
Abstract
Significance Statement
(1) Developed a novel Measurement of the Five Emotions (MFE) for predicting mild cognitive impairment. (2) Presented an idea that emotional reactions are signals of cognitive function. (3) The findings can provide a better understanding of the mind and body relationship.
Introduction
As the global aging population continues to grow, the prevalence of dementia cases is on the rise. 1 Consequently, addressing the treatment and prevention of dementia has become an urgent matter. Furthermore, there is an alarming increase in the number of individuals exhibiting symptoms of early-onset dementia. 2 Among the various types of dementia, Alzheimer's disease (AD) is responsible for over half of the cases of mild dementia. AD progresses slowly and irreversibly, with no effective treatment currently available. Moreover, mild cognitive impairment (MCI) carries a significantly higher risk of transitioning to AD compared to older individuals with normal cognitive function. 3 Therefore, early identification of individuals at a heightened risk for MCI is crucial in order to mitigate the potential population affected by AD. While there are ongoing studies exploring different approaches within the medical field,4,5 there remains a notable deficiency in theories and methods related to screening and preventive interventions.
In this current study, our objective is to develop a novel assessment tool that can effectively evaluate and predict early cognitive impairment. Our approach incorporates the concept of “mind-body integration” derived from Traditional Chinese Medicine (TCM). It is important to note that the understanding of dementia varies significantly between the medical sciences in China and Western societies. In Western medicine, dementia is predominantly viewed as a result of brain deterioration.
3
However, within TCM, dementia or cognitive impairment is seen as a manifestation of the disconnection between the mind and the body.
6
In TCM, the term “mind” refers to human emotions and thoughts, while “body” represents the functioning of organs, as described in the ancient medical text, ‘Yellow Emperor's Internal Medicine'.
7
Specifically, TCM classifies the “mind” and “body” into 5 fundamental elements: wood, fire, earth, metal, and water. These elements correspond to the 5 organs: liver, heart, spleen, lungs, and kidneys, respectively. Importantly, each organ is associated with a distinct “mind” or emotion, namely anger, joy, thought, sorrow, and fear (Figure 1). Imbalances in emotions can disrupt the equilibrium of the organs, leading to various diseases, including dementia.
7
The concept of mind-body integration has gained traction in the study of cognitive decline among aging populations.8,9 Therapeutic approaches such as meditation, tai chi, qigong, yoga, and biofield therapies have shown promise in preventing and treating cognitive decline.
9
However, there is currently no established tool for detecting or predicting dementia using this theory. The relationship among the 5 organs, 5 elements and 5 emotions defined in traditional Chinese medicine. The 5 elements, wood, fire, earth, metal and water, are believed to be the essential elements of the universe by the ancient Chinese philosophers. The white-black graphic is a symbol of Taiji, meaning the diagram of the universe in ancient Chinese philosophy.
Our research consists of 3 stages to develop a measurement tool called the Measurement of 5 Emotions (MFE), with a specific focus on preventing mild cognitive impairment (MCI). The first 2 stages of development have already been completed. 10 In the initial stage, a draft version consisting of 25 items was used to assess the connection between the reaction state of the 5 organs (liver, heart, spleen, lung, and kidney) and the 5 corresponding emotions (anger, joy, thought, sorrow, and fear). Content validity of the 25 items was assessed by 7 experts. In the second stage, 20 experts evaluated the correlation between the initially selected items and the conceptual elements, using measures such as concordance rate and index correlation. The average coefficient of the index correlation was found to be 79%. Based on the content validity test, the initially selected 25 items were refined to 20 items (Table 1). 10
The present study represents the third stage of our investigation, utilizing the survey data obtained from an aged population in Kyoto City, Japan. The aim of this study was to assess the validity and reliability of the newly developed MFE tool. In addition, our central hypothesis was that emotions are correlated with cognitive functions. By using DASC-21, a well-established scale for cognitive function in which a higher score indicates lower cognitive function, 11 this hypothesis would be supported by a negative correlation between MFE and DASC-21 scores.
Materials and Methods
Sample Size
Due to the challenge of estimating the difference (effect size) between groups using the newly developed scale, we determined the sample size by multiplying the number of items in the MFE scale by 10, resulting in a target sample size of 200. 12 In addition, we consulted previous studies that developed the MSD-28 and DASC-21 scales to guide our sample size estimation. 13 Considering potential missing values on the answer sheets and the expected collection rate, we conducted a survey with 300 participants.
Survey Deployment
Between April 1st and November 30th, 2022, survey forms along with self-addressed stamped envelopes were distributed at local dementia prevention seminars and among residents in various organizations in Kyoto City, Japan. The survey form consisted of 20 items from the MFE scale and 21 items from the Dementia Assessment Sheet for Community-based Integrated Care System (DASC-21).11,13 Additionally, background information including marital status (married, single, or divorced), existence of cohabitants (yes or no), frequency of health check-ups (once a year, once in 2 years, or irregular), and usage of in-home service (no, once a week, twice a week, or more than 3 times a week) was collected using a checklist. To convert the descriptive background information into binary data, “single” and “divorced” were combined as “single” vs “married”, “once in 2 years” and “irregular” of health check-ups were combined as “irregular health check-ups” vs “annual health check-ups”, and answers for in-home service other than “no” were considered “using in-home service” vs “not using in-home service”.
Initially, the study participants were limited to attendees of the seminars and residents aged 65 years and above.
Statistical Methods
To examine the measurement reliability of the MFE scale, item-total reliability was assessed by comparing the Spearman correlation coefficient value of each question item and the overall score. The Cronbach α coefficient of the survey was calculated to test its internal consistency reliability. Furthermore, item deletion analysis was performed. Briefly, the Cronbach coefficient was calculated after each item was deleted. If the Cronbach coefficients remained ≥.70, the reliability of the measurement was verified.
To assess the validity of the MFE scale, the number of crucial factors was calculated using the principal component analysis approach. The factors with loading <.3 in the analysis were eliminated from the question items. The test of criteria-related validity was performed using the DASC-21 developed by Awata et al11,13 Furthermore, construct validity was examined by both factor analysis and hypothesis testing. The hypothesis, originally derived by Wu et al, 14 was that elderly people who responded well to MFE were less prone to MCI. In their investigations on the relationship between cognitive function and anxiety in patients with mild dementia, Wu et al 14 noted not only a positive correlation between anxiety and memory delay but also a negative correlation between depression and language function. Thus, a negative correlation between MFE and DASC-21 should be expected.
MFE-20 Questionnaire.
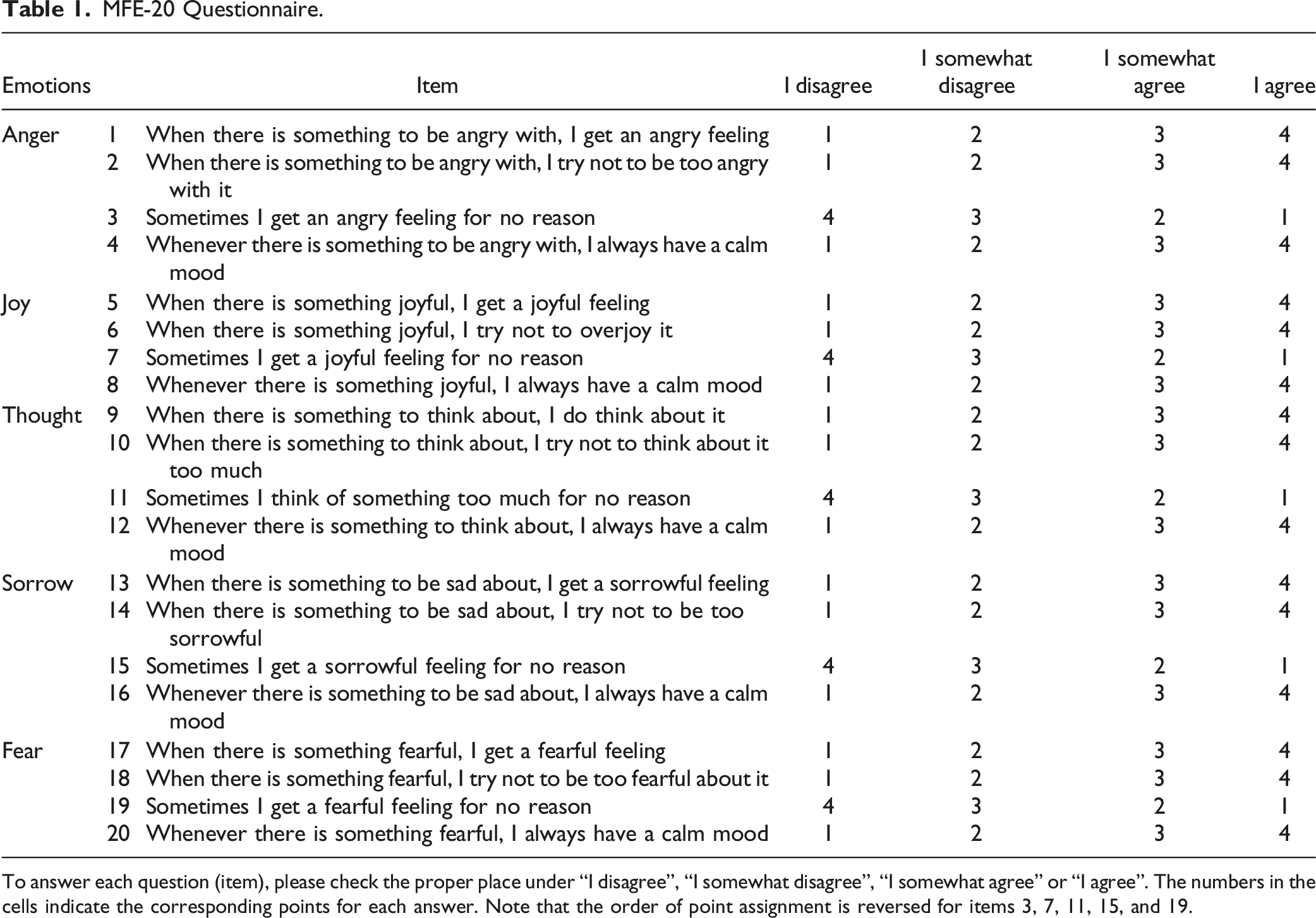
To answer each question (item), please check the proper place under “I disagree”, “I somewhat disagree”, “I somewhat agree” or “I agree”. The numbers in the cells indicate the corresponding points for each answer. Note that the order of point assignment is reversed for items 3, 7, 11, 15, and 19.
Results
Participant Characteristics
The inclusion/exclusion process during sampling is depicted in Figure 2. A total of 300 surveys were deployed. 44 and 150 surveys were received from seminar attendees and organization residents, respectively. 5 surveys with missing answers and 5 surveys from participants under age 65 were excluded, resulting in a 61.3% response rate. Among the participants, 143 (77.7%) were female and 41 (22.3%) were male, with their ages ranging between 65-97 years. The participant characteristics are shown in Table 2. Altogether, 107 people (58.2%) lived alone whereas 77 people (41.8%) did not. Moreover, 145 people (78.8%) had annual health check-ups and 39 people (21.2%) had irregular health check-ups (Table 2). 133 (72.3%) people used in-home services. Significant differences were observed in the background information between the 2 cohorts, “seminar attendees” and “organization residents.” These differences included variables such as “Marital status”, “Sex”, and “Health checkup frequency”. However, no significant differences were found in survey scores (MFE and DASC-21). Consequently, we decided to combine the 2 cohorts for the analysis. Flow chart of the inclusion/exclusion process in this study. The gray arrows and boxes indicate the excluded samples. Participants’ Characteristics. SD: Standard Deviation. MFE: Measurement of Five Emotions. DASC-21: The Dementia Assessment Sheet for Community-based Integrated Care System.

Descriptive Statistics of 20 Items of MFE
Descriptive statistics were conducted for the 20 question items related to emotional states (Table 2). The total scores ranged from 31 to 71 points, with a skewness of .69 and a kurtosis of .67. The mean scores ± standard deviations of the measurement were 57.2 ± 6.2 for men and 57.4 ± 7.6 for women, respectively. There were no significant differences in the measurement scores as a whole or at any subscale between men and women (Mann-Whitney test, P > .05).
Examination of Reliability
Examination of Reliability of the “MFE"

Examination of Construct Validity
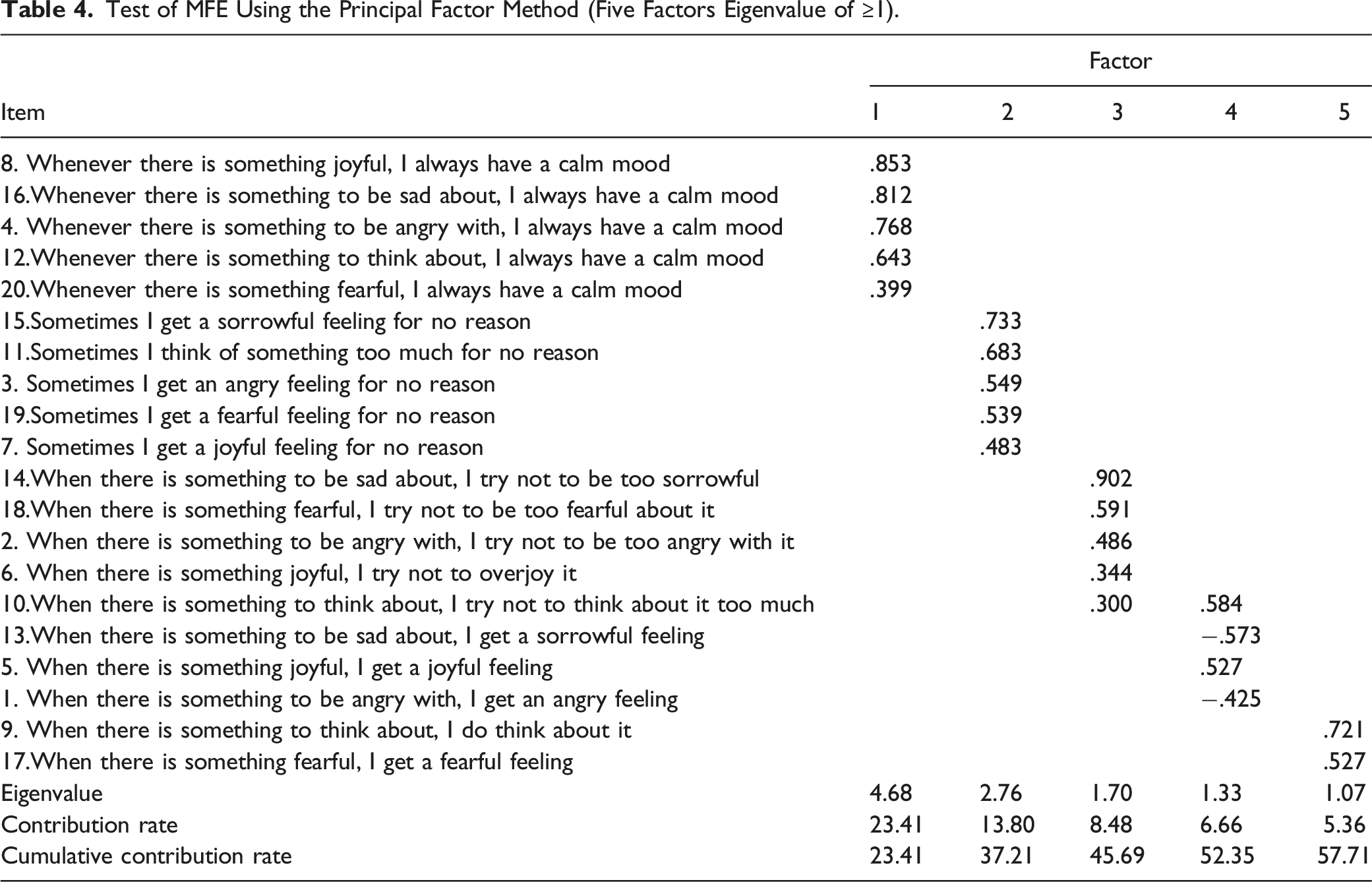
Test of MFE Using the Principal Factor Method (Five Factors Eigenvalue of ≥1).
Nomenclature of MFE
Factor analysis of the 20 items revealed 5 factors explaining the categories of the questions (Table 4). The 5 items linked to the 1st factor were named the ‘normal states of the 5 emotions’. The 5 items linked to the 2nd factor were named the ‘abnormal states of the 5 emotions’. The 5 items related to the third factor were named the “self-regulation reaction items”, except for the item 10 which read, “When there is something to think about, I try not to think about it too much”. This item had a loading of ≥.3 for both the third and fourth factors. And the fourth factor's loading was heavier. Although a few revisions were required, these items were named the “self-regulated reaction items”. Four items with the fourth factor and 2 items with the 5th factor were mixed as the ‘normal reactions of the 5 emotions items”. And 1 of the items had loading on the third factor. They were named the “normal reactions of emotions joy and anger”. When the fourth and 5th factors were combined, the analysis of the remaining 4 factors did not lead to changes in the items with the 1st and 2nd factors, but the items with the third and fourth factors were intertwined. This can be explained by the overlap between “normal reaction” and “self-regulated reaction”.
Examination of Criterion-Related Validity
In the criterion-related validity test, the Spearman correlation coefficient r was found to be -.31 (P < .01) (Figure 3), which indicated a negative correlation between MFE and DASC-21 scores. Scatter plot depicting the negative correlation between MFE and DASC-21. Each dot represents an individual participant.
To further dissect this inter-criterion relationship, we divided the MFE scores and DASC-21 scores into low and high groups by the average (57.6 in MFE and 26.9 in DASC-21). Consistently, the MFE high group had significantly lower DASC-21 scores (Figure 4A). On the other hand, the DASC-21 low group showed high emotional response scores of ‘thought’ and ‘sorrow’ in MFE scores (Figure 4B), further suggesting a relationship between the disturbance of these particular emotions and impaired cognitive function. Taken together, these results confirmed that emotions are closely related to cognitive impairment in elderly people. Criterion-related validity of MFE. (A) DASC-21 scores of MFE high and MFE low groups. The red lines indicate the average score of the group. Number over the bracket indicates the P value calculated by Mann-Whitney test. (B) MFE scores of each emotion from the DASC-21 high group and the DASC-21 low group. Numbers above the brackets indicate the P values calculated by Kruskal-Wallis test and Dunn's multiple comparison test.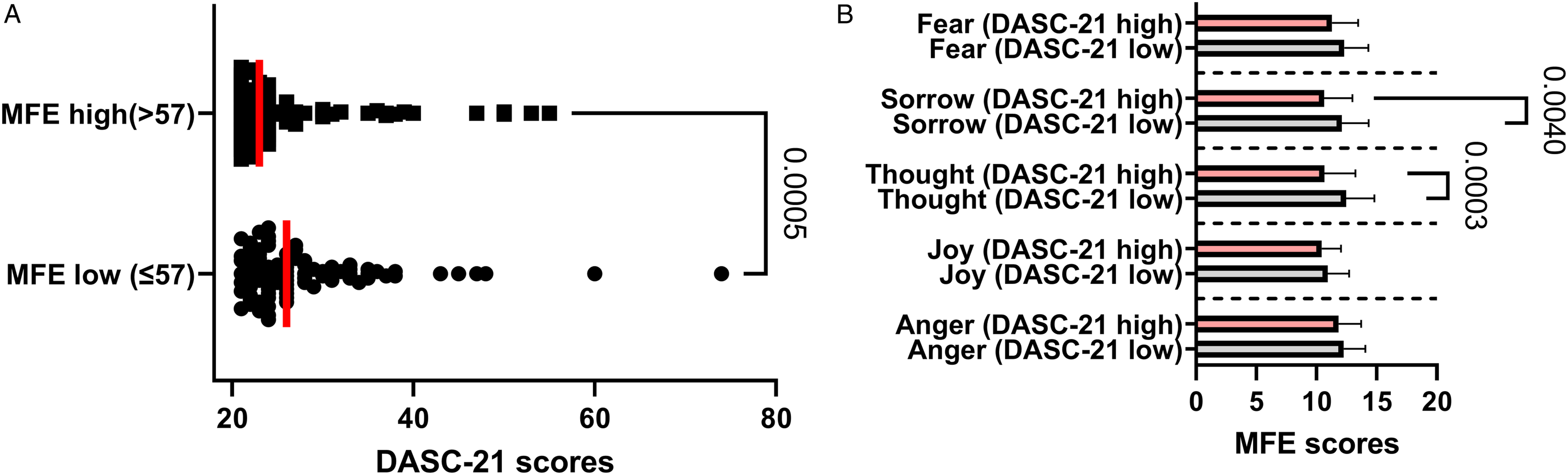
Discussion
In this study, we developed a novel measurement, MFE, and assessed its internal reliability using item-to-total correlation and Cronbach's alpha analysis. Additionally, we examined its validity by comparing it to a well-established scale for cognitive function known as the DASC-21. Correlation analysis revealed a weak but significant (coefficient = −.31, P < .01) negative correlation between the 2 measures. These findings indicate that the MFE can effectively evaluate emotions and potentially predict cognitive impairment in elderly individuals. Although the cause and effect of emotions on cognitive impairment cannot be concluded in this cross-sectional study, the substantial correlation between them implied that the emotions in early stage of cognitive impairment might be a prophylactic target in the development of dementia.
Reliability of the 20-Item Version of MFE
The reliability of the 20-item version of MFE covers the following 3 aspects: stability, internal consistency and equivalence. 15 The present study examined the reliability of MFE in terms of internal consistency.
When determining the reliability of the MFE by deleting items 1 by 1, little change in the alpha coefficient was observed, suggesting that it made a constant contribution to the overall score. The Cronbach α coefficient, which indicates internal consistency across measurements, was .71. An α coefficient of ≥.7 is required to support internal consistency. 16 The obtained value exceeded this value, indicating that each item was working appropriately in terms of internal consistency.
Validity of 20-Item Version of MFE
Criterion-Related Validity
Criterion-related validity of the 20-item version of MFE was verified by comparing it with DASC-21. The DASC-21 was developed by Awata et al,11,13 and its reliability and validity were verified using data obtained from a survey of community-dwelling elderly people aged ≥65 years. Additionally, Yamaguchi et al 17 clarified the characteristics and usefulness of DASC-21 in the initial intensive support team for dementia and showed that DASC-21 was useful for distinguishing between individuals with normal cognitive functioning and those with dementia. DASC-21 is a useful index not only for use in communities in which cognitive function tests are difficult to carry out but also for the evaluation of the nursing support functions of regional comprehensive support centers and care management by nursing care support specialists. The contemporaneous validity of MFE was established by the correlation coefficient analysis between MFE and DASC-21, which revealed a weak yet significant negative correlation (r = −.31, P < .01).
Construct Validity
The results obtained support the hypothesis that, the higher the MFE score, the lower the DASC-21 score and the lesser the cognitive impairment. In most cases, a higher MFE score was associated with a low DASC-21 score. There was a moderate association between DASC-21 and emotional responses. A possible reason for this was that DASC-21 focuses on impairments in the participants’ perceived “cognitive functions” and “life functions” that are closely related to their daily lives, whereas the emotional reactions showed the connection between cognitive and life functions. The present results showed that these 2 concepts could be predicted by each other. Furthermore, the 4 emotional reaction states (the stable and self-regulated, normal and abnormal states) of the 5 emotions that were theoretically constructed were closely related to, respectively, the 4 factors (factors 1, 2 and 3 and the combination of factors 4 and 5 in Table 4) obtained from the factor analysis. This confirmed the basic concept of the theoretically constructed patterns.
Significance in Emotional Care
The obtained results indicated that MFE was a useful index to detect early alterations in cognitive function to prevent MCI and dementia among elderly people living in communities. The developed 5 Emotional Nursing (FEN) (emotional care) model based on TCM has become popular.18,19 However, since there has been no established evaluation measurement for FENs, the tested MFE can be utilised to fulfil this need. Additionally, the tested MFE can also be applied to prevent other diseases caused by emotional problems.
The measurements applied in previous research include the Positive and Negative Effect Schedule score, 20 Apathy Evaluation Scale Score, 21 Dementia Mood Assessment Scale Score 22 (mood scale for patients with dementia), Geriatric Depression Scale, 23 and Zung Depression Self-Rating Scale.24,25 So far, there is no appropriate measurement for the 5 emotions defined in TCM, particularly for elderly people living in communities. Thus, the present findings provide a novel method to fulfil this gap.
Suggestions for Use of MFE
The 5 “organs” defined in TCM are not equivalent to the organs we know in western medicine. This is a holistic concept which incorporates understanding of the homeostasis of human health in TCM.6,7 The relationship between “organs” and emotions, i.e. the mind-body integration described in TCM suggests that diseases can either arise from or cause its disruption.26,27 Therefore, it is important to control one’s feeling in order to maintain the harmony of the 5 “organs” and prevent diseases such as dementia.
The identified 4 factors correspond to 4 reaction patterns in MFE (Table 4). Both ‘normal reaction’ and ‘self-regulated reaction’ indicate a ‘normal state of emotions’ related to a normal state of relevant organs (Figure 1). Therefore, it is possible to diagnose the abnormality of the 5 “organs” from the ‘abnormal state of emotions’.
According to the principle of mental health care described in TCM, 6 there are 2 ways to eliminate unhealthy feelings. One way is to express one's feelings, i.e. ‘Let it be if you are either angry, happy, or sad’. The other way, referred to as ‘win with emotions’, is to use the mutual effect of the 5 emotions to ease each other. For example, joy wins over sadness; thus, 1 should find joy to get rid of their sad feelings. Future studies using these approaches can provide further clinical evidence for the effectiveness of emotional interventions on cognitive diseases.
Research Limitations and Challenges
In the present study, we have verified the internal consistency of the developed MFE; however, its stability needs to be further examined. It is, thus, necessary to conduct further study on the same participants in the future. We are also aware that the actual number of included samples (n = 184) was slightly lower than our initial estimation (n = 200), due to insufficient answers and the exclusion of participants with younger age (<65). While we observed statistical significance in the differences between various groups, it is important to acknowledge the potential bias introduced due to the relatively small sample size. This may have limited our ability to detect smaller effect sizes or more subtle variations among the groups under investigation. Further research with a larger sample size is warranted to confirm and generalize our results.
Footnotes
Acknowledgments
Authors Contributions
Xiaoyu Wu conceptualized the study and Jiaojiao Ziqiu He, Youou Huang and Joe Kodama participated in the study design. Xiaoyu Wu, Jiaojiao Ziqiu He, Youou Huang, Bin Zhou, Yuemin Zhou, and Yuquan Lu conducted the data collection and analysed the data. Xiaoyu Wu wrote the first manuscript draft and all authors participated in its revisions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support from Kyoto Koka Women's University.
Ethical Statement
Data Availability Statement
All the data presented in this study is available under reasonable request to the corresponding author.