
Abstract
Background. Although several clinical studies have shown that mistletoe therapy (MT, Viscum album) may improve cancer patients’ quality-of-life (QoL), qualitative information on the improvement’s nature is still lacking. Design. This exploratory, prospective, cohort-study comprised 25 patients with different types of cancer. The patients filled in the EORTC QLQ-C30 Version 3.0 questionnaire at the beginning of MT (n = 25) and three months later (n = 21). If patients agreed, they were interviewed on both occasions (n = 17); the interviews were transcribed verbatim and submitted to a qualitative content analysis (n = 12). Results. Analysis of the questionnaires showed significant improvements in several subscales during MT. The interviews analysis revealed that most patients adopted the MT with a supportive goal, with all patients undergoing conventional therapies. After three months of MT, most interviewed patients revealed higher vitality and autonomy. MT was often seen as a chance to make an own personal contribution to the therapy, which was particularly appreciated in cases in which no conventional therapy was (anymore) advised. Concrete personal achievements such as changes in the private and/or in the professional environment were spontaneously mentioned by the patients, illustrating and corroborating their improvements in QoL. Conclusion. Our results show that the patients experienced an improvement of QoL during MT. This therapy seemed to offer a platform for an integrative coping with the disease, which might be important in reconciling the perceived shock of an existential illness with a good QoL.
Background
Viscum album (mistletoe) preparations are the most commonly used form of complementary/alternative cancer therapy in central Europe. 1 The mistletoe preparations are often used in an additive setting, together with standard chemotherapy or radiotherapy, 2 and the corresponding therapeutic effects have been described in several clinical studies and some recent reviews.1,3-6 Whereas contradicting results exist regarding possible effects of mistletoe therapy (MT) on life expectancy and tumor regression, the evidence for a favorable effect on quality of life (QoL) is accumulating. Postoperative treatment with mistletoe preparations in combination with conventional treatment has been shown to attenuate adverse reactions to tumor-destructive therapies 7 and to improve patients’ QoL.8-10 However, qualitative information on the nature of the observed QoL improvement is still lacking.
QoL assumes a relatively major dimension in the context of cancer treatment, since both disease and conventional treatments might affect it considerably. The importance of an improvement of QoL was recognized several years ago by the US Food and Drug Administration, which included QoL in the list of end points on which the approval of an anticancer drug might be based. 11 In clinical studies, QoL is mostly estimated by standardized questionnaires, frequently, the European Organisation for Research and Treatment of Cancer (EORTC) QLQ-C30. Questionnaires represent a way to objectively quantify QoL in a wide number of patients, but lack the in-depth subjective dimension of each patient’s QoL perception, which is likely to be associated with personal coping strategies or with the adaptation to a threatening disease such as cancer. It is likely that this subjective dimension is closer to concepts that may help to unveil the reasons why human beings stay healthy or are able to return to healthier conditions, for example, salutogenesis, self-regulation, and resilience12-15 than the information obtained with standardized questionnaires.
The frequent use of MT suggests that cancer patients have high expectations of this complementary and alternative medicine (CAM) treatment. The lack of in-depth knowledge on patients’ expectations and experiences while deciding for and using MT prompted us to perform the present exploratory study, which focuses on the qualitative characterization of QoL and on patient coping with the disease.
Methods
Study Design and Participants
This exploratory, prospective, before–after cohort study included consecutive outpatients (n = 25) with different types of cancer starting a treatment with subcutaneous applications of anthroposophic mistletoe preparations at the Paracelsus Hospital in Richterswil, Switzerland. All patients were informed about the study by their treating physician at the same time that MT was suggested. The study was performed under real-life conditions and can be considered as observational, inasmuch as the decisions for a given mistletoe preparation and treatment schedule were made by the recruiting physicians independently of the study, taking patients’ preferences into consideration when appropriate; no exclusion criteria were defined and the patients were free to do additional therapies. In the praxis, mistletoe preparations of the following brands were injected 2 or 3 times per week: Iscador (n = 13; Qu, M or P; Weleda AG, Arlesheim, Switzerland), abnobaViscum (n = 11; Qu or A; Abnoba GmbH, Pforzheim, Germany) and Isorel (n = 1; Novipharm GmbH, Pörtschach am Wörther See, Austria). During the recruitment period, 110 patients with C-Diagnoses (ICD-10) were registered electronically at the hospital. The study was authorized by the Ethical Commission of the canton of Zurich and was performed in accordance with the Declaration of Helsinki. All patients signed an informed consent form. The patients participating in the study filled in the following standard questionnaires on QoL at the beginning of the treatment: EORTC QLQ-C30 Version 3.0, 16 SELT-M, 17 and HLQ Version 2.5 18 ; a further nonstandard questionnaire was used to collect more data on the therapies the patients used (conventional, mistletoe, and others) and their impact on QoL as perceived by the patient. To collect information on their experiences with the therapies, the patients were asked to fill in the questionnaires a second time 3 months after beginning MT. All questionnaires were handed out to the patients by the recruiting physicians, on signing the informed consent. Four patients did not return the questionnaires 3 months after starting MT, in 3 cases because the patients had passed away in the meantime, in 1 because the patient withdraw her consent to participate in the study. The scores of the different questionnaires were determined according to the EORTC scoring manual. 19 Answers to the questionnaires filled in at the beginning of MT and 3 months later were compared with the Wilcoxon–Mann–Whitney test, which was performed with SPSS (SPSS Inc., Chicago, IL); differences between the 2 groups of data were considered statistically significant if P < .05. In the few cases in which one question was not answered, the averaged score of the relevant items was considered. 19
Content Analysis of the Interviews
If the patients agreed, they were interviewed at the beginning of MT and 3 months later (n = 17). All recorded interviews were performed by MB, a medical trainee at the Paracelsus Hospital of Richterswil, who performed the practical part of this clinical study during his MD thesis. 20 It should be stated that MB was not involved in the treatment of the patients. The present exploratory study comprises a content analysis of these guided, open-ended interviews. So as not to disturb the communication between patients and researchers, the interviews were not actively limited in time; most of them lasted between 3 and 5 quarters of an hour. The interviews performed at the beginning of MT focused on the following themes: (a) how the patients became aware of their disease, (b) how they opted for MT, (c) what they expected from MT, (d) their attitude toward CAM, (e) how the diagnosis of cancer affected their life, (f) whether they suspected particular cause of their disease, and (g) whether they used a personal coping strategy. The interviews that took place 3 months after starting MT addressed the following themes: (a) how patients felt in comparison with 3 months earlier, (b) what other therapies—conventional and from CAM—they had undergone, (c) what problems they had had with MT and the other therapies, and (d) how they evaluated the success of MT and other therapies. In a few cases, the patients came to the interview with an accompanying person; this was accepted by the interviewer since he believed that these persons were important for the patients’ coping strategy. Also, the patients’ suggested meeting venue for the interview was accepted, although the interviewer’s own suggestion was usually the hospital. The interviews were performed in German (local dialect) and the quotations presented in this manuscript were thereafter translated into English. Of the 17 patients who agreed to be interviewed, 5 were excluded from the present analysis for the following reasons: (a) 1 patient passed away after the first interview, (b) 1 patient stopped MT and withdrew his consent to participate in the study, (c) 2 patients wanted to be interviewed together since they were a couple and the resulting interview included so many aspects of couple dynamics that it could hardly be compared with the others, and (d) 1 patient could only be reached by phone for both first and second interviews.
The face-to-face interviews were recorded and transcribed verbatim, except for 2 interviews after 3 months of MT, as follows: (a) in one case, the interviewer could not record the interview because of a technical problem and took notes (F39) and (b) in the other case, the interview was performed by phone and the interviewer recorded his voice and always repeated what the interviewee said (M57, because the patient was having health problems that prevented personal contact). Transcripts were subjected to content analysis essentially as described previously 21 but allowing for an a posteriori, theory-generating approach as suggested elsewhere. 22 In this way, we were able not only to extract quantitative information from the interviews—for example, how many patients were of a certain opinion—but also gain in-depth information on the aspects that were important to patients even when these were not included in the list of themes planned for the interviews. The interview analysis consisted of the following steps: (a) the interview text was read several times, (b) the text was searched for sentences containing information on the themes established a priori (see above), (c) sentences containing information on the established themes were marked manually, (d) the new themes detected while reading were thereafter submitted to the procedure described under (b) and (c), (e) the information extracted from the marked sentences was condensed and tabulated in various sequential steps, and (f) after information had been extracted, citations were sought for illustration purposes. Throughout the analysis, the data were revisited at pertinent points. In this article and when considered appropriate, patients are referred to by a letter defining the gender and age at the first interview (eg, F45 means a 45-year-old female patient).
Results
Patients’ Demographic Characteristics
The main sociodemographic characteristics of the study patients (n = 25) are presented in Table 1. The patients were on average 62 ± 11.1 years old and in most cases male (14 out of 25). The diagnoses were varied, with a predominance of colorectal (n = 7), prostate (n = 4), breast (n = 4), lung (n = 3), and pancreatic (n = 3) cancer.
Patients’ Demographic Characteristics and Main Questionnaire Outcomes a

Age, gender, and diagnosis of all included patients (n = 25) is shown, as well as the relative importance that mistletoe therapy assumed for the patient (n = 23) and the additional therapies that were used by the patients (n = 22). If patients agreed (n = 17), they were interviewed by the researchers; 12 interviews could be submitted to content analysis (see Methods section).
While answering the questionnaire on the therapies used, all patients stated that they were using mistletoe for the first time in relation to the present disease. A considerable number (11 of 23) described its use as being important to their overall therapy and most patients were undergoing other therapies at the same time, 16 out of 22 being conventional ones (surgery, chemotherapy, radiation, and hormone therapy, Table 1).
Analysis of the EORTC QLQ-C30 Questionnaire
The data obtained with the widely used standard questionnaire EORTC QLQ-C30 at treatment beginning and 3 months later (n = 21) are shown in Table 2. The EORTC QLQ-C30 questionnaire comprises functional scales (the higher the value the better the patient’s health), which include a global assessment of the QoL, and symptom scales (the higher the value the stronger the patient’s symptom). Statistically significant differences between the average values obtained for role (P = .03) and emotional (P = .018) functioning as well as for fatigue (P = .024) at MT beginning and those obtained 3 months later could be observed. In all 3 cases, the statistically significant differences reflected improvements in the patients’ status. A tendency toward improvement could be detected in the global QoL as well (P = .057).
Results of the EORTC QLQ-C30 Questionnaires a

The questionnaire items corresponding to each scale are shown and the results obtained for each scale are expressed as percentage of the highest possible score. In the functional scales, higher value indicates better patient health, whereas in the symptoms scales, higher value indicates stronger patient symptom. Data are shown as mean and standard deviation (SD) of the percentage scores of each scale (for more details, see Methods section).
P < .05.
The results of the 2 other QoL questionnaires used (SELT-M and HLQ) corroborated the tendency toward an improvement in QoL over the 3 months in which the patients were being monitored during the present study (data not shown 23 ).
On the Interviewed Patients
As mentioned under Methods section, 17 patients accepted to be interviewed. In total, 12 out of the 17 interviews could be used for content analysis, the results of which are described in the subsections below. The QoL of these 12 patients, whose interviews are analyzed below, is likely to have been comparable to the QoL of the remaining patients, since the scores of the perceived global QoL in the EORTC QLQ-C30 questionnaire at the beginning of MT were similar in these 2 groups (60% vs 59%). The conventional cancer treatments undergone by these 12 patients and their individual scores of global QoL (as determined by the EORTC QLQ-C30 questionnaire) at the beginning of MT and 3 months later are presented in Table 3.
Treatment of the Interviewed Patients a
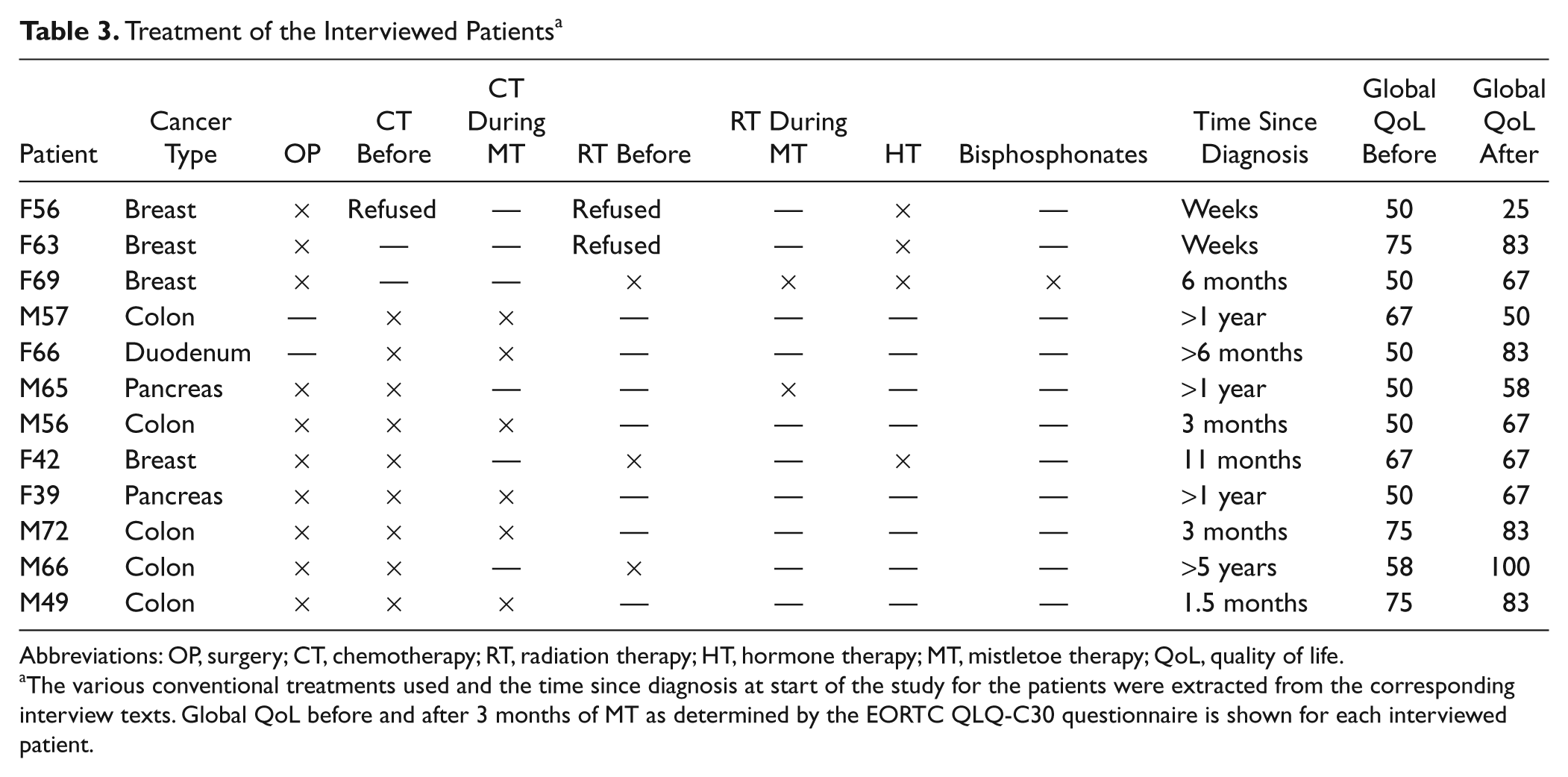
Abbreviations: OP, surgery; CT, chemotherapy; RT, radiation therapy; HT, hormone therapy; MT, mistletoe therapy; QoL, quality of life.
The various conventional treatments used and the time since diagnosis at start of the study for the patients were extracted from the corresponding interview texts. Global QoL before and after 3 months of MT as determined by the EORTC QLQ-C30 questionnaire is shown for each interviewed patient.
How Patients Decided to Look for MT
The qualitative analysis of the first interviews (performed at the beginning of MT) revealed the major role played by relatives (n = 4-5) as well as by health professionals (n = 5) in their decision to look for MT, which was often connected with the decision to go to the Paracelsus Hospital in Richterswil. Interestingly, 2 of the relatives (n = 2) worked in the health sector. Also, the acquaintance circle (outside the family) played a role in some cases (n = 3). An interest in complementary, alternative, holistic, or natural medicine was apparent in the case of several patients (n = 3) or of patients’ relatives (1 spouse, 3 daughters). Other impulses to look for a way to receive MT mentioned were patients’ own literature searches (n = 2) and lack of effectiveness of chemotherapy (n = 1).
Patients’ Expectations of MT
Some of the reasons for using MT mentioned in the first interviews can be considered medicinal; namely, to strengthen the immune system (n = 6), the need to use some therapy in situations in which conventional medicine does not (in some cases anymore) indicate any therapy (n = 4, M66 “psychologically it is better to do something against this disease”), to fight cancer and/or to support healing (n = 5), to reduce tumor growth (n = 1), to support chemotherapy in reducing tumor growth (n = 2), because MT (in contrast to hormone therapy in breast cancer) affects the whole body (n = 1), to help overcome the side effects of radiation and chemotherapy (1 each), to become acquainted with the Paracelsus Hospital, in which the patient would like to be hospitalized if inpatient health care is necessary (n = 1), because conventional treatment failed (n = 1), and to ensure multimodal treatment, which was seen as important (n = 1).
Further (rather subjective) reasons mentioned for using MT revealed during the interviews were as follows: to ensure that everything possible has been done to counter the disease (n = 2); to support internal emotional and physical strength (n = 2); because of trust in one’s physician (n = 1); because of a critical attitude toward chemical medications or conventional medicine (n = 2); to remind the patient that he can find a way to deal with his situation (n = 1); and to make one’s own contribution to treatment (n = 1).
Other Therapies and Support
During both first and second interviews, information was revealed on the other—conventional (see Table 3) and CAM—therapies that had been undergone or were being undergone by the patients. To improve the understanding of the various patients during this study, these and the following results are shown on an individual basis, always indicating the patients by their gender and age. Most patients had undergone surgery (n = 9). Chemotherapy and radiation had been avoided/refused by one patient each. In some cases, patients were undergoing chemotherapy during the 3 months covered by the present study (n = 6). Some patients were also making use of radiation (n = 2), antihormonal therapy (n = 4), and one was additionally using bisphosphonates for bone metastases. In the majority of cases, MT was used as an add-on therapy to conventional methods (chemotherapy, radiotherapy, or surgery), mainly with a secondary, supportive character. Whereas all the surgery interventions had been performed before the 3 months of MT, most (8 out of 12, see Table 3) underwent chemotherapy or radiation therapy at some point during the 3 months covered by the present study. In only one case did a patient (F56) decide not to receive the conventionally indicated adjuvant chemotherapy and radiotherapy for breast cancer. But since this patient had already undergone surgery and was having antihormonal therapy, it could not be claimed that MT was being used as an alternative treatment (Table 3). Therefore, the frequently heard criticism that patients may refrain from using potentially curative conventional therapies and instead favor MT is not supported by the interview results. On the contrary, the conventional treatment of the interviewed patients can be classified as largely appropriate.
The interviews revealed a wide range of nonconventional therapies and other activities that played a supportive role for the patients and might therefore have contributed to coping, namely, eurhythmy (F56, against depression), family constellation analysis (F56), Shiatsu (M65), lymph drainage (F56), acupuncture (F56, against pain), psychotherapy (F42), healer (F39), homeopathy (F39 and M72), reflex zone therapy (F39), mind–body therapy (M49), self-massage with an essential oil (M66), painting (M49), and intense religious experiences (M57 and F39). Here again the results are somewhat different from those of the questionnaires, with many more items mentioned during the interviews. Taken together, this shows that only one third of the interviewed patients (F63, F69, F66, and M56) did not make use of other CAM therapies, did not undergo psychology-related therapies, or did not perform activities with supporting character.
The Meaning of the Disease to the Patient and Coping
At the beginning of MT, most patients were convinced that the disease had a particular meaning to them and that this influenced coping; when asked whether this meaning might have influenced the therapeutic strategy, however, only a few (F56 and M49) thought it had.
Some patients saw the disease as a chance or clue to change their professional life (M65, M56, F42, and M49), improve personal relationships (F42 and M65) or revisit/process past events (F56 “these are very subtle things from my personal history, that mainly happened in childhood . . . the corresponding energy could only now be set free, so that I can finally come to my truth, to what I am”), live with more self-awareness (F39 and M49) or accept their own limitations (F66, “I am not as fast as before or when I’m tired, I just do what my body says,” F42, “I try not to let myself be pushed . . . I try to do just one thing after the other”). Others regarded the disease as a teacher (F56 “. . . who shows me what is happening with me at each moment”), as the result of genetic predisposition influenced by deficient nutrition (M66), as a statistical accident/defect (M65 and M72), and as a test/challenge (M72). Attributing a meaning to the disease was often associated with suspected cause–effect relationships, implying that the patients thought that their cancer had at least partially been caused by unfortunate happenings and/or circumstances in their previous biography (F56, F63, M65, M56, F42, M66, and M49).
Patients’ Appraisal of MT
The following positive changes were reported by patients after 3 months of treatment as being probably linked to MT: less depression (F63, “[Mistletoe therapy] is very good for me and I would recommend it to everyone . . . the strongest effect I felt was . . . on my mood . . . I had a strong tendency for depression and now I can manage”), increased emotional stability (F63, “I don’t let things affecting me so dramatically . . . I strongly believe that it is due to the mistletoe therapy,” and F42 “after starting the treatment . . . something changed . . . I feel now more balanced”), and feeling stronger (F56, “[Since the start of the mistletoe therapy] I feel stronger inside, this gives me energy”). Some patients experienced a reduction in pain: In one case, this reduction concerned arthritis (F63, “one can’t make it [the arthritis] disappear, but the pain is not that strong anymore . . . I can do some handiwork again . . .”). M65 suspected that he had never had a cold during the 3 months that he had MT, because he believed that under normal conditions he would have had several. M65 mentioned as well that he suffered from the side effects of radiotherapy and that he did not know whether these would have been worse if he did not have MT at the same time. One patient (M56) said that MT supported him in developing a coping strategy in that it helped him to be often aware of the disease (probably through the frequent injections).
MT Side Effects Mentioned by the Patients
Analysis of the second interviews revealed that in some cases MT had led to reactions that might be considered side effects, even though some of them—in particular the local ones—are expected reactions on subcutaneous MT. Redness (F69, M57, F66, M56, and F42) and hardening (F66 and M56) were classified by the patients as moderate, except in 3 cases in which the reaction after the first injection was strong (M65), a higher concentration was tried (M49), or the patient injected repeatedly at the same point (M72). Systemic reactions were perceived by one patient (M65, tiredness, fever, muscle pain, sleeplessness, and problems in concentrating). In no case, however, did the patients interrupt MT because of these reactions.
Perceived Changes in QoL and in Coping During the 3 Months of MT
As summarized in Table 4, after 3 months of MT, some patients mentioned a new kind of acceptance and further interpretation of the disease (F56 “I understand now that I have come much closer to my disease”) and a stronger vitality (F56 “I feel stronger inside, which gives me energy,” F63, “I’m convinced that I’m healthy now,” F69 “Sometimes I think I’m really healthy . . . why should I do the therapies if I am feeling so good?,” M66 “I shifted to a more positive attitude . . . I can again go on hiking tours for several hours without any problem”). For other patients, those improvements meant more autonomy (F63 “I don’t allow things to affect me so dramatically . . . I can defend myself”), and more self-awareness (F63, “I live more awarely now . . . my time is more fulfilled . . . I can select more, I take some things more seriously and occupy myself with them, excluding other things . . . I feel more self-assured . . .,” M66 “I live more aware of myself, I do what I love to do . . . and if I can afford something, I do it because I don’t know how long I will live . . . now if it doesn’t suit me to do a thing I don’t do it . . . I feel more free from conventions, while I used to do things I ought to do”). F39 perceived a positive effect that she could not objectively describe, but also mentioned that she felt that she was doing better in general, managing to more efficiently convert her ideas into actions and—what was new and very important for her—her family was accepting this change. For M72 it was so important to communicate that he was doing better that he had brought photos of himself cutting wood to show the interviewer and further reported that his tinnitus problem was gone (which he attributed to the homeopathic treatment undergone parallel to MT).
Summary of the Interviews Analysis Concerning Perceived Changes in QoL, in Coping, and Personal Achievements After 3 Months of MT a

Abbreviations: QoL, quality of life; MT, mistletoe therapy.
Information on the various indicated parameters were extracted from the corresponding interview texts.
Only one patient (M57) reported a decrease in QoL, which can be attributed to the strong side effects of the simultaneous chemotherapy, and passed away shortly after the second interview due to progression of the disease; this was the only patient in a terminal situation to be interviewed. Nevertheless, this patient mentioned that he still had hope and his spouse—who participated in the interview—felt that she and her husband had become closer to each other because of the process of choosing and doing MT together.
Some of the patients undergoing chemotherapy and MT simultaneously had almost no side effects and were doing better after the 3-month period, but they were not sure whether they were feeling better because of the MT, because the chemotherapy had been effective, or because the side effects of the chemotherapy had diminished (F66, M72, M56, F39, M66, and M49).
Reported Personal Achievements During the 3 Months of MT
During the second interviews, it became apparent that most interviewed patients—or their loved ones—had new achievements to report on, which were perceived as important (see Table 4). These achievements constituted the only content analysis category that was established a posteriori and comprise a variety of alterations in social behaviors, changes in professional life, new projects, a new feeling of liberation, as well as increased capacity to make own decisions and to establish priorities.
For F56, the mentioned personal achievement corresponded to a strengthening of her beliefs and better coping with earlier traumatic experiences, and resulted in improved self-awareness, strength, and freedom (“I can finally stand up for myself and fulfill my needs”). It is however conceivable that this process was difficult, which would explain the reported decreased global QoL on the EORTC QLQ-C30 questionnaire (Table 3). F63 mentioned that she did not take things as seriously as before, could better distinguish between important and less important things and say either “yes” or “no” when necessary. F69 found that she was doing so well that she decided to book a trip to visit her daughter living far away even though she disliked travel. F39 had the impression that her own will was back and that she managed better to put her ideas into practice; she decided to go to a Christmas market in another country.
F42 managed to have a personal need—that her activities should not disturb her own daily rhythm—recognized both by the health personnel responsible for her chemotherapy and by her employer; furthermore, she reported a feeling of liberation (“I now feel in terms of close relationships that I don’t always have to be everywhere . . . I can set boundaries for myself . . . it’s a relief”).
M72 described that he had started several new projects (“and there is a new project . . . I have to set up a new horse stable . . . look after the tack room . . . there is a new horse and I am taking care of him . . . I don’t fear anything—absolutely nothing; I don’t have dark thoughts . . . I feel fine and I have my projects . . . and I have a new computer”).
M65 managed to solve a difficult and stressful professional situation, thereby achieving a reduction of the pressure that had been put on him and free capacity to dedicate himself to his spouse, whom he had neglected before (“that’s over now and that was a big relief . . . I’ve needed decades . . . to realize everything she had to accept . . . I just didn’t notice it before . . . it is a shame”) and started to do something new, namely Shiatsu, which he felt helped him further.
Furthermore, M56 managed to set limits to his professional stress (“I do only what I can, not any more than 100%; I feel light, I can just say I’m not there and I know now that the others respect this”) and perceived improvements in his social life (“One has almost closer friendships. I’m no longer subject to social obligations or think that I have to behave in a certain way . . . that’s absolutely over”).
Almost at the end of the 3 months, M49 decided to quit his job and accepted another one in which he could work part time: “I think that’s a new challenge, which I find exciting and stimulating, in a place where I’m taken seriously . . . the position was described as 80% part time and I don’t want to work more than that.” He also changed his attitude toward his acquaintances (“I’ve realized that I’ve always have been very passive in social relations . . . I’ve always waited until someone phoned . . . I still have this tendency . . . now I try to actively contact people . . . I want to take care of this and strengthen it”), bought a new computer, and started to use the Internet for e-mailing as well as getting information on cancer and inputs from other cancer patients.
Discussion
Strengths and Limitations of the Study
The results reported in this work derive in part from the questionnaire analysis and in part from the content analysis of the interviews. This exploratory combined approach therefore comprises qualitative data (themes detected in the interviews and illustrated by quotations) embedded in a quantitative environment (data from questionnaires and quantitative results of the interviews). By using qualitative and quantitative data, the study sheds some light on the advantages and disadvantages of both approaches.
Limitations of the study are the small number of patients (25 patients participated in the study, of which 12 interviews could be analyzed), lack of comparison group and of a defined treatment protocol. The patients were free to make use of additional therapies and the results shown in the Tables 1 and 3 as well as those described in the subsection “Other Therapies and Support” show that the patients indeed did actively make use of this freedom in what concerns conventional and CAM-therapies as well as supporting activities, both before and during MT. In particular the interviews analysis has delivered in-depth information on what happened during the three months of MT, revealing that in most cases at least one conventional therapy (chemotherapy or radiation therapy) and at least one additional therapy/activity had been done concomitantly to MT. Therefore, no cause–effect relationship can be demonstrated between MT and changes in QoL. Because of personnel limitations, only a part of the patients presenting to the hospital during the recruitment period could be enrolled in the study; however, no selection of patients on the basis of their disease or health status was performed.
Progression of QoL During the 3 Months of MT
Analysis of the EORTC QLQ-C30 questionnaire revealed statistically significant improvements in the role and emotional functioning scales as well as a decrease in fatigue (Table 2). This questionnaire has previously been used in several clinical studies to assess the effect of MT as an add-on to different conventional therapies with benefits either in the sum score or in defined scales (pain, diarrhea, insomnia, nausea/vomiting, as well as role functioning) being detected in some but not all of the studies (see Kienle and Kiene 24 for a review from the studies published until October 2009).
Although a detailed patient-based comparison of the individual EORTC QLQ-C30 scores and the corresponding interview text is beyond the scope of this article, it can be said that the results of the content analysis of the interviews showing a higher vitality and autonomy of the patients are in line with the improvements in the role and emotional functioning scales. Interestingly, MT has been shown to lead to an improvement of autonomous coping with cancer in an individual patient data meta-analysis of previously published studies on psychosomatic self-regulation. 25 Although this latter approach (high patient number, one small self-administered questionnaire, long-term therapy) strongly differs from ours (small patient number, detailed questionnaires and interviews, short-term therapy), the results point in the same direction. A survey on patients’ perception of health status carried out on women with breast and gynecologic malignancies showed that CAM use (and MT corresponded to 77% of it) is associated with a better coping with the disease. 26 The statistically significant decrease in fatigue during MT detected in our study by the EORTC QLQ-C30 questionnaire supports results from previous studies that included breast cancer patients being treated with chemotherapy 5 and corroborates the higher vitality of the patients mentioned during the second interview. Furthermore, a decrease of cancer-related fatigue associated with MT was shown in a case report. 27
As mentioned above, the results of both the EORTC QLQ-C30 questionnaires and of the interviews point toward an improvement of QoL. We further interpret the fact that the patients spontaneously reported considerable personal achievement after 3 months of MT as a reflection of that improvement of QoL. Interestingly, the mentioned achievements were very varied—each patient had his or her own needs and these achievements correspond to different impulses. Nevertheless, all of them were perceived by the patients as positive developments and are likely to have resulted in an improvement of coping with the disease by changing conditions associated with subjective stress. The strength required to achieve these changes is probably associated with the mentioned increases in vitality and autonomy.
Our observations on QoL during MT are in line with the conclusions of several systematic reviews of the literature on MT clinical trials that have been published recently and included QoL as an outcome.1,3,4,6,24 Even though the quality of the existing trials is heterogeneous, all reviews recognize at least some evidence that the use of MT can lead to the improvement of several QoL outcomes. For example, the Cochrane review refers to 16 examples of these trials having QoL-related outcomes, with 14 of them showing some evidence of a benefit, 2 of which (breast cancer patients during chemotherapy) were considered to be of high methodological quality. 6 In a very recent review, 26 randomized and 10 nonrandomized trials were mentioned, with 22 showing a QoL improvement. 24 This latter review differentiated between QoL outcomes, coming to the conclusion that the benefits most consistently concerned mainly psychosomatic self-regulation; fatigue, sleep, exhaustion, and energy; nausea, vomiting, and appetite; and emotional well-being and ability to work. Our results not only corroborate the benefits in several of these parameters but also add in-depth information to them. In particular, the results of the interviews analysis shed some light on how these improvements are perceived by the patients and how they might translate in their daily life.
Did the Patients Think That Improvement in QoL Was Related to MT?
Although most patients answered the question “What influence has MT had on your QoL during the last three months?” from the nonstandardized questionnaire on therapies with “improvement” (8 out of the 12 analyzed interviews, other possible answers being “no influence” and “worsening,” data not shown), only 3 patients (F63, F42, and M66) attributed the perceived improvement of their QoL explicitly to MT during the interviews. This discrepancy can be explained by the possible suggestive potential of the questionnaires or by patients’ own expectations being stronger while filling in the questionnaires. Nevertheless, during the second interviews most patients reported clear improvements of some aspects of their QoL compared with the situation 3 months earlier. Moreover, the nature of the interview texts 20 (not shown) revealed clear differences between first and second interviews, with most patients showing a more positive attitude toward their situation/life, and becoming more talkative and willing to reveal more personal attitudes/events during the second interview than during the first. That the patients had learned to deal with their disease better during the 3 months, even though approximately half of them had known about their disease for 6 months or more at the start of MT (see Table 3), cannot be excluded. Also, the fact that at the time point of the second interview the patients were more familiar with the interviewer might have played a role. Finally, this development can be related to the additional therapies that the patients were doing during the 3-month period. In particular, 8 of the 12 interviewed patients were undergoing either chemotherapy or radiation therapy between both interviews (Table 3). These therapies are likely to have affected coping with the diseases either per se or because of the associated side effects. Finally, the nonconventional therapies and other activities with a supporting role (see above), which the patients practiced concomitantly to MT, have probably influenced coping with the diseases in a positive way.
Nature of the Observed QoL Improvement
The patients often appreciated the feeling of being able to control their anticancer therapy by undergoing MT, for example, by doing something in situations in which no conventional treatment was possible, and/or by participating actively in a multimodal treatment concept. In some cases, MT seemed to bring together family members, who until then had had different opinions on therapeutic choices or on disease perception, thereby fulfilling psychosocial functions. Therefore, it is likely that MT might have played a role in improving QoL, which was not confined to the distant goal of tumor-reduction, but can be seen as a chance to consider personal preferences, concepts, and settings and to integrate the help of their loved-ones. In this context, it is worthwhile to discriminate between the different components of MT, as applied in the real-life setting used in the present study: on one hand, the mistletoe preparation itself, and on the other, the setting in which the mistletoe preparation was applied. This setting comprised the subcutaneous injections (often performed by the patient), the intense personal contact with health professionals that is characteristic of CAM, and the additional contact with the interviewer.
Implications for Future Research and Integrative Care
By offering a new treatment context (self-application might have played a role), MT offered the patient the possibility to deal with the disease personally, which was very much appreciated. Furthermore, many patients seemed to need a congruent multimodal therapeutic strategy (conventional medicine and/or CAM) related to their individual attitudes/opinions. Since participation in the therapies’ decision-making process, psychosocial considerations, and personal opinions seem to play a role in patients’ QoL, more attention should therefore be given to such subjective variables by the health professionals (physicians, nursing personnel, psycho-oncologists, and CAM specialists). These patients’ needs and how they affect QoL should also be considered when designing (randomized) trials on cancer therapies.
Finally, the results of the content analysis of the interviews show that the relatives of the cancer patients and the health personnel (including nurses) have a strong influence on the MT decision-making process. The experiences and the opinions of these groups, about how the various therapies affect the patients’ well-being, deserve further investigations.
Conclusions
Mistletoe therapy was adopted by the study patients mostly with a supportive aim and seemed to offer a platform for an integrative coping with the disease, which in itself is likely to have helped the cancer patients, inasmuch as it gave them hope and probably increased their motivation to deal with this devastating disease. During MT, the patients often perceived an improvement of QoL which was associated with a higher vitality and autonomy, and translated into clear-cut personal achievements.
Our observations suggest that MT, with its various components—mistletoe preparation, repeated (self-)injection, CAM setting with intense personal contact with health professionals—and as part of a multimodal therapy seems to contribute to an improvement in QoL and a superior coping with cancer.
Footnotes
Acknowledgements
This paper is dedicated to the patients who agreed to participate in this study, thereby sharing with us and with the readers the experiences that they were having in a very challenging period of their lives. We are also indebted to the patients’ relatives, who made possible their participation in the study and also took part in the interviews, as well as to the recruiting medical doctors, in particular to Dr. Stefan Obrist. We thank Dr. Sarah Haile (University of Zurich, Switzerland) for statistical advice and Dr. Heather Murray (University of Zurich) for checking the English.
Mathias Brandenberger is presently at Psychosomatic Clinic Sonneneck, Wilhelmstrasse 6, 79410 Badenweiler, Germany.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This work was partially supported by Weleda AG (Arlesheim, Switzerland).