
Abstract
This case study aims to describe the application of the Unified Protocol (UP) for Transdiagnostic Treatment of Emotional Disorders in the case of a 30-year-old patient with a diagnosis of Ultra-high Risk for Psychosis (UHR) and comorbid anxiety and depression. UP is a psychological intervention that uses cognitive-behavioral techniques whose objective is to reduce emotional dysregulation, which is one of the transdiagnostic mechanisms of emotional disorders. UP has demonstrated its efficacy in samples of patients with emotional disorders. Frank was a 30-year-old man diagnosed with UHR and other emotional disorders (major depressive disorder, bulimia nervosa, generalized anxiety disorder, and social anxiety disorder) who underwent the UP intervention in 15 group and online sessions, lasting 2 hours each, over the course of 4 months. At the 6-month follow-up evaluation, Frank presented significant improvement in all emotional and functioning variables: anxious and depressive symptoms, negative and positive affect, neuroticism and extraversion, emotional dysregulation, maladjustment, and quality of life. There was also a reduction in subthreshold psychotic symptoms. Frank no longer met the criteria for any emotional disorder. We also found an improvement trend, although not significant, in other variables such as insight and cognitive biases measured with specific questionnaires for psychosis. Frank attended all treatment and follow-up sessions and rated the program very positively. UP may be a clinically useful treatment for young people with comorbid UHR and emotional disorders in the early stages of mental health illnesses that could improve clinical and functional outcomes.
1 Theoretical and Research Basis for Treatment
Ultra-high risk (UHR) for psychosis consists of a group of symptoms that may precede the onset of psychosis. Traditionally, they have been described retrospectively as attenuated symptoms that could appear before a first psychotic episode, and they have been referred to as “prodrome of psychosis” (Yung et al., 2005). In recent years, psychosis has been conceptualized as a continuum of clinical manifestations ranging from psychosis-like experiences in the general population to psychotic disorders (Nelson et al., 2012). In this line, a staging model has been proposed that describes the appearance of symptoms from lesser to greater clinical intensity, and functional repercussions linked to therapeutic recommendations adapted to each of them (McGorry et al., 2018). In a recent systematic review (Albert, et al., 2018), 46 studies were analyzed with the aim of estimating the comorbidity between UHR and emotional disorders (anxiety, depressive and related disorders; Barlow, Farchione, et al., 2018). The results demonstrated that a high percentage of patients with UHR also met the diagnostic criteria for emotional disorder. The percentages reached 50.9% in the case of anxiety disorders and 66.7% for major depressive disorder (MDD). Here, they recommended that emotional disorders should be the main focus of intervention for patients with UHR.
Among the available evidence-based psychological interventions, cognitive behavioral therapy (CBT) is the most widely recommended by the main clinical guidelines for the treatment of patients with UHR (e.g., NHS England, N.C.C. & Excellence, M.H., 2016), with a focus on improving subthreshold psychotic symptoms (e.g., French & Morrison, 2004; van der Gaag, Nieman, & van den Berg, 2013). The results have shown efficacy in reducing the severity of these symptoms and also in delaying the onset of psychosis in those who show a transition (van der Gaag, Smit, et al., 2013). Existing CBT for UHR patients is mainly focused on the treatment of psychotic symptoms and there is not yet a transdiagnostic proposal that integrates intervention for comorbid emotional disorders exhibited by these types of patients. In this regard, the Unified Protocol (UP) for Transdiagnostic Treatment of emotional disorders Barlow, Farchione, et al., 2018) was developed based on the vulnerability mechanisms shared by emotional disorders (e.g., high neuroticism and low extraversion). Barlow’s functional model for emotional disorders states that people with emotional disorders [1] feel frequent and intense emotions (e.g., anxiety, sadness) that provoke [2] a negative reaction (e.g., “I shouldn’t be feeling this way”) and, therefore, [3] an active attempt to avoid or escape them (e.g., going out from a cloudy space)”. The UP is a cognitive-behavioral intervention based on improving the emotion regulation strategies of individuals with emotional disorders. The aim of the UP intervention is to learn to tolerate intense emotions—that is to say, to change the way emotions are reacted to, from an attitude of acceptance and with more effective and adaptive responses that enable the goals of the people experiencing them to be achieved (Barlow, Sauer-Zavala, et al., 2018).
UP Modules of Treatment.
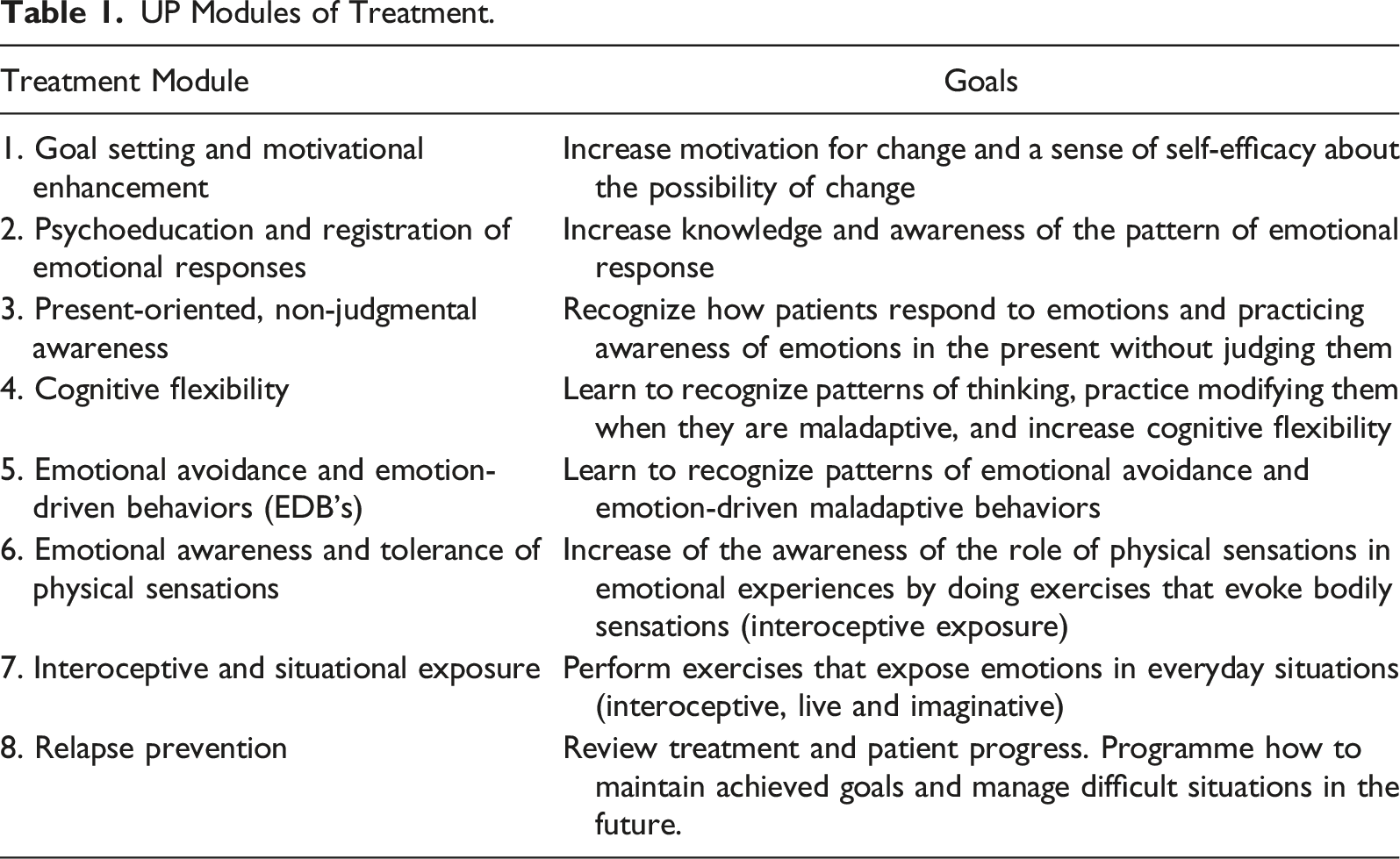
We already have scientific evidence indicating that UP is equally effective for the treatment of emotional disorders, including cases with comorbidity, as are specific treatments for each emotional disorder (Eustis et al., 2020). In addition, statistically significant changes have been observed in decreased neuroticism, increased extraversion, and improved quality of life (e.g., Sauer-Zavala et al., 2021). The UP is a protocolized and manualized treatment with great versatility, which allows it to be adapted to different contexts, formats, and clinical cases (Sakiris & Berle, 2019). The good preliminary results of these studies suggest that UP could be used to improve emotional regulation and quality of life for people with symptoms and/or emotional disorders with other comorbid mental disorders. The UP in a group format is a cost-effective therapy to apply in the public health system, as has been recently observed in our country. UP treatment was cheaper than individual face-to-face treatment, significantly improved quality of life and reduced the need for pharmacological doses at long-term follow-up (Peris-Baquero et al., 2022).
UP could be a good treatment option for young people who are in the early stages of a mental disorder, as it provides strategies to manage the full range of presenting symptoms (anxiety, depression, subthreshold psychotic symptoms) with the aim of preventing progression to more serious diagnoses.
Our research team is made up of part of the clinical team of our early intervention program in psychosis (PIPPEP), professionals of the Research Department in Parc Sanitari Sant Joan de Déu and Dr. Osma PhD from the University of Zaragoza. We are currently conducting a randomized controlled trial (RCT) to test the efficacy of UP in patients with UHR and comorbid emotional disorders (Peláez et al., 2022). This case study is from one of the patients in the sample who was treated with the UP.
Case Introduction
Frank is a 30-year-old, single, Caucasian male who was referred to the Community Mental Health Center of Ripollet (Parc Sanitari Sant Joan de Déu) by his GP for depressive symptoms and suicidal thoughts. After two sessions with one of the team’s psychiatrists, he was referred to PIPPEP for assessment due to suspected subthreshold psychotic symptoms. PIPPEP is an early intervention programme for psychosis integrated into the Ripollet Mental Health Centre (Parc Sanitari Sant Joan de Déu), which is part of the public mental health network in Catalonia. After the assessment, he was admitted to the PIPPEP programme as UHR for psychosis was confirmed.
Frank was born in Catalonia. He had an older brother and lived with his mother and brother in the family home. In school Frank already had difficulties, mainly from the age of 14. He had suffered bullying for several years. He was, however, able to finish high school and vocational training. He also had difficulties with social relationships from adolescence and thereafter experienced anxiety when he was with others outside the family. He explained to us that it was difficult for him to open up to people and he felt rejected by them. This made his social relationships very few and unsatisfactory. His hobbies included playing paintball, seeing movies, playing board games, reading comics, and collecting ceramic figures that he painted himself. He almost always pursued these activities alone and avoided social interaction as much as possible.
A year and a half before he came to the emergency room, the depressive symptoms reappeared, coinciding with the Covid pandemic. As a result, he had to quit his job and went to see his GP, who initiated treatment with antidepressants. At the time, he was working as an usher at a football stadium.
As for his psychiatric history, he reported a first depressive episode with a suicide attempt when he was 14 years old, after the death of his father. At that time, he was hospitalized for 1 month. He then had further depressive episodes, from which he achieved remission, enabling him to work intermittently.
2 Presenting Complaints
For about a year, Frank had again felt sad and irritable, and self-isolated at home. Among triggers, there was gallbladder surgery, his mother’s admission to hospital with pneumonia, and confinement due to the pandemic. He went to his primary-care outpatient clinic, where he was offered psychological treatment, with little improvement. For 2 months he had the feeling that someone was watching him, that people spoke ill of him, and that they followed him every time he went out into the street. He also felt watched when he was at home; he believed that the neighbors across the street were spying on him. When he was having a conversation, he got the feeling that people were dropping hints to make him feel bad. Occasionally, he heard footsteps and voices calling his name when there was background noise. Sometimes he had the feeling that his thoughts could be heard by other people. He thought that all these sensations could be the product of his mind, but even so, he couldn’t help but feel a lot of anxiety every time they appeared, and he avoided leaving the house in order to reduce the anxiety. When he was in the salon of his house, he needed to have the curtains drawn so as not to feel excessive discomfort. Depressive symptoms had also worsened in the preceding 2 months. He had negative thoughts about himself and ideas of guilt (“I do everything wrong”, “I am worthless”). It took a great effort to carry out everyday activities and he did not enjoy the things he normally did for entertainment. He had started to close himself in his room because he did not think he was able to go out, or even interact with his family. He also stopped doing his daily activities and started having suicidal thoughts again. At times when the anxiety and guilt were very intense, he needed to cut himself or binge eat to relieve the discomfort.
3 History
Frank lived with his parents and brother until his father passed away when he was 13, from an acute myocardial infarction in his presence and in the presence of his mother. According to Frank’s psychiatric family history, he stated that his father had problems with gambling and alcohol. He never sought help from a psychiatric service. Shortly before his death, the family had financial problems that ended with the foreclosure of the house in which they lived. For this reason, they had to move house and change schools several times, to which Frank was able to adapt without too much difficulty. As a child he was shy, although he had no problems with his schoolmates. As his mother explained, he was orderly and very polite.
Frank began to have academic difficulties at vocational training, after his father’s death and had to repeat the second grade twice. Nevertheless, no school support was requested. At the age of 14, he had his first depressive episode that required hospital admission after a suicide attempt. After this, he gained a lot of weight and was bullied by his classmates because of it. From this moment on, social interaction became increasingly rare. Since he was 14 years old, he has undergone psychiatric and psychological treatment with several professionals. At this point they conducted a cognitive examination, including a WISC. His intelligence quotient was 114.
Depressive episodes were repeated on various occasions, leading to isolation in his room. Between these episodes there were periods in which the depressive symptoms subsided and during which he was able to work and enjoy his hobbies. At the age of 24, he had a job that required him to travel around Europe, and he lived abroad for a while. He worked in a company as a mechanic assembling production lines in factories. He lived with his mother and brother. The family relationship was good. He had had few friends. According to his mother, he was always very generous to them, but they took advantage of him.
4 Assessment
When Frank was referred to our service, he was administered the CAARMS (Comprehensive Assessment of At-Risk Mental States) to determine if he met UHR criteria and could benefit from our Early Intervention Program for Early Psychotic Episodes (PIPPEP). The CAARMS (Yung et al., 2005) is a semi-structured assessment tool used by mental health professionals and researchers to identify young people seeking help who are at UHR for psychosis. For diagnosis of UHR, the short version of the interview is used, which includes the four subscales of positive symptoms (‘unusual thought content’, ‘non-bizarre ideas’, ‘perceptual abnormalities’ and ‘disorganized speech’). He scored points on the subscales ‘unusual thought content’ (e.g., feeling that his thoughts could be heard by other people), ‘non-bizarre ideas’ (e.g. feeling that he was being watched, talked about, followed and talked to in double meanings), ‘perceptual abnormalities’ in the auditory modality (e.g., feeling that his name was called when he was in a place with background noise) and ‘disorganized speech’ (subjectively referring to feeling that he was not expressing himself properly). Subsequently, and after confirming that he met the criteria for the ‘Attenuated Psychosis’ subgroup, he was offered the opportunity to participate in the clinical trial of the application of UP in patients with UHR. Before randomization, he was evaluated with the battery of tests of the study protocol (Peláez et al., 2022).
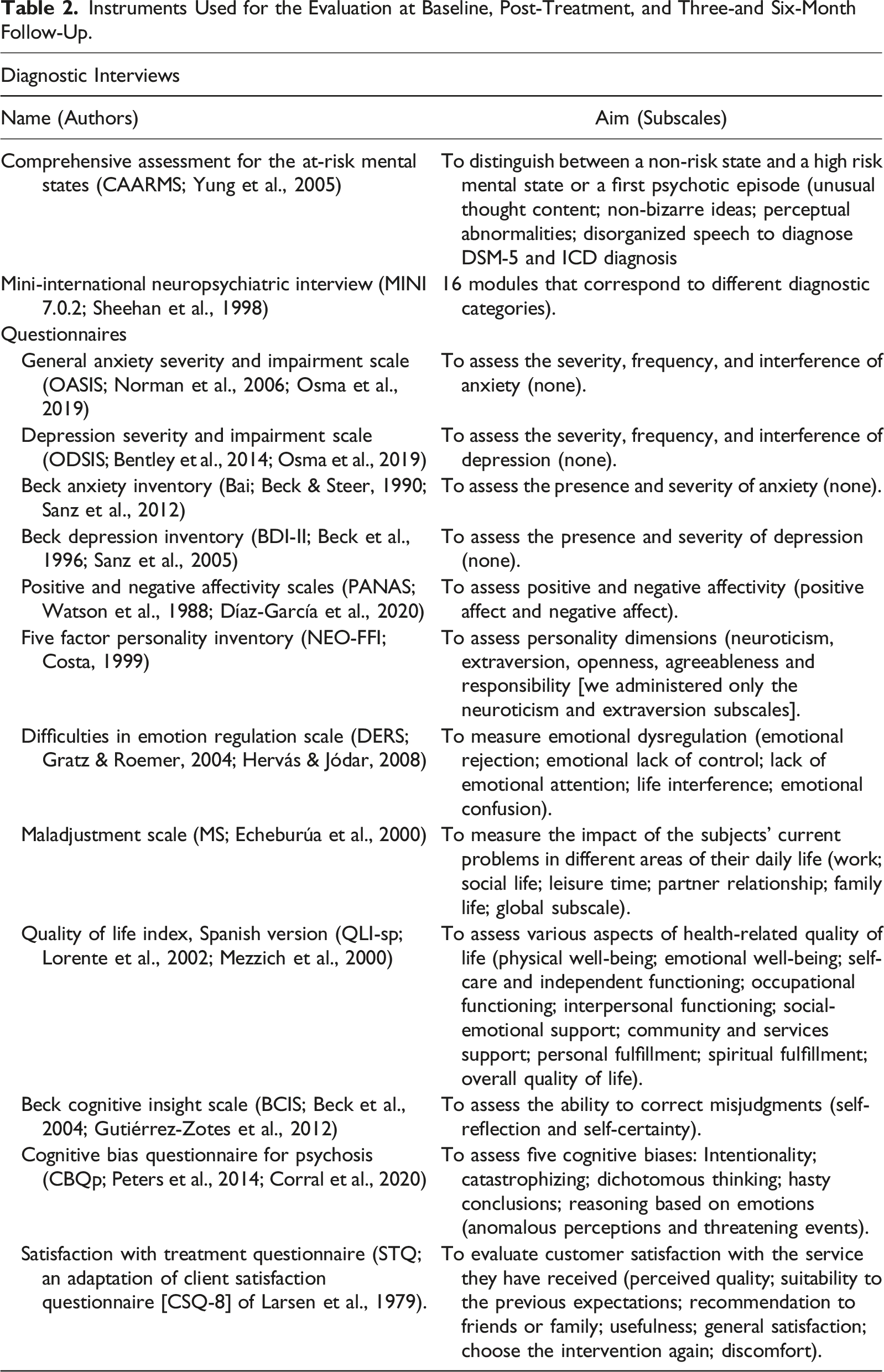
Frank’s scores for anxiety and depression were very high, as were his scores for emotional dysregulation, negative affect and maladjustment. His score for quality of life was very low, as was his score for positive affect. He also had a high score for neuroticism and a low score for extraversion. In the MINI 7.0.2, Frank met the criteria for five diagnostic categories: Major Depression, Agoraphobia, Generalized Anxiety Disorder, Bulimia Nervosa and Social Anxiety Disorder.
Instruments Used for the Evaluation at Baseline, Post-Treatment, and Three-and Six-Month Follow-Up.
5 Case Conceptualization
The case formulation or conceptualization according to the UP raises the need to evaluate four fundamental elements. In the case of Frank, the affected areas due to the experience of intense and frequent emotions were professional, family, social, physical health, and leisure. The emotions that he experienced frequently and intensely that caused him great discomfort were, above all, anxiety, depression, guilt, and anger. We may observe Frank’s rejection of the emotional experience by the interpretations he made when experiencing anxiety, for example, “anxiety means that it is true that they are watching me”, or regarding sadness, “I will never be like the others.” Regarding avoidance or escape behaviors (also known as emotional behaviors), we identified cutting himself, binge eating, isolating in his room, spending a lot of time in bed, not going out, avoiding going to places he used to go, and needing to close the curtains when he was in the salon at home. When he did go out, he would walk fast, avoid people, and try to distract himself as much as possible by looking down and listening to music.
6 Course of Treatment and Assessment of Progress
Course of Psychological Treatment
Frank began treatment at the Ripollet Mental Health Centre (Parc Sanitari Sant Joan de Déu) with a psychiatrist, with whom he completed two sessions. Noting possible symptoms of attenuated psychosis, she referred him to the PIPPEP team, located in the same mental health centre. The PIPPEP team consists of a clinical psychologist, a psychiatrist, a nurse, and a social worker who provide intensive treatment for up to 5 years. The team members have been working with patients with early psychosis for 2–18 years and have received special training in early intervention for psychosis. When he started visiting our Mental Health Center, Frank had great difficulty coming in due to the anxiety he experienced on the way home, in the waiting room, and inside the office. When he was able to, he avoided eye contact, had a hard time expressing himself, and was very fidgety throughout the session. When the individual intervention sessions had been completed, he was offered the opportunity to participate in our randomized clinical trial to evaluate the efficacy of UP in the treatment of comorbidity in patients with UHR treated in our program of early intervention in psychosis (PIPPEP). As a participant in the RCT, Frank took part in an online group intervention with the UP as a supplement to the TAU in PIPPEP, where he also received individual CBT sessions. The therapists in the group are clinical and research psychologists and have been trained in the application of the UP. The online group format of the UP treatment was an advantage for Frank since he could do the sessions from home. We shall describe the psychological intervention in two phases: the first part that was carried out individually before starting the UP group, and then the intervention applying the UP modules.
Initially, eight individual sessions were held, four for evaluation and four for intervention. In between, online visits were made, since Frank could not attend in person due to anxiety. In these sessions, we worked on the normalization of psychotic experiences, providing information on studies of psychotic-like experiences in the general population (Garrett et al., 2006). We began to work on the “emotional reasoning” bias at a metacognitive level, which in Frank’s case involved thinking through together to what extent the feeling of being watched could be taken as a reality test that people were really looking at him (van der Gaag, Nieman, & van den Berg, 2013). At this point, we made a connection between the fear that someone might hurt him and the increased hypervigilance as a result of the bullying experiences he had had in his youth. From then on, we started designing behavioral experiments to gather evidence for and/or against the idea that he was being watched by others every time he had this feeling. For example, when he was walking down the street and felt that he was being watched, he did not look at the ground but looked around and counted how many people were there and how many of them were watching him. Each time he did this, he wrote it down in a log and the results were discussed in session to see if they could be considered as evidence for or against the belief “If I feel I am being watched, it is because everyone is staring at me”. It was difficult for Frank to pay attention to the people around him, as he usually avoided eye contact as a safety behavior. The anxiety associated with going out on many occasions also prevented him from doing so. Despite this, he was able to collect evidence when he felt observed at home and when he went out the few times he could. The “selective attention for threat” cognitive bias has also been identified in people who meet UHR criteria for psychosis (van der Gaag, Nieman, & van den Berg, 2013). In Frank’s case, this manifested itself mainly when he went out to the street and there were people around him. We began to work on this hypervigilance to danger as a factor in maintaining the problem, since this turned his attention to stimuli that, according to him, could pose a threat. At this point in the intervention, we began the UP sessions in an online group format. Below, we will examine the content of each module and how this was worked on in Frank’s case.
Module 1: Setting Goals and Maintaining Motivation
The medium-term goals that Frank proposed were to reduce fear of people and going out, improve mood, decrease irritability, lose weight, gain self-confidence, overcome fear of the perceptual disturbances he experienced (footsteps and murmurs that called him by his name), and, finally, go back to work. When we defined the specific goals to work on in the UP sessions, Frank chose to take public transport again to go to a game store to play cards, and also to spend less time in his room.
The decisional balance exercise is part of this module. It aims to address the ambivalence of change by analizing the advantages and disadvantages of engaging with the UP treatment or not. This exercise is often used when applying the motivational interviewing technique to create discrepancy in patients and motivate them to change (Miller & Rollnick, 2002). In Frank’s case, the decisional balance exercise was very useful, since he had been having depressive episodes and anxiety symptoms for years and had lost hope of improving with treatment. In addition, the fact that the format of the therapy was group introduced an additional doubt until the last moment as to whether to accept participation in the study or not. However, he considered the benefits he could derive if he tried the UP intervention, (such as being less depressed, going to places where there are other people, getting involved in positive activities again and having more satisfying relationships) and finally decided to give himself another chance to recover.
Module 2: Understanding Emotions
A fundamental part of the approach to subthreshold symptoms of psychosis consists in normalizing psychotic experiences with the aim of reducing discomfort, since there are many erroneous beliefs associated with its appearance (Garrett et al., 2006). This, in turn, often produces negative emotions that increase the frequency and intensity of these experiences. The ARC is a concept used in UP to understand how emotional experiences develop. It is an acronym where A refers to the antecedent that triggers the emotion (Antecedent), R refers to the emotional response (Response), which is made up of thoughts, physical sensations and emotion-driven-behaviors (EDB’s) and C refers to the short- and long-term consequences (Consequences) of the EDB’s. In this module, these concepts are explained and practiced using examples offered by the patients based on their own experiences. Frank learned to do ARCS and recognized that when he went out, and sometimes also when he was at home, he had the feeling of being watched (‘Antecedent’). This triggered an intense anxiety (‘Emotional Response’) that was made up of negative automatic thoughts (‘Thoughts’) such as “if I feel observed, there must necessarily be someone watching me” (people on the street or neighbors across the street). In addition, he always tended to make negative and threatening explanations as to why they might be looking at him (“they are going to mess with me because of my physique”, “they are judging me”, “they think I’m fat”). When this happened, he needed to do certain behaviors (EDB’s) to try to decrease the intensity of the emotion, such as avoiding eye contact by looking at the ground, distracting himself (listening to music or thinking about something else), or walking faster to get home as soon as possible and lock himself in his room. If this happened to him at home, he needed to draw the curtains to calm the anxiety caused by the thought that the neighbors across the street were looking at him. All these behaviors, in the short-term, provided relief, but in the long term they made him feel sad and guilty because they did not solve his problem. Regarding sadness, Frank identified some negative automatic thoughts (“I’m doing everything wrong”, “I’m worthless”, “I’m a burden to the family”, “I should be dead”) that justified his discomfort. This produced a feeling of heaviness throughout his body and a knot in his stomach and localized tension, mainly in his head. When he was under the influence of this sadness, Frank felt like isolating himself and self-harming.
Module 3: Mindful Emotion Awareness
In this UP module, three exercises are carried out with the aim of focusing on the present and observing the emotional response without acting and without judging oneself. In the first, the ability to accept and normalize emotional experiences is developed, instead of labeling emotions as problematic and trying to eliminate them. To do this, a group exercise was carried out that consisted of eating a piece of candy and focusing attention on that experience. When thoughts appeared that distracted Frank’s attention from the present, he had to refocus his attention on the candy without judging himself. As homework, Frank chose to paint a figure by focusing his attention on the smell and color of the paint, the feel of the figure, and how the brush moved around its outline. The second exercise consisted of listening to two songs to induce a moderate emotion and observing the emotional response at that moment and without reacting, just observing. When the song finished, the members of the group shared their thoughts and physical sensations, and what they had felt the need to do. In the third exercise, an alarm was programmed without the members of the group being able to anticipate when it was going to sound, and at that moment the goal was to anchor themselves in the present and observe each component of their emotion. It was discussed together whether the behavior had to do with what was happening in the present or, rather, with an event related to the past or the future. If the reaction had nothing to do with the present, they were given instructions to change their behavior to one more in keeping with the situation in which they found themselves at that moment.
Module 4: Cognitive Flexibility
The aim of this module is to improve understanding of how thoughts influence emotions, to recognize negative automatic thoughts when intense emotions occur, and to generate alternative thoughts to increase cognitive flexibility. Examining Frank’s ARCs, we were able to identify several negative automatic thoughts related to anxiety (“people are going to think I’m fat and they’re going to mess with me”, “people keep looking at me because there’s something wrong with me”, “they follow me”) and other thoughts (“I don’t move ahead”, “whatever I do I will always be wrong”) related to sadness and guilt. Frank was helped by using cognitive flexibility to find alternative thoughts to explain why people might look at him (“they look at me because they like my shirt, because I’m very tall, or just by chance”) and others (“now nobody messes with me, this is part of the past”, “it doesn’t happen, why go over it again”, “now I’m different, if they messed with me, I would know how to deal with it”). This eased his anxiety considerably and he realized that when he was walking down the street and looked at someone, it was for much the same reasons. At this point in the intervention, we began to differentiate when emotion was justified and when it was not, to decide if the group members had to solve the problem or generate alternative thoughts to regulate their emotion. To do this, we used a decision diagram (Crespo-Delgado et al., 2020) that could be applied in all situations that arose. Therapists provided some psychoeducation about the problem-solving and assertiveness techniques as resources for interpersonal situations that could generate discomfort (e.g., “I was at the post office to post a parcel, and the person who waited on me spoke to me in a derogatory tone. I asked him to speak properly, as I had been polite to him”). It is worth mentioning that the original UP (Barlow, Farchione, et al., 2018) for adults does not include training in problem solving or assertiveness techniques, although in this case, we considered it relevant to include them briefly. In the case of Frank and many of his colleagues, the acquisition of the skill worked on in this module was the one that required the greatest effort of all the skills developed in the UP.
Module 5: Countering Emotional Behaviors
Emotional-motivating avoidance coping strategies constitute a factor in the maintenance of emotional disorders (Barlow et al., 2021) and also of psychosis (Phillips et al., 2009). In fact, it has been included as one of the main transdiagnostic mechanisms involved in the maintenance of emotional disorders and neuroticism (Barlow et al., 2021). In Frank’s case, his BDE’s of anxiety and sadness consisted of not going out into the street, not leaving his room and drawing the curtains to avoid feeling observed by the neighbors, and looking at the ground and walking quickly to get home as soon as possible. As for subtle avoidance behaviors, he closed his eyes when he had to go out or wore headphones to listen to music. He also went out accompanied whenever he could (safety behavior). He engaged in cognitive avoidance behaviors: he was distracted by thinking about other things, he worried excessively, or he had ruminative thoughts. In this module we worked on the short-and long-term consequences of emotional behaviors. In the short term, all these behaviors produced relief, but in the long term, they did not allow him to achieve his goals, and they also generated more negative emotions (sadness, guilt, and anger). Being aware of the role these behaviors played in maintaining his problem helped him feel motivated to change them to more useful ones (opposite or alternative behaviors).
Module 6: Understanding and Confronting Physical Sensations
This module aims to improve recognition of physical sensations as part of the emotional response, to better tolerate them and to work through the associated catastrophic thoughts that usually increase the intensity of negative emotions. The physical sensations that Frank experienced when he felt anxious (tachycardia, sweating, nausea, pressure in his head, burning face) were interpreted by him as signs that something bad was going to happen to him (having a heart attack, collapsing, dying, losing control). From here, we thought of exercises that he could use to voluntarily induce these physical sensations (hyperventilate, put weight on his chest, put on lots of clothes and the heater to get over-heated and then go outside) and see if the catastrophic interpretations appeared. In the case of sadness, the physical sensation that caused the most discomfort was heaviness of his body. In order to better tolerate this sensation, Frank exposed himself to it by putting on a backpack and a coat that he had previously loaded with heavy objects. The conclusion Frank reached was that the discomfort associated with his physical sensations had to do with the catastrophic interpretations he made of them when they appeared in the context of intense emotion and that, in contrast, they were absent when he recreated them voluntarily. This helped to lessen the intensity of the negative emotions he was feeling, and furthermore, repeated exposure to these feelings helped him to better tolerate them, so that they were no longer so unpleasant when he did experience them.
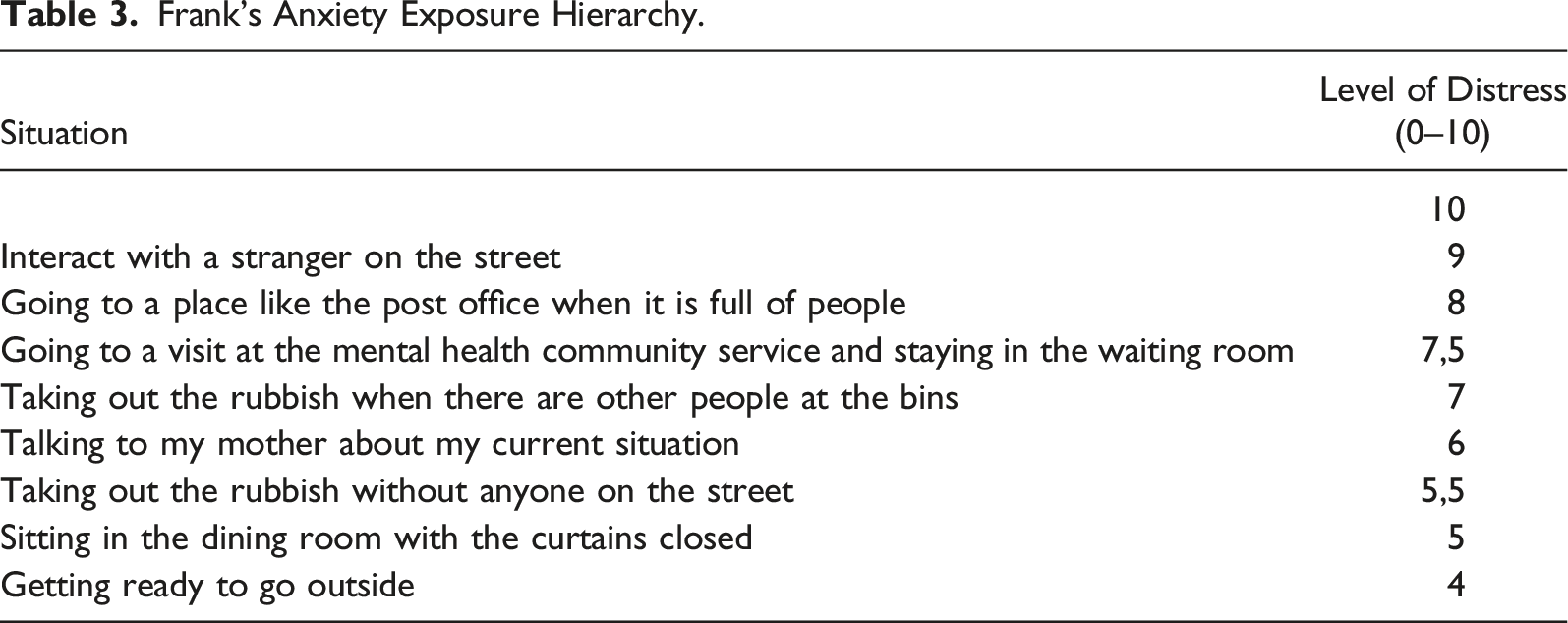
Module 7: Emotional Exposures
Frank’s Anxiety Exposure Hierarchy.
Module 8: Recognizing Accomplishments and Looking to the Future
In this last module of the treatment, we identified and reinforced all the achievements made throughout the sessions. We encouraged Frank to congratulate himself every time he made an effort to expose himself to a situation that caused him discomfort using emotional regulation techniques. Frank selected some activities that he could use as reinforcements for the achievements he was achieving. Among these was buying a new figure to color or having a sugar-free soda. We also worked on the importance of remembering your goals whenever you feel a drop in your motivation. Lastly, we identified new goals for the future, including connecting with more people and getting back to work.
Pharmacotherapy
Before coming to PIPPEP, Frank was taking antidepressant medication (150 mg/day of Sertraline) prescribed by his general practitioner (GP), to treat his depressive and anxiety symptoms, but there was no improvement. The GP referred Frank to the Community Mental Health Centre for specialized treatment. Then the psychiatrist suspected that there might be subthreshold psychotic symptoms and referred Frank to PIPPEP for assessment. The psychiatrist of PIPPEP then changed the antidepressant treatment with Sertraline to 375 mg/day of Venlafaxine, to treat anxiety adding 75 mg/day of Pregabalin, 30 drops/day of Rivotril, and for psychotic symptoms up to 7.5 mg/day of Olanzapine. The latter was also used at times when Frank felt a lot of anxiety. During the time that he was taking the medication, adjustments were made to the dosage, since he had great difficulties controlling anxiety and he had not noted any improvement in his mood.
Assessment of Progress
The attenuated psychotic symptoms measured with the CAARMS improved considerably, to the extent that he did not fulfill the UHR criteria at the 6-month evaluation. More precisely, non-bizarre ideas remitted. He no longer felt that someone was following him or watching him as he walked down the street. He could stay in the dining room of his house with the blinds drawn up without experiencing anxiety because the thoughts of the neighbors watching him also disappeared. He no longer noticed people speaking ambiguously to him with the intention of making him feel bad. Unusual thought content also improved. He no longer felt that his thoughts could be heard by other people. Perceptual abnormalities also disappeared (hearing his name being called). Frank began to feel less threatened by people and to stop caring what others might think of him. He started going out, shopping at stores near home, and going to the gym.
At baseline, Frank met criteria for five emotional disorders, in addition to the UHR criteria: MDD, agoraphobia, bulimia nervosa, generalized anxiety disorder (GAD), and social anxiety disorder. In the follow-up 3 months after finishing the intervention with the UP, he met the criteria only for social anxiety disorder. At the 6-month follow-up, he did not meet criteria for any of the five emotional disorders.
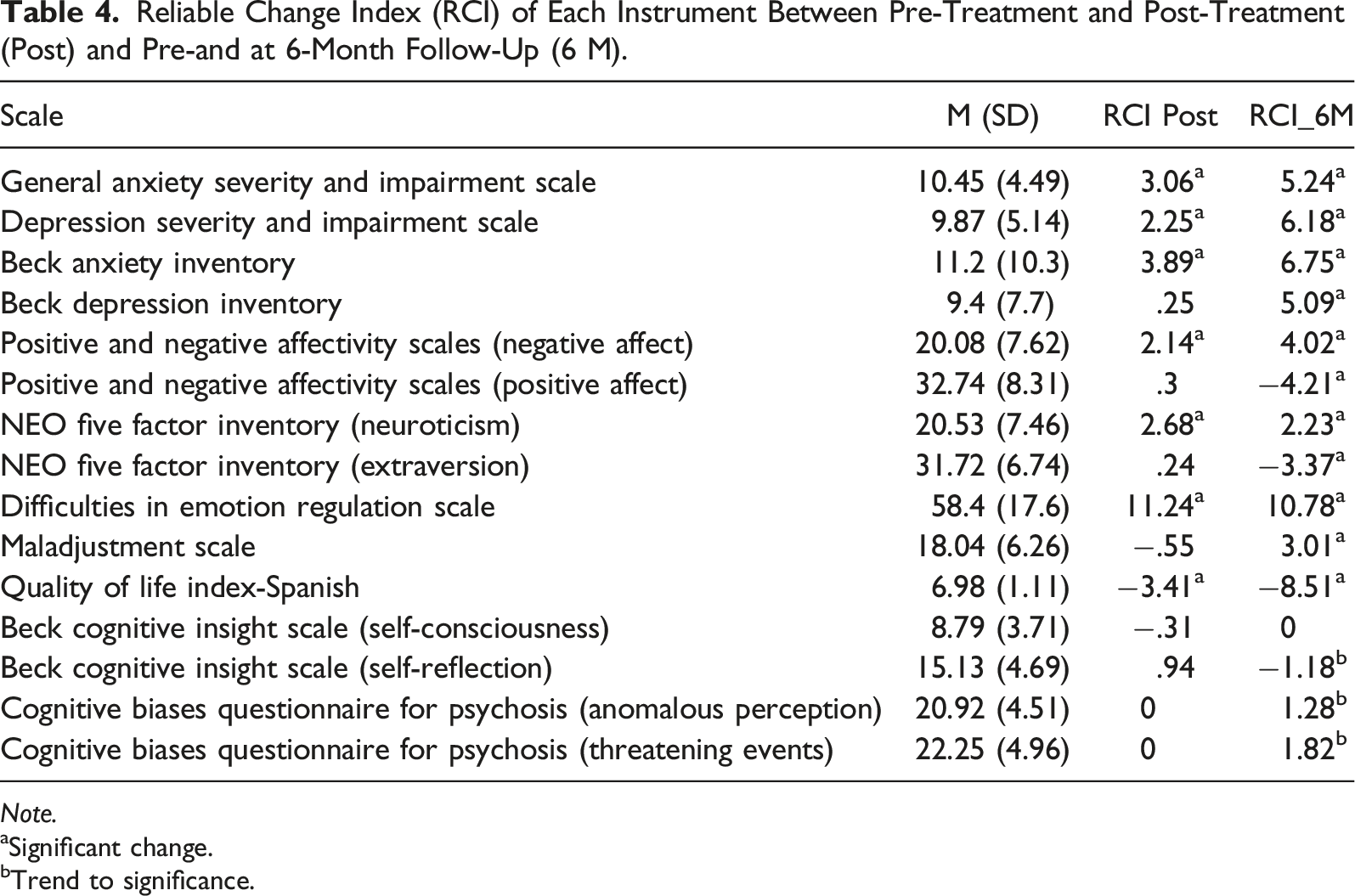
Reliable Change Index (RCI) of Each Instrument Between Pre-Treatment and Post-Treatment (Post) and Pre-and at 6-Month Follow-Up (6 M).
Note.
aSignificant change.
bTrend to significance.
In the first place, the improvement in anxious and depressive symptoms and their interference in daily life, measured with the OASIS and the ODSIS, was significant, both post-treatment and at 6 months of follow-up. We also found a significant improvement in anxiety and depression measured with the BAI and the BDI-II at 6 months. Depression improved more slowly, since in the post-test the change was not yet significant, while anxiety was significant. Regarding the PANAS, there was a significant reduction in negative emotions in the post-test, and this was even greater at the 6-month follow-up. There was also an increase in positive emotions, which reached significant values at the 6-month follow-up. Neuroticism and extraversion measured with the NEO-FFI also improved significantly at the 6-month follow-up. In the case of neuroticism, the improvement was already observed in the post-test. DERS scores decreased significantly, both at post-treatment and at 6 months of follow-up. Maladjustment also decreased significantly at the 6-month follow-up. The quality of life increased significantly in the post-treatment evaluation, reaching the highest values at 6 months.
The ODSIS and OASIS scales were also administered during treatment sessions. In Figure 1 we provide a graph with the scores for both throughout the treatment sessions, as well as in the two follow-up evaluations. Anxiety remained at high levels at the beginning, with peaks in an ascending and descending direction, coinciding with environmental stressors (family visits, compulsory departures from home). From session 15 on, anxiety began to decrease in a stable and significant manner (3 out of 20) until reaching scores below the cut-off point established for the Spanish clinical population with a diagnosis of emotional disorder of 10 points. This reduction coincided with the onset of emotional exposures. Depressive symptoms decreased more slowly, and a peak was also recorded between sessions 12 and 14. Subsequently, it began to decline, reaching scores of four points out of a maximum of 20, also below 10 points. At 3 and 6 months of follow-up, both anxiety and depression scores continued to be very low, always below the cut-off points for the clinical population. These decreases in anxiety and depression occurred when all the emotional regulation techniques had been worked on and Frank began to make the exposures. ODSIS and OASIS results throughout the 15 UP sessions, post-treatment, and at three- and 6-month follow-up.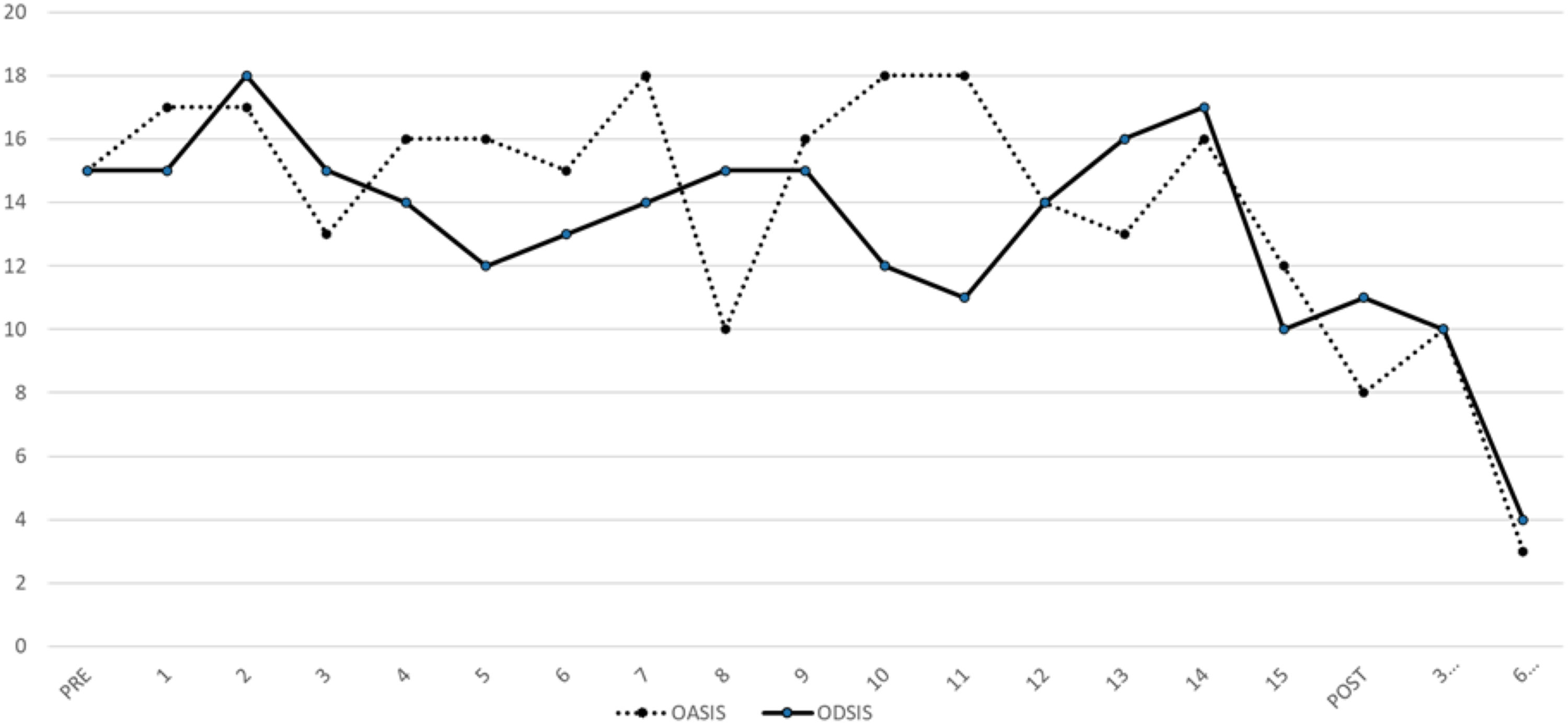
Regarding the specific instruments for psychosis, there was a reduction in the cognitive biases measured with the CBQp at the 6-month evaluation for the PA and TE dimensions, although it was not significant. The results of the BCIS SR scale—that is, the ability to reflect on one’s own thoughts—improved with a trend towards significance at the 6-month follow-up. In contrast, in the SC scale there were no significant changes either in the post-test or in the follow-up.
About halfway through the UP-group sessions, Frank stopped all medication on his own initiative and only told the team after 3 months. After discussing this with his psychiatrist, they decided not to reintroduce it for the moment, since the improvement was significant and had been maintained up to that time. Now, after more than 6 months without taking medication, Frank continues to improve. The physical exercise he did daily had a positive impact on his health, since he began to lose weight (20 kg), was eating better, and was sleeping better as well. Frank did not binge eat again. He valued his participation in the UP group very positively according to the scores on the Satisfaction Scale. The arithmetic mean of the scores was 10 points. The techniques he found most helpful were ARCS and mindfulness. The technique used the least was interoceptive exposure. In this case, it should be noted that the online format facilitated Frank’s decision to participate in the study, since the anxiety caused by interaction with unknown people was very high. Nevertheless, in his final assessment, he answered that he would have liked to do the group work in a face-to-face format.
7 Complicating Factors
We know that there are numerous environmental factors that can act as vulnerability factors for developing psychosis in people with UHR (Fusar-Poli et al., 2017). In the case of Frank, we identified a family history of mental illness, the traumatic experiences of witnessing the death of his father and being bullied, and difficulties in social relationships, as well as school and work problems. Furthermore, Frank had a history of several depressive episodes and had a comorbid depressive disorder at baseline, which added complexity to our case, as comorbid depressive symptoms have been shown to be associated with poor outcomes in UHR patients (Polari et al., 2018).
The stage model in psychiatry states that initially mental health problems manifest from non-specific symptoms to the evolution of more specific syndromes (McGorry et al., 2014). This does not lessen the difficulty when it comes to carrying out a comprehensive intervention to improve all the symptoms, social functioning, and employment, and to prevent chronification and development of a serious mental disorder in the future.
In Frank’s case, there was also a health problem, morbid obesity, which had a negative impact on his self-esteem and social relationships, and which also conditioned the type of activities he could carry out.
8 Access and Barriers to Care
The main barrier we found in Frank’s case was the difficulty in attending sessions due to the anxiety caused by self-referential experiences. If he managed to attend face-to-face sessions at the center, he could hardly stay for 5–10 minutes because his anxiety was so high that he could not stand it. The care team discussed Frank’s case and decided to initially conduct the visits by video conference with the entire therapeutic team to test whether the problem could be solved. Frank’s anxiety gradually decreased as he began to complete sessions in the online format from home. Medication could be adjusted and some of the initial psychotherapeutic work could be done, especially building engagement. Later, when UP group therapy began, Frank had already become more accustomed to the online format of the sessions and we believe this contributed to his adherence to the intervention. The fact that the UP intervention was in a group was also an obstacle, as Frank experienced a lot of anxiety when he was in a social setting, especially with more than two people. The online format of the group intervention contributed to the anxiety’s not being quite so intense. Thanks to this, and to the fact that he could choose whether or not to activate the camera and even intervene using the chat rather than audio, he was able to participate in the group sessions and expose himself to discomfort. At the end of the intervention, Frank was integrated with the rest of the group and came to express his desire to meet his colleagues in person. According to recent studies, online psychotherapy has an efficacy comparable to face-to-face therapy (Andersson et al., 2013) and is highly acceptable for patients with psychotic spectrum disorder (Santesteban-Echarri et al., 2020).
9 Follow-Up
Frank had maintained the clinical improvement at 6 months after finishing the intervention with the UP. Subsequently, he continued treatment in our Program for Early Intervention in Psychosis (PIPPEP) and had biweekly psychotherapy visits. In these, the emotional regulation techniques worked on in the UP sessions were reinforced, and the progression of emotional exposures was worked on together. New medium-term objectives were also set, such as starting a new leisure activity and going back to work. Regarding subthreshold psychotic symptoms, there was no transition to psychosis at 6 months of follow-up nor in the following months. In fact, the attenuated psychotic symptoms improved significantly, reaching the point where they did not meet the UHR criteria. In some specific situation he might experience symptoms of anxiety, but this was mild, and he was able to handle it without difficulty. He felt that his self-esteem was increasing, as well as his assertive behaviors and his desire to establish friendships with other people. He went to the gym, socialized with the people he met there, and picked up his hobbies again. He even began to go out in groups on outdoor excursions and spend the day outside. At the time he was referred to our unit and during the first weeks of treatment, Frank went to the hospital emergency unit when he had symptoms of very intense anxiety, but now he has no need to do so anymore. At follow-up, Frank also no longer met criteria for a social anxiety disorder. In Frank’s case, as with the UHR population, ongoing long-term monitoring is paramount to ensure that symptoms continue to improve and do not worsen. In addition, as part of our early intervention program for psychosis, we have a mobile phone number that patients can use to communicate with the team if they notice any warning signs. We have also worked on a relapse prevention plan so that Frank can recognize his early warning signs and avoid future relapses.
Furthermore, he has not needed to take more psychotropic drugs since he stopped taking the medication. He managed to lose 20 kg of weight and continued to follow a diet monitored by a nutritionist. He did not binge eat again. Obesity is a cardiovascular risk factor that in recent years has been pointed out as a highly relevant aspect in the treatment of people with psychotic spectrum disorders (Mitchell et al., 2013). Frank’s family also greatly appreciated Frank’s improvement. They reported that they saw him happier and more expressive and that he often left the house to do his activities. They said Frank had become “his former self”.
Treatment Implications of the Case
In the case of Frank, we think that the clinical improvement occurred as a consequence of the treatment carried out with the UP. Although the initial CBT sessions helped to normalize the psychotic experiences he was having and allowed him to better understand them, it was not until he underwent the UP treatment that significant changes began to be observed at a clinical and functional level. The baseline evaluation was made just before the beginning of the UP therapy.
Transdiagnostic interventions make it possible to bring together patients with different pathologies in the same group. We think this approach is highly recommendable for treating young people with subthreshold psychotic symptoms, given the low-stigmatizing and highly practical nature of UP. In this intervention, the main objective is to improve emotional regulation, regardless of the diagnosis. Recent studies have begun to highlight the role of emotional dysregulation as a vulnerability factor within the continuum of psychosis (Chapman et al., 2019). The results obtained in this case indicate that the UP is an easily acceptable treatment and of great clinical utility. At the 6-month follow-up, Frank no longer met criteria for any of the emotional disorders he presented at baseline, nor did he meet the UHR criteria for psychosis. One of the most interesting results of this case is the changes observed in temperament measured with the NEO-FFI after the intervention. In the case of neuroticism, previous studies have already shown an improvement in patients who received treatment with the UP (Sauer-Zavala et al., 2021). This has an important impact on the improvement of the anxiety symptoms presented by patients with emotional disorders (Barlow et al., 2021; Osma, Peris-Baquero, et al., 2021). In our case, the increase in extraversion could be explained by the group format of the intervention. These changes translate into a reduction in depressive symptoms. Furthermore, it has been shown that there is an inverse correlation between extraversion and social anxiety (Watson & Naragon-Gainey, 2010). According to the article validating the PANAS in a Spanish sample, a correlation was found between low PANAS-P and high depression (Díaz-García et al., 2020). In the case that we present, we also found an increase in positive affect measured with the PANAS after the intervention, which also coincides with a decrease in depressive symptoms. The difficulties observed during cognitive flexibility training could be explained by deficits in executive functions involved in cognitive flexibility tasks which are already observed in the UHR symptom phase (Bora & Murray, 2014).
10 Recommendations to Clinicians and Students
Although there are studies that demonstrate the efficacy of CBT in psychosis, there is still a belief that these types of symptoms (whether subthreshold or frank psychosis) can only be treated with psychotropic drugs. Especially in the public health system, patients with psychotic symptoms are offered few evidence-based psychological interventions despite the fact that these have been shown to be effective in both psychosis (van der Gaag, Smit, et al., 2013) and in emotional disorder (Sakiris & Berle, 2019). The main objective of our research is to study the efficacy of the UP in the emotional comorbid symptoms of UHR patients. Still, the results obtained in this case raise the possibility that they may also be effective for subthreshold symptoms of psychosis. Given that mental illnesses in young people debut with a conglomerate of non-specific symptoms, varied and with different levels of intensity (McGorry et al., 2018), we believe that transdiagnostic treatments can help to treat this variety of symptoms while equipping young people with long-term strategies to deal with future difficulties. For this reason, we believe that UP therapy in a group format could benefit young people who present symptoms of this type in the public health system in a cost-effective manner (Osma, Martínez-García, et al., 2021).
Footnotes
Acknowledgments
We would like to acknowledge Frank, who agreed to participate in this trial and in this study in order to help other people to improve in the same way that he has. We also thank Parc Sanitari Sant Joan de Déu and Sant Joan de Déu Foundation for encouraging research and facilitating the means and providing funding to carry out this research.
Declaration of Conflicting Interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed by a grant from Parc Sanitari Sant Joan de Déu [AR202003] and by the program SGR-Cat 2021, Agència de Gestió D’ajuts Universitaris i de Recerca (AGAUR) through the grant 2021 SGR 01380. Jorge Osma has received funding from Gobierno de Aragón (Departamento de Ciencia, Universidad y Sociedad del Conocimiento) al grupo S31_23R. This work was funded by Govierno De Aragon. Feder 2014–2020 under grant S31_20D.
Ethical Approval
This study was evaluated and approved by the Drug Research Ethics Committee (CEIm) of Parc Sanitari Sant Joan de Déu. All participants were provided with an information sheet explaining the objectives and procedure of the study as well as the confidentiality of the data collected. All participants were asked for their consent in writing in accordance with the Declaration of Helsinki (WMA, 2013) and Law 14/2007 on Biomedical Research. Our research was registered as a controlled trial at ClinicalTrials.gov (NCT04929938).