
Abstract
Caring for a person with dementia can negatively impact the physical, mental, and social wellbeing of an informal carer. Providing complex and challenging care often results in carer burden, stress, and distress, which can continue even when the care recipient transitions into an aged care facility. This case study aims to demonstrate that optimising carer support, knowledge, skill acquisition, and promotion of wellbeing benefits carers and those they care for across contexts. It provides a weekly account of an informal Australian carer’s experience with the STrAtegies for RelaTives (START) manualised intervention program. The study used reliable change indices, standardised measures, and carer surveys to provide insights into the carer’s experience of the program and outcomes during and after the therapy. The results showed reliable and clinically significant change, demonstrating an improvement in all measures. The carer’s mood symptoms and their perceived burden of care decreased. The carer also reported decreased dementia symptoms in their care recipient. Both the carer and the care recipient experienced increased quality of life. These findings are consistent with recent literature on the feasibility of the START program and are aligned with the National Dementia Plan.
1 Theoretical and Research Basis for Treatment
Informal carers (here referred to as carers) are integral to the dementia care model in Australia. Carers provide practical, emotional, and physical support to an estimated 470,000 people with a diagnosis of dementia, 76% of whom live at home, and 46% depend solely on informal care (Australian Institute of Health and Welfare, 2023). Carers also assume a disproportionate amount of the financial and human costs associated with caring for a person living with dementia (PLWD: The National Centre for Social Economic Modelling, 2017).
Dementia is a progressive neurological disease that damages several areas of an individual’s functioning. These include behavioural, social, and cognitive functions, language, reasoning, judgement, and attention (Kelly & McDonald, 2020). It can also lead to disturbances in perception, thought content, mood, and behaviour, with 97% of PLWD expected to experience some form of behavioural and psychological symptoms of dementia (BPSD: Cloak & Al Khalili, 2021). Dealing with BPSD daily can become a source of burden, stress, and distress for carers and can decrease their quality of life (Hoe et al., 2007), especially where behaviours are viewed as challenging.
Several factors contribute to carer-related stress. Carers endure the emotional impact of managing changed behaviour and behaviours that challenge grief and loss, feeling socially isolated and stigmatised, and underlined by insufficient-support, dementia-specific knowledge, and skills. Carers may also have legal and financial responsibilities (Field & Cartwright, 2016; Schoenmakers et al., 2010). Furthermore, these concerns do not abate when transitioning into an aged care facility (ACF). Transitions to ACF might see a reduction in day-to-day demands on carers. However, while a carer’s role is altered by context, it continues, as does carer-related stress and distress. Indeed, Moore and Dow (2015) found that the level of stress and distress often increases for both carer and PLWD during the transition and for months following.
Caring for a PLWD can be emotionally challenging, especially when the disease progresses and the individual’s behaviour changes. Behaviours that challenge (BtC) refer to the symptoms of distress or suffering for the person with dementia or behaviours that cause distress for the carer. It can be challenging to identify the reasons behind BtC. Furthermore, BtC may occur in as many as 60% of cases (Jackman & Beaty, 2015). BtC can arise from the PLWD’s inability to communicate their unmet needs, problems, or pain caused by co-morbidities or fluctuations in the BPSD (James et al., 2022). Managing the situation without the required skills can be highly stressful for the carer, even where understood. As a result, the carer may respond in ways detrimental to their and the PLWD’s wellbeing. It could also harm the relationship between the carer and the PLWD, negatively affecting the sense of personhood in both (Mitchell & Agnelli, 2015).
The impact of care is further exacerbated by the ambiguous loss of the psychological person they once identified with and anticipatory grief around the PLWD’s pending death (Boss & Yeats, 2014). Loss of connection for carers often occurs due to competing demands of care requirements, carer fatigue and stigma attached to social indiscretions perceived by society (Schoenmakers et al., 2010). Social isolation exacerbates grief and negatively impacts mental health. Studies show that almost 40% of carers experience clinically significant anxiety and depression (Mahoney et al., 2005). Decreases in carer mental health tend to align with the breakdown of care, which in turn may result in premature entry into an ACF and a diminished prognosis for the PLWD (Hoe et al., 2007).
Providing care for a PLWD can also provide positive experiences and facilitate meaning-making (Pallant & Reid, 2014). Spending quality time together, providing comfort and companionship, preserving their life stories, and engaging in meaning-making narratives can enrich the relationship and create lasting memories (Boerner & Schulz, 2009). It can promote positive and adaptive grief where the end-of-life experience provides a quality ending, dignity and meaning (Supiano et al., 2022). Unfortunately, without sufficient support, caring for a PLWD can be exhausting and overshadow special moments.
Australian carers frequently prioritise the needs of the person they care for above their own, often sacrificing their wellbeing (Karg et al., 2018). Health professionals also tend to overlook the needs of the carers, as their primary focus is on the care recipient. As a result, carers may experience poor outcomes, highlighting their need for appropriate and timely support and relevant psychoeducation (Bressan et al., 2020). Improving access to support carers was identified as a priority for action in the National Dementia Action Plan. The Plan highlights that: ‘Carers (should) have the information, training and support they need to undertake their caring role and maintain their own health and wellbeing.’ (Department of Health and Aged Care, 2022, p. 46)
Despite this goal, an evidence-based intervention that meets this strategic agenda is not yet freely accessible within the Australian context, though several are being investigated.
Several systematic reviews have analysed methods to enhance the overall wellbeing of carers. For example, Rosa et al. (2010) and Selwood et al. (2007) found that multicomponent psychosocial interventions are the most effective solution to improve carer wellbeing, education, perceived competence and confidence, resilience, and positive care delivery. While other interventions, such as systemic interventions, can be effective, only some consider the full and unique scope of individual carer needs.
The Newcastle Model is an example of a systemic approach to managing BtC in an ACF (Jackman & Beaty, 2015). It involves a Specialist Dementia Intervention Team (SDIT) that visits an ACF and leads an individualised formulation-led intervention that includes family members and staff to resolve complex BtC (Holle et al., 2017). The SDIT then implements the care plan and provides tailored training to staff (Jackman et al., 2017). This model considers Kitwood’s person-centred conceptualisation of dementia and takes an interest in the PLWD’s background story (cited in Mitchell & Agnelli, 2015). The Newcastle Model represents a unique though costly aspect of optimal care. It does not, however, address the scope of carer needs and support. As such, it is best suited to complex behavioural challenges outside of the carer’s scope of competence.
The STrAtegies for RelaTives (START) multicomponent manualised intervention program is an eight-week carer-focused model of care that aims to offer a viable and economical approach that addresses the full scope of carer needs (Livingston et al., 2014). It includes behavioural analysis and considers the PLWD’s background story and needs preferences, per the Newcastle Model. It is consistent with treatment as usual (TAU) as it has a robust Cognitive Behaviour Therapy (CBT) component. For example, it contains behavioural activation, pleasant-event planning, cognitive restructuring, communication skills and planning, and mood monitoring. START, however, also includes novel components and can be delivered by a range of healthcare professionals, including provisionally registered psychologists.
The novel components of START target dementia-specific care requirements and education. For example, the communication model refers to different communication styles and addresses ways to communicate more effectively with a PLWD. It provides carer-specific psychoeducation to generate a more informed approach to understanding carer-related stress and ways to manage it best. START focuses on future planning provisions covering care and support service options, significant legal and financial considerations in care planning, and end-of-life care and preparation. Participants in START are also provided with a comprehensive care manual and resources to refer to post-participation.
Research outcomes have demonstrated that START produces long-term clinical and cost-effective outcomes, with promising results soon after the intervention and six years post-intervention. START was more effective than TAU in improving carers’ mood symptoms and quality of life in the UK (Livingston et al., 2014) and Australia (Kelly et al., 2024). Furthermore, improvements in depressive symptoms remained clinically effective six years after START, and related costs were three times lower than TAU (Livingston et al., 2020). In contrast, those who received TAU reported an increase in depressive symptoms (Li et al., 2014).
STrAtegies for RelaTives (START) was adapted to the Australian context as part of a broader pilot study. A panel of experts aligned START resources to local services offered by the Australian healthcare systems including those that met the demands of a geographically dispersed population. Minor language changes were made, and audio recordings were recreated with an Australian accent. Studies of the feasibility of this adapted START version in Australia have found that carers and therapists report higher overall satisfaction and acceptance of the intervention than TAU (Kelly et al., 2024). Loi et al. (2022), our collaborators inter-state reported high completion rates and generally positive feedback about START’s structure and content from carers. Moreover, 97% of carers stated they would recommend START to other carers and described it as ‘a lifeline.’ Walter et al. (2024) also demonstrated the acceptability of the manualised program to therapists. Additionally, the telehealth modality (START-online) was a practical and acceptable method of intervention delivery relevant to regional and remote locations (Kelly et al.; Loi et al.; Walter et al.). These results demonstrate START’s applicability, adaptability, and acceptability to the Australian context.
Current Case Study
This case study offers valuable first-hand insight into the experience of an Australian carer who participated in START. It provides new knowledge as it explores the initial impact of providing care at home and subsequent care in an ACF. It also considers the mutual relationship and outcomes between the carer and the PLWD.
The carer selected for this case study was the first participant accepted into the START study and underwent therapy with the study’s co-author (and supervisor). Therapy sessions were delivered in the University Psychology Clinic. It was hypothesised that upon completion of the intervention, the carer would report (a) an improvement in their mood and quality of life, (b) a subsequent reduced level of carer burden, and (c) reduced observation of BPSD with a (d) concurrent improvement in the quality of life for the recipient of care.
Study Procedures
STrAtegies for RelaTives (START) Program Outcome Assessment Protocol.
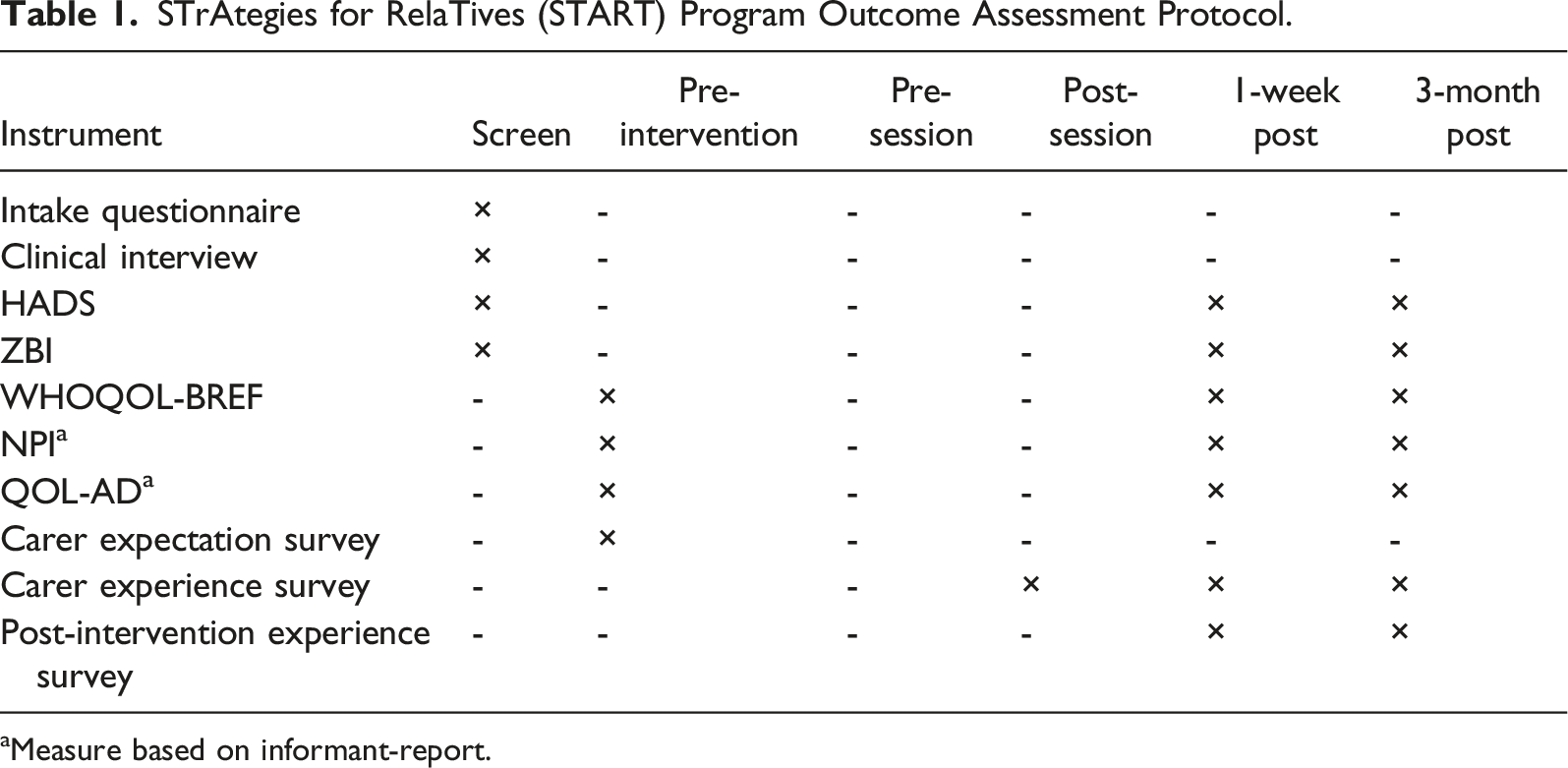
aMeasure based on informant-report.
The carer in this case study was an informal community-dwelling Australian carer recruited through a dementia support organisation. The carer self-referred after attending a presentation on the START study (see Figure 1). The study supervisor contacted the carer and used computerised blocked randomisation at a ratio of 2:1 to assign intervention type. The student researcher obtained informed consent, completed intake, and administered pre-intervention measures via an online forum. Between the point in which the carer self-referred and the pre-intervention measures were administered, the PLWD transitioned to care. Flow chart depicting the phases and process of carer’s recruitment, assessment, intervention, and follow-up through the STrAtegies for RelaTives (START) Program.
The carer opted for face-to-face therapy in the clinic and was blinded to the intervention type. The researcher was initially blinded to outcome measures using online completion of standard measures and survey instruments.
2 Case Introduction
‘June’ (pseudonyms and other deidentifying details have been used to describe each person to protect the client’s confidentiality) was a 49-year-old Caucasian female from a middle-class family, who self-referred to the START study. She lived with her husband and their four children, as well as with her mum (Edith), who had been diagnosed with Alzheimer’s disease.
Edith was an 86-year-old widow and retired special needs teacher living with Alzheimer’s disease. Her husband had cared for her until his death. After that, her daughter June became her primary carer. Edith had two adult children, June and Albert. She was able to walk moderate distances unaided and was continent. She was taking several medications, including two antidepressants, although the details of the medication were not obtained.
3 Presenting Complaints
June reported her mood as depressed and anxious and that she was experiencing stress and distress in her carer role and was finding it difficult to function in her daily tasks. She described withdrawing from social interaction and enjoyable activities. June reported a recent experience of impulsive behaviour when feeling overwhelmed and described how she left her home without her mobile and her mum unattended. She stated she walked for over 4-hours before contacting a friend. This was the trigger that led June to seek support.
4 History
June lived in their newly acquired family home with her husband and their four children (aged 10, 13, 16, and 17). They had recently purchased the property, which June described as her dream home. June was financially secure and reported a good relationship with her husband. She held a university degree and was not currently employed. June was not taking any medications during her participation in START.
June reported being sociable with a close group of friends and two particularly close friends she considered to be like sisters. She had a good relationship with her sister-in-law but not with her brother since they lived far apart. June was an active person and had three dogs.
June’s mum, Edith, had been diagnosed with Alzheimer’s disease and was initially cared for by her husband. June never really understood the pressure her dad was under whilst caring for her mum. She confided that her dad would complain a lot; however, everything seemed fine whenever she visited. June concluded that her dad was just exaggerating. She remembers him saying, ‘When I go, you won’t know what hit you.’ On reflection, June acknowledged the truth in his statement. June reported that her mum ‘was completely different when (she) became the primary carer’ and was ‘in the firing line.’
June described her dad as a ‘grumpy man’ and her mum as a ‘very gentle woman who loved kids,’ June stated that her mum ‘just wanted to spend time with her grandchildren, but (her) dad would not let her.’ She said her ‘mum was the educated one’ and her dad ‘was the controlling one.’ June remembered the frequent arguments between her parents and took solace in that her mum only remembered the good times. After her father passed away, June assumed care of Edith and brought her to live with her family. June had always thought that Edith was more independent and capable than she was. However, the situation caught June off-guard, and she felt guilty about dismissing her dad’s concerns.
June felt overwhelmed caring for her mum without much support from her husband and children. She expected more understanding and help from her family but instead felt emotionally drained and out of her depth. June stated she had ‘no idea how to fix things’ and ruminated on thoughts of guilt and regret. She felt anxious and depressed.
5 Assessment
Outcome Measures
Psychometric Results and Scope of Change: Reliable Change (RC), Clinically Significant Change (CSC^), No Change (NC), or Deterioration (D) According to Time Point.
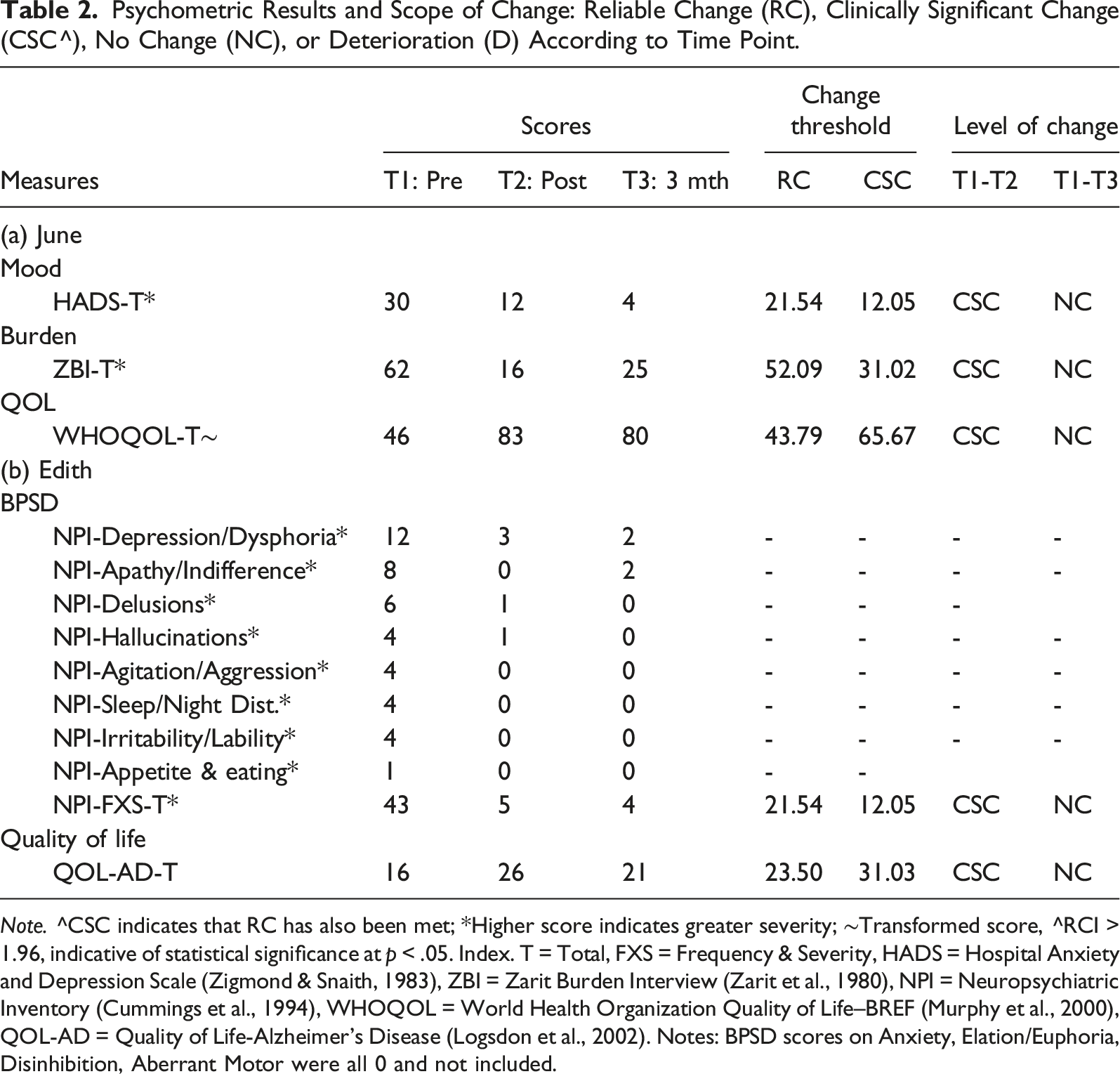
Note. ^CSC indicates that RC has also been met; *Higher score indicates greater severity; ∼Transformed score, ^RCI > 1.96, indicative of statistical significance at p < .05. Index. T = Total, FXS = Frequency & Severity, HADS = Hospital Anxiety and Depression Scale (Zigmond & Snaith, 1983), ZBI = Zarit Burden Interview (Zarit et al., 1980), NPI = Neuropsychiatric Inventory (Cummings et al., 1994), WHOQOL = World Health Organization Quality of Life–BREF (Murphy et al., 2000), QOL-AD = Quality of Life-Alzheimer’s Disease (Logsdon et al., 2002). Notes: BPSD scores on Anxiety, Elation/Euphoria, Disinhibition, Aberrant Motor were all 0 and not included.
Outcome measures for Edith were completed by June through an informant report. The measures included the Neuropsychiatric Inventory (NPI) (Cummings et al., 1994), which was used to measure the frequency and severity of BPSD, and the Quality of Life–Alzheimer’s Disease (QOL-AD) (Kahle-Wrobleski et al., 2016) was used to measure Edith’s quality of life, with higher scores indicative of increased quality.
Carer Surveys
Carer Surveys were completed to measure carer expectations, experience, and helpfulness of START. The surveys were completed pre-intervention, pre- and post-session, one week after intervention, and three months after intervention.
6 Case Conceptualisation
Presenting Problems and Mental State Exam
June reported symptoms consistent with depression and anxiety within the context of caring for her mum. She was observed to be somewhat flat in affect, and her speech was slow and monotone. She was oriented to person, place, and time. She maintained good eye contact, and her thinking was generally focused and thought form unremarkable. Memory appeared intact. She appeared to have reasonable insight into her situation and its impact on her functionality. She denied any history of substance misuse or current suicidal, self-harm, or homicidal ideation.
Pre-existing Vulnerabilities
June reported a similar caring situation in which her coping skills were stretched due to increased family responsibilities. Following the birth of her fourth child, June experienced an episode of depression, which required treatment, suggesting June may be predisposed to doubt her ability to cope and care for her mum. Also, when June assumed responsibility for Edith’s care, she was still mourning the recent loss of her dad.
Activating Events
June was not prepared for the impact of moving her mum into the family home. She did not fully understand the scope of her mum’s Alzheimer’s or the level of care she would require. The family dynamics were disrupted, and she struggled to meet everyone’s needs.
Perpetuating Factors
June felt entangled in uncertainty and grieved the life she once had. June believed she lacked the required skills to care for Edith and thought she ‘should be more organised’ and ‘better able manage her situation’. June was living in anticipation of her mum’s death and experiencing both ambiguous loss and anticipatory grief, triggering unrelenting emotional pain. She reported that her ‘mum was physically there but (no longer) the person (she once) knew and loved’. She felt trapped and hopeless, along with a deep sense of despair.
Equally, June regretted ‘not taking the time to have a more meaningful conversation with (her) mum’, stating ‘it is sort of too late now.’ She also felt guilty for not being empathetic towards her dad during the time of providing care, yet she also resented him for ‘never letting her (mum)’ spend time with her grandchildren.
June’s maladaptive beliefs led to self-doubt, negative thoughts and unhelpful coping. For example, June felt ‘out of her depth’ and ‘overwhelmed’ and acted on these feelings of self-doubt when she left her home and mum for 4-hours with no means of contact. She was consumed by self-blame (e.g., June had felt that she was ‘caught off guard,’ her dad had said, ‘You will not know what hit you when I am gone,’ and she did not believe him, yet now here she was ‘breaking down’), and self-criticism (e.g., ‘I really have no skills at all,’ ‘I say the wrong thing… (and) upset her,’ ‘I have let (everything) go, and now I do not know where to start’) and ruminated on these negative thoughts and judgements.
June withdrew from her social network, limiting support and meaningful connection (e.g., she opted out of a hike with friends because she felt ‘anxious and could not leave (her) mum’). June likewise neglected self-care (e.g., she stopped swimming and practising yoga). June’s avoidance contributed to her mood problems and perception of burden. June engaged in passive communication, so even where she actively sought support from her family, support was rarely forthcoming in a way she found helpful. As time went by, June became more fatigued, distressed, and overwhelmed, further exacerbating her symptoms.
Protective Factors and Strengths
June was resourceful and socially connected. She took the initiative, self-referred to START, and remained actively engaged throughout the program. She had a history of overcoming life’s challenges, and it was evident that she was invested in her and her family’s quality of life. Throughout the program, June demonstrated a healthy response to new insights and the uptake of skills. She employed active coping, as evidenced by her participating fully in the START program; she reconnected with her network of friends and reached out to her sister-in-law for emotional support.
7 Course of Treatment and Assessment of Progress
Treatment Plan
STrAtegies for RelaTives (START) Program Treatment Outline.
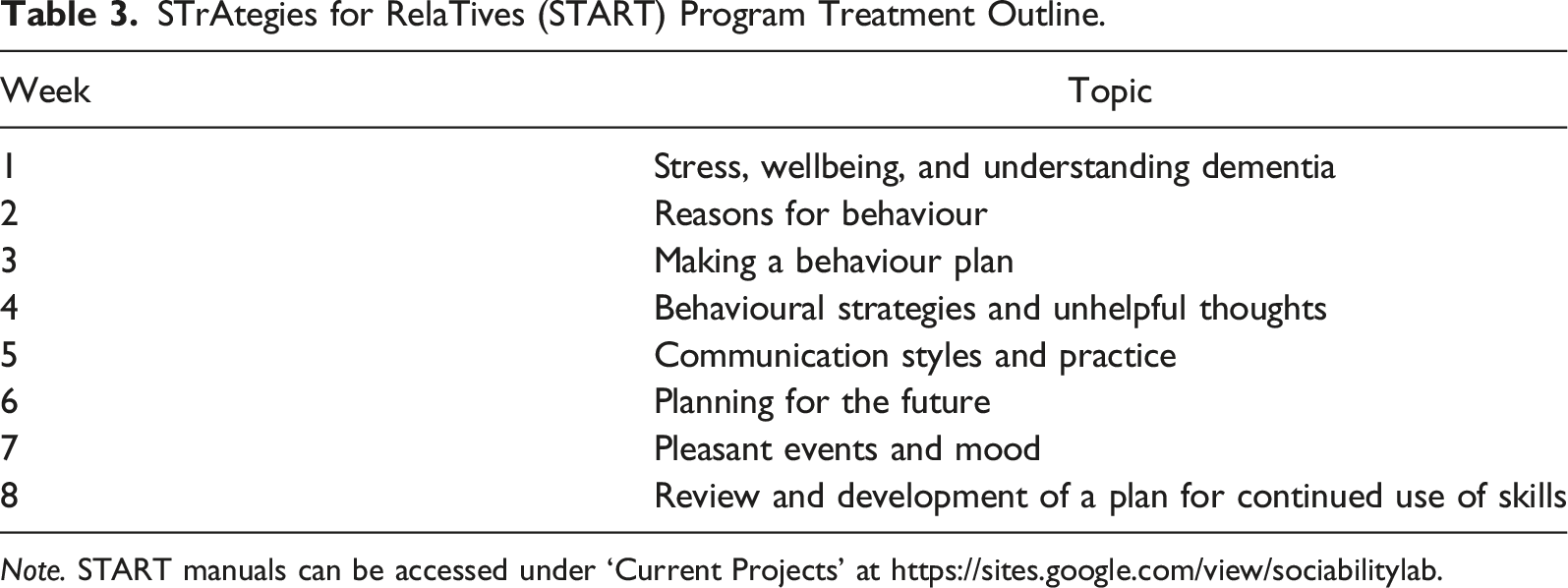
Note. START manuals can be accessed under ‘Current Projects’ at https://sites.google.com/view/sociabilitylab.
June continued to be actively involved in Edith’s care following her transition into an ACF. She visited regularly and continued to provide support and companionship. This included engagement in meaningful and pleasurable activities, coordination and escorting Edith to appointments and safeguarding Edith’s daily and nutritional preferences. June managed her personal belongings and seasonal wardrobe and worked with staff to problem-solve BtC. She also participated in decision-making regarding care. For these reasons, June remained interested in completing the program.
Assessment of Progress
Pre-Intervention
June completed all pre-intervention measures and surveys following Edith’s transition into formal care. On the Pre-Intervention Expectation Survey, June identified her therapeutic goals, which were: ‘learning new ways to cope with her mum’s Alzheimer’s and learning new skills to help her.’
The therapist first normalised June’s experience and relayed the benefits of developing dementia-specific care skills to help her cope better in her carer role. June rated her stress 5 out of 5, indicating she was ‘extremely’ tense. A risk assessment was conducted in response, and an agreed-upon safety plan was implemented. The therapist then socialised June to home practice, and the between-session tasks were designed to help her master and integrate new skills into her carer role. The session was finished with a single-breath relaxation practice.
Upon transitioning into an ACF, Edith reportedly accused June and the staff of ‘taking her clothes’. The therapist explained that with Alzheimer’s, the memory is usually the first thing to go. What remains of their cognitive function is telling them that the item is no longer where they ‘recall’ putting it; they then become confused, which often leads to paranoia and mistrust. They then completed the ‘Trigger-Behaviour-Reaction’ Record to investigate why Edith thought the staff stole her clothes.
June explained that Edith had become stressed whenever a nurse entered her room. Edith was also ‘getting cranky with the nurses, not talking to anyone, and refusing to leave her room’. Recounting and recording events as part of the template helped June better understand what triggered her mum’s behaviour.
For example, during the previous week, June had swapped her mum’s clothes over for her winter wardrobe, which made her mum very happy. When reflecting on this event, June realised that her mum had not had access to her suits and, importantly, that her mum ‘always wore suits in winter.’ June concluded that Edith was ‘triggered’ to look for her suits when the weather cooled. When she could not find them, she accused the staff of giving away her clothes (behaviour). Upon returning the suits to her mum (reaction), Edith thanked her (desired behaviour). June rated her stress 3.5 out of 5, indicating she felt ‘moderately’ to ‘really’ tense. The session was finished with a meditation relaxation practice.
‘Her wardrobe is at the entry of her room. The clothes basket is in her wardrobe, and her underwear is in the basket. She likes to wash her underwear out herself. Every time she goes to the bathroom, she checks for her underwear. When she checks for her underwear, she sees the basket, reminding her that someone else is washing her suits even though she has only worn them once. This makes her distressed over her suits and that people are taking her clothes.’
It was determined that if there was no basket or underwear present, Edith might not be triggered by any memory cues and that avoiding going into the room might also be helpful. A checklist of potential triggers was created to either remove or avoid. June agreed to conduct the ‘underwear’ experiment as part of her home practice. The therapist reminded June that trying different strategies is essential, and if removing the triggers did not work, then distraction can also help shift her response.
It was agreed that a list of three ‘talking points’ would provide a good diversion strategy that staff could also use. Reinforcement strategies for encouraging desirable behaviours were also explored, including gestures such as getting excited about a topic of interest, hugging, or touching her mum’s hand. June rated her stress 3 or 4 out of 5, indicating she felt ‘moderately’ to ‘really’ tense. The session was finished with a physical grounding relaxation practice.
Unhelpful thoughts were explored next. June mentioned she had been thinking about her friends, sharing, ‘They have not been calling me much, and why would they want to talk to me when all I have is negative stuff to say.’ The therapist rationalised to June that her current conclusions might include cognitive errors, such as misinterpreting the thoughts and beliefs of others. She added that acting on cognitive errors can result in a cycle that maintains mood problems, negative self-appraisal, and social withdrawal. Alternative, more helpful interpretations were discussed. June had avoided calling her friends and, therefore, felt sad, lonely, and isolated. With guidance, June reframed her negative thoughts by adopting a balanced view. June rated her stress 1 - 2 out of 5, indicating she felt ‘not at all’ to ‘slightly’ tense. The session was finished with a guided imagery relaxation practice.
June created a digital photo album to preserve her mum’s memories as part of this shift. When asked about her thoughts on how her mum would like to be treated at the end of her life, June replied, ‘She would prefer to be touched and cared for and to be quiet and comfortable.’ Together, they role-played difficult end-of-life conversations that June needed to have with her family. June found this helpful, as she was experiencing resistance from some family members. June rated her stress 0 out of 5. The session was finished with a guided imagery relaxation practice.
8 Complicating Factors
Complicating factors included a delay between June’s self-referral and commencement, Edith’s entry into an ACF, purchasing a new family home, demanding family and home management responsibilities, and dealing with her parents’ estates. Her only sibling was absent and unwilling to contribute to disposing of the estates or caring for their mum.
9 Access and Barriers to Care
There were no significant access or barriers to care for June and no out-of-pocket costs. June could not complete homework on one occasion, but this did not interfere with therapy. Returning to work meant that she needed to complete the final two sessions as one.
10 Follow-Up
Post-Intervention Outcome Measures
Psychometric measures were repeated 1-week- and 3-months- post-intervention to assess June and Edith’s therapeutic outcomes. Data were exported to Excel and analysed using Morley and Dowzer’s (2014) Leeds Reliable Change Indicator simple Excel calculator for a single Case Study to assess if a reliable change had occurred on psychometric measures. The Morley and Dowzer calculator is based on the formula outlined by Jacobson and Truax (1991), whereby reliable change (RC) indicates the amount of change that occurs outside of potential error (RC = +/− 1.96). Normative and clinical reference data were used to determine reliable change and clinically significant change parameters.
Data for mood, burden, and quality of life were examined to investigate the intervention’s immediate and 3-month follow-up effects for June. Data for BPSD and quality of life was examined to investigate immediate and 3-month follow-up dyadic effects on Edith.
Changes in June’s Self-Report Measures
Analysis of June’s self-reported mood (HADS-T) and burden (ZBI) indicated that June showed a reliable and clinically significant decrease in her mood symptoms and perceived level of carer burden, respectively. These decreases were maintained at three-months post-intervention follow-up. June’s self-report on her quality of life (WHOQOL-BREF) indicated a reliable and clinically significant increase maintained at a 3-month follow-up (See Figure 2 Changes in June’s and Edith’s measures over time). Reliable changes (RC) and clinically significant changes (CSC) in June’s self-report for mood on HADS-T, burden on the ZBI, and QoL on the WHOQOL-BREF, and in Edith’s self-report for frequency and severity full-total (FXS-FT) and quality of life on the NPI and QoL-AD, respectively, at pre, post and three-month.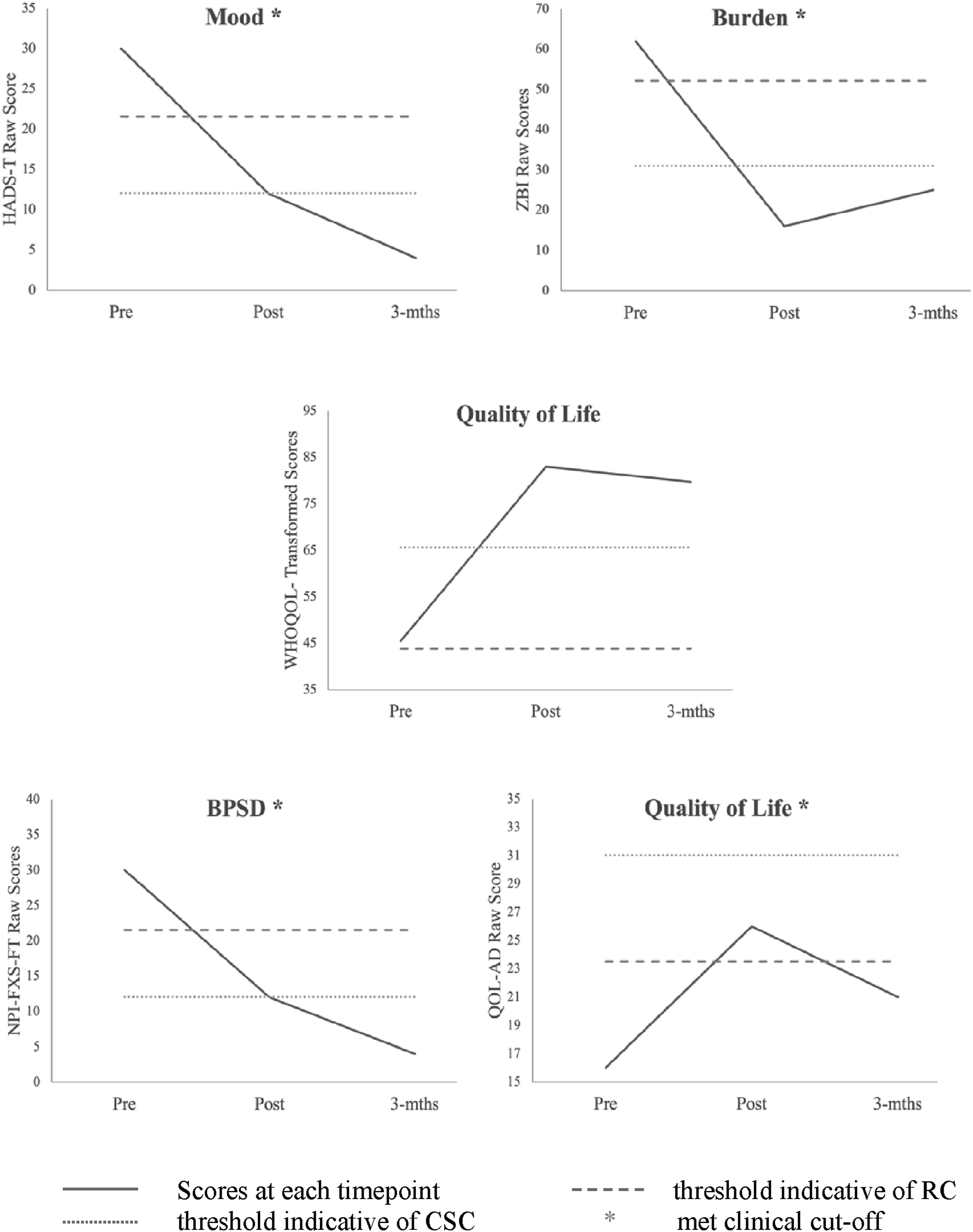
Changes in Edith’s Informant Measures
Analysis of Edith’s informant-reported BPSD (NPI) indicated a reliable and clinically significant decrease across all assessed symptoms, which was maintained at a 3-month follow-up. Her Quality of Life (QOL-AD) score indicated a reliable and clinically significant increase post-intervention, maintained at a 3-month follow-up.
Post-Intervention Experience Survey Measures
June’s Intervention Experience
June’s experience of START was assessed using the 1-week and 3-month post-intervention surveys. On the 1-week post-intervention, June indicated that the program exceeded her expectations and was highly relevant to her situation. She wrote that ‘learning about the behaviours and problem solving when they occur’ was most helpful. She added that she ‘valued the support, being able to talk about problems and knowing that her mum’s behaviours were normal for dementia.’ June indicated that the program would have lasting effects, and she intended to continue using her new skills. June also indicated that she would refer other carers to the program. When surveyed on what we could do to improve the program, she wrote that ‘fortnightly might offer more significant opportunities to implement new learning’ and that she ‘looked forward to each session’.
At the 3-month follow-up, June was again asked to reflect on the program. Her responses remained consistent with those provided 1-week post-intervention. June found all aspects of the program to be either extremely helpful or very helpful and indicated that the most useful skill overall was the Behaviour Change Plan. When asked about her most valuable insight, June wrote, ‘understanding why (her) mum would do certain things, knowing how to deal with them and that (her) mum’s behaviours were typical for someone with Alzheimer’s.’ When asked to rank the usefulness of the sessions in descending order, June ranked ‘behavioural strategies’, ‘stress and wellbeing’, and the ‘communication styles’ sessions as her top three, respectively.
At 36-months, a brief follow-up phone call to June confirmed that she still benefited from the program and continued to refer to her manual.
11 Treatment Implications of the Case
The case study extends current evidence for the feasibility of START for Australian carers by demonstrating its efficacy across contexts. START remained influential even after the PLWD moved to an ACF. It demonstrates the importance of supporting carers during and following the transition to formal care. It also highlights the importance of adequate support to carers across contexts, as this can facilitate positive flow-on effects for the PLWD. The study provides detailed insights and elucidates the therapeutic and lived experience of the carer completing START whilst caring for a PLWD. Importantly, these insights may inform others of the challenges and rewards of caring for a PLWD. Lastly, it supports using standardised instruments such as the NPI to help carers and the care team better understand the presenting symptoms and set meaningful goals for optimised care.
12 Recommendations to Clinicians and Students
The first recommendation from this study is that clinicians and students should consider using manualised multicomponent interventions to support carers of PLWD. The manualised approach ensures consistent information delivery regardless of the therapist’s experience. The manual also serves as a valuable resource to therapists and clients. June, for instance, reported that the manual was an excellent resource she could refer to regularly.
It is important to note that manualised programs can sometimes lead to therapists adhering too strictly to the program’s structure. For instance, the structure of the START program allows for later sessions to be delivered earlier if deemed appropriate. Unfortunately, this did not happen in this study. In retrospect, the therapist could have delivered Session 6 earlier, as it would have provided more benefit to June at this time point given Edith’s transition into formal care.
Clinicians and students should also consider learning about different types of dementia and associated symptoms. Tailoring interventions to the individual and using standardised measures can improve outcomes. Supervision from an experienced psychologist trained in START is highly recommended.
Footnotes
Acknowledgments and Credits
The authors would like to thank all participants, carers, and therapists who participated in the study. We acknowledge the members of the START advisory group, in addition to Anita Panayiotou, Hannah Capon and Ellen Gaffy, for their contributions to the manual adaptation. We further acknowledge Dr. Penny Rapaport and Dr. Claire Nussey for support in START training and Professors Gill Livingston and Briony Dow for their mentorship and collaboration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.