for other diseases, claims with diagnosis code of prostate cancer were defined as cancer-specific visits. Claims without a diagnosis code of prostate cancer were defined as non-cancer-specific visits. Patients who have used cancer-specific visits were defined as cancer-specific users. Patients who have never used cancer-specific visits were defined as non-cancer-specific users.
Statistics
Demographic characteristics of CM users and nonusers were compared. The prevalence of CM use in each cross-sectional year was calculated. Visit frequency, medical institutes, patterns of therapies, and cost of CM from 1996 to 2008 were examined. The utilization patterns of cancer-specific and non-cancer-specific CM visits were compared. All costs were presented in US$ (US$1 = NT$32.18 based on the average exchange rate during 1996-2008).
The database software ASIQ 12.5.7 (Sybase Inc, Dublin, CA) was used for data linking and processing. The data were analyzed using SPSS for Windows Version 13.0 (SPSS Inc, Chicago, IL). The distribution and frequency of each category of variables were examined by χ2 tests. A P value <.05 was considered statistically significant.
Results
During 1996-2008, 78 323 prostate cancer patients have used ambulatory services under NHI. Among them, 30 383 (38.8%) patients used CM outpatient services, with a total of 327 063 CM visits (average 10.8 visits per users).
User Demographics
The demographics are presented in Table 1. The median age was 70.5 years in CM users and 71.5 years in non-users. There were a higher portion of CM users than nonusers in their 60s and 70s.
Patient Characteristics of Study Population a

Note: CM = Chinese medicine.
Demographic data at the first time of diagnosis of prostate cancer. There were missing demographic data of 784 (1.0%) patients in age, 1028 (1.3%) in insured amount, 1203 (1.5%) in region, and 847 (1.1%) in unit.
All family members who are unemployed and not in low-income households.
People who are unemployed or younger than 20 years and have insured family member.
In terms of income (insured payroll-related amounts), there was a slightly higher portion of CM users with lower income (<$622 monthly), compared with nonusers. In terms of insured regions, there were a higher proportion of CM users registered in central and southern Taiwan. In terms of insured unit, those who were insured unit at the government, schools, enterprises, institutions, members of occupational unions, alien seamen, farmers, and fishermen constituted a greater proportion of CM users.
New Patients and Users
New prostate cancer patients increased from 5578 in 1996 to 6372 in 2008 (Figure 1). The number of CM users increased from 1389 in 1996 to 2824 in 2008. The proportion of new CM users in new prostate cancer patients increased from 24.9% in 1996 to 44.3% in 2008.

The percentage of new Chinese medicine (CM) users among new prostate cancer patients
Visit Frequency
As shown in Table 2, prostate cancer patients who used ambulatory services of Western medicine and CM increased from 5578 in 1996 to 23 990 in 2008. CM users increased from 1389 in 1996 to 6144 in 2008. CM visits also increased from 8729 in 1996 to 42 218 in 2008. Average CM visits per user ranged from 5.6 to 6.9 during 1996-2008. The prevalence of CM use in each cross-sectional year increased slightly from 24.9% to 25.6% (up to 26.7% in 2004) during 1996-2008.
Trends of Chinese Medicine (CM) Use Among Prostate Cancer Patients From 1996 to 2008
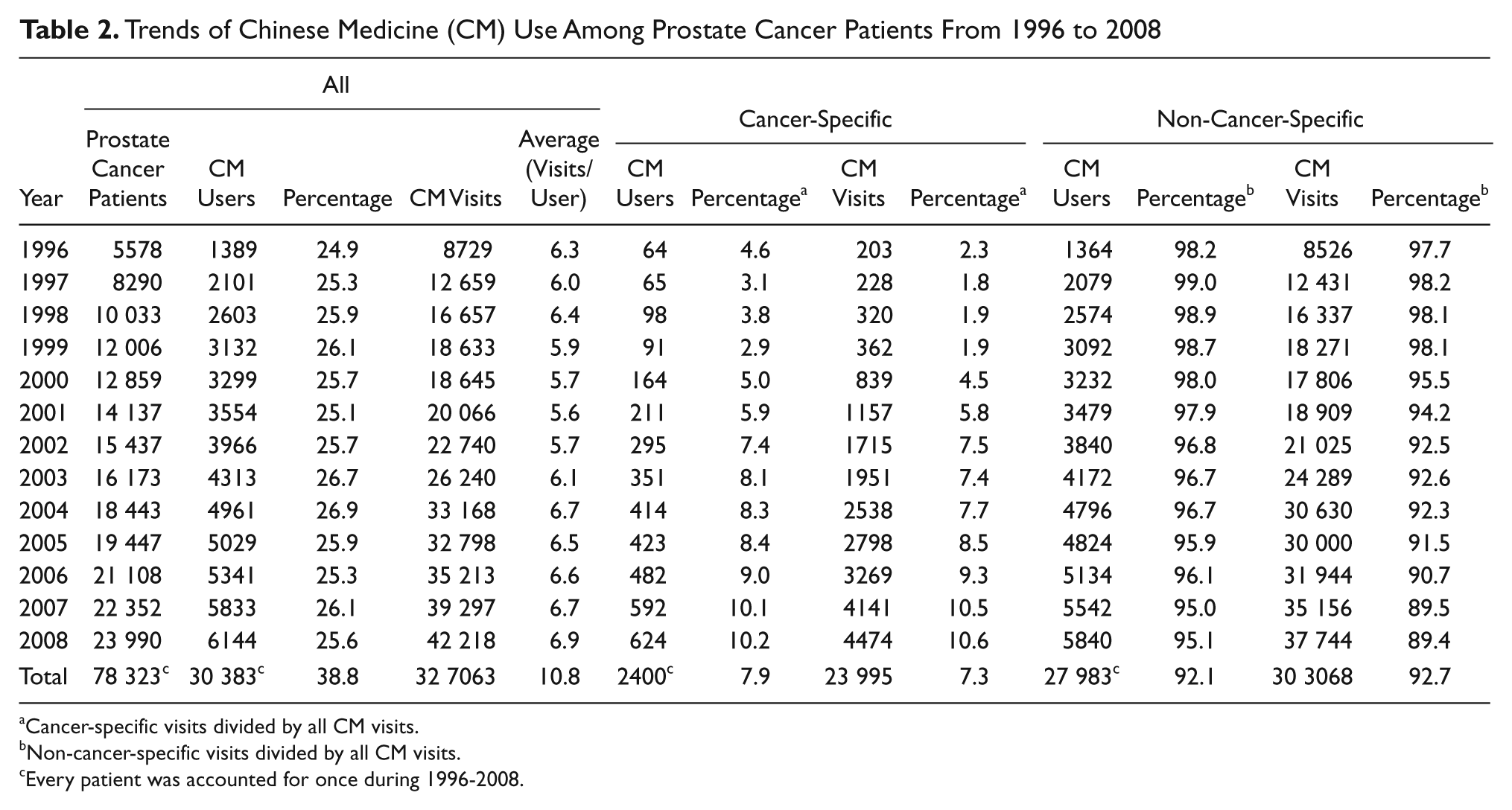
Cancer-specific visits divided by all CM visits.
Non-cancer-specific visits divided by all CM visits.
Every patient was accounted for once during 1996-2008.
The majority of CM visits (92.7%) were non-cancer-specific. However, cancer-specific CM visits increased from 2.3% to 10.6% during 1996-2008. Most CM users were non-cancer-specific users (92.1%). However, cancer-specific CM users increased from 4.6% to 10.2% during 1996-2008.
Only a small portion of CM users used CM frequently (>12 visits/year). The proportion of high-utility users (>12 visit/year) in cancer-specific CM users increased from 3.1% to 19.7% during 1996-2008. The proportion of high-utility users (>12 visit/year) in non-cancer-specific CM users was relative stable, ranging from 11.1% to 14.7% (Figure 2).

The percentage of high-utility users (>12 visit/year) in cancer-specific and non-cancer-specific users of Chinese medicine
Medical Institutes
Most CM outpatient services were provided by private clinics (68.1% to 79.2%), followed by private hospitals (12.1% to 25.2%), public hospitals (5.9% to 9.5%), and public clinics (0.0% to 0.1%). However, a higher portion of cancer-specific CM visits were provided by private hospitals after 2000 (Figure 3A). The proportion of CM services provided by private clinics in non-cancer-specific visits increased substantially during the study period (Figure 3B).
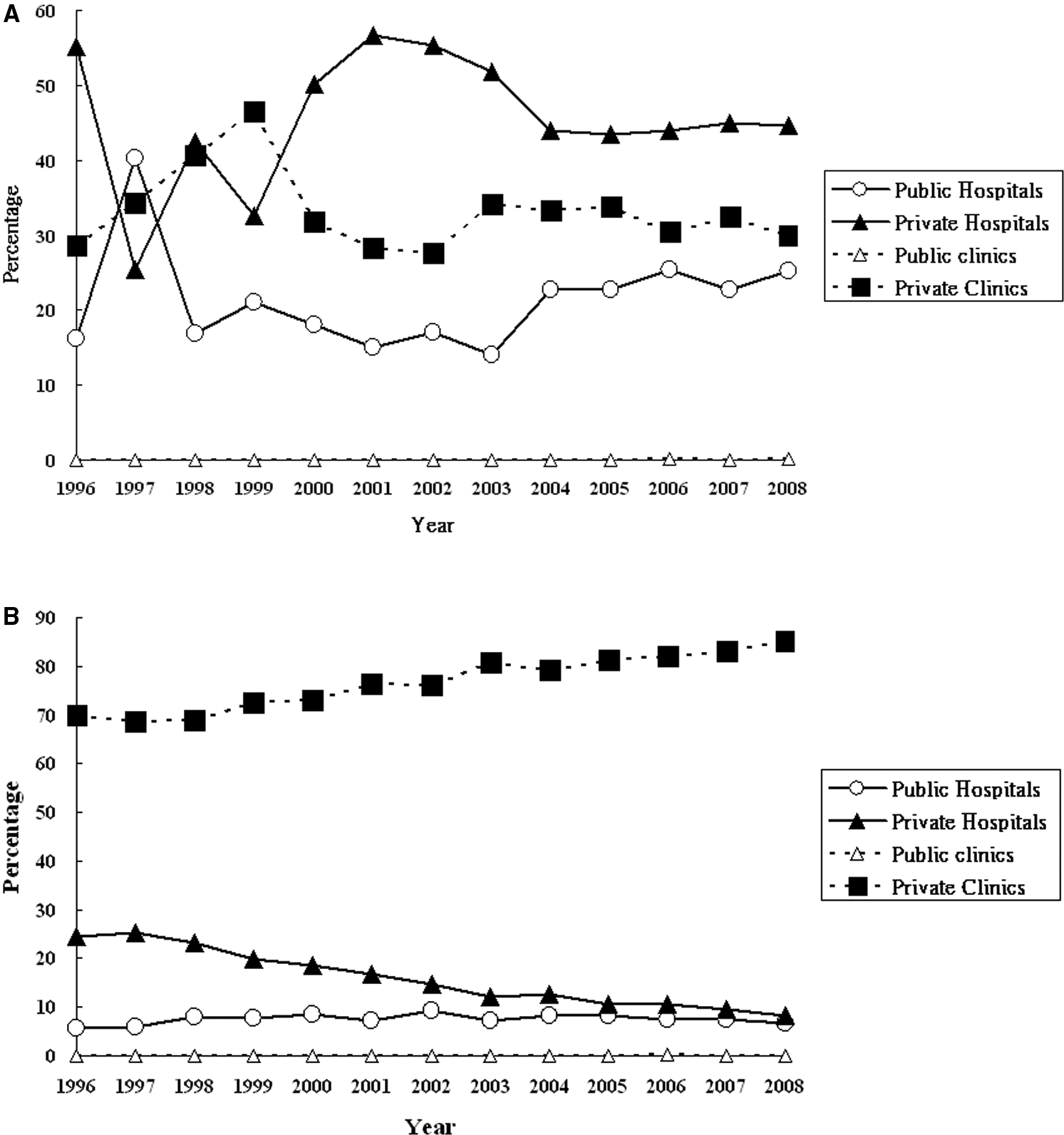
Distribution of medical institutes that provided Chinese medicine (CM) for prostate cancer patients
Patterns of Therapies
The most frequently used CM therapies were Chinese herbal medicine (72.8% to 78.8%), followed by acupuncture/traumatology manipulative therapies (28.1% to 36.8%; Figure 4). A higher proportion of users used Chinese herbal medicine in cancer-specific visits (69.7% to 95.6%) than in non-cancer-specific visits (71.1% to 78.5%). A higher proportion of users used acupuncture/traumatology manipulative therapies in non-cancer-specific visits (30.0% to 37.6%) than in cancer-specific visits (0.9% to 32.0%).

Trends of therapies of Chinese medicine used by prostate cancer patients for cancer-specific and non-cancer-specific visits
Cost
The details of cost of CM are shown in Table 3. Total CM cost increased from $122 247 to $825 454 during 1996-2008. The average cost per CM visit increased from $14.0 to $19.6. The annual cost per CM user increased from $88.0 to $134.4.
Trends of Cost (US$) of Chinese Medicine (CM) Among Prostate Cancer Patients

Total CM cost increased from $2799 to $103 896 in cancer-specific visits and from $119 448 to $721 558 in non-cancer-specific visits during the study period. Non-cancer-specific visits accounted for the majority of cost (87.4% to 98.4%). However, the proportion of cost for cancer-specific CM visits increased by year from 2.3% to 12.6%. The average cost per CM visit increased from $13.8 to $23.2 in cancer-specific visits and from $14.0 to $19.1 in non-cancer-specific visits. The annual cost per CM user increased from $43.7 to $166.5 in cancer-specific visits and from $87.6 to $123.6 in non-cancer-specific visits.
Most of the cost of cancer-specific visits was drug fees (38.0% to 59.1%; Figure 5), whereas most of the cost of non-cancer-specific visits was diagnosis fees (33.7% to 39.6%).

Trends and component of cost of Chinese medicine (CM) used among prostate cancer patients
Copayment accounted for 6.6% to 11.7% of the total cost. For cancer-specific visits, copayment was limited, ranging from 1.6% to 4.8%. Copayment in non-cancer-specific visits was higher, ranging from 6.6% to 12.1% (Figure 6).

Trends of copayment of Chinese medicine (CM) used among prostate cancer patients under National Health Insurance
Discussion
Within the trends of integrating CAM into mainstream medicine, the Taiwan experience is unique because most CM services were covered by NHI. With more than 90% coverage rate of NHI, the NHIRD is representative of the whole population in Taiwan. This study is the first report on long-term trends of Chinese medicine use among prostate cancer under NHI. All complete claims of ambulatory care of cancer and Chinese medicine of 23 million beneficiaries from 1996 to 2008 were obtained for study. Among 78 323 prostate cancer patients identified during 1996-2008, there were 30 383 (38.8%) CM users and 327 063 CM outpatient visits. Our study found increasing trends of CM use among prostate cancer patients under NHI, attributable primarily to the increase of CM users, rather than the increase of CM visits per user. The proportion of new CM users in new prostate cancer patients increased from 24.9% in 1996 to 44.3% in 2008. Prostate cancer patients used CM for noncancer diseases (non-cancer-specific visit) more than cancer (cancer-specific visit). The utilization patterns between cancer-specific and non-cancer-specific CM were distinctly different, including visit frequency, therapies, medical institutes, and costs. There were a greater increase in users and visits of cancer-specific CM visits during the study period. Moreover, the proportion of high-utility users (>12 visit/year) in cancer-specific CM visits increased more than that in non-cancer-specific CM visits.
During 1996-2008, CM visits increased to 4.8 times (8729 to 42 218). New prostate cancer patients increased 1.1 times (5578 to 6372) whereas CM users increased 2 times (1389 to 2824). The proportion of new CM users in new prostate cancer patients increased from 24.9% in 1996 to 44.3% in 2008. The average CM visits per users also increased from 6.3 to 6.9 during the study period. Therefore, increase of CM use was attributable primarily to an increase in the proportion of the population seeking CM, rather than increased visits per user.
The prevalence is much higher than found in our previous cross-sectional study. 23 Our previous study found that the prevalence of CM use for prostate cancer was only 2.6%. The main reason is the different criteria of data selection in the 2 studies. Our previous study was visit based and this study was patient based. To compare the medical utilization of CM and Western medicine related to prostate cancer directly, our previous study only accounted for CM visits with diagnosis code of prostate cancer (ICD-9-CM code 185). CM visits for other diseases by prostate cancer patients were not included. In this study, all CM visits of prostate cancer patients were selected, including claims with and without diagnosis code of prostate cancer. CM visits were classified as cancer specific and noncancer specific. According to NHI regulation, claims for reimbursements are requested to record up to 3 items of diagnosis codes. NHI examines the items, quantities, legitimacy, and quality of the medical care services, approves and pays the costs and expenses incurred from such services. Among 23 995 cancer-specific CM visits in this study, 20 214 (84.2%) visits recorded prostate cancer as the principal diagnosis, including 9336 (38.9%) visits that recorded prostate cancer as the only diagnosis. Therefore, the presence of the diagnosis code of prostate cancer can reflect that the patients visited for prostate cancer. In this study, the majority of CM visits among prostate cancer patients were noncancer specific (92.7%). With no prostate cancer diagnosis code in most of the CM claims, it is possible that most CM physicians were not aware that the patients had been diagnosed with prostate cancer. Prostate cancer patients tended to visit clinics for CM and visit hospitals for Western medicine. It is also probable that most doctors of Western medicine were not aware that these prostate cancer patients also used CM.
Our study found that the utilization patterns between cancer-specific and non-cancer-specific CM were distinctly different, including visit frequency, therapies, medical institutes, and costs. Although the prevalence of CM use among prostate cancer patients had increased slightly, there was a greater increase in cancer-specific CM than non-cancer-specific CM during the study period. The users increased to 9.8 times and the visits increased to 22 times in cancer-specific CM, whereas those in non-cancer-specific CM increased to 4.3 and 4.4 times, respectively. Our study also found that the proportion of high-utility users (>12 visit/year) in cancer-specific CM users had largely increased, compared with non-cancer-specific CM during 1996-2008. After 2002, there were a higher proportion of high-utility users (>12 visit/year) in cancer-specific CM than in non-cancer-specific CM. In NHI, patients are free to choose Western medicine or CM services without referral. With the increase of high-utility users (>12 visit/year) in cancer-specific CM, CM seems to play a more important role in the care of prostate cancer patients.
Most cancer-specific visits used Chinese herbal medicine (69.7% to 95.6%). Use of acupuncture/traumatology manipulative therapies in cancer-specific visits was limited (0.9% to 32.0%). However, there was a higher proportion of non-cancer-specific visits that used acupuncture/traumatology manipulative therapies (30.0% to 37.6%). Because most of these prostate cancer patients were elderly, musculoskeletal diseases were frequently reported. In our further analysis, there were 51.5% non-cancer-specific CM visits after 2002 with the diagnosis of diseases of the musculoskeletal system and connective tissue (ICD-9-CM code 710-739). With increasingly high use of CM for cancer-specific visits, the efficacy and safety of these Chinese herbal medicines for prostate cancer patients need further investigation. The potential drug–herb interactions should also be investigated.
Total CM cost increased to 6.8 times during 1996-2008. The cost of both cancer-specific and non-cancer-specific visits increased. However, the increase of total cost in cancer-specific visits was greater than that in non-cancer-specific visits. There were a higher portion of drug fees in cancer-specific visits than in non-cancer-specific visits. This is consistent with most cancer-specific CM visits that used Chinese herbal medicine.
The copayment was both limited in cancer-specific visits and non-cancer-specific visits. However, the copayment was less in cancer-specific visits than that in non-cancer-specific visits. Under NHI regulation, cancer patients can submit application for a catastrophic illness certificate. The application is formally reviewed, and if approved, the information is entered into his or her IC card. Patients with the catastrophic illness certification who get care for the illness or related conditions within the certificate’s validity period do not have to pay copayment.
Our study found CM users tended to be in their 60s and 70s, with lower income (<$622 monthly), living in central and southern Taiwan, and insured unit at the government, school, enterprises or institutions, members of occupational unions, alien seamen, farmers, and fishermen. Previous studies showed that the use of CAM varies by patients’ cultural, religious, ethnic, gender, and geographic distributions.4,5,8,9,11,24-30 Because Chinese medicine is the traditional medicine in Taiwan and covered by NHI, the demographic and socioecomic characteristics of CM users might differ widely from those in Western countries. In previous studies of Western countries, CAM users with prostate cancer tend to be highly educated, with higher income, and with multiple comorbidities.4-12,26,31-33
Our study found that there were fewer very elderly (>80 years old) prostate cancer patients who used CM. Frail elderly are probably afflicted with physical or mental disabilities that may interfere with the ability to independently perform activities of daily living. Because NHI provided only CM outpatient services but not CM inpatient services, there is a barrier for very elderly patients to use CM frequently. Our study also found there was a slightly higher portion of CM users with lower income (<$622 monthly), in central and southern Taiwan. This is consistent with previous studies in Taiwan. 34 “Usable resources” was an important factor that influences the CM purchasing behavior. 35 There are more Chinese medical institutes per person in central and southern Taiwan. Besides, our study also found a higher proportion of prostate cancer patients with lower income (<$622 monthly) in central (80.7%), southern (81.9%), eastern Taiwan and offshore islands (82.4%) than that in northern Taiwan (73.2%). With respect to insured unit, there were a higher proportion of CM users who were insured at the government, schools, enterprises, institutions, occupational unions and who were alien seamen, farmers, and fishermen. Those persons who are employed might have better performance status and thus more ability to seek CM outpatient services.
As CM is gaining popularity in Taiwan, NHI-contracted CM medical institutes increased by 67.7% from 1722 to 2888 during 1996-2008. By the end of 2008, 21 (95.4%) hospitals had CM sections and 2867 (90.7%) CM clinics were contracted with NHI. The study by Chen et al 22 found that most CM services were provided by clinics (82.6%) rather than hospitals in the general population. In this study, most CM services were also provided by private clinics (68.1% to 79.2%). However, most cancer-specific CM visits were provided by hospitals. This reflected that prostate cancer patients preferred seeking CM services in the CM section of hospitals for prostate cancer and in CM clinics for other diseases. In Taiwan, there are few oncology clinics. Most cancer patients receive treatment and follow-up for cancer-related conditions at hospitals. For patients who use CM for prostate cancer, it would be more convenient to visit the CM section of the same hospital to share the medical records. With more hospitals establishing CM sections, oncologists might prefer transferring cancer patients to their CM colleagues rather than CM clinics for better collaboration.
There were several limitations in this study. The study population was selected by the diagnosis code of prostate cancer. Overcoding can occur. Prostate cancer patients might be overestimated. Out-of-pocket herbal medicine and noncontracted clinics were not investigated. Previous studies reported there was higher demand for noncovered rather than covered CAM under NHI in Taiwan. 36 Besides, clinical characteristics, including staging, prostate-specific antigen, and biochemical data were not available in this study. The efficacy and safety of CM also need further investigation.
In conclusion, there was a trend of increased CM use among prostate cancer patients under NHI. Although prostate cancer patients used CM mostly for noncancer diseases, cancer-specific CM visits increased greatly. The utilization patterns between cancer-specific and non-cancer-specific CM were distinctly different.
Footnotes
This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by National Health Research Institutes. The interpretations and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health, or National Health Research Institutes.
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article:
This work was supported by Cheng Hsin General Hospital (Grant No. 99-39), the National Science Council (Grant No. NSC 99-2320-B-350-001), and the Department of Health, Taiwan (Grant No. DOH99-TD-C-111-007).