
Abstract
Introduction
Given the prevalent use of tobacco and betel nut in the Taiwanese community, an increase risk of oral, oropharynx, and hypopharynx cancers (head and neck cancers) is apparent. The use of Traditional Chinese Medicine (TCM) and acupuncture is both common and conveniently accessible in Taiwan, with treatments being financially supported by the National Health Insurance (NHI). This study aims to investigate the use of TCM in head and neck cancers in Taiwan through a longitudinal cohort study.
Methods:
The Taiwan National Health Insurance Research Database (NHIRD) was utilized in order to conduct this study. The study populations consisted of oral, oropharynx, nasopharynx, and hypopharynx cancers (head and neck cancer) patients in 2002, which were then followed up until 2007 in regards to TCM use, until 2013 in regards to acupuncture use and until 2014 for all-cause mortality. Patients were divided into 4 groups. Common symptoms, Chinese herbs and formula used, TCM visits and 5 and 12 years all-cause mortality were analyzed.
Results:
The use of TCM was increased in the second to fourth-year post-diagnosis. TCM use in nasopharynx cancer patients was higher compared to other cancers. The number of TCM visits per patient was increased post-diagnosis. The findings suggest a non-significant reduction in 5 and 12 years all-cause mortality between TCM II and CON II groups.
Conclusion:
The use of TCM in new patients suffering from head and neck cancers was increased in close proximity to the cancer diagnosis. The relation between TCM use and mortality of head and neck cancer should be investigated through larger scale studies.
Keywords
Introduction
Head and neck cancers are reported to be the seventh most commonly diagnosed cancers worldwide. 1 Identifying and addressing the significance of this matter has led to comprehensive investigations in this regard. Currently, according to the global cancer statistics of 2020, the ranking of cancer variant commonality is as follows: oral 18th, nasopharynx 24th, oropharynx 26th, and hypopharynx 27th. 2 The specific prevalence of oral cancer in South and Southeast Asia is relatively high compared to other regions. 3 Furthermore, the dominant use of tobacco, betel nut and alcohol use as common habitual activities is proportionately related to the prevalence of head and neck cancer.1,4 Exposure to the Human Papilloma Virus (HPV) is yet another risk factor associated with head and neck cancers, and directly affects the disease progression. 1 Typically, tobacco consumption (smoked or chewed) is the most common cause of oral cancer. 5 Bagnardi et al 6 showed that the ratio of relative risks associated with the development of oral cancer in heavy drinkers compared with nondrinkers or occasional drinkers was 5 to 13. Novel evidence has further identified the risk that East Asians, and especially Taiwanese and Taiwanese aborigines, face with regard to detrimental genetic predispositions. Specifically, these populations may be more susceptible to the carcinogenic effects of alcohol, due to the high prevalence of the Aldehyde Dehydrogenase 2 (ALDH2) allele absence.7,8 ALDH2 deficiency, more commonly known as Alcohol Flushing Syndrome or Asian Glow, is a genetic condition that interferes with the metabolism of alcohol. Furthermore, incidences of oral cancer, nasopharynx cancer, and oropharynx cancer are generally also linked with a poor diet consisting of a reduced intake of fresh fruits and vegetables.9-11 The manifestation of head and neck cancer is related to a variety of symptoms, and patients can suffer from a series of associated pathologies such as non-healing oral ulcers, mouth swelling, pain, malnourishment, dysphagia, dysarthria, odynophagia, neck mass, etc.12,13 Of these signs and symptoms, some can be treated with the use of Traditional Chinese Medicine (TCM) and acupuncture, which has demonstrated recognized positive effects in the treatment of many diseases. In 1995, the Taiwanese government implemented a National Health Insurance (NHI) that covers 99% of Taiwan’s population and over 90% of health service providers. This insurance also includes most TCM and acupuncture clinics, and serves as an extensive foundation for the assimilation and investigation of various data points. 14
This topic was previously investigated by Lin et al 15 in a 10-year follow-up of the Taiwanese population. This study also briefly investigated the TCM used in similar patients. In addition to the study of Lin et al our study provides a more detailed analysis of TCM and acupuncture used, with specific signs and symptoms, and all-cause mortality in each head and neck cancer.
The objective of this study was to investigate the use of TCM and acupuncture among head and neck cancers (in close proximity to the mouth: oral, nasopharynx, oropharynx, hypopharynx cancers) before and after diagnosis. This was conducted in the form of a retrospective longitudinal cohort study from 2001 to 2007. The study used data from outpatient TCM clinics. Head and neck cancers patients were divided into 4 groups: Conventional treatment excluding chemotherapy (CT) or radiotherapy (RT) (CON I), Conventional treatment excluding CT or RT with TCM (TCM I), Conventional treatment including CT or RT (CON II) and Conventional treatment including CT (or RT) plus TCM (TCM II). In the TCM groups, details on acupuncture use were also investigated. Furthermore, an analysis of key signs and symptoms treated was included. Data on all groups also incorporated age, sex, occupation, and residential location in Taiwan.
Methods
Data Source
The data for this study were collected from the Taiwan National Health Insurance Research Database (NHIRD) data file Longitudinal Health Insurance Database 2000 (LHID 2000). This database contains the original claimed medical data of over 99% of Taiwan residents. We used the outpatient, hospital admission, medication, and treatment data of 1 million randomly selected subjects. This study was approved by the Institutional Review Board of China Medical University Hospital Research Ethics Committee (CMUH104-REC2-115(AR-4)).
Study Population
The patients who were diagnosed with head and neck cancer in 2002 were included as the primary study population. Head and neck cancer patients were defined by the diagnosis code of the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) 140 to 149, 230.0, 232.0, and with IC cards for severe illness. Patients aged younger than 20 were excluded. Included subjects were then divided according to the treatments they received. The first group received Conventional treatment excluding CT or RT (CON I) The second group received Conventional treatment including CT or RT (CON II), such as antineoplastic therapy, CT, immunotherapy (ICD-9-OP procedure code V58.1)/ CT (ICD-9-OP procedure code V66.2) / RT (ICD-9-OP procedure code V66.1). The third group received Conventional treatment excluding CT or RT with TCM (TCM I). The last group received Conventional treatment including CT or RT plus TCM (TCM II). Surgical intervention can be applied in all groups depending on the patient’s condition; for surgical ICD 9 codes see Supplemental Table 1. The use of TCM was followed up until 2007, the acupuncture use was followed up until the end of 2013, and 5 and 12 years all-cause mortality was followed up until 2014.
Acupuncture was defined as: Manual acupuncture (B41, B42, B80-B84, B90-B94, P27041, P31103, P32103 and P33031), Electroacupuncture (B43, B44, B86-89, and P33032) and complex acupuncture (B45 and B46).
Signs and Symptoms
The development of the signs and symptoms before and after the diagnosis of cancer was of specific interest to the study. The symptoms including pain (ICD-9-CM code 780.96, 784.1), dyspnea, respiratory abnormalities (ICD-9-CM code 786.0), malnutrition (ICD-9-CM code 263.9,579.3,783.2,783.3,783.7,995.84,V85.0), cachexia (ICD-9-CM code 260,261,262,263.0-263.1, 263.3-263.9,799.4), oral soft tissue symptoms (ICD-9-CM code 528.2,528.9,784.2), digestive system (ICD-9-CM code 525.8, 527.7, 528.6, 528.79, 530.1, 531-537, 564, 578.1, 787.01, 787.91), injury (ICD-9-CM code 840-848), dysarthria (ICD-9-CM code 784.51), swelling, mass, or lump in head and neck (ICD-9-CM code 784.2) were included in the data recordings and observations.
2.4 Statistical analysis
The distribution of baseline characteristics in the different treatment groups was examined by the Chi-square test, the Student’s t-test and the one-way Analysis of Variance (ANOVA). All groups were compared to the reference group CON I. The odds ratio was estimated by the logistic model which included sex, age, urbanization, occupation, and residential location variables with its respective 95% confidence inference (CI). For all-cause mortality analysis the Cox proportional hazard model with a multivariate survival analysis (adjusted by: sex, age, urbanization, occupation, and residential location) and a Kaplan-Meier plot with a log-rank test was used. All statistical analysis was performed by SAS (version 9.4; SAS Institute, Inc., Cary, NC, USA) and a P-value of <.05 was considered statistically significant. In cases where subjects’ information on sex and age were missing, the cases were excluded from the analysis.
Results
In 2002, 1063 patients were diagnosed with head and neck cancers from NHI registration. There were 464 patients included in the CON I group, 87 in the CON II group, 424 in the TCM I group and 88 in the TCM II groups (Figure 1). There were 246 patients lost to follow-up due to possible reasons such as stopping NHI membership, or immigration to another country. The losses to follow-up per group: CON I—178 patients, CON II—43 patients, TCM I—101 patients, and TCM II—40 patients.
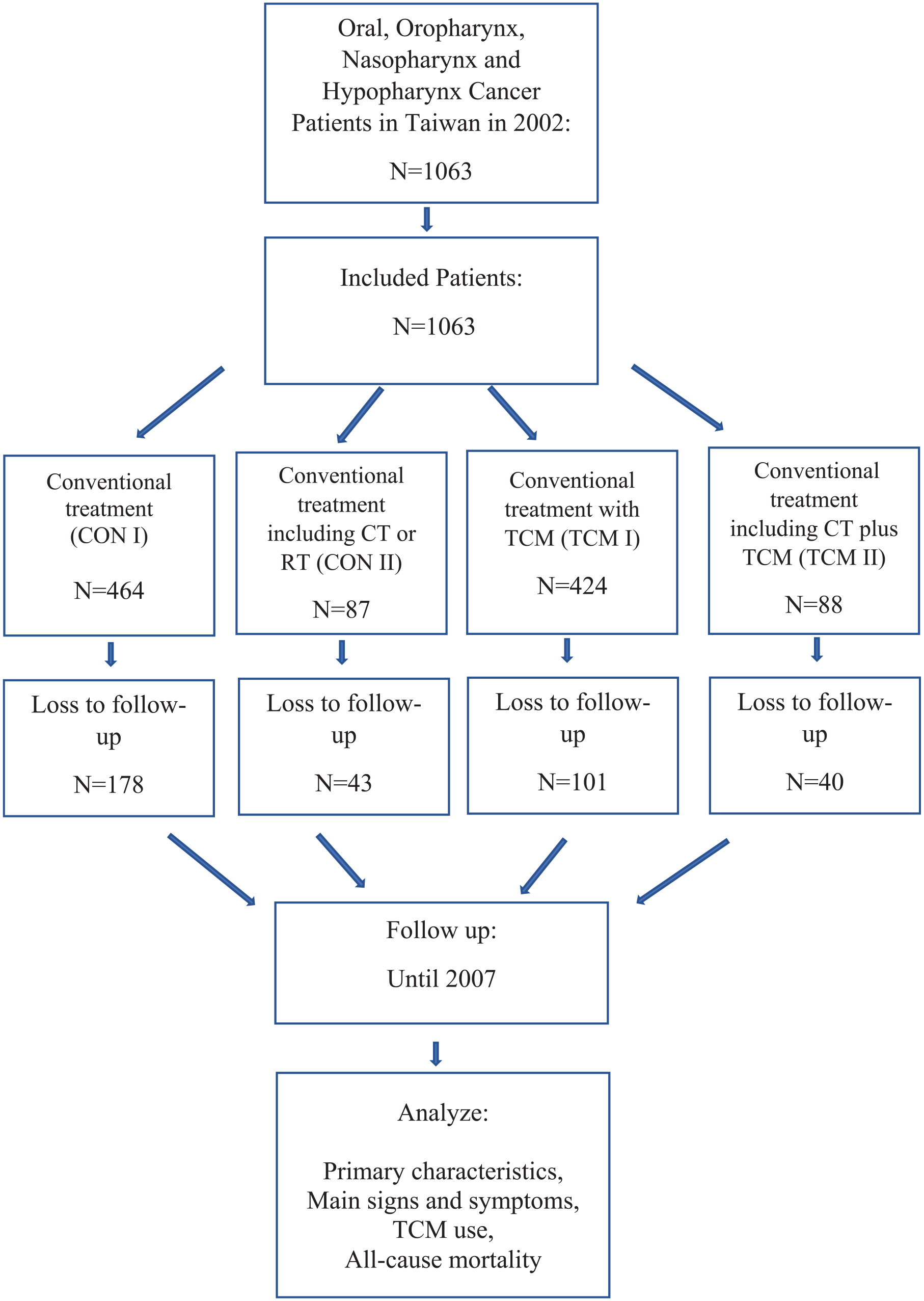
Study flow chart. The figure depicts study processes. Abbreviations: CT, chemotherapy; RT, radiotherapy; TCM, traditional Chinese.
All the patients in the CON II and TCM II groups received surgery as part of the therapy. In the CON I group there were 277 out of 464 patients that did not receive surgery. In the TCM I group, there were 157 out of 424 patients that did not receive surgery. The remainder of the patients in those groups received surgery (Supplemental Table 2).
Table 1 shows the usage of traditional Chinese medication (TCM) among these patients. Before the diagnosis of head and neck cancers, 27% of them had used TCM. The average visits of TCM treatments increased after the diagnosis of head and neck cancers. None of the included patients received acupuncture prior to cancer diagnosis. However, post-diagnosis acupuncture was used by 103 patients in the total follow-up time, with only 0.8% of patients per year receiving acupuncture in the 2 to 13 years of the post-diagnosis period. The acupuncture use peaked in the third, fourth and ninth post-diagnosis years, with 1.31%, 1.22%, and 1.41% respectively (see Supplemental Table 3). The time interval from cancer diagnosis to the first acupuncture visit was 6.4 years. The average number of visits was 2.67 with a range of 1 to 20 visits (see Supplemental Table 3).
The Usage of Traditional Chinese Medication for All Types of Head and Neck Cancer Patients.

Depicts the use of TCM in the cases of oropharynx, nasopharynx, hypopharynx, and oral cancers according to pre-diagnostic and post-diagnostic data. In 2001, a total of 1063 patients were diagnosed with head and neck cancers. 27% of the patients used TCM prior to the diagnosis of head and neck cancers. The use of TCM post-diagnosis was 21%, 24%, 27%, 25%, 28%, and 11% in 2002, 2003, 2004, 2005, 2006, and 2007 respectively.
Table 2 presents the baseline features of head and neck cancer patients with different treatments. Female patients (30%) were more willing to receive TCM in addition to Conventional treatments. Patients from the CON I intervention had older mean age (57.4 ± 13.6), while patients in the CON II group had the youngest mean age (51.1 ± 12.5). The patients’ living urbanization across each of the 4 series of interventions were insignificantly distributed. Patients who principally selected CON I or CON II interventions were largely classified as agricultural workers, but patients who underwent a combination of conventional treatment with TCM remedies were mostly classified as office workers. However, the difference between occupations among the 4 treatment groups revealed non-significant differences. The top 3 residential locations utilizing the aforementioned treatments in Taiwan were Taipei, Central, and Kao-Ping (south part of Taiwan).
The Baseline Characteristics of the Head and Neck Cancer Patients Receiving Different Treatments.

Depicts the baseline characteristics among the 4 groups of head and neck cancers. Briefly, females were willing to accept TCM treatment in comparison to males who were more willing to accept therapy. Patients who received western medicine treatment only had older mean age, although patients in the western medicine and therapy treatment group had the youngest mean age. There is no significant difference between the occupation among the groups, and the primary residential locations of those receiving the treatments were Taipei, Central, and Koa-Ping.
1 Office workers: Public servants, schools, colleges and universities staff, teachers, employees of non-profit institutions, employees of public institutions, employees of private institutions, members of professional trade unions, trainees of vocational training institutions.
2 Agricultural workers: Seafarers, farmers, members of water conservancy associations, members of fishing associations.
3 Others: Dependent family members, unaccompanied military family members, military academy students and military servicemen, substitute service, low-income households placed in social welfare service institutions, monks and religious persons.
The signs and symptoms that developed before and after head and neck cancer diagnosis are depicted in Table 3. We considered patients who received CON I interventions as a reference group. In the pre-diagnosis year symptoms of cachexia, oral soft tissues, digestive system diseases, swelling, mass, or lump in head and neck occurred frequently in patients the CON II group compared to the CON I group (P < .05). A year before the diagnosis, patients in the TCM I group were less likely to have oral soft tissues symptoms compared to patients in the CON I group(P < .05). Within 5 years after the diagnosis, there were reasonable increases of most signs and symptoms among the 4 groups when compared to the baseline of 1 year before diagnosis. The patients in both the TCM I, and the TCM II groups required more medical attention due to symptoms of pain and injury in the 5 years post-diagnosis measurements when compared to the CON I group (P < .05). The TCM I group was related to less clinical symptoms of swelling, mass, or lump in head and neck 5 years post-diagnosis compared to the CON I group (P < .05). In the following 5 years post-diagnosis period the CON II group showed reduction in oral soft tissues symptoms compared to the CON I (P < .05).
The Symptoms Developed Before and After the Diagnosis of Head and Neck Cancers in Different Treatments.

Depicts the percentage of symptoms developed before and after the diagnosis of head and neck cancers among the 4 groups. Pain, dyspnea, and respiratory abnormalities, malnutrition, cachexia, oral soft tissues, neoplasms alcohol related, digestive system disease, injury, dysarthria, swelling, mass, or lump in head and neck other were of the included symptoms analyzed. OR: odds ratio adjusted by sex, age, urbanization, occupation, and residential location. 95% CI: 95% confidence inference.
P-value < .05. **P-value < .01. ***P-value < .001.
For detailed data on each specific cancer see Supplemental Table 4 to 7.
Table 4 lists the top 10 single herbs and herbal formulas used by oral cancer patients. The top 3 common single herbs were Dān Shēn (丹參), Yán Hú Suǒ (延胡索), and Bèi Mǔ (貝母) and Mài Mén Dōng (麥門冬). Additionally, Shū Jīng Huó Xiě Tang (疏經活血湯), Gān Lù Yǐn (甘露飲), and Sháo Yào Gān Cǎo Tang (芍藥甘草湯) were the most frequently used herbal formulas.
Ten Most Used Single Herbs and Herbal Formulas.

Depicts the most used single herbs and herbal formulas among the 4 groups. Briefly, the top three common single herbs were Dān Shēn (丹參), Yán Hú Suǒ (延胡索), and Bèi Mǔ (貝母) and Mài Mén Dōng (麥門冬). Moreover, Shū Jīng Huó Xiě Tang (疏經活血湯), Gān Lù Yǐn (甘露飲), and Sháo Yào Gān Cǎo Tang (芍藥甘草湯) were the most frequently used herbal formulas.
The all-cause mortality rates in the same year of cancer diagnosis were the highest in patients in the CON II group (8%). The 5 years all-cause mortality rates in different types of head and neck cancer patients were also listed (see Table 6), and recorded 15.1% (70 patients out of 464) in the CON I group; 8.5% (36 patients out of 424) in the TCM I group; 18.4% (16 patients out of 87) in the CON II; and 17.0% (15 out of 88) in the TCM II group, as shown in Table 5. For 5 years all-cause mortality the TCM I group was compared to the CON I group and showed a non-significant reduction in mortality in the TCM I group as hazard ratio of 0.73 (0.26, 2.05 95% CI) in the crude analysis and a hazard ratio of 0.92 (0.51, 1.65 95% CI) after adjusting for sex, age, urbanization, occupation, and residential location. The TCM II group was compared to the CON II group and showed a non-significant reduction in mortality in the TCM II group as hazard ratio of 0.70 (0.34, 1.47 95% CI) in the crude analysis and a hazard ratio of 0.75 (0.30, 1.88 95% CI) after adjusting for sex, age, urbanization, occupation, and residential location. For the 12 years all-cause mortality TCM I group was compared to the CON I and showed a non-significant trend of reduction in mortality in the TCM I group as hazard ratio of 0.38 (0.09, 1.7 95% CI). However, after adjusting for sex, age, urbanization, occupation, and residential location the results show a non-significant increased mortality rate with the TCM I group a hazard ratio of 1.08 (0.59, 1.98 95% CI). The survival log-rank test P = .80 between the TCM I and CON I groups. The TCM II group was compared to the CON II group and showed a non-significant reduction in mortality as hazard ratio of 0.69 (0.4, 1.19 95% CI) in the crude analysis in favor of the TCM II group, and a hazard ratio of 0.74 (0.41, 1.35) after adjusting for sex, age, urbanization, occupation and residential location. The survival log-rank test P = .20 for the TCM II and the CON II groups (Table 6, Figure 2).
The Mortality Rate in Each Year.

Depicts the mortality rate in each year. The 5-year all-cause mortality was reduced in patients who received Western medicine with TCM treatment when compared with Western medicine only, especially in the oral and oropharynx cancer group.
All-Cause Mortality for 5 and 12 Years.

Cox proportional hazard model with a multivariate all cause survival analysis (adjusted by: sex, age, urbanization, occupation and residential location). Depicts the TCM use of patients in 2002. The table explains the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) for each cancer. Data are presented as number of patents (N) and percent (%).

(a and b) Survival analysis between the groups. All-cause mortality analysis is shown by the log-rank test.
Discussion
This study is a population-based study of the use of TCM in cancers of the head and neck. The study showed that 27% of head and neck cancer patients in Taiwan used TCM, while the TCM usage was decreased after the cancer diagnosis and peaked in 2006, the fourth year post-diagnosis. The average TCM visits peaked at the first-year post-diagnosis in 2003. Nasopharynx cancer patients had the highest number of TCM use when compared to other kinds of head and neck cancers. There are differences in common signs and symptoms between the groups. Acupuncture was not used in all patients, prior to the cancer diagnosis. Post-diagnosis acupuncture was used by 103 patients in the total follow-up time of 11 years. The acupuncture use peaked on the third, fourth and ninth post-diagnosis years at 1.31%, 1.22%, and 1.41% respectively.
Lin et al 15 showed that in head and neck cancer patients, the use of TCM was associated with a 32% reduction in all-cause mortality levels in a 10 years follow-up time of the Taiwanese population. Our study also discovered a non-significant reduction in the 5 and 12 years all-cause mortality and between the TCM II and the CON II groups. For all-cause mortality, it is important to note that our study did not include data on tumor stage or comorbidities. There is a high likelihood that the CON II and TCM II include more severe patients with possible later stage tumors compared to the CON I or the TCM I. A systematic review and meta-analysis conducted by Kim et al on herbal medicine use for nasopharyngeal cancer that included 22 studies displayed significantly less mortality in 1, 3,and 5 years follow up in the combined herbal and Western medicine group when compared to the conventional treatment. The systematic review and meta-analysis also identified the most commonly used herbs: Radix Ophiopogonis (Mai Men Dong) and Radix Salviae Miltiorrhizae (Dan Shen) are the top 2. 16 Our study found a similarity of Radix Ophiopogonis (Mai Men Dong) and Radix Salviae Miltiorrhizae (Dan Shen) usage in the top 5 used single herbs. A systematic review of Chinese herbal treatment for radiotherapy-induced xerostomia including 15 studies found limited evidence that Chinese medicine may reduce xerostomia in head and neck cancer patients. 17 A clinical trial of 70 patients discovered that along with a significant reduction in xerostomia, the Chinese medicine group also significantly reduced oral pain in head and neck patients. 18 A study conducted by Yamashita et al 19 on 80 head and neck patients found that herbal medicine can prevent and alleviate severe oral mucositis induced by chemo-radiation when compared to patients only receiving chemo-radiation. In our analysis, we found that 10% to 22% of the head and neck cancer patients seek treatment for oral soft tissue symptoms. Our study also found a reduction in symptoms of swelling, mass, or lump in head and neck 5 years post-diagnosis in the TCM II group. This finding supports the use of TCM for those symptoms. However, the CON II group showed a significant reduction of oral soft tissues symptoms in the 5 years after the diagnosis. This reduction might be contradictory to Yamashita et al study findings. Another Taiwanese NHIRD study demonstrated a protective effect of the TCM use against the development of a second primary cancer in esophageal cancer patients. 20 A retrospective cohort study from Taiwan on radiotherapy related weight loss in head and neck cancer patients compared 2 groups; hospitalized patients receiving radiotherapy with Chinese medicine compared to non-hospitalized patients receiving radiotherapy, whereby the study showed a significant reduction in weight loss in the Chinese medicine group. 21 This might be a result of the TCM use. The patients in both TCM I and TCM II groups, had an increase pain and injury symptoms within 5 years after the diagnosis. It might indicate that those patients visit the TCM clinic not solely due to the cancer; visits might be due to unrelated pain or injury for these patients.
Our study discovered that the most commonly used Chinese herbal formula was Shū Jīng Huó Xiě Tang, followed by Gān Lù Yǐn. The formula Shū Jīng Huó Xiě Tang includes the following herbs: Chinese Angelica Root (Dang Gui), White Peony Root (Bai Shao), Raw Rehmannia Root (Sheng Di Huang), Szechuan Lovage Root (Chuan Xiong), Peach Kernel (Tao Ren), Poria (Fu Ling), Atractylodes Root (Cang Zhu), Citrus Peel (Chen Pi), Notopterygium Root (Qiang Huo), Angelica Root (Bai Zhi), Clematis Root (Wei Ling Xian), Stephania Root (Han Fang Zi), Fang Feng Root (Fang Feng), Scabrous Gentiana Root (Long Dan), Achyranthes Root (Niu Xi), and Chinese Licorice Root (Gan Cao). This formula is used in order to resolve blood stasis with wind-damp in the channels according to TCM theory, whereby both blood stasis and wind damp are part of the generating factors in malignancy development. 22 The formula Gān Lù Yǐn includes the following herbs: Sheng Di Huang (Raw Radix Rehmanniae), Mai Men Dong (Tuber Ophiopogonis), Tian Men Dong (Tuber Asparagi), Shi Hu (Herba Dendrobii), Pi Pa Ye (Folium Eriobotryae), Yin Chen Hao (Herba Artemisiae Scopariae), Huang Qin (Radix Scutellariae), Zhi Shi (Fructus Immaturus Aurantii), and Gan Cao (Radix Glycyrrhizae). This formula is mainly used for treating the mouth area, for damp-heat and yin deficiency in the stomach channel. Long term yin deficiency leads to damp-heat and blood stagnation; when left untreated for a long period of time it can also result in malignancy generation. 22 The 2 most used single herbs are Radix Salviae Miltiorrhizae (Dan Shen), and Rhizoma Corydalis (Yan Hu Suo), both of which are used in treating blood stasis and alleviating pain. Blood stasis is recognized as an important factor in cancer development as discussed above.
The use of acupuncture in the Taiwanese population was reported as 7.98% in 2001, however, only 0.12% of head and neck cancers patients used acupuncture for neoplasms. 23 This can demonstrate the general opinion of the Taiwanese people on the effectiveness of acupuncture in the treatment of neoplasms. Our study showed that in the 2 to 13 post-diagnosis years, only 0.8% of the patients used acupuncture every year, and those findings are in accordance with the overall acupuncture use in neoplasms. 23
Limitations
There are several limitations in our study. First, the patients were not randomized. Second, we could not access data on lifestyle habits like tobacco, alcohol or betel nut consumption. Third, only the all-cause mortality data were available for this study. For all-cause mortality analysis, there was no comparison of confounding factors and no data on tumor stage. Fourth, details on which acupuncture points were used are not provided in the NHIRD database. Last, a similar, larger scale study was conducted over a longer time period by Lin et al, 15 although our study served to provide more detailed information on a variety of novel aspects. Additional research is required to confirm these findings.
Conclusion
In conclusion, 27% of head and neck cancer patients used TCM. The use of TCM was increased in the second to fourth-year post-diagnosis. TCM use in nasopharynx cancer patients was higher when compared to other cancers. The number of TCM visits per patient was increased post-diagnosis compared to pre-diagnosis, especially in the second post-diagnosis year. The post-diagnosis acupuncture use was 0.8% per year, with 2.67 visits per patient. Non-significant reduction in mortality was found in the study in the TCM II group compared to the CON II group. Ultimately this work serves to provide evidence that clarified the use of TCM as a treatment intervention in ameliorating the signs and symptoms commonly associated with head and neck cancers.
Supplemental Material
sj-docx-1-ict-10.1177_15347354221132790 – Supplemental material for The Use of Traditional Chinese Medicine in Patients with Oral, Oropharynx, Nasopharynx, and Hypopharynx Cancers: A Retrospective Longitudinal Cohort Study in Taiwan
Supplemental material, sj-docx-1-ict-10.1177_15347354221132790 for The Use of Traditional Chinese Medicine in Patients with Oral, Oropharynx, Nasopharynx, and Hypopharynx Cancers: A Retrospective Longitudinal Cohort Study in Taiwan by Eyal Ben-Arie, Chanya Inprasit, Bernice Lottering, Hei-Tung Yip, Wen-Chao Ho, Yu-Chen Lee and Pei-Yu Kao in Integrative Cancer Therapies
Footnotes
Author contributions
Conceptualization; E.B.A, Y.C.L, P.Y.K, W.C.H, H.T.Y
Data curation; H.T.Y
Formal analysis; H.T.Y
Funding acquisition; H.T.Y, Y.C.L
Investigation; E.B.A, Y.C.L, P.Y.K, W.C.H, H.T.Y, C.I, B.L
Methodology; E.B.A, Y.C.L, P.Y.K, W.C.H, H.T.Y
Project administration; E.B.A, Y.C.L, P.Y.K
Resources; E.B.A, Y.C.L, P.Y.K
Software; H.T.Y
Supervision; Y.C.L, P.Y.K
Validation; C.I, B.L
Visualization; E.B.A, H.T.Y
Roles/Writing - original draft; E.B.A, C.I, B.L
Writing - review & editing; E.B.A, Y.C.L, P.Y.K, W.C.H, H.T.Y, C.I, B.L
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported in part by Taiwan Ministry of Health and Welfare Clinical Trial Center (MOHW109-TDU-B-212-114004, MOHW111-CMAP-M-113-112101), MOST Clinical Trial Consortium for Stroke (MOST 109-2321-B-039-002), China Medical University Hospital (DMR-109-231), Tseng-Lien Lin Foundation, Taichung, Taiwan.
Data Accessibility
The study data is only available to members of the National Health Insurance Research Database personals. The data contains individual patients’ personal information and cannot be made available by request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.