
Abstract
Introduction
Advances in medical treatments and new technologies as well as increased utilization of screening have increased the life expectancy of people living with cancer1,2; 62% of adults diagnosed with cancer are expected to survive 5 years past their diagnosis dates in the absence of competing causes of death.3,4 The National Cancer Institute defines a cancer survivor as a person living with cancer from the time of diagnosis until the end of life. 5 Cancer survivors live with sequelae of their illness and lingering side effects and consequences of treatment. Many cancer survivors are interested in self-care strategies to improve their health-related quality of life and to reduce the chance for recurrence 2 ; increasingly, they are turning to complementary and alternative medicine (CAM) for solutions.6,7
CAM is defined as a group of diverse medical and health systems, practices, and products that are usually not considered part of conventional medicine. 8 In the general population, CAM use ranges between 9% and 65%, 9 variation that is explainable, in part, by differences in study methodology and CAM definitions employed by investigators. Compared with CAM use by the general population, less is known about its use among oncology patients. In one US study, 91% of patients receiving either chemotherapy or radiotherapy had used some type of CAM since being diagnosed with cancer. 10 In our systematic literature review of colorectal cancer survivors, up to 75% had used some type of CAM 11 ; however, all 4 included studies were cross-sectional and unable to describe patterns of CAM use over time.
CAM use occurs at all stages of the cancer care trajectory. Whereas conventional mainstream approaches to cancer treatment are evidence based (ie, evaluated for safety and effectiveness using rigorous scientific methodologies), much less is known about the safety and effectiveness of CAM.3,12,13 In fact, concerns about CAM use include the following: (a) unknown risks of unproven CAM therapies and practices, (b) interference or interaction with chemotherapy or radiotherapy,14,15 (c) CAM practitioners and products are often not regulated, and (d) their use may increase health care costs (public or private) without necessarily improving patient quality of life or well-being. 16 As such, cancer patients who are using or considering CAM might benefit from discussing with their physicians their decisions and desires to use specific CAM therapies, some of which may interfere with or be harmful when used simultaneously with mainstream cancer treatment. 17 However, there is a lack of patient–physician dialogue about CAM16,18; physicians commonly are unaware of their patient’s use of CAM and patients often remain uninformed about possible helpful therapies. For example, in one survey of oncologists, two thirds reported sufficient comfort discussing CAM with their patients but only 21% reported actually initiating such discussions. 19 Insufficient CAM knowledge may dissuade health care professionals from engaging in detailed CAM discourse. 20
With the goal of initiating a future longitudinal study of CAM use by oncology patients treated in conventional health care settings, the present study aimed to determine the feasibility of recruitment methods for such a project and to assess the adequacy and comprehensiveness of a questionnaire designed to assess CAM. Secondarily, we sought to gather preliminary data about CAM use by site of cancer, reasons for their use and rates of use disclosure to treating physicians, and to better understand CAM use and patient perspectives of CAM discussions that occur or not between cancer patients and their physicians. The present study provides one perspective from Canadian health care consumers who are getting comprehensive cancer care in a secondary community hospital.
Methods
The study was conducted at St. Mary’s Hospital Center (November to December, 2008), a Montreal University–affiliated secondary care urban hospital serving a large multiethnic population. Ethics approval was obtained from the hospital’s Research Ethics Board.
Patients were eligible if they were aged 18 years and older and conversant in English or French. Survey participants were recruited from the oncology outpatient clinic from amongst those waiting to receive care from oncologists and/or nurses. The research assistant (RA) approached a convenience sample of patients in the waiting room prior to their scheduled appointments and asked about their interest in participating in a study designed to assess use of various therapies and treatments that may or may not have been recommended by their doctors. Patients agreeing to take part provided written informed consent; the RA then administered the study questionnaire to gather sociodemographics (age, sex, cultural group, education, marital status, household income), clinical information (self-reported health, comorbidities, cancer site, date of diagnosis, cancer treatment received in the last year), and data on insurance coverage for CAM.
CAM use was assessed using a preliminary version of the International CAM Questionnaire (I-CAM-Q) 21 as the questionnaire had not been finalized or published at the time of the conduct of the study. The I-CAM-Q, a 38-item questionnaire, was developed in an international forum to improve measurement of CAM utilization and to facilitate measurement of CAM according to theoretical concepts (eg, ability to create several user subgroups according to type and number of therapies, main reason for use and degree of helpfulness).
Respondents were prompted to choose from among the listed CAM modalities those that they used in the previous 1 month and within the preceding 12 months, reasons for use of a particular CAM modality (treat/be good to myself, relieve symptoms/side effects of treatment, cure disease, improve quality of life, used the therapy instead of traditional cancer treatment) and to indicate, when CAM was used, if this use was disclosed to their physicians (yes/no). Given the wide range of practices that fall under the designation of CAM, for the purposes of the present study we grouped therapies into three broadly defined categories: natural health products (NHP), CAM practitioners (CP), and mind–body therapies (MBT; Table 1). Each CAM category included several “other” open-ended items in which patients could include in the therapies that did not appear on the list.
Complementary and Alternative Medicine (CAM) Categories and Examples of Therapies Within Each Category

Focus group participants were recruited from family practices within the hospital’s Family Medicine Centre and had been diagnosed with cancer for at least 2 years. Family doctors identified patients who were agreeable to learning more about the focus group. The study RA then contacted those patients and provided a description of the study. Interested patients were convened to a focus group where informed written consent was obtained prior to beginning the discussion. The focus group leader and one member of the research team (MJS) prepared an interview guide.
The focus group discussion was audiotape recorded and transcribed verbatim using standard rules of transcription and analyzed using the constant comparative approach. 22 We used a constant comparative thematic content analysis to guide the data analysis. The focus group facilitator and one member of the research team (MJS) independently read the transcript and identified recurrent themes and subthemes. Additional codes for newly emerging topics were created as needed. Consensus was used for the development of major themes and patterns, the reduction of data into these categories and the identification of exemplar quotations illustrating each theme.
Statistical Analyses
Descriptive statistics were used to characterize the study population. χ2 and Fisher’s exact (for analyses where the cell size was less than 6) tests were used to determine differences on selected variables between CAM categories and cancer sites. Feasibility was assessed by response rate and rates of CAM use by category. The response rate was calculated as the number of participants divided by the total number of patients approached to participate. Rates of CAM use were calculated as the number of patients who separately answered yes to use in the previous month and during the previous 12 months, divided by the total number of patients who completed the survey. Disclosure of CAM use to the physician was computed as the proportion of users per CAM category who disclosed use. Reasons for CAM use were reported according to the proportions of users per CAM category who endorsed the particular reason for use.
Results
Of 103 patients approached for participation, 100 (97.1%) consented. Table 2 presents the demographic and clinical characteristics of these participants. Mean age was 61.8 years (SD = 12.6), 77% were female, and 87% were white. Primary cancer sites were breast (41%), colorectal (29%), and 11 other cancer types accounted for the remaining 30%. In the previous 12 months, 91% of patients had received chemotherapy, 52% had undergone surgery, and 33% had received radiotherapy. Health status of participants was reported as excellent for almost half (48%), 41% indicated very good/good health, while 11% reported fair/poor health status. Insurance coverage for CAM was 37%.
Characteristics of Cancer Patients (N = 100) a
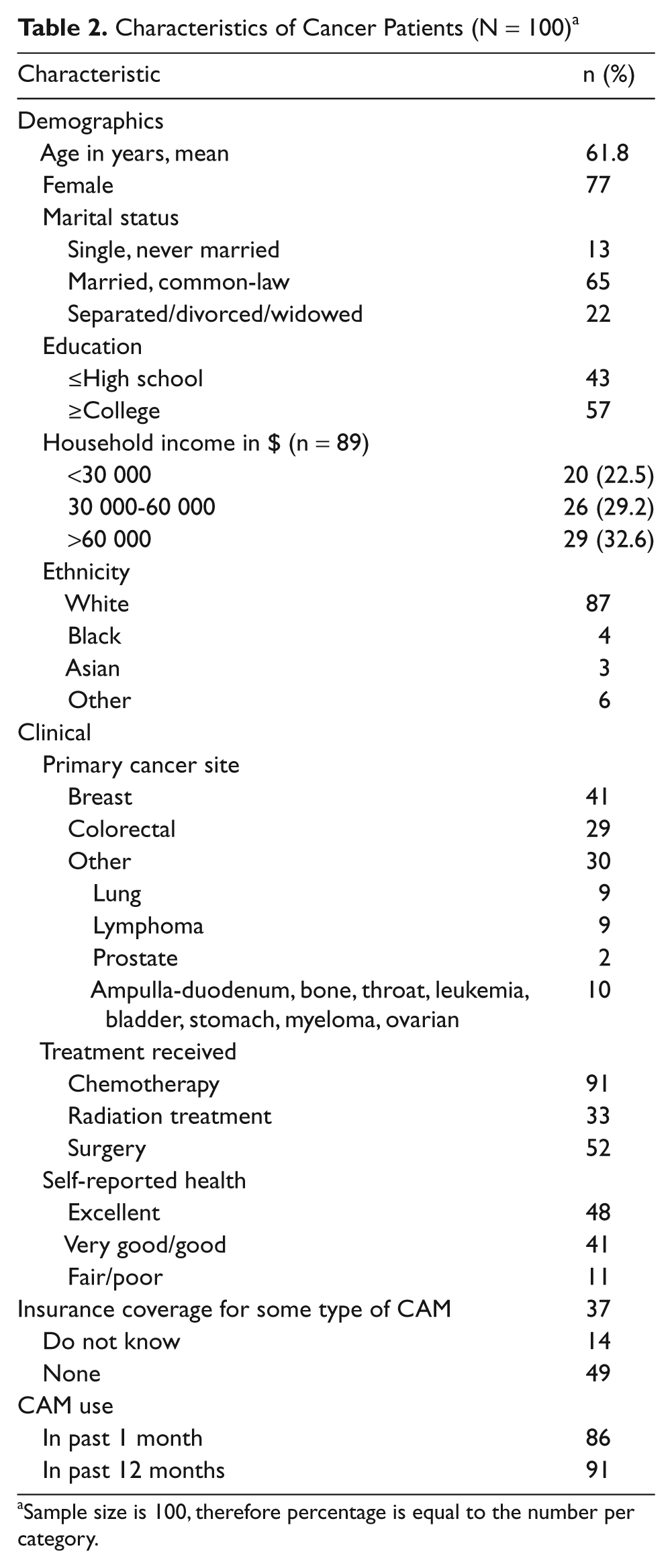
Sample size is 100, therefore percentage is equal to the number per category.
Table 3 presents CAM use overall and according to primary cancer site. In total, 86% and 91% of respondents reported using at least one form of CAM in the previous 1 and 12 months, respectively. NHP was the most commonly used CAM, followed by MBT and CP. Overall CAM use was less in the previous month compared with previous 12 months. In the past month, 37 (90.2%) breast cancer, 25 (86.2%) colorectal cancer, and 24 (80%) other cancer patients had used at least one type of CAM. In the past 12 months, more patients with breast cancer followed by colorectal cancer and other cancers used some type of CAM (95.1%, 89.7%, and 86.7%, respectively). NHPs were used by significantly more patients with breast compared with colorectal and other cancers in the past 1 and 12 months (P = .0108 and P = .0490, respectively). CP users were significantly younger compared with CP nonusers (52.9 vs 62.9 years, P = .0126). Overall, 20% of patients reported using prayer in the past 1 month.
Complementary and Alternative Medicine (CAM) Therapy Use by Cancer Site in Past 1 and 12 Months (N = 100)

Multiple CAM use was reported by 57% and 81.3% respondents in the past 1 and 12 months, respectively. The most common combination was NHP and MBT, which was used by 44.2% and 39.6% of multiple CAM users in the past 1 and 12 months, respectively (data not shown).
Table 4 shows the reasons for CAM use and disclosure of such use to doctors. Nearly all used CAM to improve quality of life (98.8%, 100%, and 98.5% of NHP, CP, and MBT users, respectively). A large proportion of MBT users (46.2%) also reported “treat/be good to myself.” In contrast, considerably fewer patients used CAM to relieve cancer-related symptoms, reduce treatment side effects or cure cancer; only 2% of respondents used CAM in place of traditional medicine. In total, 68.5% of all CAM users disclosed such use to their physicians. 68.3% disclosed NHP use, 51.7% disclosed CP use, and 32.3% disclosed MBT use.
Reason for and Disclosure of Use to Physician of NHP, CP, and MBT

Abbreviations: NHP, natural health products; CP, complementary and alternative medicine practitioner; MBT, mind–body therapy.
The focus group consisted of 5 patients (2 women, 3 men), 4 of whom reported using CAM. Therapies that were used included NHPs (ginger, green tea, bell prostate tea, herbal tea, valerian), dietary change (exclusion of red meat), acupuncture, meditation, prayer, Tai-chi, and osteopathy. Not all CAM use was for cancer. Three patients felt that CAM discussions with their physicians were strained when they occurred. One patient reported that her physician used verbal and nonverbal cues to express negativity regarding her questions about CAM, saying “nothing’s been proven” or “my physician doesn’t say anything negative but she gets that look on her face.” Another patient felt that it was insulting to physicians to ask about CAM, “that’s sort of like giving your doctor a knock, isn’t it. You’re not curing me right, so I’m going to find something else.” One patient felt his questions about CAM were ignored
I’ve asked my doctor about my friend who is on a particular CAM and gets great relief from it. I don’t get a no and I don’t get a yes. The doctor just slides right over it . . . and now this is your prescription!
One patient received a physician referral to a CAM practitioner for pain. Although patients wanted to discuss CAM with their physicians, they feared a backlash. “If you can’t ask your doctor, who can you ask?” “At this stage of the game, I’m not questioning him.” One patient wanted the physician to ask if there were any questions (about CAM) at the end of the visit to which another patient responded, “but he’s only got 5 seconds left!” Patients thought that an information session held by a physician who also practices CAM would be worth attending: “Someone who’s equal between the two.”
Discussion
In this study of oncology patients, feasibility for undertaking a future longitudinal study of CAM use at our institution was demonstrated by the very high rates of response and CAM use. Since nearly all patients used CAM, a comparison of CAM users and nonusers would not be feasible. With more than 75% of our study sample being female and Caucasian, a recruitment strategy stratified by gender and ethnicity would ensure adequate representation of males and non-whites. We also would revise the study questionnaire to learn more about patterns of use since other researchers found that only 15% of breast cancer patients completely adhere to CAM treatment. 23 Thus, we would include items such as the approximate dates of CAM initiation and termination, whether CAM use began prior to or since the cancer diagnosis and include prayer as a unique category as the lack of same may help to explain the low utilization rate found in our survey compared to others, who reported use up to 77%. 10
Only 8% of survey respondents had not used CAM at all in the previous 12 months. This finding may reflect the growing acceptance of CAM or the multicultural population treated at St. Mary’s Hospital Centre. Although utilization rates exceed some prior findings24-26 they mirror those found among newly diagnosed cancer patients receiving traditional cancer treatment. 10 The lower use of CPs may stem from its high cost. 23 The high rate of disclosure of CAM use to physicians is consistent with increased acceptability of CAM by society and by some mainstream health care professionals. 27 The majority of NHP and CP users discussed use with their physicians, but only one third of MBT users disclosed use, similar to findings by others, 25 perhaps because MBT is not considered CAM. Almost all CAM users sought to improve their quality of life, a finding that was seen by others but was not as prevalent.9,23,25 In contrast to previous studies,25,26 few users wanted to treat the symptoms, side effects, or cancer itself.
Communication is important to the delivery of high-quality patient care, a value now reflected in the teaching and assessment of communication skills as one of the foundational elements of medical professionalism.28-30 Within the context of the doctor–patient relationship, patient-centered communication is essential to establishing trust and positively affects patient satisfaction, decision making and adherence to medication.31,32 Yet although cancer patients’ disclosure of CAM use to their physicians is increasing, our focus group findings suggest that informative CAM discussions with family physicians are not occurring. Some of the patients who broached the topic of CAM with their family physicians were met with resistance and skepticism; patients expressed exasperation with having to access information themselves from unreliable sources such as the internet without the accompanying discussion from a trusted health professional to make informed choices. 28 Whether concern is with the lack of scientific data supporting the safety and efficacy of many CAMs, the possibility for legal repercussions or the fear that their CAM discussions may be interpreted as moral support for CAM,33,34 physicians need to be aware that the overwhelming majority of oncology patients use CAM to self-manage and improve quality of life and that patients want them to engage in effective communication that empowers them to make informed and valued decisions. 29
Limitations
Several study limitations are acknowledged. Inconsistent definitions of CAM throughout the literature preclude comparison of results among studies.23,26,35,36 Selection bias may have been introduced in the survey as recruitment occurred in the oncology outpatient clinic of one institution during November and December and participants may not be representative of all patients registered at the clinic. In the future longitudinal study, we plan to obtain the complete list of patients registered in all participating clinics and then randomly select patients to participate. Present findings may have limited generalizability because of the small sample size, the limited number of males and non-whites, and the inclusion of only one institution. We were not able to distinguish NHPs that were chosen by the patients from those prescribed by CPs, partial from full coverage for CAM, or different types of prayer. Women may have been overrepresented because breast cancer is one of the identified areas of focus for our oncology department.
Conclusions
In conclusion, this study provides evidence to initiate a large-scale longitudinal study with modifications to particular aspects of study methodology. First, recruitment methods were acceptable to patients but a sampling strategy stratified by sex and ethnicity will ensure that subgroups of interest are represented. Second, nearly all patients used at least one CAM and the future study may have sufficient numbers to explore use of a particular therapy or combination of therapies. Third, nearly all CAM users sought to improve quality of life and the future study could explore relationships between type of CAM and components of quality of life. Finally, the CAM use questionnaire will require modifications such as adding items that pertain to the timing of CAM initiation, termination, and beginning prior or subsequent to the cancer diagnosis, as well as including a specific item on use of prayer. Further insight on CAM use and discussions was gleaned from the focus group. Most patients consumed herbal teas and made dietary changes following the cancer diagnosis. Experience with CAM discussions varied from receiving a CAM referral to being ignored or dismissed when a question about CAM was posed, suggesting the increased disclosure of CAM use is not promoting interactive and informative exchange of CAM information. These findings have implications for the future study, which will aim not only to measure CAM use in the same individuals at several time points over a 1-year period but also to examine the facilitating and inhibiting factors related to CAM use when care is provided by more than one health care professional within the same institution and to assess reliability of the CAM use questionnaire. Given the growing number of cancer survivors who want to engage in self-care, communication that includes adequate CAM information exchange may not only respond to patients’ emotional needs but also improve the therapeutic relationship between patients and their treating physicians.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The authors disclosed receipt of the following financial support for the research and/or authorship of this article:
This research was supported by a grant from the St. Mary’s Hospital Center Foundation. Dr Sewitch is supported as a research scientist of the Canadian Cancer Society through an award from the National Cancer Institute of Canada.