
Abstract
Despite the high prevalence of emotional disorders (EDs), access to appropriate treatment remains limited due to factors such as cost, lack of human resources, and geographical barriers. To overcome these barriers, it is crucial to implement effective evidence-based therapies in more cost-effective therapeutic formats. The Unified Protocol (UP) was developed for treating comorbid EDs by specifically targeting shared transdiagnostic mechanisms. It can be applied in different therapeutic formats, and combining the group and online formats could enhance the dissemination and accessibility of the UP. This case study describes the application of a 12-week UP intervention via online videoconference to a group of eight adults diagnosed with comorbid anxiety and depressive disorders. The participants were assessed pretreatment, posttreatment, and at a 3-month follow-up. The Reliable Change Index (RCI) was used to assess the clinical significance of treatment outcomes. Five participants completed the intervention and showed a clinically significant decrease in depressive symptom severity, whereas four presented a significant reduction in anxiety symptoms. Significant improvements in emotional regulation and behavioral activation were observed in five participants. Four participants also demonstrated improvements in mindfulness and quality of life. Therapeutic gains were generally maintained or improved at the 3-month follow-up, except in one participant. High levels of participant satisfaction were reported regarding both the intervention program and its delivery format. This case study highlights the acceptability, feasibility and clinical utility of online group UP for treating adults with comorbid EDs, suggesting promising potential for this intervention format.
Theoretical and Research Basis for Treatment
Emotional disorders (EDs) constitute the most prevalent cluster of mental disorders worldwide (World Health Organization, 2022) and include anxiety, depression and other related disorders. While emotional experiences such as anxiety are common in daily life, emotional disorders refer to diagnosable conditions that cause significant distress and impairment in daily functioning (Bullis et al., 2019). EDs are characterized by high levels of neuroticism (i.e., the tendency to experience intense and frequent negative emotions), aversive reactions to emotional experiences (e.g., evaluating them as uncontrollable or inadequate), and engagement in emotion-avoidant strategies (e.g., behavioral or cognitive avoidance). These shared temperamental and psychological mechanisms are factors related to the high rates of comorbid EDs (Bullis et al., 2019). Comorbidity has been associated with increased severity of EDs and greater interference in daily functioning (Antunes et al., 2018), as well as increased economic costs (Organization for Economic Cooperation and Development [OECD], 2018) and difficulty accessing adequate treatment (Knapp & Wong, 2020).
Research on diverse transdiagnostic cognitive‒behavioral treatments (T-CBTs) has recently increased (Schaeuffele et al., 2021). Under the umbrella of T-CBT, unified approaches have been developed to treat people with multiple mental disorders using the same protocol by specifically targeting shared transdiagnostic mechanisms (Bullis et al., 2019; Schaeuffele et al., 2021). Compared with single-disorder protocols, unified T-CBTs offer several advantages, as they appear to be a more cost-effective and accessible solution for patients and health care services (Peris-Baquero et al., 2023; Schaeuffele et al., 2024).
Unified Protocol for Transdiagnostic Treatment of Comorbid Emotional Disorders
The Unified Protocol (UP; Barlow et al., 2018a) is a unified transdiagnostic CBT intervention that is manualized, encompassing a therapist manual (Barlow et al., 2018a) and a workbook (Barlow et al., 2018b). There is strong empirical evidence of the effectiveness of UP in reducing anxious and depressive symptoms (Carlucci et al., 2021), improving negative and positive affects (e.g., Osma et al., 2015), and increasing the durability of therapeutic gains (e.g., Osma et al., 2022). In addition to being applied to heterogeneous populations (Carlucci et al., 2021), the UP can be adapted to different therapeutic formats, such as individual, group and internet-based formats (Schaeuffele et al., 2024), and has already proven efficacy in face-to-face settings, both individually (e.g., Barlow et al., 2017) and in group format (Ayuso-Bartol et al., 2024). With respect to online settings, there is strong empirical evidence that synchronous online CBT is as effective as face-to-face CBT (Lin et al., 2022), including when it is delivered in group formats (e.g., Ryan et al., 2023). In the particular context of the UP, while several studies have demonstrated its effectiveness through web-based programs (Schaeuffele et al., 2024), empirical research on its feasibility and effectiveness when delivered specifically in a synchronous online group format remains scarce (Celleri et al., 2022). Given the UP’s emphasis on emotion-focused and experiential techniques, it may be important to examine how these strategies are implemented in videoconference-based group settings, as their application may differ from other therapeutic formats. To date, the application of the UP in a synchronous online group format has been studied only in Argentina (Celleri et al., 2022) and Spain (e.g., Martínez-Borba et al., 2022). Celleri et al. (2022) conducted a pilot study with seven adults diagnosed with EDs who completed 11 weekly group sessions delivered via videoconference. The results indicated significant reductions in depressive symptoms, hopelessness, emotional dysregulation, and negative affect, along with improvements in quality of life. Martínez-Borba et al. (2022) implemented a brief preventive version of the UP (six sessions) with five women undergoing fertility treatment. The intervention was delivered in a hybrid format, with two sessions conducted face-to-face and four delivered via videoconference. These studies emphasize the need for further research in clinical populations receiving the standard version of the UP delivered in a fully synchronous online group format.
In Portugal, access to evidence-based psychological interventions is limited, with the main challenges being the geographical location of people in rural and isolated areas, the unequal distribution of therapists and mental health services, and patients’ barriers to continuing treatment (e.g., treatment costs and time constraints to attend appointments; Entidade, 2023). Therefore, adapting and implementing the UP in a synchronous online group becomes an even more accessible and cost-effective solution than other therapeutic formats, as it allow more people to participate in therapeutic sessions without the need to travel (Celleri et al., 2022; Curreri et al., 2023). Recent evidence has shown that the Portuguese general population seems receptive to receiving psychological treatment online (Pedro et al., 2024).
To our knowledge, this is the first case study worldwide describing the application of the UP in a synchronous online group format with individuals who have comorbid anxiety and depressive disorders. In addition to detailing the session-by-session application of the UP and the adaptations made to adjust the intervention to a combined group and online format, in the present study, we presented the main clinical results regarding changes in anxiety and depressive symptoms, transdiagnostic mechanisms (e.g., emotion regulation, mindfulness), and quality of life posttreatment and at 3-month follow-up, as well as patient satisfaction with the intervention.
Case Introduction
Participants’ Sociodemographic and Clinical Information.
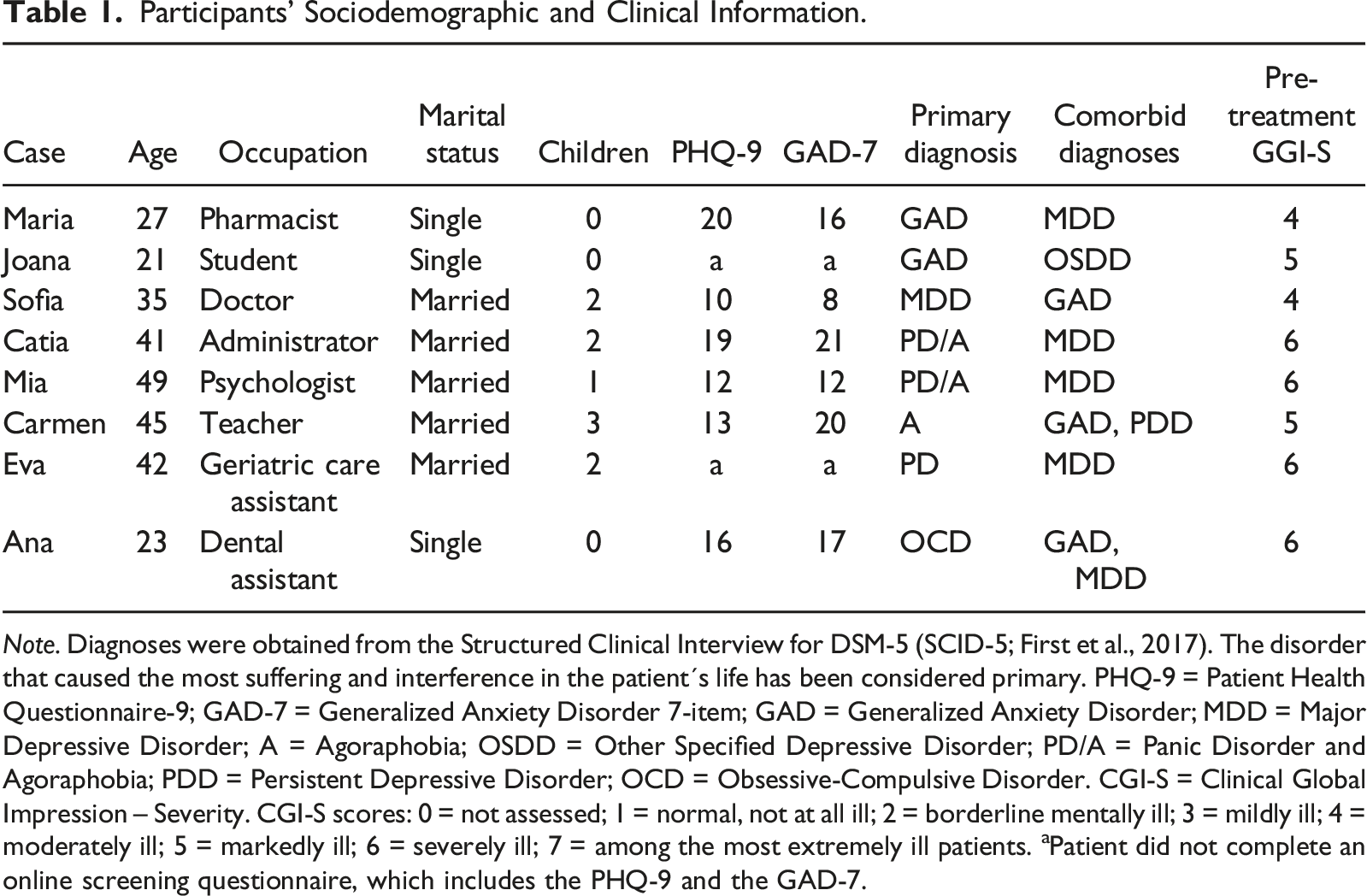
Note. Diagnoses were obtained from the Structured Clinical Interview for DSM-5 (SCID-5; First et al., 2017). The disorder that caused the most suffering and interference in the patient´s life has been considered primary. PHQ-9 = Patient Health Questionnaire-9; GAD-7 = Generalized Anxiety Disorder 7-item; GAD = Generalized Anxiety Disorder; MDD = Major Depressive Disorder; A = Agoraphobia; OSDD = Other Specified Depressive Disorder; PD/A = Panic Disorder and Agoraphobia; PDD = Persistent Depressive Disorder; OCD = Obsessive-Compulsive Disorder. CGI-S = Clinical Global Impression – Severity. CGI-S scores: 0 = not assessed; 1 = normal, not at all ill; 2 = borderline mentally ill; 3 = mildly ill; 4 = moderately ill; 5 = markedly ill; 6 = severely ill; 7 = among the most extremely ill patients. aPatient did not complete an online screening questionnaire, which includes the PHQ-9 and the GAD-7.
Presenting Complaints
Most participants had primary diagnoses related to anxiety symptoms, with only Sofia having a primary diagnosis of major depressive disorder (see details in Table 1).
Maria, Joana, Sofia, and Ana reported intense and persistent anxiety in various aspects of their daily lives (e.g., work, family, daily routines, and unpredictable events). They all mentioned experiencing excessive worrying, irritability, sleep problems, fatigue, muscle tension, concentration difficulties, and procrastination.
Catia, Mia, and Carmen felt intense fear in situations or places in which something could happen that would make them feel ashamed or in situations in which they had no means of escaping or receiving help if they had a panic attack. As a result, they engaged in various avoidance behaviors. Catia avoided leaving the house alone as well as using public transport and driving on busy roads. Mia avoided crossing bridges, driving alone on “long highways with few exits,” and staying in places difficult to escape (or, in such cases, tried to remain near a door or bathroom). She also recognized that her anxiety symptoms led her to refuse job offers. Carmen avoided cinemas and crowded places. Additionally, all three participants reported that it was challenging to shop in supermarkets or shopping centers. While Carmen noted that she had never experienced unexpected panic attacks, both Catia and Mia had experienced several such attacks and remained fearful of their recurrence. Eva also experienced recurrent panic attacks and felt very anxious about having another, although she did not have agoraphobic fears. Owing to her symptoms, she was unable to work for one month.
Ana, in particular, experienced intense stress when objects were not orderly or positioned in a certain way. She also reported unwanted thoughts, such as “Something bad could happen” or “If you don’t do this, something will go wrong.” Ana also mentioned spending much of her time engaging in compulsive behaviors (e.g., only going to bed after ensuring that all the rooms in the house were tidy or aligning the laces of her sneakers before entering the house) to reduce her anxiety and prevent bad outcomes.
Maria, Sofia, Mia, Carmen, Eva and Ana also experienced a persistent depressed mood, lack of interest in pleasurable activities (e.g., [Mia] “I just want to sit on the sofa and do nothing”), feelings of guilt and worthlessness, low energy, poor appetite, changes in sleep patterns, irritability, difficulty concentrating or making decisions, and low self-esteem (e.g., [Sofia] “I can’t identify anything good about myself”).
The anxiety and depressive symptoms experienced by the participants caused significant distress and had a major impact on their daily functioning and general life (e.g., their professional, family, and social lives). At the time of the study, Joana, Sofia, Mia, and Eva were on stabilized doses of psychiatric medication for at least three months, as required by the inclusion criteria, and were instructed to maintain the dosage throughout the treatment. Catia was only taking an anxiolytic as needed. None of the participants presented with current suicidal ideation or substance abuse.
History
All the participants had received a prior diagnosis of an emotional disorder, reported persistent anxiety symptoms over time, and had previous experience with individual face-to-face psychotherapy. Five participants had received CBT, but all met the inclusion criterion of having completed fewer than eight sessions in the past five years, and none had received transdiagnostic treatment. Most reported a family history of diagnosed psychopathology. The onset of psychological symptoms occurred predominantly during adolescence or early adulthood, between the ages of 14 and 19. Maria, Joana, Sofia, Cátia, and Eva reported at least one depressive episode, with Sofia and Eva experiencing three distinct episodes across adulthood. Cátia, Mia, and Eva reported previous experiences of panic attacks. Carmen described lifelong difficulties with emotional regulation, whereas Ana reported obsessive–compulsive symptoms beginning at age 16. Adverse developmental experiences, including childhood domestic violence (Joana), academic stress (Maria, Joana, Ana), parental abuse, bullying, divorce (Sofia, Carmen), and perinatal challenges (Sofia, Eva), were common. Mia was also diagnosed with irritable bowel syndrome at age 47, which exacerbated her anxiety. Maria, Joana, Sofia, and Eva had received psychiatric care.
Assessment
Most participants became aware of the intervention program through online advertisements on social media. They completed an online screening questionnaire that included questions to assess sociodemographic and clinical data, as well as the Patient Health Questionnaire-9 (PHQ-9; Ferreira et al., 2018) and Generalized Anxiety Disorder-7 (GAD-7; Sousa et al., 2015) to assess the severity of clinically significant depressive and anxiety symptoms, respectively (see Table 1). PHQ-9 scores higher than 9 and GAD-7 scores equal to or greater than 8 were used as cutoff points to indicate clinically significant depressive and anxiety symptoms, respectively. Two participants (Eva and Joana) were referred by the Tondela-Viseu mental health service.
Before treatment, all participants provided informed consent and were assessed by a clinical psychologist through a synchronous online interview, using the Structured Clinical Interview for DSM-5 (First et al., 2017; see Table 1) and Clinical Global Impression–Severity (CGI-S; Guy, 1976; see Table 1) to confirm ED diagnoses.
Outcome Scores and Reliable Change Index (RCI) at Pretreatment, Posttreatment, and 3-Month Follow-Up.
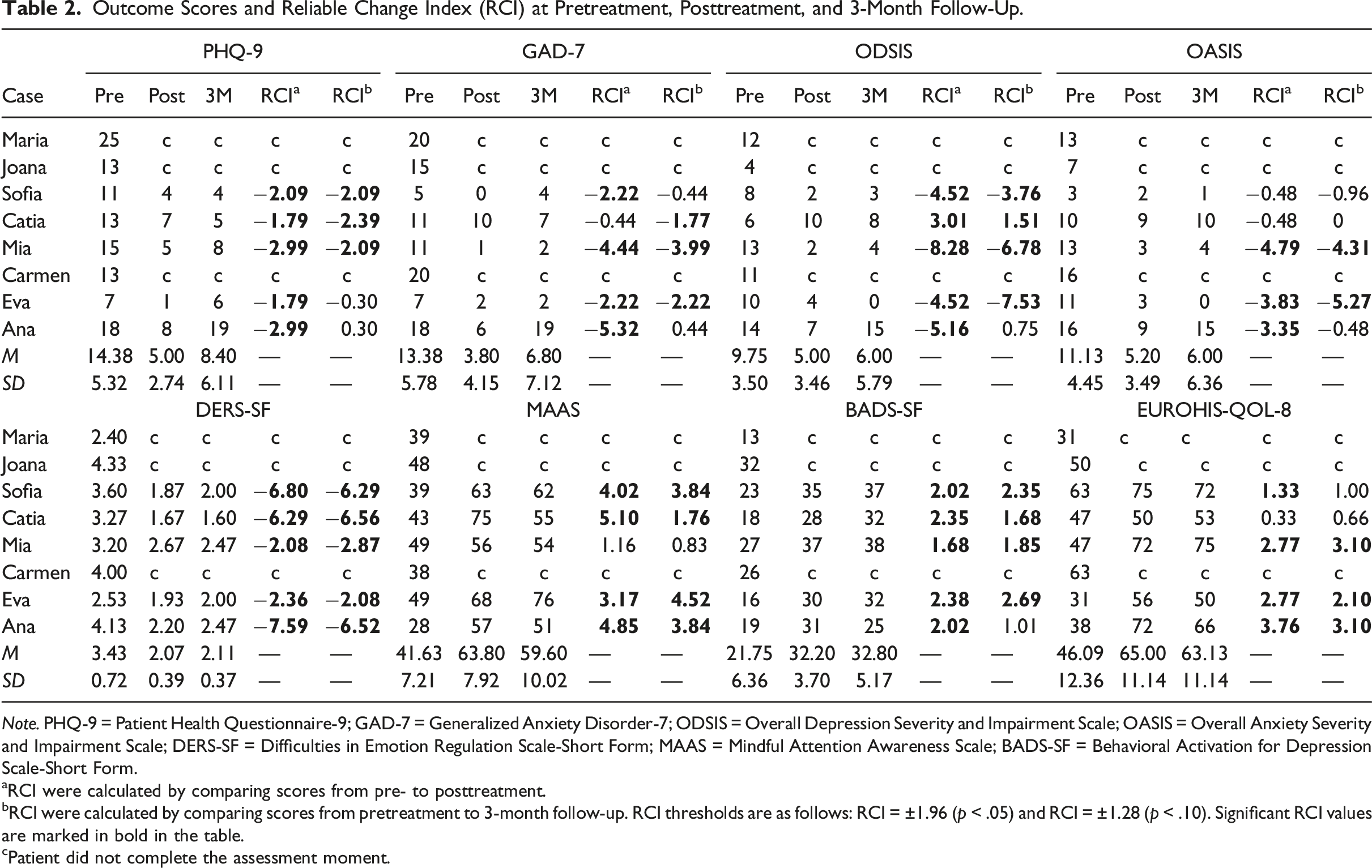
Note. PHQ-9 = Patient Health Questionnaire-9; GAD-7 = Generalized Anxiety Disorder-7; ODSIS = Overall Depression Severity and Impairment Scale; OASIS = Overall Anxiety Severity and Impairment Scale; DERS-SF = Difficulties in Emotion Regulation Scale-Short Form; MAAS = Mindful Attention Awareness Scale; BADS-SF = Behavioral Activation for Depression Scale-Short Form.
aRCI were calculated by comparing scores from pre- to posttreatment.
bRCI were calculated by comparing scores from pretreatment to 3-month follow-up. RCI thresholds are as follows: RCI = ±1.96 (p < .05) and RCI = ±1.28 (p < .10). Significant RCI values are marked in bold in the table.
cPatient did not complete the assessment moment.
Posttreatment, therapists assigned both CGI-S and Clinical Global Impression–Improvement (CGI-I; Guy, 1976) ratings. The participants also completed the same research protocol at baseline and two additional self-report measures to assess their satisfaction with the UP. The Satisfaction with Treatment Questionnaire (STQ; Larsen et al., 1979), adapted by our research team, was used to evaluate satisfaction across various factors, including perceived quality, usefulness of learned techniques, and discomfort experienced. Additionally, we included the following questions: “Is there any other content you think would be interesting to include in the program? If so, what? Do you think there is any content in the program that does not need to be covered? If so, what? Which program contents did you find most useful? Do you think the program duration was sufficient? What is your opinion of the group format used to implement the program?”. To further assess the usefulness of the UP and its specific components, participants completed the Questionnaire for the Evaluation of UP Components (Osma et al., 2015), which comprises nine items rated on an 11-point scale ranging from 0 (not at all) to 10 (very much). Finally, indicators such as the number of sessions received and homework assignments completed were used to assess patients’ compliance and adherence to treatment.
Case Conceptualization
Consistent with the case conceptualization of the UP (Barlow et al., 2018a), the patients’ difficulties were evaluated through the ED functional model (Bullis et al., 2019), which is framed within the transdiagnostic ED framework. This model emphasizes the experience of strong and frequent negative emotions, aversive reactions to these emotional experiences, and efforts to avoid or escape them.
At the initial assessment, all patients reported experiencing intense and frequent negative emotions, such as anxiety, sadness, anger, frustration, and guilt. Next, they manifested aversive reactions to overall emotional experiences or to one part of their experience (e.g., physical sensations or thoughts). For example, Maria said, “I can’t stop feeling so anxious”; Joana and Carmen said, “I feel that I can’t control my emotions”; Sofia noted, “I’m always so overwhelmed”; Catia and Eva perceived their physical sensations as dangerous (e.g., “I’m going to have a panic attack”); Mia judged her emotional experiences as uncontrollable and unpredictable; and Ana mentioned several times, “I’m ridiculous (feeling this way)!”. Finally, all patients engaged in efforts to avoid or suppress their unpleasant emotions through avoidance behaviors that included the following: (a) emotion-driven behaviors (e.g., leaving a place when feeling anxious; checking behaviors); (b) overt situational avoidance (e.g., avoiding shopping centers, highways, and enclosed spaces; refusing invitations); (c) subtle behavioral avoidance (e.g., procrastination; excessive planning); (d) cognitive avoidance (e.g., worry/rumination; listening to music for distraction); and safety signals (e.g., traveling by car only when accompanied; carrying medication). Although these behaviors may result in short-term relief, they paradoxically prolong patients’ experience of intense emotions over the long term, increase their suffering, reinforce their maladaptive beliefs, and limit their functioning in different life contexts.
Therefore, the application of the UP in group therapy (Bullis et al., 2015; Osma et al., 2015), which focuses on the common mechanisms of EDs, seemed to be the appropriate treatment plan for this group of patients, since the UP helps patients understand and tolerate their intense emotions while developing new coping strategies (e.g., mindful awareness; cognitive flexibility) to respond to them more adaptatively (Barlow et al., 2018a).
Course of Treatment and Assessment of Progress
Therapist
Two clinicians (therapist and cotherapist), both of whom hold master’s degrees in clinical psychology, implemented the treatment. They were previously trained in the UP and supervised by a UP-certified expert. During the intervention, the therapists followed the Portuguese version of the therapist manual (Barlow et al., 2018/2023).
Course of Treatment
Summary of the Contents of Each of the Treatment Sessions.
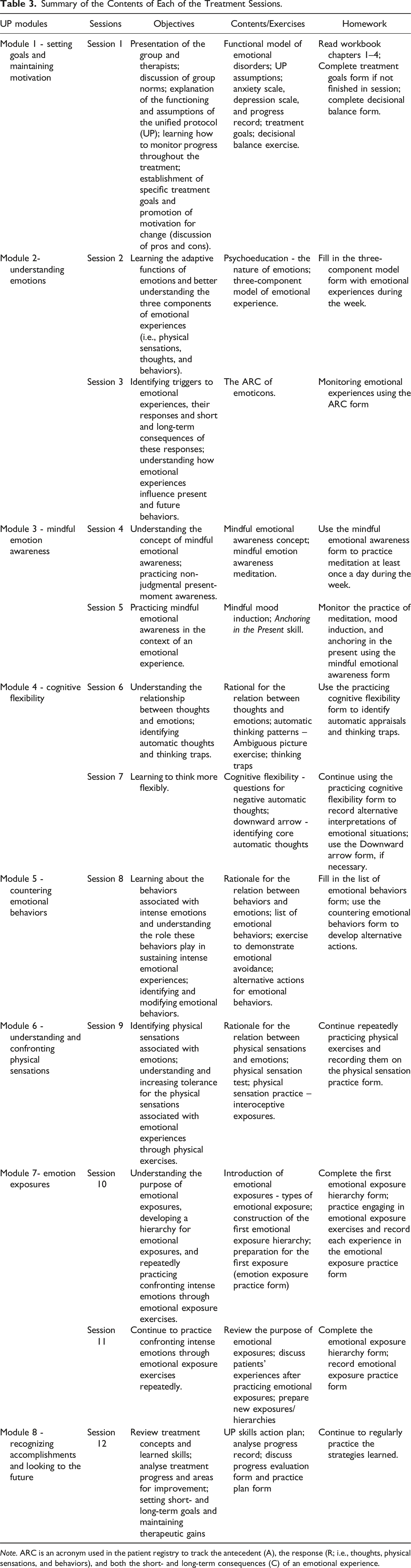
Note. ARC is an acronym used in the patient registry to track the antecedent (A), the response (R; i.e., thoughts, physical sensations, and behaviors), and both the short- and long-term consequences (C) of an emotional experience.
Following the structure recommended by Bullis et al. (2015), each session, with the exception of the first one, was divided into two parts: (1) a review of the prior session and homework and (2) a presentation of new content, in-session exercises, conclusions, and new homework assignments. Moreover, the aims and contents of each of the eight modules (see Table 3) were determined according to the distribution outline in Pastor et al. (2019), as described below.
Module 1 - Setting Goals and Maintaining Motivation (Session 1)
The session began with introductions of the therapists and group members. Since it was each patient’s first group intervention, the patients felt somewhat uncomfortable. Then, group norms (e.g., confidentiality, participation) and the session schedule were discussed. The first hour focused on psychoeducation on ED characteristics, key UP components, session structure, and the therapeutic format. All patients were receptive to sharing personal examples of their emotional experiences, finding common aspects among themselves (e.g., [Carmen] “It is curious to see that I am not the only one who feels this way”). In the second part of the session, the importance of motivation for treatment outcomes was discussed, and goals were established. Each participant was asked to identify two problematic areas and two specific and realistic goals for each area as well as to define small steps for attaining each goal. For example, one of the top problems identified by Sofia was becoming easily irritated with her husband, so the goal she defined was “being able to delegate tasks to my husband calmly.” Similarly, Mia quickly identified her main problems (e.g., “not being able to drive on long highways”) and goals (e.g., “going to the beach alone”). She readily offered to help Catia, as they shared similar difficulties. In contrast, Eva struggled to identify her goals during the session. The decisional balance exercise was discussed together, identifying the common pros and cons of a change. After the homework was explained (see Table 3), the therapists provided positive reinforcement for this first session. Maria and Joana missed the session, and Joana informed us that, owing to scheduling conflicts, she would have to drop out of treatment.
Module 2 - Understanding Emotions (Sessions 2–3)
At the beginning of session 2, the therapists reviewed the content of the previous session, paying special attention to analyzing patients’ Treatment Goals Forms. Catia and Eva expressed difficulty in concretizing their goals, so the therapists reinforced the relevance of defining specific and tangible goals over general goals (e.g., “being able to control my emotions in various situations” was defined as “being able to travel by bus with less discomfort”). To help patients commit to completing their homework, it was also important to discuss barriers to finishing the task and possible ways of overcoming them. The focus of the second part of this session was providing psychoeducation about the functional role of emotions and identifying the three components of emotions (i.e., thoughts, physical sensations, and behaviors). All the participants recognized a lack of awareness regarding their emotional experiences. During the presentation of the Three-Component Model UP Form, Mia shared a personal example: (a) situation: “going to a supermarket”; (b) emotions: “anxiety, fear”; (c) thoughts: “I will not be able to stay as long as needed”; (d) physical sensations: “rapid breathing, sweating, and stomachache”; and (e) behavior: “shopping online”. Maria, Carmen and Ana missed this session. Later, Carmen informed the therapists that she was not available to continue treatment because she had to care for a family member with a chronic illness. Owing to the importance of reviewing Ana’s goals, an individual session was scheduled with her.
In session 3, the participants learned, via the ARC Form, to identify what happens when they feel an emotion. Sofia, Catia, Mia and Ana, who completed the homework, were able to identify the components of their emotional experiences. Sofia and Mia appreciated these forms, as they helped them better understand their emotions and recognize when they were or were not justified by the situation. Catia acknowledged that during intense emotional experiences, she often had self-critical thoughts that further intensified her emotions. During Mia’s participation, Catia validated her emotions and recognized common experiences (“I feel the same”). Eva missed this session.
Module 3 - Mindful Emotion Awareness (Sessions 4–5)
At the beginning of session 4, when reviewing the homework (see Table 3), the patients recognized that they often judged their emotional experiences (or parts of them) as bad, uncontrollable, or inadequate and consequently judged themselves for feeling this way. Additionally, they often engaged in reviewing past situations or making future predictions (e.g., “What if I go and feel bad?”). In this context, therapists introduced the concept of mindfulness and conducted guided meditation, allowing patients to practice this skill in a neutral emotional state. Sofia and Mia had meditation experience, but they did not practice it regularly. To facilitate practicing mindfulness in everyday life, the therapists proposed simple mindfulness exercises with routine activities (e.g., paying attention to smells and sensations during a bath). Only Sofia and Mia attended this session. Both mentioned that they had already made therapeutic progress (e.g., Mia could drive without taking an anxiolytic) and were very satisfied with the first UP modules. For professional reasons, Maria could not attend the sessions and subsequently dropped out.
In session 5, the patients learned that they were able to feel strong emotions without avoiding them. Sofia and Catia considered it difficult to use breathing as an anchor, and recommendations were made for them to use other cues as anchors (e.g., the sensation of the feet on the ground). Eva revealed having difficulty practicing meditation during the previous week due to a lack of time. However, she tried to practice mindfulness by anchoring herself in the present while drinking coffee. The group congratulated Catia for sharing that, over the past weekend, she had managed to visit her aunt by following a new route and without taking medication.
Module 4 - Cognitive Flexibility (Sessions 6–7)
Session 6 began with a discussion on the link between thoughts and emotions. Next, the therapists shared an ambiguous picture from the UP Workbook (via screenshare), which prompted the patients to share automatic interpretations. All patients initially provided negative interpretations (e.g., “the daughter/wife died”). When asked for other explanations, they suggested other possibilities (e.g., [Sofia]: “She might have had a baby”; [Catia]: “They are celebrating finding a transplant donor”; [Eva]: “They might not be related to the ill person”). The patients recognized their tendency to jump to conclusions or to think the worst in personal situations.
In session 7, the therapists explained the concept of cognitive flexibility through an illustrative picture that included a list of UP questions that helped generate alternative thoughts. The downward arrow strategy was also explained as a tool to identify core automatic thoughts and alternatives. Sofia, Catia, and Mia identified their core thoughts as “Nobody likes me”, “I am alone in the world”, and “I have no value”, respectively. Ana, who struggled with intrusive thoughts (e.g., “Something terrible will happen to me or my family”), received personalized attention. When asked what these thoughts meant, Ana said, “I am a failure.” Arguments for and against this belief were discussed.
Module 5 - Countering Emotional Behaviors (Session 8)
Sofia, Catia, Mia and Eva recognized emotion-driven or avoidance behaviors that they frequently engaged in to reduce or prevent experiencing certain emotions. Consequently, they were able to develop and engage in alternative actions. For example, Mia said, “Last week, I felt angry with my trainer for not meeting our agreed schedule. I emailed him to express my dissatisfaction and ask for clarification, but speaking directly would have been more effective, even though it would have been uncomfortable”. The therapist used this example to explain why alternative actions tend to cause more discomfort in the short term but reduce emotional intensity and impairment in the long term. At the end of the session, the therapists proposed homework (see Table 3) and encouraged patients to begin exposure to slightly threatening situations that may provoke intense emotions. Ana missed this session.
Module 6 - Understanding and Confronting Physical Sensations (Session 9)
Since Mia, Catia and Eva’s experiences of anxiety were associated with higher levels of somatic symptoms, this module was significant for them. The group members identified physical sensations they often experienced that were associated with intense emotions (e.g., [Mia] “When I’m very anxious, I feel a heaviness in my head”; [Catia] “I feel short of breath”; and [Sofia] “I feel frequent muscle tension”. Once again, Catia and Mia reacted aversively to their physical sensations, saying, “Physical sensations are a complicated part.” After a demonstration by the therapists, the patients performed symptom-inducing exercises (e.g., hyperventilation) in the session and completed the Physical Sensation Test Form. For example, Mia rated breathing and spinning exercises with high levels of discomfort (breathing: 7 of 10; spinning: 8 of 10) and noted their similarity to the symptoms she typically experienced (breathing: 8 of 10; spinning: 9 of 10). Eva and Ana missed the session.
Module 7 - Emotion Exposures (Sessions 10–11)
In session 10, after the rationale behind emotion exposure was explained, the patients were prompted to create their emotion exposure hierarchy. They were separated into simultaneous video chat rooms to facilitate their reviews with the therapist and cotherapist. Patients’ hierarchies included opportunities for exposure to situations that could trigger intense emotions (e.g., driving over a bridge, scheduling a work meeting, writing or talking to someone close about their feelings, or imagining exposures). Exposures were not conducted in the session but independently by each patient as homework, which made it essential to prepare the patients during the session. Through screen sharing, the therapists and patients collaboratively completed the Emotion Exposure Practice Forms before the first exposure.
Session 11 took place two weeks after the previous session, which allowed patients more time to practice their emotional exposures. Catia, Mia, Eva, and Ana exposed themselves to external situations, whereas Sofia used imagination to visualize a conversation she had had with her father, which made her feel very uncomfortable and sad. The patients’ debriefings after the exposures were analyzed in the session. As no one completed an initial hierarchy of exposures, the therapists encouraged the patients to continue gradually practicing the exposures in daily life. Given the need to observe and prevent Ana’s attempts at emotional avoidance, the therapist scheduled an individual session with Ana to conduct imaginal exposure to thinking about bad things happening to her. Because Mia missed this session and because of the importance of the module, the therapist also met with her individually to review Mia’s practice and work together to advance the hierarchy. To maintain consistency with the group protocol, the duration of these individual sessions was less than 45 minutes.
Module 8 - Recognizing Accomplishments and Looking to the Future (Session 12)
All patients recognized the improvements in their symptoms and the importance of the strategies they had learned. Afterward, the therapists analyzed the patients’ improvements, long-term goals, plans for practicing the learned skills, and potential future difficulties. The patients’ Progress Record Forms were discussed via screen sharing. Figure 1 shows the mean patient scores on the OASIS and ODSIS across the 12 treatment sessions. It was important to discuss the individual peaks that occurred in various sessions, peaks that coincided with relevant life events of the patients (e.g., when Ana took her driving exam) or weeks of greater emotional exposure. At the end of the session, the therapists praised the patients for their commitment throughout the treatment and asked for feedback. All group members expressed great satisfaction with the group format (e.g., [Catia]: “The shared experiences helped me a lot… they encouraged me”; [Mia]: “One of the advantages is being in a group… the way the UP treatment is organized and structured helps a lot… it promotes a different level of commitment to the treatment”; [Ana]: “I learned a lot from this group”; [Sofia]: “I would highly recommend this intervention”; and [Eva]: “I really liked it because I did not feel alone”). Mean patients’ scores on severity and impairment of anxiety and depressive symptoms across 12 weeks of UP. Note. OASIS = Overall Anxiety Severity and Impairment Scale; ODSIS = Overall Depression Severity and Impairment Scale.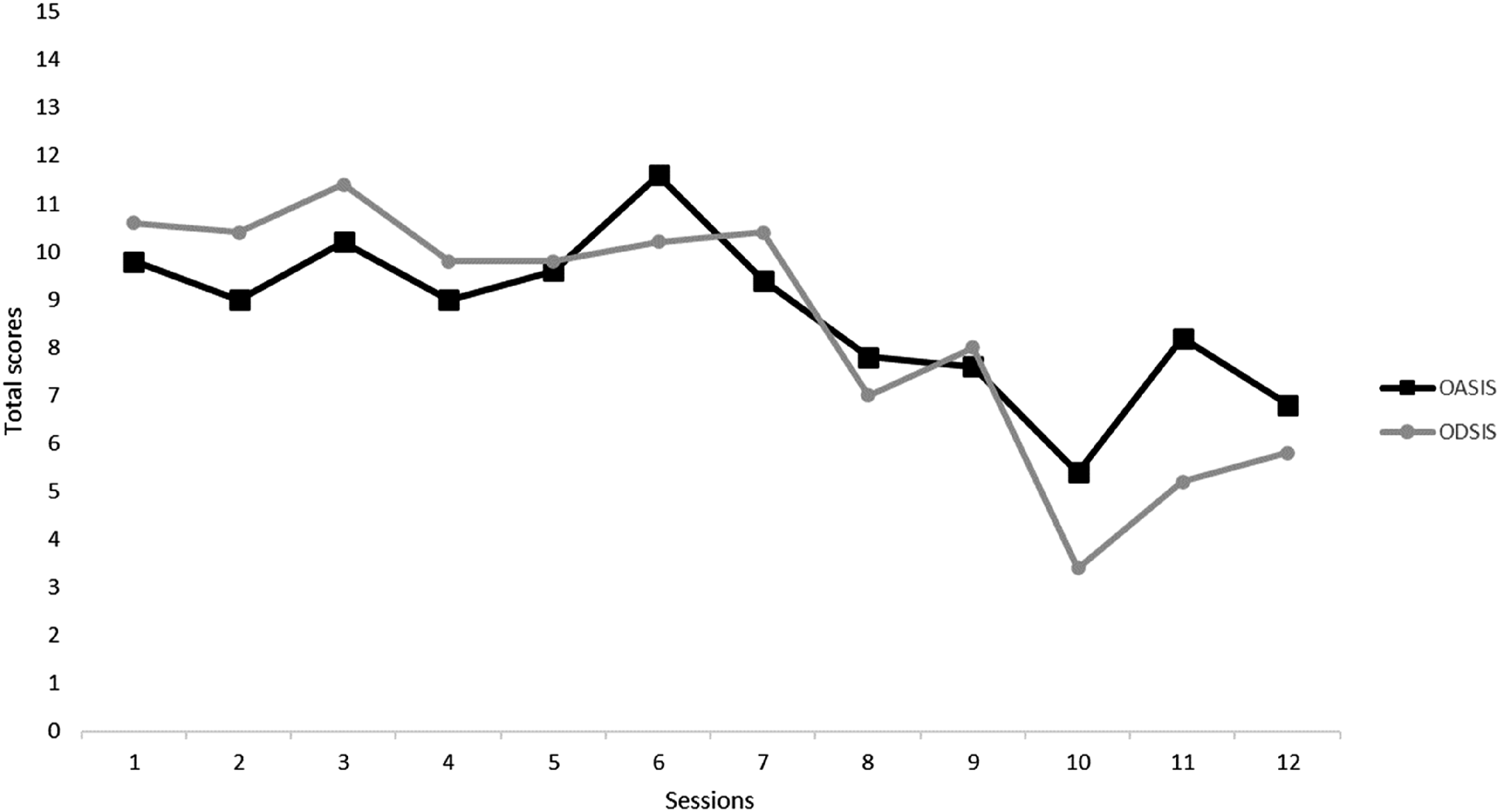
Assessment of Progress
At the posttreatment assessment, treatment gains were evident in patients who completed the treatment. The therapists noted positive changes in the severity of all five patients’ EDs compared to the baseline (see Table 1). Sofia’s CGI-S score decreased to 1 (normal, not at all ill), and her CGI-I score of 1 confirmed significant improvement. Cátia and Ana’s CGI-S scores improved from 6 (severely ill) to 4 (moderately ill), with a CGI-I score of 2 indicating much improvement. Mia was considered mildly ill with a CGI-S score of 3, whereas her CGI-I score of 1 reflected very much improvement. Eva showed notable improvement, with her CGI-S score dropping from 6 (severely ill) to 2 (borderline mentally ill) and her CGI-I score of 1 indicating much improvement.
The Reliable Change Index (RCI; Jacobson & Truax, 1991; Tingey et al., 1996) was computed to examine the changes in self-report measures from pretreatment to posttreatment (see Table 2) via the following formula:
Table 2 shows pre- to posttreatment changes in clinical variables, including depression severity (PHQ-9), anxiety severity (GAD-7), and impairment related to these symptoms (ODSIS for depression, OASIS for anxiety). It also includes changes in emotional regulation (DERS-SF), mindfulness (MAAS), behavioral activation (BADS-SF), and quality of life (EUROHIS-QOL-8). Posttreatment, all participants who completed the treatment showed significant decreases (p < .10) in PHQ-9 scores, indicating minimal to mild depression levels. With respect to the GAD-7 score, all participants showed reliable improvement (p < .05), with minimal to mild anxiety, except for Catia, whose scores remained in the moderate range. On the ODSIS, Sofia, Mia, Eva, and Ana demonstrated reliable improvement, whereas Catia showed a deterioration in depression impairment. Mia, Eva, and Ana had significant reductions in anxiety impairment on the OASIS, whereas Sofia and Catia showed no change. All participants who completed the treatment significantly improved emotional regulation and behavioral activation (p < .05). Sofia, Catia, Eva, and Ana demonstrated reliable improvement in mindfulness. Finally, the quality of life scores improved for all participants; however, only Sofia, Mia, Eva, and Ana showed significant changes in their perceived quality of life.
Acceptability and Satisfaction
The five patients who completed the intervention attended an average of 10 sessions, with four participants completing their homework each session. Most participants were very satisfied with the UP treatment, with all rating the treatment quality as excellent and indicating that they would recommend the UP to a friend needing therapy. Additionally, all patients who completed the program reported little or no discomfort from the treatment. With respect to the group format, all patients found it very acceptable, except for Ana, who found it only acceptable. Moreover, all of them indicated that they would choose the group format again. Sofia, Mia, and Eva classified the treatment duration as quite sufficient, whereas Catia and Ana rated it as very sufficient. The patients considered Conscious Emotional Awareness and Cognitive Flexibility to be the UP components most helpful in regulating emotions. Mia suggested adding an individual session at the end of the treatment. Susana was the only patient to rate a UP component below 7, awarding emotional exposures of 5 points out of 10.
Complicating Factors
Several factors complicated the group intervention. First, several participants struggled to complete the homework assignments, possibly because of the complexity of certain UP worksheets and resistance to written tasks (Kazantzis & Miller, 2022), as noted by Eva. To address this complication, the therapists suggested modifying tasks to meet individual needs, such as using audio recordings for weekly reflections. They also extended the homework review time in the main modules to enhance patient skills, following UP group guidelines (Bullis et al., 2015). Furthermore, the therapists’ decision to extend the interval between Module 7 sessions to two weeks proved beneficial, providing patients with more time to practice emotional exposures. Second, providing personalized feedback and adapting treatment skills in a group format proved challenging (Bullis et al., 2015) because of the limited time available for each patient. Sofia and Mia’s prior knowledge facilitated their understanding of concepts in this group, whereas others found them more challenging. None of the group members tended to monopolize the group, but several patients were less participatory, requiring the therapists to address them directly. Certain patients (e.g., Catia and Ana) could benefit from combining the UP with individual sessions to address specific difficulties.
Access and Barriers to Care
The online format of the UP group removed significant barriers to accessing treatment at home, and since the intervention was free as part of a research project, the patients incurred costs only for internet access. All patients had a computer or mobile phone and an internet connection at home. However, Catia struggled to find a private space and often attended meetings by phone in her car. Sessions were scheduled on Saturday afternoons to increase accessibility. Nevertheless, Eva and Ana faced challenges in punctuality because of their unpredictable work schedules. When patients missed sessions, the therapists provided support via email and telephone. Maria, Carmen, and Joana discontinued treatment because of personal and professional issues.
Follow-Up
A synchronous follow-up online group session was scheduled three months after treatment to determine whether the patients had continued to practice the skills they had learned (e.g., cognitive flexibility, emotional exposure) and to evaluate the maintenance of therapeutic gains over time. Sofia said that her mood had fluctuated over the last three months but mentioned, “I do not think I am depressed again.” Catia lost a family member in an accident and was still managing the grieving process. However, she reported that she was managing the situation better than expected. She also continued to practice emotional exposures (e.g., “traveling on the road with traffic does not disturb me so much anymore”) and was satisfied that she had not experienced any panic attacks in recent months (“I have had anxiety, but it is normal”). Mia continued to practice the learned strategies and mentioned that when she was exposed to previously feared situations, her anxiety levels “were acceptable”. Eva reported feeling “very well” over the past three months and continued to practice mindful emotional awareness exercises regularly. She said, “I was anxious about the meeting with my directors, feeling palpitations and nervous beforehand. But I attended without medication, expressed myself fully, and it went very well—no panic attack”. In contrast, Ana said that she came back feeling very anxious and depressed. She acknowledged that it had been difficult to continue practicing the strategies she had learned without weekly therapeutic accompaniment. All of the patients demonstrated a less judgmental attitude toward their emotional experiences.
At the follow-up session, the patients completed the same self-report measures that were completed at previous assessments (i.e., the PHQ-9, GAD-7, ODSIS, OASIS, DERS-SF, MAAS, BADS-SF and EUROHIS-QOL-8). As shown in Table 2, the patients generally maintained the improvements in their symptoms of depression and anxiety after therapy, except Ana, whose symptoms worsened and whose symptoms returned to moderately severe and severe levels of sadness and anxiety, respectively. Compared with the preintervention values, all the subjects had better scores on the DERS-SF, MAAS, BADS-SF and EUROHIS-QOL-8.
Treatment Implications of the Case
This case study illustrates the promising implementation of the UP in a synchronous online group format for treating comorbid EDs, highlighting its flexibility. In line with the findings of Celleri et al. (2022), the outcomes of the five patients who completed the intervention suggest that the UP in this format has a positive effect on reducing depressive and anxiety symptoms and improving difficulties in emotional regulation, mindful awareness, behavioral activation, and quality of life. This demonstrates that the UP may be useful and effective in addressing shared factors underlying the etiology and maintenance of EDs, making it potentially more effective for treating comorbid EDs, as supported by other studies (e.g., Osma et al., 2022; Steele et al., 2018). However, certain participants may not have shown clinically significant changes in certain variables. Possible explanations for this lack of significant quantitative change include underestimating or overestimating symptoms, as well as situational and temporal factors (e.g., fatigue) at the time of assessment. For example, Catia did not show significant changes in PHQ-9 or GAD-7 scores between pre- and posttreatment. Nevertheless, these changes would be significant if we considered her initial screening scores. Another possible explanation is limited practice between sessions, which may have limited the gains achieved with the UP and hindered the development of emotional regulation strategies.
We highlight that no participants received additional interventions during the 3 months following treatment. However, four patients maintained therapeutic gains at the follow-up assessment, and some showed more significant clinical improvements. Having more time to practice the strategies learned in daily life may have contributed to these positive outcomes. In contrast, the lack of consistent practice of the skills learned during treatment could explain the deterioration of Ana’s symptoms.
Furthermore, consistent with the findings of Celleri et al. (2022) and Martínez-Borba et al. (2022), all the participants who completed the treatment reported high satisfaction with the format and content of the sessions, suggesting that the UP in a synchronous online group format is a promising and acceptable therapeutic approach. The advantages of combining group and online formats that the patients highlighted, such as easier access, scheduling flexibility, reduced travel costs, decreased isolation, and increased social support and vicarious learning, align with the findings of prior research (Osma et al., 2019; Pedro et al., 2024). However, the treatment adherence rate was 62.5%, which is lower than the rates reported in other studies on online group CBT (e.g., Ryan et al., 2023) or other UP formats (e.g., Barlow et al., 2017). Nevertheless, it should be noted that the three dropouts occurred for reasons unrelated to the treatment itself or the format of its delivery, such as sudden changes in family or professional routines. To improve participant adherence and between-session engagement in future studies, several strategies could be implemented, such as using digital reminders for homework completion, simplifying some exercise forms, or integrating app-based tools to support the daily practice of UP skills.
Despite all the adaptations made to preserve the integrity of the treatment (e.g., using screen sharing to explain the UP forms), we must acknowledge certain barriers to applying the UP in this therapeutic format for both therapists and patients (Gros et al., 2013; Osma et al., 2019). Therapists faced technical failures and found that conducting certain UP exercises via videoconference (e.g., interoceptive exposure exercises) was more difficult. Additionally, ensuring patients’ privacy and safety was challenging because therapists could not control patients’ physical environments. Moreover, when a patient missed a session, additional contact was needed to explain the session’s content and the exercises that were missed. Some patients struggled to understand and personalize the learned strategies and might benefit from a combination of individual and group sessions. For example, Ana could benefit from additional sessions focused on specific modules (e.g., cognitive flexibility) and more personalized exercises targeting particular difficulties, such as intrusive thoughts and compulsions. Although the group protocol was preserved, two participants received brief individual sessions (1–2 sessions, each lasting less than 45 minutes) to review content they had missed or found particularly challenging, particularly the emotional exposure module. These sessions were intended solely to support understanding of and adherence to the group content. While not considered a deviation from the protocol, they may introduce a source of variability and should be considered when interpreting the results, and further explored in further efficacy studies. Although the quantitative and qualitative data are encouraging, the results of this case study should be interpreted conservatively and cannot be generalized to all patients. Importantly, all the participants in this study were women, which may limit the generalizability of the findings. This was not an intentional exclusion criterion but rather reflects the recruitment response, aligning with the findings of Pedro et al. (2024), which suggest that women tend to be more receptive to transdiagnostic and group treatments than men. This sample composition may have influenced group dynamics and outcomes.
Recommendations to Clinicians and Students
This study has several implications for research and clinical practice. In addition to the considerations of receiving certified training in the UP and obtaining treatment manuals, the importance of therapists’ specific skills for effectively implementing the UP in online and group formats should be emphasized. These skills include technological familiarity, flexibility, organizational skills, effective communication, and the ability to create connections and remain empathetic while virtually moderating group dynamics (Pastor et al., 2019). As a future research direction, the research team will conduct further studies to assess the clinical viability and efficacy of the UP in a synchronous online format through a clinical trial, comparing it with face-to-face group formats. Additionally, given the lack of resources in mental health services, the effectiveness of the UP in online and group formats within public health services in Portugal should be explored. Finally, future research should also focus on studying transdiagnostic mechanisms as mediators of psychological change. Moreover, whether the results differ across mixed-gender groups should be examined, and gender-based comparisons in response to UP should be explored.
Footnotes
Acknowledgments
We would like to thank all the participants who were encouraged to participate in this study and kindly allowed them to share their stories in this publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Liliana Pedro was supported by a PhD scholarship by the Portuguese Foundation for Science and Technology [Fundação para a Ciência e a Tecnologia] (2021.04854.BD).