
Abstract
Autism spectrum disorder (ASD) frequently presents alongside emotional disorders (e.g., anxiety, depression) in youth. Existing treatments for youth with ASD most often focus on social communication, behavior management, and daily living skills, with generally less focus placed on emotional symptoms. This paper describes the theoretical rationale for and application of the Unified Protocol for Transdiagnostic Treatment for Emotional Disorders in Adolescents (UP-A) to youth with ASD. A case example is presented to highlight adaptations to the UP-A and illustrate the impact of these adaptations on treatment engagement, process, and outcomes. The case reviewed in this study features an adolescent male presenting with generalized anxiety disorder and persistent depressive disorder with a current major depressive episode. His comorbid ASD informed the adaptations to the UP-A that are discussed throughout. Considerations for case conceptualization, treatment planning, and progress monitoring during UP-A treatment are also reviewed.
Keywords
Theoretical and Research Basis for Treatment
Autism spectrum disorder (ASD) is a neurodevelopmental and psychiatric condition generally characterized by difficulties with social interactions and communication, restricted and repetitive behaviors, and sensory sensitivities, although symptoms vary widely between individuals and across development (Hodis et al., 2025). Once thought to be relatively rare, ASD and related disorders have been increasing in prevalence steadily over the last few decades. According to the most recent data from the Center for Disease Control and Prevention (CDC), approximately one in 31 children aged eight years and older have ASD (CDC, 2022). Several evidence-based interventions have been developed to support autistic youth (Hume et al., 2021). Evidence-based interventions for ASD generally aim to enhance social awareness and communication, promote adaptive skills (e.g., activities of daily living), and/or teach parents effective behavior management strategies (Du et al., 2017). While such interventions exhibit efficacy in improving certain symptom domains of ASD, there is a continued interest in expanding the range of treatment options available for autistic youth, particularly those who present with psychiatric comorbidity who may benefit from other existent evidence-based approaches.
There are markedly high rates of psychiatric comorbidity among autistic youth (Romero et al., 2016). Autistic youth commonly present with other co-occurring neurodevelopmental disorders such as attention deficit hyperactivity disorder (ADHD; Domenico et al., 2025) and tic disorders (Kalyva et al., 2016). Moreover, autistic youth also commonly present with co-occurring emotional disorders such as anxiety disorders, depressive disorders, and obsessive-compulsive disorder (Kerns et al., 2021), as well as co-occurring behavior disorders (e.g., oppositional defiant disorder; Fuca, 2023). Importantly, comorbidity between ASD and other neurodevelopmental, emotional, and behavior disorders is not just an artifact of overlapping diagnostic criteria. Rather, comorbidity may be explained by shared genetic predispositions (Morimoto et al., 2021) as well as other shared difficulties in emotional and behavioral regulation that serve to increase risk for and maintain multiple disorders in parallel or in sequence (Astenvald et al., 2022).
The Unified Protocol for Transdiagnostic Treatment of Emotional Disorders in Adolescents (UP-A; Ehrenreich-May et al., 2017) is a transdiagnostic cognitive-behavioral intervention designed to target the shared dysfunctions in emotion regulation processes that underpin a range of emotion-related disorders (e.g., anxiety, depression). The UP-A incorporates a range of cognitive-behavioral strategies including emotion psychoeducation, behavioral activation, cognitive restructuring, mindfulness, and exposure. An adapted version of the UP-A additionally includes content to aid irritability, anger, and frustration-related symptoms (Grossman & Ehrenreich-May, 2019; Hawks et al., 2020). The UP-A content is modular such that clinicians can determine the optimal order and pacing of various components based on the client’s presenting symptoms. The UP-A is designed to be delivered in approximately 15 to 16 sessions, but treatment length can vary depending on clinical need and rate of treatment response.
The UP-A has been investigated in multiple empirical studies with adolescents (e.g., Ehrenreich et al., 2009; Ehrenreich-May et al., 2017; Ehrenreich-May et al., 2025; Garcia-Lopez et al., 2024; Maleki et al., 2021) and is recognized as an evidence-based intervention with demonstrated efficacy and effectiveness for youth anxiety and depression. Recently, researchers have begun to investigate the efficacy of the UP-A for a range of other psychiatric conditions, including post-traumatic stress disorder (O'Donnell, 2021; Mohajerin et al., 2023), feeding and eating disorders (Thompson-Brenner et al., 2021), misophonia (Tonarely-Busto et al., 2023), obsessive-compulsive disorder (Milgram et al., 2025), and borderline personality disorder (Lopez et al., 2014). Still, no studies thus far have examined the application of the UP-A specifically to autistic youth.
Although the UP-A has demonstrated efficacy across a range of emotional disorders in adolescents, there is limited guidance on how to adapt this treatment for autistic youth. Given the distinct developmental, cognitive, and sensory profiles of autistic youth, modifications to the standard treatment protocol may be necessary to enhance accessibility, engagement, and therapeutic outcomes. Identifying specific adaptations for autistic youth is critical to ensure that interventions like the UP-A are both effective and responsive to the needs of this population. This case study reviews the overarching components and goals of the UP-A and provides preliminary insight into how targeted adaptations can be integrated into the treatment to support youth with ASD, thereby addressing an important gap in the literature.
Case Introduction
Jake, a pseudonym, is a 17-year-old biracial Latino male who received treatment from a university-based specialty research and training clinic. Jake is an only child and lives with his mother and father. Jake was diagnosed with Level 1 autism spectrum disorder (ASD) at three years old based on the results of a psychoeducational evaluation including the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2; Lord et al., 2012) conducted within an autism assessment clinic. Jake demonstrates core features of ASD including cognitive rigidity, distress with change in routine, ritualistic routines (e.g., clearing his entire desk before sitting down at it), difficulties understanding social cues, and deficits in social interactions. His special interests include drawing and digital art, areas in which he demonstrates deep knowledge and reportedly often spends extended periods of time engaged.
Presenting Complaints
At the time of the intake for UP-A treatment, Jake and his parents reported persistent worries about the future and about making mistakes in social situations. In response to these worries, Jake reported frequent rumination. In addition to feelings of anxiety, Jake reported persistent low mood and irritability. At intake, Jake was experiencing feelings of isolation and difficulty concentrating. Jake and his parents reported that he was engaging in significant withdrawal and avoidance behaviors. Jake and his parents also reported excessive masking of ASD symptoms, leading to feelings of burnout. These symptoms had reportedly been present for several years but had intensified within the past two years due to increased academic demands and social expectations.
History
At intake, Jake was a senior at a public high school. Although he was reportedly doing well in school academically, Jake's teachers did not consistently implement the accommodations outlined in his Individual Education Plan (IEP). Jake had not previously received treatment to address emotional concerns, but Jake had participated in three different social skills groups in the past. These groups focused on basic social interaction strategies. Jake and his mother reported that these groups were not fully effective to address his needs. Jake reportedly experienced difficulty relating to peers with higher levels of ASD, limiting his engagement, and his mother reported challenges in finding social skills groups tailored to fit the needs of youth with Level 1 ASD, contributing to Jake’s feelings of social isolation.
Assessment
Prior to the start of UP-A treatment, Jake and his parents were administered various diagnostic tools and symptom measures.
Diagnostic Interview
To assess symptoms of a wide range of psychiatric disorders, Jake and his parents were administered the Diagnostic Interview for Anxiety, Mood and Obsessive-Compulsive Disorder and Related Neuropsychiatric Disorders: Child and Adolescent Version (DIAMOND-KID; Tolin et al., 2022), The DIAMOND-KID is a two-hour semi-structured diagnostic interview used to assess diagnostic criteria in correspondence with the Diagnostic and Statistical Manual of Mental Disorders (5th ed; DSM-5; American Psychiatric Association, 2013). The DIAMOND-KID may be administered to the child alone or together with a parent or guardian. Each section of the assessment provides guidance indicating the most reliable source of information relevant to the disorder. The DIAMOND-KID has demonstrated very good test-retest reliability and convergent validity with other measures of anxiety, depressive, and obsessive-compulsive related disorders based on DSM-5 field trials (Tolin et al., 2023). The DIAMOND-KID instructs assessors to assign Clinical Severity Ratings (CSR) for each diagnosis, with scores ranging from 1 (no distress or impairment) to 7 (extreme distress or impairment). Scores greater than or equal to 3 indicate clinical levels of disorder-specific impairment. Jake’s interview was administered by a DIAMOND-KID-trained clinician, whose reliability was supported by previously matching on diagnosis and severity scores on two training cases with an already trained clinician. Following the interview, Jake was assigned diagnoses that are discussed in detail in the Case Conceptualization section below.
Jake’s Clinical Global Impression-Severity and Improvement (CGI-S and CGI-I, respectively; Guy, 1976) was assessed by his interviewer. The CGI-S and CGI-I are psychometrically validated measures of overall psychiatric symptom severity and improvement throughout the treatment course. CGI-S scores range from 1 (normal, not ill at all) to 7 (extremely ill), and CGI-I scores range from 1 (very much improved) to 7 (very much worse).
Standardized (Nomothetic) Measures of Treatment Progress
The Strength and Difficulties Questionnaire (SDQ; Goodman et al., 1998) was administered to Jake and his mother at pre-, mid-, and post-treatment to assess emotional and behavioral difficulties. The SDQ is a 25-item, child- and parent-report measure of five different subscales: emotional problems, conduct problems, hyperactivity/inattention, peer relationship problems, and prosocial behaviors. Each subscale is scored from 0 to 10. A raw total difficulty score is calculated on a scale ranging from 0 to 40 and interpreted using cutoff values, with scores between 14 and 16 indicating borderline levels of emotional and behavioral difficulties and scores of 17 or higher reflecting clinically significant concerns (Goodman et al., 1998).
The Difficulty in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004) was administered to Jake’s mother at pre- and post-treatment to assess her perception of Jake’s ability to understand and manage his emotional responses. The DERS is a 36-item measure of difficulties in emotion regulation. The DERS measures six subscales of emotion regulation: non-acceptance of emotional responses, goals, impulse control, awareness of own emotions, strategies for emotion regulation, and clarity of own emotions. The DERS subscales have exhibited strong internal consistency in previous studies (Hallion et al., 2018). Total scores on the DERS range from 36 to 180, with higher scores indicating greater difficulty in emotion regulation (Gratz and Roemer, 2004). Subscale scores range as follows: Non-acceptance = 6–30, Goals = 5–25, Impulse = 6–30, Awareness = 6–30, Strategies = 8–40, and Clarity = 6–30.
Patient-Centered (Idiographic) Measure of Treatment Progress
Jake’s Top Problem Ratings: Pre-vs Post-Treatment

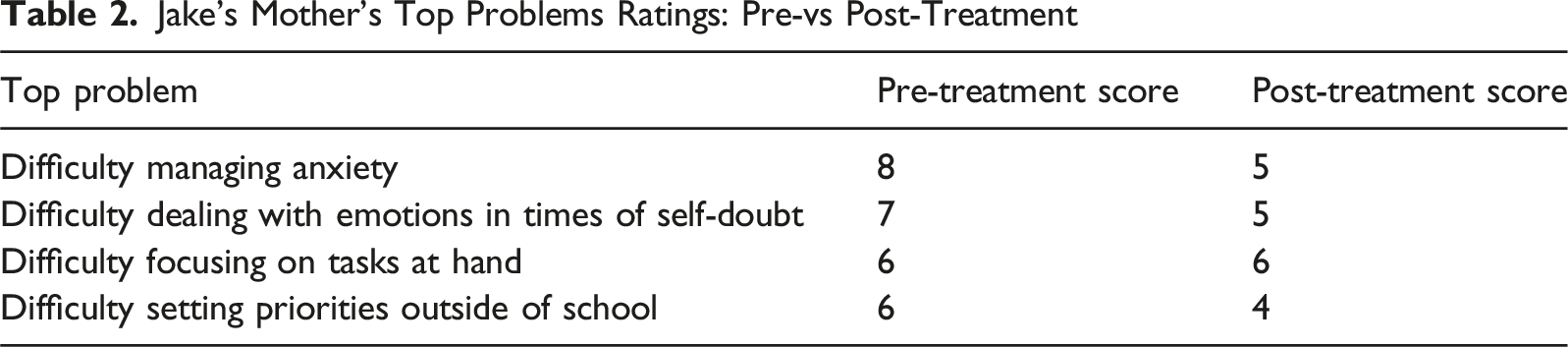
Jake’s Mother’s Top Problems Ratings: Pre-vs Post-Treatment
Case Conceptualization
Based on information obtained through the DIAMOND-KID diagnostic interview, the following diagnoses were assigned to reflect Jake’s symptom presentation and associated impairment.
Persistent Depressive Disorder
Jake reported feeling isolated and loss of interest in engaging with others and in activities. As a result, Jake reported that, when not at school, he withdrew and spent the majority of his time lying in bed. Jake described difficulties concentrating, largely due to ongoing feelings of hopelessness and worthlessness, which led to significant feelings of frustration. Both Jake and his mother reported consistency of these symptoms over the past year. To account for his persistent low mood and feelings of sadness, Jake was diagnosed with persistent depressive disorder (F34.1). Additionally, at the time of the intake, Jake reported a notable decrease in his mood over the past couple of weeks, describing it as worse than he has felt during the past year. To capture this, Jake was diagnosed with a current major depressive episode. Jake and his mother indicated these symptoms have caused significant functional impairment at home and in school. Given the level of distress and impairment, persistent depressive disorder, with current major depressive episode diagnosis, was given a CSR rating of 5.
Generalized Anxiety Disorder
In addition to the reported feelings of sadness, Jake and his mother reported persistent and excessive worry. Jake and his mother reported these persistent worries have occurred more days than not for at least six months and cover multiple domains. More specifically, Jake reported worries about the future, including job security and life after death. Jake also described frequent worries about making mistakes, saying the wrong thing, and navigating social situations. As a result, Jake avoided social encounters and described a decreased motivation to try to spend time with friends. In response to his frequent worries, Jake reported frequent rumination and inability to distract himself from worry thoughts. Jake reported that his anxiety is often accompanied by somatic symptoms, including stinging and sinking sensations in his chest. Jake also reported increased irritability when anxious. A separate diagnosis of generalized anxiety disorder (F41.1) was assigned to account for Jake’s persistent and excessive worry, with a CSR rating of a 4.
While social worries and feelings of isolation from peers were reported during the initial evaluation, these worries were reportedly mainly attributed to the ASD-related challenges of engaging in social interactions and forming strong connections. Because these social difficulties were considered specific to Jake’s ASD and not excessive given the context of his ASD, he was not given a social anxiety disorder diagnosis.
Autism Spectrum Disorder
While the DIAMOND-KID is not intended to be a diagnostic measure for ASD, Jake was assigned a by-history diagnosis of ASD based on his prior evaluation and diagnosis. Jake reported feeling disconnected with others and uncertainty in how to respond in certain social situations. Both Jake and his mother reported patterns of cognitive rigidity, particularly with academic tasks, as well as a strong preference for a structured routine. In response to disruption of routine, or things not happening as he wishes, Jake reportedly experienced emotional shutdowns. Jake reported learning how to mask his ASD symptoms well, especially in the school setting, emulating his peers. While Jake shared this strategy has been beneficial in navigating certain environments, it has also resulted in significant emotional exhaustion. Despite putting considerable effort into learning and applying proper social skills, he continued to experience frustration in social situations. No CSR was assigned for the ASD diagnosis given that it was assigned by history.
Overall, at the time of the intake, Jake was struggling with persistent feelings of sadness and frequent worries. To escape these emotional experiences, Jake reportedly avoided social interactions, withdrew from activities and interacting with family members, and engaged in excessive worrying and rumination. The behaviors Jake used to suppress his feelings, along with external factors including bullying and increasing academic pressure, maintained his emotional disorder symptoms by contributing to a cycle of avoidance and maladaptive behaviors. For example, Jake learned that isolating himself when he was feeling down was easier than having to engage with people who care about him. Jake reportedly learned that by masking his ASD traits at school, he experienced less anxiety and less perceived judgment from others. However, over time, masking his ASD symptoms became a coping strategy that, while reducing social discomfort in the moment, contributed to ongoing emotional exhaustion and burnout.
Course of Treatment and Assessment Progress
Treatment
Treatment was delivered within a university research and training clinic by a graduate student therapist completing a master’s-level clinical practicum at the time of the study. Prior to treating the case discussed in this study, the therapist completed an eight-hour video-recorded training delivered by the first author of the Unified Protocols for Transdiagnostic Treatment of Emotional Disorders in Children and Adolescents (UP-C/A). Then, the therapist participated in a 12 week-long clinical ‘role play’ group to practice UP-C/A delivery with a certified UP-C/A supervisor. This case and all of the therapist’s active cases were supervised by a UP-C/A certified licensed clinical psychologist. Supervision consisted of weekly meetings with video tape review to ensure UP-C/A treatment fidelity.
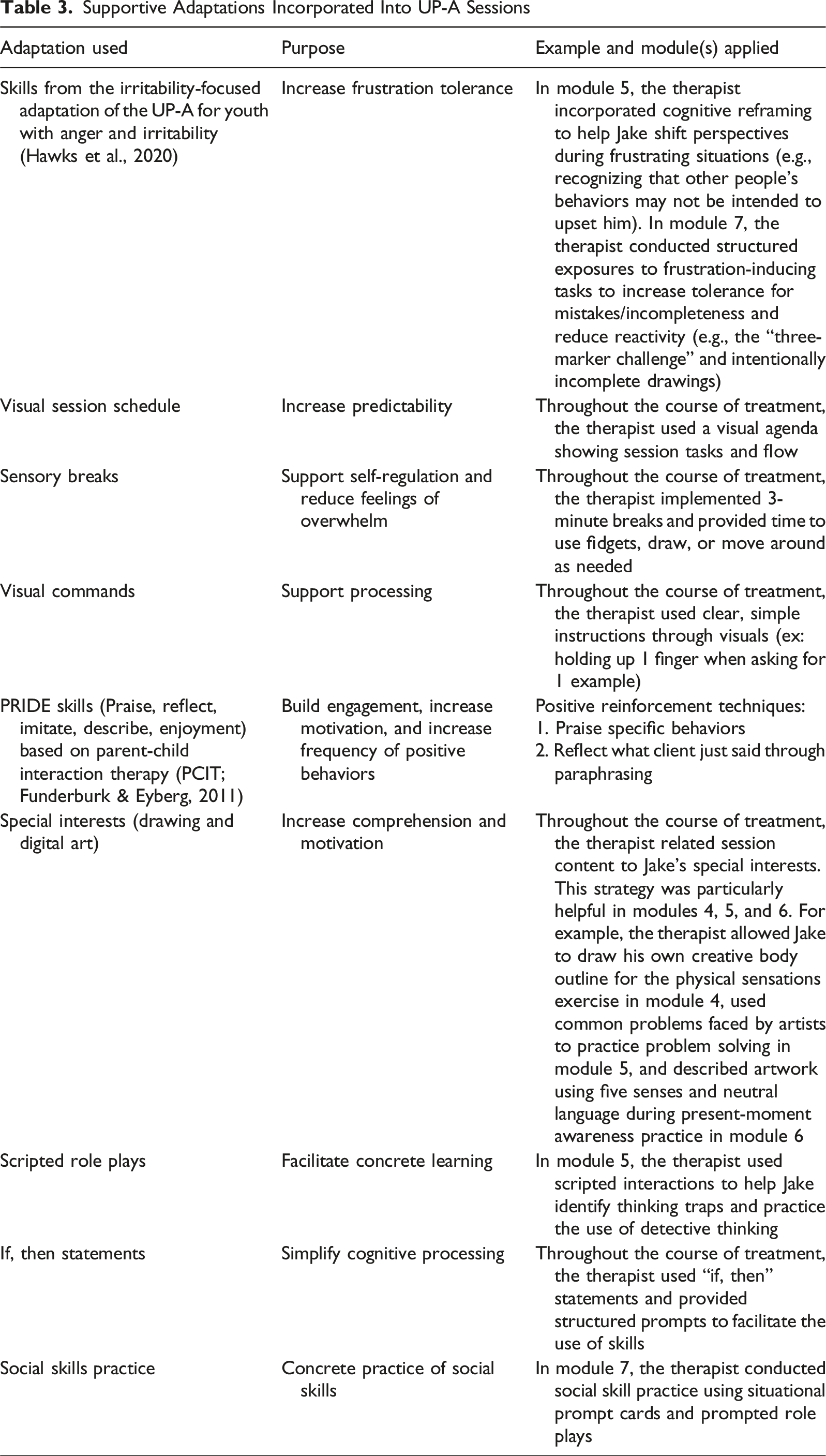
Supportive Adaptations Incorporated Into UP-A Sessions
Module 1: Building and Keeping Motivation
The goals of the first module of the UP-A include explaining the basic treatment concepts and structure of the UP-A and identifying goals for treatment. In the first module, the therapist addresses the family’s motivation for change. As mentioned earlier, top problems are identified from both parent and child during the first session. Jake’s top problems included: (a) difficulty managing anxiety (rating: 7/8), internalizing emotions (rating: 5/8), and difficulty responding to situations when overwhelmed/irritated (rating: 8/8). His mother’s top problems were as follows: difficulty managing anxiety (rating: 8/8) difficulty dealing with emotions in times of self-doubt (rating: 7/8), difficulty focusing on tasks at hand (rating: 6/8), and difficulty setting priorities outside of school (rating: 6/8). Jake and his parents displayed enthusiasm for beginning treatment and reported high motivation. To help maintain this motivation throughout treatment, the therapist intentionally incorporated Jake’s special interests in drawing and digital art into session activities throughout treatment.
Module 2: Getting to Know Your Emotions and Behaviors
In module 2, the therapist focused on increasing psychoeducation on emotions including their purpose, function, and impact on behavior. The therapist introduced the concept of a trigger (the thing that causes the emotion) and the three parts of the emotional experience (e.g., thoughts, physical feelings, and behaviors). After practice with made-up examples, Jake worked with his therapist to break down his own personal emotions into these different parts (e.g., Jake was feeling anxious to talk to his art teacher about bullying he was experiencing in the classroom that is interfering with his work). The therapist then introduced the before (trigger), during (thoughts, physical feelings, behaviors) and after (short-term and long-term consequences of emotional behaviors) framework (BDA) to track emotional experiences. While the BDA framework itself is designed to be concrete and structured, the integration of thoughts, feelings and behaviors can still feel abstract and challenging, especially for autistic youth. To support Jake’s understanding, extra time was spent on practice examples, specifically using very concrete examples. This was followed by Jake generating examples involving other people before applying the framework to his own experiences. This approach was used to reduce emotional intensity, support concrete thinking, and promote development of emotional insight. At the end of the session, Jake was instructed to continue practicing breaking down his emotional experiences using the BDA over the next week.
Module 3: Introduction to Emotion-Focused Behavioral Experiments
The goal of this module is to help adolescents understand how they can use opposite actions to break the cycle of avoidance and reduce the reinforcement of maladaptive emotional behaviors. In the UP-A, opposite action refers to the practice of intentionally engaging in a behavior different from, or opposite to, the behavior the emotion is urging the individual to engage in. For Jake, learning about opposite actions to address patterns of avoidance, withdrawal, and internalization were particularly helpful. One of the first opposite actions Jake practiced was writing down emotions instead of suppressing them, which eventually progressed to verbalizing them to his mother. Other opposite actions Jake engaged in throughout the course of treatment included initiating brief conversations with peers, doing something enjoyable when feeling like withdrawing, and taking small steps to advocate for himself in the classroom. While opposite actions are formally introduced and discussed in module 3, they are consistently revisited, adapted, and assigned as home-learning assignments for each session. Following the introduction and discussion of opposite actions, Jake’s therapist introduced the concept of behavioral activation as a form of opposite action. Jake learned about the connection between emotions and behaviors. Jake was instructed to track his emotion and activities level daily and encouraged to engage in enjoyable activities when feeling down as an emotion-focused behavioral experiment. Jake demonstrated difficulty identifying enjoyable activities outside of his special interests (e.g., drawing, digital art). This module was very important for Jake as it targeted behaviors contributing to the maintenance of his emotional disorders.
Module 4: Awareness of Physical Sensations
In module 4, the therapist introduced the concept of physical sensations and their relationship to strong emotions. Jake learned the function of these physical sensations during an emotional experience and practiced identifying where on his body he experienced these strong emotions. Jake reported that he often experienced physical sensations when he is feeling anxious, particularly in social situations and when thinking about the future. Jake completed a body drawing exercise in which he identified specific parts of the body where he feels physical sensations during emotional experiences. To increase engagement, the therapist incorporated Jake’s special interest in drawing by having him draw out the body figure before starting the activity instead of using the worksheet provided by the manual. Jake then completed sensational exposures (e.g., shaking his head back and forth, running in place, etc.) and was able to see that these feelings eventually go away on their own. Jake learned how to do a body scan to sit with uncomfortable body feelings, which he responded well to and found helpful. Jake reported that he would like to use this skill when he feels very overwhelmed and irritated. This module was introduced following module five and six to prioritize other treatment targets.
Module 5: Being Flexible in Your Thinking
Module 5 introduces the concept of unhelpful automatic thoughts and interpretations, which the UP-A refers to as thinking traps. For Jake, practicing identifying other people’s thinking traps was helpful in learning to recognize unhelpful thinking patterns of his own. Once Jake demonstrated comfort identifying thinking traps, the therapist introduced a skill called detective thinking. Detective thinking is a strategy designed to help adolescents challenge and reframe their automatic interpretation. For Jake, role-play exercises with therapist prompts were used to practice identifying thinking traps and applying detective thinking. Because cognitive rigidity, a common feature of ASD, makes thinking flexibly more challenging, the prompted role plays offered a structured way for Jake to practice considering multiple possible explanations in a given situation. Additionally, role plays incorporated concepts from the irritability-focused adaptation of the UP-A to specifically address managing irritability and emotional reactivity. This supported Jake in thinking flexibly in situations that evoke frustration. Following thinking traps and detective thinking, module 5 introduces another skill to help adolescents identify more than one possible solution when feeling stuck in a strong emotion. This skill, called problem solving, was introduced to Jake using his special interest, art, and the therapist and Jake worked together on made-up problems related to art in order to practice this skill. Using the special interest allowed Jake to practice generating possible solutions in a familiar context.
Module 6: Awareness of Emotional Experiences
In Module 6, Jake’s therapist introduced the concept of becoming aware of emotional experiences and tuning into what is happening in the “here and now.” The UP-A refers to this skill as present moment awareness (PMA). Jake was taught the five senses exercise as a form of PMA, which involves intentionally noticing and naming a structured number of things he can see, hear, touch, smell, and taste in the present moment. This clear and concrete structure was especially helpful for Jake, as it provided a manageable and predictable framework to focus his attention. For individuals with ASD who struggle with overwhelming sensory input or difficulty shifting attention, having a set number of specific things to identify can make grounding exercises more accessible and effective. Another form of present moment awareness taught to Jake was nonjudgmental awareness. This approach encourages noticing one’s thoughts, feelings, and behaviors without attaching labels like “good” or “bad,” and instead fosters a compassionate, accepting attitude toward one’s experiences. To practice using neutral, descriptive language, the therapist incorporated Jake’s special interest in art. For example, Jake was asked to select a drawing he would typically criticize and instead describe it using neutral, objective language. The therapist first introduced PMA prior to module 3 and then reintroduced it following module 5.
Module 7: Situational Emotion Exposure
Module 7 introduced the rationale for situational exposures aimed at helping Jake increase tolerance for frustrating and anxiety-provoking situations that typically lead to avoidance and parental accommodation. Jake and his therapist worked together to develop an exposure hierarchy, starting with less challenging tasks and progressing to more difficult ones. When generating the hierarchy, Jake was asked to rate his anticipated distress in each situation using a subjective units of distress scale (SUDS) ranging from 0 (no discomfort) to 8 (extreme discomfort). The higher the SUDS rating, the more challenging the exposure was expected to be. Jake’s exposures targeted situations such as making mistakes, dealing with unfinished tasks and uncertainty, transitioning between activities, and social exposures for social worries as well as social situation, including both those tied to social anxiety as well as situations in which he felt uncertain about how to use or recognize appropriate social skills. This gradual and structured approach aimed to reduce avoidance behaviors and increase Jake’s confidence in handling emotionally challenging situations. Throughout each exposure, the therapist collected SUDS ratings to assess Jake’s engagement and response to the exposure. Over the course of exposures, Jake demonstrated habituation, meaning that his anxiety gradually decreased with repeated engagement in certain tasks, particularly those related to perfectionism and feelings of incompleteness.
Jake’s frustration tolerance exposures focused on increasing his flexibility and reducing perfectionistic tendencies in situations involving mistakes or incomplete tasks. For instance, he participated in the “three-marker challenge,” where he closed his eyes to randomly select colors for a drawing (highest SUDS rating = 5), followed by drawing a bird while intentionally leaving off the beak and sharing it with his mother (highest SUDS rating = 6). Additional exposures included purposefully making a mistake in a drawing and leaving it in a visible place (highest SUDS rating = 6) as well as limiting himself to clearing only three items from his desk instead of organizing it completely (highest SUDS rating = 6, later decreasing to 4 with repetition). These activities encouraged Jake to tolerate imperfections, and resist urges toward overcorrection. In parallel, Jake also engaged in social exposures designed to address discomfort in social interactions and uncertainty about social cues. Following role-play exercises, he practiced initiating and maintaining conversations in mildly anxiety-provoking situations (highest SUDS rating = 4). These exposures helped Jake challenge anxious thoughts, build social confidence, and generalize skills practiced during sessions to real-world contexts.
Module 8: Relapse Prevention and Maintaining Gains
Module 8 of the UP-A focuses on maintaining treatment gains and planning for relapse prevention. In this final module, Jake reviewed the core skills learned over the course of treatment, highlighting the ones that have been most useful to him and his presenting concerns. Jake and his therapist reflected on progress in top problems identified during the initial session. Jake identified things he would still like to work on and, with his therapist, created a structured plan for continued at-home practice following the end of treatment. This plan aimed to support maintenance of gains and provide Jake with the tools needed to navigate future challenges.
Module P: Parenting the Emotional Adolescent
Jake’s therapist met with Jake’s mother for 10 to 15 minutes at the end of each session to discuss Jake’s progress at home and review skills learned in session. Module P consists of various parenting skills which are presented throughout the course of treatment as needed. Jake’s therapist placed emphasis on addressing parenting behaviors such as excessive avoidant emotional modeling, criticism, and accommodation. Jake’s mother reported that she often became frustrated with Jake’s behaviors, particularly with irritability and difficulty shifting between tasks, which sometimes led to critical responses or accommodation to avoid escalation. She also noted that Jake’s father engaged in frequent criticism. Discussing opposite parenting behaviors supported Jake’s mother in using more consistent and supportive responses to Jake’s emotional needs.
Assessment Progress
At the time of termination, while at a lower level of severity, Jake was still experiencing worries in multiple days, more days than not. To capture these worries, Jake’s diagnosis of generalized anxiety disorder remained. At the end of treatment, Jake had experienced absent or minimal feelings of sadness for at least two months and was considered in full remission from persistent depressive disorder (dysthymia). At the time of termination, Jake’s autism spectrum disorder (ASD) by history diagnosis remained, reflecting prior clinical assessment. At the time of the intake, Jake received a CGI-S of a 4, indicating moderate symptom severity. Following treatment, Jake’s therapist reassessed symptom criteria and severity based on the DIAMOND-KID criteria. Jake’s CGI-S score at post-treatment was 3, indicating mild symptom severity, and his CGI-I score was 2, indicating much improvement.
Jake’s symptom improvement was highlighted by his and his mother’s reports on the Top Problems Assessment. Jake and his mother reported improvements in Jake’s ability to manage anxiety and related emotional symptoms and identify more helpful responses when feeling strong emotions. See Tables 1 and 2 for Jake’s and Jake’s mother’s scores on the Top Problems Assessment at pre- and post-treatment, and see Figure 1 for change in Top Problems scores across the treatment course. Parent and child reported change in top problem scores over the course of treatment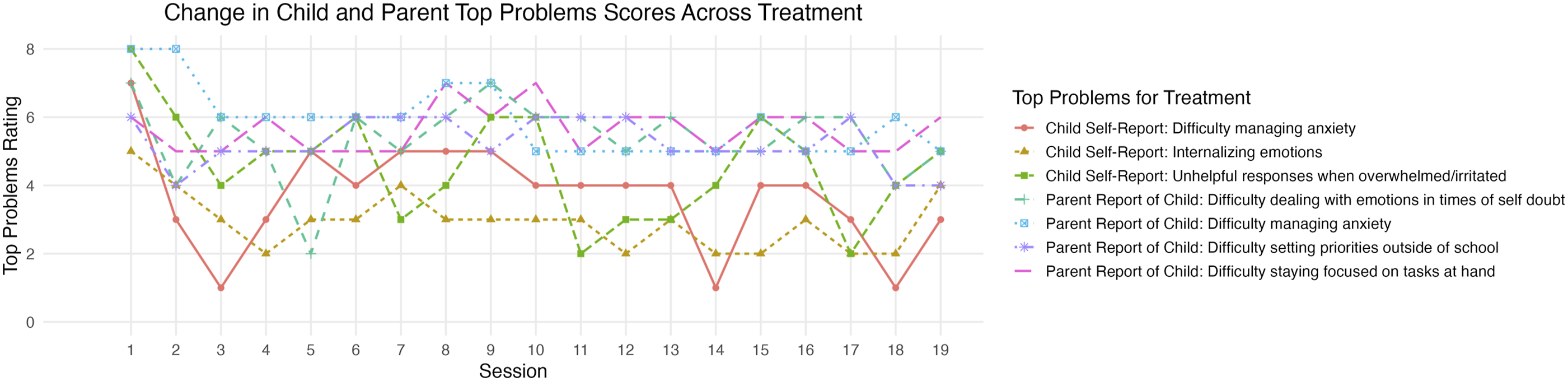
Jake’s mother also noted improvements on standardized assessment measures. At pre-treatment, Jake’s mother reported an SDQ total difficulties score of 26, which fell in the clinically elevated range. Subscale scores were as follows: Emotional Problems = 5, Conduct Problems = 0, Hyperactivity = 5, Peer Relationship Problems = 8, Prosocial Behaviors = 8. At the mid-treatment timepoint, Jake’s mother reported an SDQ total difficulties score of 25. Subscale scores were as follows: Emotional Problems = 6, Conduct Problems = 0, Hyperactivity = 3, Peer Relationship Problems = 8, Prosocial Behaviors = 8. Based on Jake’s mother’s report on the SDQ at post-treatment, the total difficulties score decreased to 19, indicating a notable reduction in reported difficulties, though still falling within the clinically elevated range. Post-treatment subscales were as follows: Emotional Problems = 1, Conduct Problems = 0, Hyperactivity = 3, Peer Relationship Problems = 7, Prosocial Behaviors = 8. These scores reflect reductions in emotional problems and hyperactivity, with peer relationship problems and prosocial behaviors remaining largely unchanged. These observed areas of improvement are consistent with clinical observations. See Figure 2 for change in SDQ scores over the treatment course. Parent reported change in SDQ scores over the course of treatment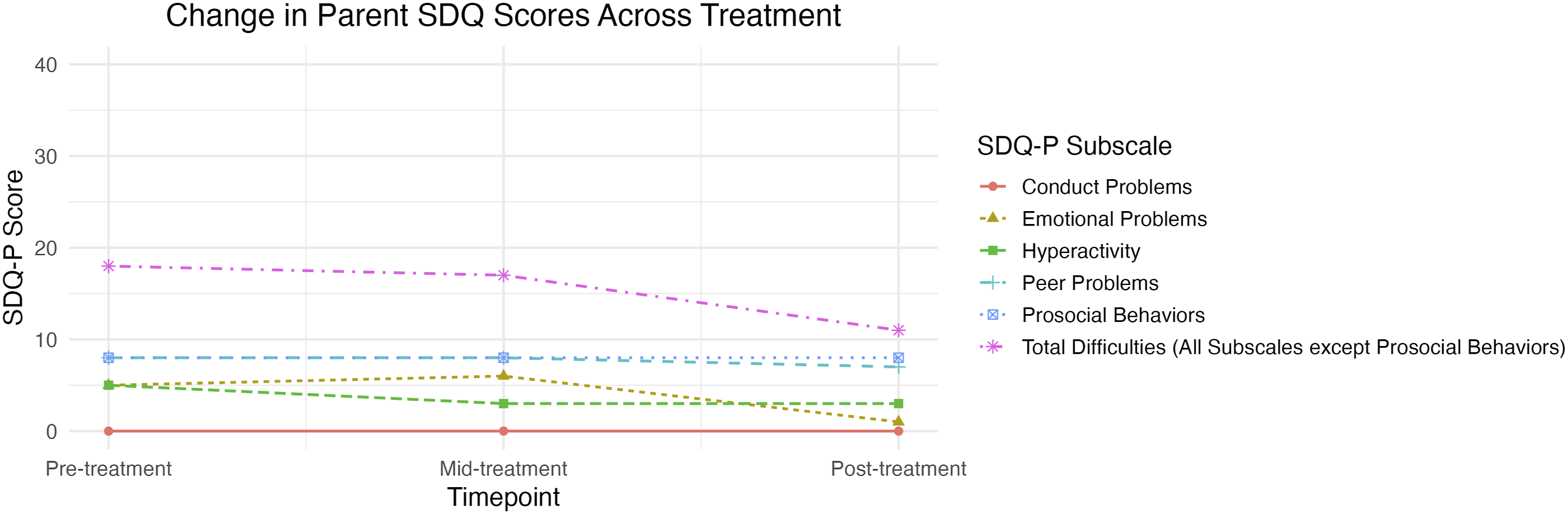
Similarly, Jake’s mother reported improvements in Jake’s emotion regulation skills. At pre-treatment, Jake’s mother reported a total difficulty in emotion regulation (DERS) score of 60, indicating some difficulties. Subscale scores were as follows: Non-acceptance = 10, Goals = 12, Impulse = 9, Awareness = 11, Strategies = 11, and Clarity = 7. At the mid-treatment timepoint, Jake’s mother reported a total DERS score of 66. Subscale scores were as follows: Non-acceptance = 14, Goals = 13, Impulse = 11, Awareness = 8, Strategies = 14, and Clarity = 6. Based on Jake’s mother’s report at post-treatment, Jake demonstrated a notable decrease in overall emotion regulation difficulties. She reported a total difficulty in emotion regulation score of 48. Subscale scores at post-treatment were as follows: Non-acceptance = 6, Goals = 11, Impulse = 6, Awareness = 8, Strategies = 11, Clarity = 6. Based on her report, these scores reflect reductions in non-acceptance of emotions, impulse difficulties, emotional awareness, and emotional clarity, while goal-directed behaviors and emotion regulation strategies remained unchanged. These reported areas of improvement are consistent with clinical observations. However, based on clinical judgement, Jake also demonstrated increased ability to engage in goal-directed behaviors and to use more effective emotion regulation strategies. See Figure 3 for change in DERS scores over the treatment course. Parent reported change in DERS scores over the course of treatment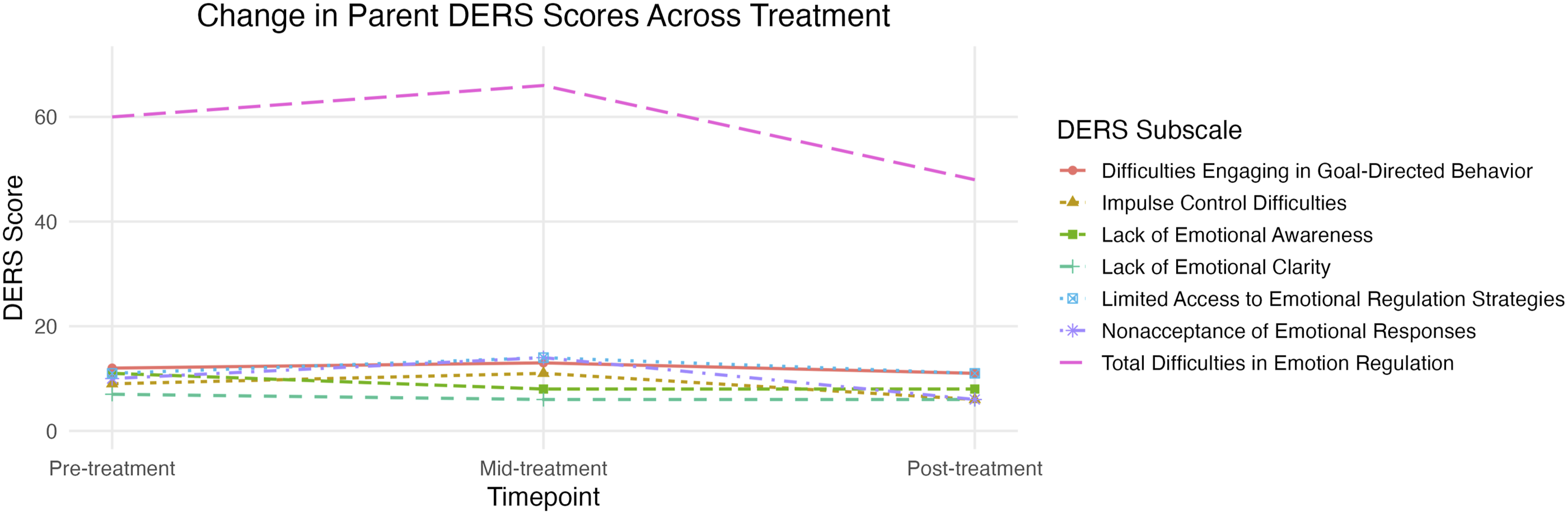
It is important to note that certain SDQ and DERS subscale scores may have been limited by floor effects as baseline scores left minimal room for improvement. Based on clinical observation, it is possible that Jake’s mother was underreporting symptoms, particularly at baseline. This should be considered when interpreting treatment-related changes. Additionally, some of Jake's behaviors may reflect a combination of ASD-related difficulties and symptoms of anxiety and depression, which may further complicate differentiating between these presentations when interpreting treatment-related changes. Additionally, the SDQ and DERS are broad, global measures of symptoms and emotion regulation difficulties, which may limit their sensitivity to more nuanced or context-specific changes observed clinically. While idiographic assessments and global clinical judgement were used to assesses progress over the course of treatment, the lack of weekly standardized assessment data limited the ability to track more fine-grained weekly symptom fluctuations.
Complicating Factors
Some factors added increased need for extra support and slight modifications to how materials were presented. However, it should be noted that these variables did not significantly impact engagement or ability to complete the course of treatment. As previously mentioned, Jake received his UP-A treatment via telehealth. Many of the adaptations used to support ASD-related difficulties had to be tailored for use in a virtual context. For example, reinforcement and rewards systems could not be physically administered by the therapist during the session and rather relied on the mother’s implementation following the session. Social exposures were also slightly more challenging to accomplish full desired effects via telehealth. Additionally, Jake’s history of bullying from peers led to increased rigidity around certain social-related worries and overgeneralization. To address each of these challenges, sessions were paired with guided parent support and structured at-home assignments that encouraged Jake to apply skills in multiple contexts outside of session. Role-playing, video modeling, and repeated practice of cognitive strategies were also used to help transfer skills from virtual sessions to real-world situations.
Access and Barriers to Care
Jake received treatment via telehealth, which enabled him to attend sessions consistently each week and complete his UP-A treatment. Without this option, continuing treatment may have been challenging. Additionally, Jake received treatment through a research and training clinic that offers no cost treatment to families living in Miami-Dade County (Florida, USA). If the program was unable to provide no-cost treatment, Jake may not have had access to evidence-based treatment such as the UP-A.
Follow Up
Following the completion of treatment, Jake was offered two booster sessions to be used within three months following the end of treatment. The family elected not to utilize these sessions as they did not feel additional support was necessary at that time.
Treatment Implications of the Case
Adaptations were necessary to accommodate some of Jake’s ASD-related needs such as cognitive rigidity; however, modifications were limited to the structure and delivery of the UP-A and did not involve any fundamental changes to the therapeutic content. This suggests that the UP-A may be effectively implemented with adolescents with ASD through careful, individualized adaptations, without the need to develop a separate, extensively modified treatment manual.
Recommendations for Clinicians and Students
Considering individual factors that may influence the course of treatment or indicate a need for additional support is critical for effective intervention. This case highlights a broader clinical need for guidance on how to flexibly adapt evidence-based treatments for autistic youth, as many interventions, including the UP-A, were not specifically designed for this population. This case study provides preliminary insight into how structural and content adaptations can enhance engagement and effectiveness for neurodiverse youth. Such considerations can guide treatment planning and delivery by informing when and how to adjust protocols while maintaining treatment fidelity.
A suggestion for future clinicians is to become comfortable with the flexibility of modular evidence-based protocols such as the UP-A. Formal therapist training is required to deliver the intervention; however, with experience, clinicians can learn to deliver content flexibly to patient needs, tailoring modules to the individual’s presenting concerns rather than following a strictly linear sequence. For first-time clinicians, it is recommended to initially follow the modules in order until they are familiar with the material. In Jake’s case, introducing PMA skills earlier in treatment was beneficial for building emotion regulation that supported him through challenges encountered in later modules.
Looking ahead, a key direction for researchers and clinicians is to evaluate which structural adaptations to the UP-A are most effective in improving engagement and treatment outcomes for youth with ASD. Such research could inform strategies to strengthen the UP-A’s capacity to address psychopathology in youth with comorbid ASD without requiring the development of an entirely separate protocol. This continued research and treatment development will increase the availability of effective and tailored options for autistic youth who may benefit from treatment for emotional concerns that extend beyond their ASD-related symptoms.
Footnotes
Ethical Considerations
Informed parental consent and youth assent were collected from the case presented in this paper. All study procedures were conducted within a protocol approved by the University of Miami Institutional Review Board (IRB #20230860, Approved 9/11/2023).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The treatment described in this case study was funded by The Children’s Trust, a social services organization that serves youth in Miami-Dade County, Florida (GR025527).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jill Ehrenreich-May, Ph.D. receives a royalty from the sales of the Unified Protocols for Transdiagnostic Treatment of Emotional Disorders in Children and Adolescents from Oxford University Press. She also has grant funding related to this intervention from the National Institute of Health, Patient Centered Outcomes Research Institute, Institute of Education Sciences, the Children’s Trust, and the Batchelor Foundation. She is also paid for clinical training and implementation support services related to this intervention by a variety of institutions. All other authors report no potential conflicts of interest.
Data Availability Statement
The data for this case study are not available.