
Abstract
Introduction:
The introspective experience of cancer patients using mistletoe therapy has received little scientific interest, although it is crucial for a holistic understanding of this therapy. This study contributes to patient-centered research and treatment by documenting the subjective experiences of individuals undergoing mistletoe therapy.
Methods:
In this qualitative, explorative study, 20 outpatients with a history of various cancer types were recruited from Arlesheim Hospital (Arlesheim, Switzerland). All patients received subcutaneous mistletoe therapy for at least 2 years (median 7.5 years). Data was collected through 2 semi-structured, in-depth interviews per patient. Qualitative content analysis was applied to examine the data. The individual experience of mistletoe therapy was analyzed in relation to 6 predefined levels of human experience: physical, vital, emotional, mental, spiritual and social. In addition, 3 further aspects, considered as cross-dimensional perspectives, emerged out of the material: warmth, immune strengthening, and general wellbeing.
Results:
Data analysis revealed considerable heterogeneity among patients’ experiences with mistletoe therapy. The importance of specific aspects became apparent, such as increased vitality to manage daily life, greater emotional and mental stability, warmth as a multidimensional phenomenon, feelings of safety and protection through mistletoe therapy, heightened self-awareness and improved self-care, as well as sensations of spiritual connectedness.
Conclusions:
Prior to this study it had not been shown that cancer patients using mistletoe therapy do have observations on different levels of experience. These results may lead to a deeper understanding of patients receiving mistletoe therapy, enabling them to be supported in a more holistic way both during mistletoe treatment and on their life path. Further investigations into the effects of mistletoe therapy on the emotional, mental, and spiritual level are warranted.
Introduction
Extracts of European mistletoe (Viscum album L.) are widely used and studied as supportive treatment by patients diagnosed with cancer. About half of all cancer patients use complementary medicine therapies worldwide,1 -4 and in German-speaking countries these are mostly mistletoe extracts.5 -7 Mistletoe extracts contain many highly interesting pharmacological compounds, such as lectins, viscotoxins, phenolic acids, flavonoids, and polysaccharides.8 -10 Preclinical investigations have shown that mistletoe extracts can induce the release of pro- and anti-inflammatory cytokines, protect DNA from cytostatics-induced damage and lead to a specific COX-2 inhibition.8,11 Their subcutaneous application, also known as mistletoe therapy (MT), has been shown to affect both biological processes, especially immunomodulatory changes,12 -16 and clinical outcomes, in particular in relation to improved quality of life (QoL) and survival.17,18 The immunomodulatory properties, for example, are associated with a reduction in neutropenia rates 19 and a release of beta-endorphins, which have a mood-brightening and pain-reducing effect. 20
The effects of MT have been shown in numerous quantitative, but few qualitative, studies. MT has been shown to improve global QoL, fatigue, insomnia, appetite, pain, and patients’ tolerance of standard oncological therapies in meta-analyses,21,22 randomized controlled trials (RCTs),23,24 and non-randomized studies of interventions (NRSIs).25,26 Such effects were also reported by MT-experienced physicians, in a qualitative interview study,27,28 as well as other effects including increased vitality and sensations of warmth and reduced susceptibility to infections. This study revealed effects attributed to MT by physicians, which have not yet been investigated in clinical trials. Furthermore, very few studies have directly addressed patients’ subjective experiences of MT through in-depth interviews. A systematic review by Evans et al. based on the question “What are cancer patients’ views on and experiences with the use of MT?” yielded only 3 publications using a qualitative approach to address the inner world of patients. 29 Only one of these explicitly addressed patients’ experiences during subcutaneous MT. 30 In this study, having used MT for 3 months, participants observed a life of greater self-confidence, autonomy, and vitality in this period of time. However, only 3 of 25 patients could clearly assign their perceptions to MT. Thus, knowledge about patients’ experiences with MT is very limited.
It is not clear yet whether patients are able to distinguish between different levels of experiences of MT through introspection. As defined by Nunan et al. introspection is “the process of observing and reflecting on one’s thoughts, feelings, motives, reasoning processes, and mental states with a view to determining the ways in which these processes and states determine our behavior” (p. 115) 31 or by James et al. “looking into our own minds and reporting what we there discover” (p. 185). 32 As summed up by Wallendorf and Brucks, the method of introspection has been used in “psychology (including social, cognitive, psychoanalytical, and phenomenological), sociology (symbolic interactionism as well as other fieldwork-based studies), and anthropology (cultural and linguistic), as well as consumer research”.33 -39 Lapping-Carr and Heavey are even more precise and define “pristine inner experiences” as “momentary” experiences that are not yet colored by interpretation. 36 Researching these experiences and enabling participants in describing them is reported as highly valuable in helping uncover facets of psychological functioning as well as in scrutinizing gathered information from questionnaires and the like.
The present lack of information on patients’ introspective experiences with MT and the potential for further exploration of MT’s effects prompted us to perform the present exploratory study. Holistic treatments, which address the whole person on different levels of their existence, can be fully understood only by qualitative research. Qualitative research focuses on people in all their facets, aiming to reach their inner core, and reveal the inner world and secrets that are inaccessible through physiological measurements or questionnaires. Qualitative research also aims to explore possibly new, hitherto unknown effects of medical interventions, which could then later be studied by quantitative clinical research. We were motivated by the importance of understanding cancer patients’ perspectives on MT in order to purposefully target treatment and research to their needs in the future. 40 Our aim was therefore to explore cancer patients’ experiences with MT, initially on 6 differentiated levels: physical, vitality, emotional, mental/consciousness, spiritual, and social. These predefined levels then became extended and differentiated through the patients’ experiences.
Methods
Study Design and Participants
The study was set up as a single center, exploratory study of qualitative design with cancer patients undergoing subcutaneous MT (with the mistletoe extract Iscador®) at Arlesheim Hospital, Arlesheim, Switzerland. Reporting is according to the COnsolidated criteria for REporting Qualitative research (COREQ) guidelines 41 (completed COREQ checklist is available in Supplement 1). The experiences of MT were examined using 2 semi-structured, in-depth interviews and drawings. The approach of introspection was chosen to gain a first-person observation that will bring insights that are hardly accessible by a third-person view34 -36,38ta,39 and has not been investigated before.
Sampling strategy
Initially, a total of 15 to 20 participants was set to maximize thematic saturation. Participants were purposively sampled42,43 to achieve broad heterogeneity in terms of gender, age, cancer type, duration of disease and MT, and the specific mistletoe host tree. Only German speaking, adult cancer patients (≥18 years), treated with subcutaneous MT (Iscador®) for at least 6 months were included in the study.
Data collection
Data collection was performed by semi-structured interviews as well as patient-completed drawings and paintings on pre-printed body outlines. Written, informed consent was obtained prior to the first interview and verbal consent obtained again prior to the second interview. Patients were invited by letter prior to attending their regular appointment with their oncologist at the outpatient department at Arlesheim Hospital. Concomitant therapies were recorded on a separate form (see Supplement 2).
Interviews
Development of the interview guide
Pilot interviews carried out on the oncology ward at Arlesheim Hospital by AM revealed that 2 interviews per person were necessary. The in-depth and personal nature of the questions turned out to require a relationship of trust between the interviewer and the patient. Furthermore, it became clear that a certain time until the second interview was needed for the patients to reflect up on the questions in order to enable a greater depth in a second interview.
To develop a semi-structured interview guide, an extensive literature search was conducted on previously studied topics related to MT, cancer and healing. Research questions were developed and further refined in the pilot interviews with the patients. They were further shared with oncologists, art therapists and researchers for reflection. There it became clear, that these questions were not suitable for inpatients, who are challenged by acute somatic or psychological distress. So we decided to perform the interviews with outpatients.
The chosen questions were intended to capture the individual experiences from a holistic perspective, with the focus on the question as to how a person may experience MT (interview 1, question 1, 2 and 3, interview 2, questions 1a, 1b) and cancer (interview 1, question 1 and 3, interview 2, questions 2a-2d) on different levels of experience, as well as what meanings terms such as “healing,” “health” and “sickness” (interview 2, question 3b) hold for a cancer patient. The holistic anthroposophic concept of the “4-fold” human constitution was used as a starting-point since Anthroposophic Medicine has led the way for implementing MT in cancer therapy and research.44 -47 Anthroposophic Medicine understands the human being not only as a material being, but also in its non-material existence, being differentiated into the physical body, the vitality body, the soul and the higher self. This concept, being very complex in its details, was then simplified to make it as comprehensible as possible for patients. In this way, according to the interview guide, 6 levels of human experience were explored: the physical, vitality, emotional, mental/consciousness, spiritual and social level (for the complete interview guide, see Supplement 3). The aim for the interview guide was to provide some structure to the interview, while leaving enough room for individual responses. Furthermore, patients were also asked to draw and paint their experiences along a pre-printed body outline. We hypothesized that the drawings might add information on patients’ experiences on a different level of expression. We strived to investigate if drawing helps the participants to express emotions and inner experiences, and further facilitates them in finding the right words for describing them.48 -52
Procedures of the interviews
All interviews were performed face-to-face by AM. The interviewer and participants were not known to each other prior to the study. AM identified herself to the participants as a medical doctor wishing to understand more deeply how a remedy, in this case mistletoe, affects a person on different levels, and to learn more about the patients’ perspective on mistletoe therapy.
After the first interview, patients received a folder containing several documents: the contents summary, a copy of the patient information, a copy of their informed consent, the form for collecting the concomitant therapies, the interview questions, a sheet with a body outline, and a box of colored pencils. Participants were asked to use the colored pencils to draw the perceived effect of MT on the body outline at home between the interviews, while the completed body outlines were discussed in the second meeting.
Interviews were audio recorded, transcribed verbatim, and proofread. They took place between 05.06.2020 and 14.08.2020. The time span between first and second interviews ranged from 4 to 20 days. The duration of the Interviews ranged from 15 to 85 minutes, with the first interview lasting an average of 45 minutes and the second interview lasting an average of 70 minutes. The meeting place for the interviews was usually in the outpatient oncology department of the Arlesheim Hospital, unless this was not possible, or it was more practical to interview patients at home. The interviews were carried out in the patients’ mother tongue (German or Swiss German). Transcripts were not returned to participants for correction.
The quotations presented in this manuscript were translated into English. The source information for the transcripts are structured as follows: Identification number and time of interview (t1 or t2).
Content Analysis
The analysis in this article focuses on patient’s experience of their MT as revealed in the oral interviews; the drawings and the topics of cancer perception and healing will be reported elsewhere. The qualitative content analysis53 -55 was performed with the help of the MAXQDA 2020 (VERBI GmbH, Berlin) computer software. Deductive-inductive coding was conducted by reading through the texts several times and adding new (sub-)categories to the 6 previously defined categories from the interview guide. The deductive categories were complemented by inductive sub-categories and further inductive categories were built in cases of comprehensive topics stretching over all of the deductive main-categories. A coding frame was established via definitions, inclusion and exclusion criteria for categories and sub-categories (see the coding frame in Table 1, extract of codebook in Table 2 and full codebook in Supplement 4). Categories could also be co-assigned within a single segment of data if several topics co-occurred. The different stages of developing main- and sub-categories involved paraphrasing, interpreting, and coding. Interview transcripts were coded inductively in 2 iterations by AM in consultation with the interpretation group and under supervision of experts in qualitative research (BB, LD, SR). The second coding round was conducted at least 3 weeks after first coding for any transcript to avoid direct influence from immediate memory. Subsequently, each category was examined individually to verify that coded segments of the transcripts were appropriate, congruent, and justified. Eighteen sessions of multi-professional interpretation groups were held to conduct both case-oriented and topic-oriented analyses. These included 3 to 5 people per session (usually 2 alternating groups) including a molecular biologist, biologists, physicists, physicians, and people with backgrounds in nursing science, health/cultural science and clinical research. Patients’ statements were placed within the context of their sociodemographic and biographic backgrounds, and the interpretation groups explored the individual’s perspectives and the selected categories accordingly. Within the interpretation groups, it was possible to create a perceptual space for each interviewee, during which both the spoken and unspoken aspects were explored. To achieve this, body language and facial expression were captured in field notes and reported to the interpretation group. In addition, the rules for transcription included saliences in the way of speaking, pointing out stuttering, loud or soft talking, pauses and speech rate. The results of the interpretation group formed an important basis for the overall data analysis. Participants were not asked to provide feedback on the findings. In addition, a continuous self-reflection process was undertaken by the researchers. Personal attitudes and experiences on the topics studied were reflected upon, as were the researchers’ own expectations and hypotheses. Furthermore, questions such as to how to approach a patient with such personal and in-depth question and, how the interviewees were perceived overall during the interviews (including on a nonverbal level), were also addressed.
Coding Frame.

All the main- and sub-categories are displayed. Indents are marking the sub-categories to the respective higher category above.
Excerpt of the Codebook.

Displayed is an excerpt from the codebook. Illustrated are the 6 levels of experience, for an overview of the definitions of the deductive main-categories. The whole codebook can be found in Supplement 4.
Results
Participants’ Demographic Characteristics
An overview of the characteristics of the patients having completed both interviews is presented in Table 3. The patients were 15 women and 5 men ranging in age from 46 to 83 years (median 62 years). Willingness to participate was high, with only 4 out of 30 people approached declining participation due to personal reasons. Another 6 patients were excluded before or after the first interview because of the defined inclusion and exclusion criteria, or as they had to travel too far for a second interview, or for other personal reasons. Breast cancer was the most common cancer type among interviewees (n = 11), including patients with relapse (n = 3) and those with more than one cancer type or with metastases (n = 3). Other diagnoses were prostate cancer (n = 3), colon cancer (n = 2), malignant melanoma (n = 2), ovarian carcinoma (n = 2), bladder carcinoma (n = 1), chronic lymphatic leukemia (n = 1), endometrial carcinoma (n = 1), and tubal carcinoma (n = 1), with 8 patients diagnosed with multiple cancers or metastases. Three patients had active disease, two with metastases (P. 530 and P. 535) and one with a second primary cancer diagnosis (P. 523). Therapy duration of MT at the time of the interviews was 2 to 30 years (median 7.5 years). Nineteen Patients also received other therapies concurrently (at the time of the interviews): allopathic medication (concerning cancer or other, 13 patients), naturopathic medication (8 patients), supplements (13 patients), also osteopathic, art-based, psychotherapeutic and other therapies were being applied, but only 6 patients were still receiving standard oncological therapies (see table in Supplement 2).
Patients’ Characteristics.
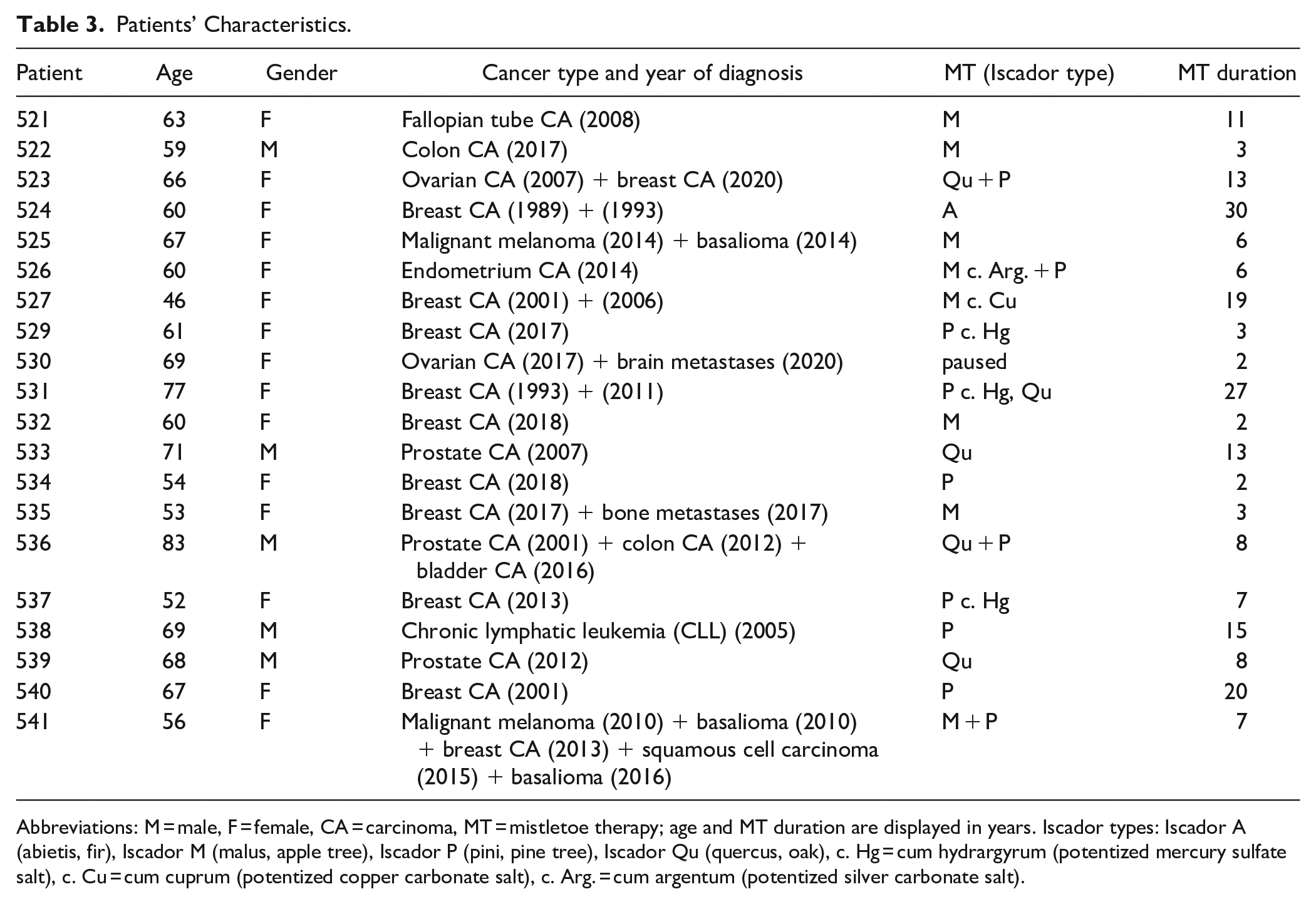
Abbreviations: M = male, F = female, CA = carcinoma, MT = mistletoe therapy; age and MT duration are displayed in years. Iscador types: Iscador A (abietis, fir), Iscador M (malus, apple tree), Iscador P (pini, pine tree), Iscador Qu (quercus, oak), c. Hg = cum hydrargyrum (potentized mercury sulfate salt), c. Cu = cum cuprum (potentized copper carbonate salt), c. Arg. = cum argentum (potentized silver carbonate salt).
Content Analysis
For each of the levels of experience defined at the beginning of this article (physical, vitality, emotional, mental/consciousness, spiritual, and social), different individual experiences were ascribed to MT. By using an inductive approach in addition to deductive analysis, additional topics emerged from the material, enriching and differentiating the analysis. These included all the inductive sub-categories, as well as the additional main-category of “cross-dimensional perspectives” including experiences of warmth, immune strengthening and general wellbeing with qualities extending across all the deductive categories.
The coding frame in Table 1 illustrates the various categories: (1) the physical level at which, for instance, regression of 2 non-melanoma skin cancers could be observed, (2) the level of vitality, where a quality-of-life-enhancing increase in strength was experienced, and (3) the emotional level, at which stabilization, relaxation, mood brightening, and a strong sense of security were related. Furthermore (4) the level of consciousness, whereby an increase in self-perception, self-efficacy, self-confidence, and self-care was described, and (5) the spiritual level, on which insights into an experience of an immaterial force of the MT occurred, including an intimate feeling of being at home, a sense of being protected, as well as being connected with a higher (divine) entity. Finally explored were (6) the social level on which the effects of the processes of the conscious levels were expressed, and (7) the cross-dimensional perspectives with differentiated experiences of warmth, a strengthened immunity and a general sense of wellbeing. Table 4 displays the ascribed experiences of the participants to the 6 deductive main-categories as well as the 3 inductive categories contained in “cross-dimensional perspectives.”
Patients’ Experience of MT on the Differentiated Levels of Perception.


Abbreviations: M = male, F = female, CA = carcinoma, immune str. = immune strengthening, general wellb. = general wellbeing; age and mistletoe therapy (MT) duration are displayed in years. Green fields display patients expressing an experience related to MT and red fields no experience on the respective level, white fields correspond to no statement (eg, experiences weren’t clearly attributable to MT for the patients). The column of the sum displays the number of categories with observations (change or no change). The table is sorted according to the total number of different levels with stated experiences.
Physical Experience
The term “physical” refers to the purely material structures of the human body (ie, stripped of the concept of vital forces keeping it “alive”). Two patients mentioned a regression of non-melanoma skin cancers as a result of MT. Several reports concerned the experience of warmth, where patients felt or even measured a rise in body temperature after injecting. Also a strengthened resilience against colds and improved immune parameters were described. One interviewee emphasized the role of the physical level in connection with his conscious activity: “The mistletoe supported me in a way that it gave me this stable physical foundation, and thereby I also became free again from the physical complaints, then came back to reflect more and was able to reconnect more to my original motivation in life.” (P. 522, t2).
Vitality Experience
“Vitality” here refers to the domain of life forces, that is, the forces keeping the physical structures alive and maintaining their form and function. Descriptions like one’s own “vital body” being revived again, as related by one of the patients (P. 522), were given. He reported feeling more alive inside his body and more in touch with himself as a whole person. Indeed, most of the interviewees reported a considerable increase in vitality and strength, being less tired and exhausted. Patients in general related having more energy with improved QoL in terms of being able to manage everyday life, and further feeling supported or relieved with regard to their emotional inner life. As one patient reported “So, so tired, so indefinably tired, I used to be much more tired before the MT. […] I don’t have that basic tiredness anymore, as I always had before. Before, there were days when I had the feeling that I had no energy. Undefinable. I don’t have that anymore.” (P. 521, t2).
Emotional Experience
On the emotional level, MT was observed to induce an emotional brightening, relaxation, and stabilization, which in turn was connected to other levels of experience and further improvements in the patients’ QoL. Perceptions of gratitude, anxiety reduction, mood lifting, emotional relaxation and reassurance were particularly paramount for the patients in this sample population. Attentive kindness toward oneself was described along with a sense of emotional relaxation. The subjective inner world was experienced as more comfortable and satisfied, which further induced a calming on the mental level with respect to jumbled and circling thoughts. Furthermore, emotional relaxation positively influenced vitality and vice versa. Thus, emotional relaxation appeared closely interwoven with aspects of self-awareness and physical sensations.
A sense of reassurance experienced through MT emerged as a relevant topic for the interviewees. Although it was not explicitly inquired about, most of the patients emphasized it with regard to their personal experience. Terms such as “safety,”“protection”, “ground under one’s feet”, “trust”, “being protected”, “protective cover,” and “the feeling of being in safe hands” came up when respondents described the inner sensations attributed to MT. In an impressive complexity of experience, the feeling of safety appeared connected with the vitality, emotional, logical, and spiritual levels while MT was credited with a reassuring effect that worked “from the outside in.” This sense of security attributed to MT also facilitated a rise in self-confidence and self-efficacy from within the participants: “I did not doubt myself, I did not doubt the circumstances, I did not doubt the chemotherapy. Yes, it was unnecessary, it wasn’t very nice, but it was clear: THIS is the way. And I’m convinced that it’s because of the mistletoe, because I’ve seen others who were in a lousy condition, who weren’t morally well.” (P. 523, t1). It is interesting to note that respondents who did not mention any sense of reassurance did not report any other impact of MT on the emotional level either.
Mental/Consciousness Experience
Experiences connected with MT on the mental and consciousness level were related by all interviewees and represent an essential outcome of this study. MT as an act of self-love and self-help held deep connections to notions of increased self-confidence, self-efficacy, and self-care for the patients. Various interviewees had firmly integrated MT into their everyday life. It had become a fixed part of their daily routine with a corresponding assignment of meaning. “It accompanies me. And it also reminds me. […] So it is also a little light. Look after yourself! It makes me aware of how I am doing. Because often in everyday life, a lot of things fall out of sight.” (P. 532, t2). The feeling of being able to direct one’s life stimulated self-confidence and was perceived as supportive with respect to the course of disease and beyond.
Various aspects of personal growth were assigned to MT and appeared as the capacity for self-reflection (eg, being honest with oneself, ridding oneself of habitual patterns), loving self-awareness and self-regulation (being attentive to one’s own needs), self-confidence and self-acceptance. In addition, MT was attributed with the strengthening, relaxing, and stabilizing of mental capacities. The relationship with oneself and self-understanding were emphasized in connection with MT and cancer. Furthermore, some patients reported an increased self-awareness in the present moment, as well as within their own body. However, 5 patients did not report any personal development. They had no specific impetus to deal with the disease or its therapy on a conscious level.
In some cases, the positive feeling toward MT was more intuitive than mental and conscious. Descriptions like MT “does me good” expressed a kind of undifferentiated conviction of MT being beneficial, rather than describing a clearly understood impact of MT. “You don’t feel anything. But I think you do something to improve your immune system. And that makes me feel good, purely intuitively.” (P. 529, t1). Statements like this expressed the “indirect” experience of MT effects, such as the observation of no longer being prone to contract infections, which is a secondary observation in contrast to feeling for example, immediate warmth in the body. Some interviewees even did not want to go without MT anymore as it had become an integral part of their lives. “And I don’t feel like stopping. Because, well that’s interesting isn’t it. […] I never asked myself whether I would stop now.” (P. 537, t2).
Spiritual Experience
In the context of this work, no predefinition of spirituality was given to the interviewees, so that they could tell their experiences free of outside concepts. It was noticeably difficult for the participants to put experiences attributed to the spiritual level into words, or even to consciously grasp and classify them. Some patients ascribed to MT a spiritual experience with “higher powers” - from a vague inkling of inexplicable forces described as something “magical” or “mysterious” to a feeling of being “embraced and protected” or “connected to something bigger.” One patient described “In this respect, I have to say that I have an experience with mistletoe. […] That is something that touched me and strengthened my belief that there is certainly something. A - yes, a spiritual world. So not heaven. No, a spiritual structure that we do not understand and do not need to understand.” (P. 533, t2) MT was considered by patients as a companion on the way “home,” to the innermost self and to total connectedness. One patient described the sense of an “uplifting and connecting power between heaven and earth” (P. 530, t2) “Yes, that just felt strengthening. Or arriving. Or, um, connecting. Like that. [AM: What exactly is being strengthened?] My whole. . . like. . . being. Where I had the feeling that this is, like, um, a kind of arrival.” (P. 530, t2). Four patients described having found a new understanding of life using MT, which enabled them to perceive themselves as being in a constant process of development and to embrace themselves as they really are. Among other things, spiritual openness was also described as a consequence of a marked gain of physical strength and relief experienced through MT (P. 522).
Social Experience
Social aspects appeared only of secondary importance in the context of MT and were always linked to other levels of experience. Patients described themselves as being more empathic not only with themselves, but also with others. Furthermore, an ability to communicate more openly as reported on the basis of emotional relaxation or increased self-confidence: “So if you had a bit of a tendency to be stuck or rather not say anything […] which of course became stronger and stronger due to the periods of illness, that you keep it all bottled up inside you a bit. [MT] dissolved this again a bit, in the direction of also becoming more mentally and emotionally flexible in that context [. . .] Yes, the openness has increased, and with it the relation to myself. . . and. . .and to the world. So it’s both. Before I was more in self-protection mode and now I’m more in a flow.” (P. 522, t2). In addition to this openness, a clearer perception of one’s own limits following a development of consciousness was described: “I have become more critical. I have become clearer… And I am more aware of my limits and also communicate them clearly. I have not necessarily become more pleasant for my surroundings (laughs).” (P. 534, t2).
Cross-Dimensional Perspectives
Warmth
An aspect that emerged from the interviews without having been explicitly enquired about was an experience of warmth in connection to MT. As mentioned previously, we consolidated all reported experiences of warmth into one category to display its multidimensionality. This appeared as a phenomenon that was not only related to body temperature. Several interviewees described “warmth sensations” in connection with MT on different levels: a pleasant warmth in the body after many years of latent coolness for example, or a warming flow up to the tips of the fingers and toes, or a “warm envelope.” It could also be experienced as a rather unpleasant excess of heat in case of mistletoe extract overdoses.
Warmth on emotional and consciousness levels were also perceived by MT users. The emotional warmth was primarily associated with a desire to help oneself, touching aspects of self-efficacy and emotional wellbeing, which further positively influenced social interaction. On the consciousness level, the feeling of warmth was described as a medium through which one’s own awareness could re-establish conscious contact with the body.
Most frequently, several aspects of warmth were described simultaneously: “So today, when I inject now, I would say I feel more awareness. And more warmth. And circulation. […] I have the feeling that everything is warmer in my body. So, all the way to the periphery. So the feet are warmer. The hands. Especially the hands. […] Always a little warm, well supplied with blood. And yes. How can I describe…? It’s like a whole, yes, a presence within my body.” (P. 526, t2).
Immune strengthening
Patients reported the experience of a strengthened immune system through MT by being more resilient against colds, being sick less frequently or not becoming sick at all anymore. “It protects me. It makes me strong. So I realize that, yes sometimes […] I’m the only one who never has anything in this school [workplace]. So ergo, [the one] who is always working. [. . .] Damn – yes, I also want to be at home a bit! No. (laughs).” (P. 537, t1). Furthermore, immune strengthening was experienced as helpful by some patients in reducing the fear of being in contact with other people for example, during the COVID-19 pandemic.
General wellbeing
On a very general level, some of the participants described an improved general condition, general wellbeing or an overall benefit of mistletoe. As illustrated by one cancer patient: “I can tell: It’s good for me. It feels like it is enveloping me. It helps me. It strengthens me. Those are the things that come to my mind about mistletoe. And it carries me, it gives me something as a person. So it’s like, not something where I feel it’s only about cancer. Rather, it is something that is very good for me as a whole. You know, that is good for my health, it keeps me healthy.” (P. 537, t2).
Discussion
Insights Into the Personal Experience of MT
Our study revealed a wide range of experiences with MT by cancer patients. Participants described a multi-dimensional feeling of warmth brought about by MT, not only pertaining to thermal comfort, but also to the emotional and spiritual level, ranging from “warm feelings” to a conscious connection to and a heightened awareness within the body. Furthermore, participants highlighted the emotional aspect of feeling reassured with the help of MT. A feeling of emotional safety found expression in everyday life, for example, through more confidence in one’s own physical strength or in connection with sense of being protected. The application of MT gave participants a feeling of reassurance “from outside” and thereby further mobilized forces from inside, resulting in self-confidence, self-efficacy, and a more conscious appreciation of oneself. The practice of loving self-awareness through the act of applying MT was displayed and further promoted deep experiences of increased self-confidence, self-efficacy, and self-care in many patients from this sample. Various interviewees had firmly integrated MT into their everyday life, some as a self-care ritual. Mental convictions as well as the meaning response56,57 played an important role in the context of attributions to MT. Several patients attributed spiritual experiences to MT, such as a confirmatory sense of “something higher.” They expressed feelings of spiritually support and protection without regard to any physiological effect or any logical explanation of the effectiveness of MT. In addition, a deep sensation of connection to the inner self as well to “something ungraspable” were ascribed to MT.
Participants had a range of cancers at different stages with different prognoses and treatment, which also seemed to shape the individual’s experience with MT. For example, one man with CLL (P. 538) never felt his disease or MT impacting him, in contrast to a woman (P. 535) in acute disease progress. She was undergoing chemotherapy and suffering from pain due to bone metastasis after breast cancer and from severe fatigue, which was alleviated during MT and so distinctly improved her QoL.
Furthermore, the particular life situation at the time of the survey, such as age or social situation also seemed to influence patients’ experience with MT, as did the temporal relationship to the disease itself and the severity of the cancer and having previous experience of MT. One patient in the sample group (P. 523) expressed this when a new cancer (mamma carcinoma) was discovered 13 years after her first tumor (ovarian carcinoma). “This was very present, so this basic safety with taking mistletoe, nothing will happen to me, it was there… Now, not at all. I take it because I know it’s good for me. But from the feeling, from this, so this inner security, it doesn’t exist.” (P. 523, t2). This may support the notion that the experience of MT can at least partially be shaped by the interviewee’s meaning response as described by Moerman.57,58
Furthermore, in the interpretation groups the hypothesis emerged, that a certain mental and spiritual openness seemed to facilitate personal experiences in the analyzed areas. The way patients talked about connected topics such as their personal development, life story, view of life or spiritual path lead to the interpretation that experiences of MT are largely determined by each person’s individuality. For example, respondents with a keen body awareness also observed the effect of MT on the vitality level more intensely than others whose outlook on life was primarily shaped by logical thinking. The hypothesis of the congruence between the patients’ reported experiences with MT and the way they experienced other aspects of life should be further investigated.
Patients’ perceived effects of MT on the non-material levels of their existence were found to be just as important as the purely physical level. This underscores the importance of expanding clinical research to include the “finer realms” of human experience, as has previously been done, for example, in the areas of psycho-oncology with approaches taken including “mindfulness-based stress reduction” or investigations into the unmet spiritual and existential needs of cancer patients.59 -61 However, not all patients attributed a particular meaning to MT or associated it with a special experience, which seems remarkable considering that some of the patients in this sample had been using MT for 20 years and still did not want to quit. It was observed that 3 of the 20 patients (P. 536, P. 538, P. 539) could not relate to the majority of the questions, especially concerning the emotional, mental, spiritual and social level, which were partly felt to be “strange.” They did not identify any changes or specific effects attributable to MT. Rather, these patients related a general “sense of wellbeing” in connection with the therapy, which could not be further specified. These 3 patients noticed the effect of MT “indirectly,” by not having had a cold since starting it. However, all 3 were convinced of the effectiveness of MT. A systemic view could be useful here to examine how patients are perceived and supported by their social environment, for example, their spouse, family, friends, etc., in their respective individual ways of dealing with the disease and their personal resources. For future work, it would be desirable to use the qualitative method of type formation to identify different approaches and ways of coping of people experiencing existential challenges such as cancer, and their respective resources.
How This Study Fits in to Previous Qualitative MT Research
Brandenberger et al. conducted a qualitative interview study investigating patients’ QoL during MT, the meaning of cancer to them and how they coped with the disease. 30 At the beginning and after 3 months of MT, interviews were conducted using the EORTC QLQ-C30 questionnaire. Patients described an increase in vitality, less susceptibility to infections, experiencing less pain, less depression, greater emotional stability, a sense of strengthened self-efficacy, increased self-confidence, an improved ability to cope with their illness, and changes in their social and professional life due to the holistic anthroposophical therapies they received. However, only 3 out of 25 patients decidedly attributed these changes to MT. Thus, other therapeutic interventions or the general inner process in relation to the disease could also be seen as reasons for the reported positive experiences. It is important to note the difference to the present study, in which MT had already been used for at least 2 years (up to a maximum of 27 years) and thus the immediate impact of the cancer diagnosis was generally no longer present (except for 3 participants with active disease). In addition, only 6 of 20 patients were still using other therapies with the aim of treating the cancer.
The results of the qualitative interview study by Kienle et al. with 35 MT-experienced doctors correlate well with our findings.27,28,62,63 The doctors described patients’ improved strength, vitality, thermal comfort, clinical recovery, fatigue, appetite, sleep, pain, resistance to infections, and the amelioration of side effects of toxic anti-cancer therapies due to MT as well as a strengthening on an emotional level and improvement of coping abilities, autonomy, and functional abilities.
Our observations of the impact of MT on QoL are also in line with recent systematic reviews on the quantitatively assessed effects of MT on QoL in clinical trials.17,18,21,22,64,65 As shown in the meta-analysis by Loef and Walach, mistletoe extracts produce a significant, medium-sized effect on QoL in cancer patients. 21 The effect was found to be more pronounced with longer treatment, in younger patients, and particularly marked regarding role functioning, social functioning, nausea, diarrhea, pain and dyspnea. Furthermore, treatment with mistletoe extracts has been shown to have a moderate effect on cancer-related fatigue, approximately equaling the impact of physical activity. 22 Improvements regarding coping, sleep, exhaustion, energy, depression, anxiety, ability to work, as well as emotional and functional wellbeing in general have been shown in addition to reduction in the side effects of conventional treatments, regardless of the cancer type or stage. 18
What is not apparent in these articles, but has emerged from the present study, are the effects of MT on the patient’s inner spiritual experiences, as well as on further aspects of consciousness, such as an increased awareness of one’s own physical presence (facilitated through sensations of warmth) or detailed aspects of self-awareness. Furthermore, accounts of a heightened sense of reassurance and deeper and differentiated introspective experiences facilitated by MT appear to have been missed by previous surveys. An explanation for this might be that the questionnaires used did not explicitly target these levels of patients’ experience.
It is known from studies concerning the spiritual needs of chronic pain and cancer patients that spirituality, inner peace, and a feeling of connection to a higher power positively affect their self-esteem, conveying a sense of purpose in life as well as a feeling of emotional wellbeing and hope.66,67 Furthermore, research on personal growth during the experience of advanced cancer shows that an active search for meaning in connection with illness and the question of one’s own life and death results in personal development. This includes aspects of improved self-esteem, focus on the present moment, increased spirituality and, most often, a deeper appreciation of life and improved social relationships with loved ones.68,69
How This Study Fits in to Previous Qualitative Complementary Medicine (CM) Research
A handful of qualitative studies on cancer patients can be found in the field of CM therapies showing that other complementary therapeutic approaches are also experienced on different levels of human existence.70 -81 Different responses of patients were reported on various levels of experience depending on the therapeutic approach taken. These studies use their individual coding frames and definitions of the respective levels and we use their terminology in the following discussion. Where authors use the same expressions as used in the current study (eg, if they speak of the vital or emotional level), the content may differ depending on their definition. It should be noted that the CM interventions in the studies listed below cannot be compared directly to MT due to their respective difference in approaches, concepts, codings, and backgrounds. Possible differences between MT and other CM methods would need to be examined in specifically designed studies.
In a study of massage, the physical and vital levels played a major role, in turn affecting other areas such as spiritual, mental, or social levels. 80 In the studies on mindfulness-based stress reduction meanwhile, many patient experiences seemed to parallel those described in the present study with MT. Specifically, patients experienced impacts on mental/consciousness and spiritual levels, which in turn further affected the other levels. A spiritual development and increased mindfulness in relation to oneself as well as with regard to interpersonal relationships, both improved abilities to cope with emotions and stress, improved sleep, or reduced pain.70,71,74,75,77,78 In a study of patients receiving acupuncture a pronounced effect on all levels of the human existence was expressed. 76 Interestingly, these respondents described very similar impacts on several levels as the patients in the present study – except for the social level, although this could be due to the fact that this aspect was not inquired about. In a small study concerning homeopathic treatment, five patients perceived improvements on physical, vital, and emotional levels. 81 Finally, in a study about CM rituals, such as mental or physical exercises, prayers, or specific nutritional interventions, patients also reported a physical, emotional, mental, and spiritual strengthening. 73
Strengths and Limitations of the Study
A strength of this study is the qualitative study design itself, which delves deeply into the individual MT experience of cancer patients through 2 interviews per person, capturing a rich and diverse amount of information. The participants’ deeply personal experiences were appreciated in a trusting and open atmosphere through the confidentiality of the setting as well as the interviewer’s empathic listening and authentic interest in the interviewees’ experience. Another strength is the heterogeneity of the sample population achieved through purposive sampling in terms of age, gender, time of diagnosis, tumor type, tumor stage, tumor treatment, type, and duration of MT.
Furthermore, for quality assurance purposes, recognized quality criteria were followed (COREQ Guidelines, 41 for the checklist see Supplement 1), monitoring visits were conducted, supervision by qualitative research experts was provided and the study was accompanied by constant self-reflection. To ensure content quality, 2 coding cycles were conducted independently of each other at a minimum interval of 3 weeks, and regular interdisciplinary interpretation groups were held on a case-oriented and topic-centered basis.
The study has some limitations. The sample population is limited to 2 cultural backgrounds: 18 Swiss-Germans and 2 Germans now settled in Switzerland, white and German-speaking, with secure socio-economic status. The results acquired from this population are therefore not generalizable to other populations (with different cultural backgrounds, social status, age, etc.). Quantifiable statements cannot and should not be made here. Displayed numbers are shown to characterize this sample and cannot be generalized in any way. The purposive sampling method also represents a limitation, since the patients were not randomly included in the study. A selection bias must be taken into account, as this is a single-center study conducted in the context of integrative medicine. The study participants were recruited from an anthroposophical hospital that had specifically been chosen by the patients for MT. Thus, there was a self-selection of patients and any prior skeptical prejudices toward MT or CM were already overcome, suggestive of the participants having had an overall positive attitude toward MT. In contrast, Arman et al. show that patients without previous contact with anthroposophic medicines or therapies can be overwhelmed by the subcutaneous application or the possible side effects of MT. 82 In the present study, such negative experiences only occurred to a limited extent or were put into perspective by the time that had passed since the beginning of therapy, as the patients had found ways to manage them (eg, fear of injections). Due to the method of sampling, patients who had stopped MT due to such difficulties were not included here.
In addition, it was often not possible to clearly attribute patients’ mental or emotional processes to a single causal factor. For example, whether the shock/trauma induced by the cancer diagnosis, or the MT initialized a personal development process or a meaning response which was subsequently attributed to MT. Patients clearly assign supportive qualities on different levels to MT, but cancer itself may often trigger major changes in a person’s life, as was partly the case with participants in this study and is also related in many other places in literature.68,69 As it was formulated by one patient: “You could also say illness is a transformational tool. And many who have gone through illness have also changed. […] And mistletoe helps to go through this process of illness in such a way that it becomes a process of transformation. Mistletoe supports self-transformation.” (P. 522, t2).
In the anthroposophic hospital where the patients were recruited for the present study, cancer is treated with a multimodal therapy concept. Patients underwent several medicinal, supplemental, art and psychotherapeutic therapies besides MT, which sometimes made it difficult for them to precisely attribute the perceived effects to one single intervention. In such cases, the respective patient statements were not included into the present analysis. In most of the cases presented here, the cancer diagnosis, and thus the start of MT, dated back several years and MT often remained the only constant therapy used over time, which might have aided patients to distinguish effects elicited by MT from those brought about by other therapies.
Finally, a potential favoritism bias should be mentioned, since it is possible that patients related experiences with the subconscious motivation to respond in a socially desirable way. To counteract such an effect, the interviewer took great care to create a conversational environment in which the patients felt free and not judged. It should nevertheless be noted, that all interviews were conducted by a female interviewer considerably younger than the patients, at 28 years of age, and this may have impacted patient responses.
Reflection on the Methods
During analysis the question arose of how to distinguish if a patient’s observation was based on a pristine inner experience 36 or whether it was merely a mental interpretation, so acquired knowledge, something the person read or heard and reproduced. However, this was put into perspective by the fact that consequently both – inner experience and conscious interpretation, association, memory, etc. – affected the patient deeply. So it should be emphasized that this qualitative study does not address the question of the efficacy of MT on a physiological or psychological level or any causality, but rather the meaning response of the patients.56,57 The aim of this study was to explore the levels of the subjective experiences of cancer patients with regard to MT. The importance the respondents assigned to MT and how this affected them and their journey with the disease was of interest.
Possible Therapeutic Effects of the Interviews
Some observations led to the hypothesis of a “therapeutic effect” of the interviews themselves. Due to the open and at the same time protected space for conversation, an increase in the patients’ self-awareness became evident during the course of the interviews. This was observed, for example, by how patients articulated themselves, stuttering less and becoming calmer and more precise in their ways of expression. A search for words was seen as indicative of an increasing awareness as interviewees tried to express things they had not put into words or thought of before. 48 There was a noticeable difference in patients’ behavior between interview 1 and 2. An increase in trust, openness and comfort was observed with the interviewees, the time to reflect in between the interviews having enabled them to clarify (subconsciously or consciously) remaining questions concerning their own processes with the disease, the MT and themselves. This finding has also been identified in investigations on the therapeutic effect of qualitative research interviews.83,84 Interviewees are thus not only sharing information but are also affected by the interview process, for example, by coming into the powerful position of a helper, finding a voice, or getting an “observer view” for themselves, which may result in increased self-esteem or new insights about themselves. The result of the great variety and depth of experiences the patients ascribed to MT in this study raises the question of whether the process of introspection could support healing processes and could therefore be used therapeutically.
Implications for Future Research and Integrative Care
To better understand patients’ experiences with MT, it would be interesting to follow the development of patients’ experiences over time, that is, before the onset and during the course of MT. To investigate the role of the therapeutic setting and possible cultural influences, studies should be done in different clinics, including non-anthroposophic settings and different countries. To determine the potential specificity of patients’ experiences with MT, comparison groups without MT and/or with other complementary or conventional medical treatments would be needed. Furthermore, the possible generalizability of the experiences observed in this study should be investigated through prospective investigations with appropriate questionnaires. For certain aspects identified in this study, development of new questionnaires might be necessary.
It became apparent in the present study that the questions used in qualitative research are not only useful as a research tool. They may also stimulate awareness for inner processes and thus may be of value for the inner development of patients. Maybe they could even to healing processes. We suggest to actively empower patients to engage in introspection. Many patients are not used to paying attention to inner experiences and their various aspects, for example, their own body sensations psychological processes, mental insights and spiritual experiences. This raises the important question as to what extent introspection could support healing processes, autoregulation and self-management of patients. Whether this could enhance the effect of MT – or of medical drugs and therapeutic applications in general – is a question that should be further explored. It would also be very interesting to combine or compare MT with mindfulness training in introspection for patients and health care professionals.
The understanding that patients are capable of having differentiated perceptions of medical drug and therapeutic effects could have a profound impact on the attitude of practitioners. This work intends to motivate researchers, doctors, and therapists to develop differentiated inner perceptions of their patients, illness, treatment, and also themselves. This appears to be an important prerequisite for fully understanding the person who is seeking help, incorporating both their outward expression and inner, more personal levels. In this way, a clearer idea of what is needed for individualized and holistic patient care is likely to ensue. With an awareness of the different possible levels of experience, a deeper space for mindful encounter and healing could emerge.
Conclusions
In this study, we observed that cancer patients express differentiated experiences in connection with MT. The experiences with MT reported by the present sample population included various elements on multiple levels: the physical, vitality, emotional, mental/conscious, spiritual, social level, as well as experiences of warmth, immune strengthening, and general wellbeing. Since this research question has not been investigated in-depth before, this first study wants to encourage a more profound understanding for patients’ individual experiences on MT. We presume that the present sample exhibits just a subset of possible experiences and we want to encourage doctors to ask their patients for their individual experiences, in order to receive answers and to be able to support and accompany them in a more profound and holistic way during MT, cancer treatment more generally and on their life path.
Supplemental Material
sj-pdf-1-ict-10.1177_15347354231198474 – Supplemental material for The Introspective Patient Experience of Mistletoe Therapy in Cancer: A Qualitative Study
Supplemental material, sj-pdf-1-ict-10.1177_15347354231198474 for The Introspective Patient Experience of Mistletoe Therapy in Cancer: A Qualitative Study by Annika Mascher, Florian Pelzer, Lorna Jane Duncan, David Dominique Martin, Stephan Baumgartner and Bettina Berger in Integrative Cancer Therapies
Supplemental Material
sj-pdf-2-ict-10.1177_15347354231198474 – Supplemental material for The Introspective Patient Experience of Mistletoe Therapy in Cancer: A Qualitative Study
Supplemental material, sj-pdf-2-ict-10.1177_15347354231198474 for The Introspective Patient Experience of Mistletoe Therapy in Cancer: A Qualitative Study by Annika Mascher, Florian Pelzer, Lorna Jane Duncan, David Dominique Martin, Stephan Baumgartner and Bettina Berger in Integrative Cancer Therapies
Supplemental Material
sj-pdf-3-ict-10.1177_15347354231198474 – Supplemental material for The Introspective Patient Experience of Mistletoe Therapy in Cancer: A Qualitative Study
Supplemental material, sj-pdf-3-ict-10.1177_15347354231198474 for The Introspective Patient Experience of Mistletoe Therapy in Cancer: A Qualitative Study by Annika Mascher, Florian Pelzer, Lorna Jane Duncan, David Dominique Martin, Stephan Baumgartner and Bettina Berger in Integrative Cancer Therapies
Supplemental Material
sj-pdf-4-ict-10.1177_15347354231198474 – Supplemental material for The Introspective Patient Experience of Mistletoe Therapy in Cancer: A Qualitative Study
Supplemental material, sj-pdf-4-ict-10.1177_15347354231198474 for The Introspective Patient Experience of Mistletoe Therapy in Cancer: A Qualitative Study by Annika Mascher, Florian Pelzer, Lorna Jane Duncan, David Dominique Martin, Stephan Baumgartner and Bettina Berger in Integrative Cancer Therapies
Footnotes
Acknowledgements
The authors wish to thank especially the patients who made this study possible by sharing their deep personal experiences. Further, we thank the medical doctors who made the recruitment possible, Bettina Böhringer, Marion Debus, Rainer Penter and Damian Quero. We thank Stefan Rädiker (SR) for external methodical advice. Further, we thank all the contributors of the interpretation groups, as mentioned above, and Susanne Aeberhard for transcribing most of the interviews. We also thank Sarah Monz for polishing up the English in the manuscript.
Author Contributions
Annika Mascher (AM) was the principal investigator, wrote the study protocol, coordinated the study, and wrote the first draft of the paper. Bettina Berger (BB) was the main supervisor in methodological issues. Conception and design: AM, BB, Stephan Baumgartner (SB). Collection and assembly of data: AM. Data analysis and interpretation: AM, BB, SB, Florian Pelzer (FP), Hartmut Ramm, Ulrike Weissenstein, Daniel Krüerke, Petra Zibulski, Devika Shah, Viola Schultz, Karolina Königsberger, Andreas Heertsch, Susanne Aeberhard. Study monitoring: FP. Methodological assistance: BB, Lorna Jane Duncan (LJD), SR. Transcription was largely performed by an internal administrator, Susanne Aeberhard, with two transcripts undertaken by an external transcription service (Transcripto.de). Study protocol and paper (advice and editing): BB, LJD, SB, SR, FP, David Dominique Martin (DDM). All authors read and contributed to the editing of the article and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The nonprofit organization Society for Cancer Research is a minority shareholder of Iscador AG, a manufacturer of mistletoe extracts. AM is an employee of the Society for Cancer Research and was employed by Hospital Arlesheim until June 2021. SB is a part-time employee of the Society for Cancer Research and Iscador AG. FP was employed by the Society for Cancer Research until March 2022, and is employed by Iscador AG since then. BB, LJD, DDM have no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by institutional resources of the Society for Cancer Research.
Ethics Approval and Consent to Participate
The study was approved by the Ethical Commission of Northwest and Central Switzerland (EKNZ) and performed in accordance with the Declaration of Helsinki (Project-ID 2020-00905). All patients gave their consent.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.