
Abstract
Objective
This study aimed to evaluate the effect of clearing heat and resolving phlegm for acute exacerbation of chronic obstructive pulmonary disease with the syndrome of phlegm-heat obstruction of the lung.
Methods
This was a real-world retrospective cohort study of inpatients at our institution from 1 January 2015 to 31 December 2017. The patients were divided into two groups according to whether they received oral traditional Chinese medicine (TCM) for clearing heat and resolving phlegm or routine treatment (controls). Efficacy and safety indicators were analyzed. Propensity score matching was used to control for confounding factors.
Results
Among 488 patients, 164 (82 pairs) were successfully matched. The changes in neutrophils (%) and C-reactive protein levels were more significant in the TCM group than in the control group. The duration of fever was significantly shorter in the TCM group than in the control group.
Conclusions
The therapy of clearing heat and resolving phlegm might effectively control the inflammatory reaction of acute exacerbation of chronic obstructive pulmonary disease in patients with the syndrome of phlegm-heat obstruction of the lung, especially for those with fever. Nevertheless, large-scale and prospective studies are required to provide a higher quality of evidence.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by significant airflow limitation associated with a chronic inflammatory response in the airways and lungs, resulting in destruction of lung tissue.1,2 COPD commonly affects adults >40 years of age who smoke, with an estimated worldwide prevalence of 4% to 10%.1,2 The disease course is usually progressive, with a long-term decline in lung function.1,2 COPD is the third leading cause of mortality worldwide. 3 COPD is a preventable and treatable disease commonly associated with comorbidities (e.g., cardiovascular disease) and significant systemic consequences (e.g., skeletal muscle dysfunction).1,2 Smoking is the most common risk factor for COPD. 4 Other risk factors of COPD include occupational exposure to organic and inorganic dust, chemical agents, and fumes, α-1 antitrypsin deficiency, and indoor air pollution, particularly from biomass smoke caused from burning biomass fuels in confined spaces.1,2 The 4-year mortality rates range from 28% for mild-to-moderate COPD to 62% for moderate-to-severe COPD. 5
COPD has several complications, including acute exacerbation of COPD (AECOPD), respiratory failure, and pulmonary hypertension.1,6 AECOPD is an acute worsening of COPD characterized by changes in baseline symptoms (cough, dyspnea, and/or sputum) beyond the normal daily variations and requiring changes in therapy.1,7 Patients with stages 2 to 4 COPD have one or two exacerbation events per year. 8 The complications of AECOPD include the requirement for mechanical ventilation, altered mental status, cardiac arrhythmia, and cardiovascular events. 1 Management of AECOPD includes short-acting β-2 agonists, corticosteroids, antibiotics, titrated oxygen, and non-invasive mechanical ventilation.1,7 Nevertheless, the in-hospital mortality rate of AECOPD remains at 0.3% to 54.6%, depending upon the number of risk factors found in these patients.9–11
Traditional Chinese medicine (TCM) has been used for a long time for managing COPD.12–16 There are many clinical TCM studies of treatment of AECOPD with the syndrome of phlegm-heat obstruction of the lung.12–16 Most of these studies were randomized, controlled trials (RCTs) with strict inclusion and exclusion criteria, and many patients with severe conditions, complications, or old age were excluded from those trials, limiting their generalizability. Additionally, standardized treatments limit the possibility of drug combinations.
The available RCT results cannot be directly applied to the population of patients with AECOPD. Therefore, to evaluate the clinical efficacy of clearing heat and resolving phlegm for AECOPD with the syndrome of phlegm-heat obstruction of the lung in a real-world setting, this study adopted a retrospective cohort study design without strict inclusion and exclusion criteria. Propensity score matching (PSM) was used to control for confounding factors. We hope that our findings will be more representative of the real world.
Patients & Methods
Study design and participants
This was a retrospective cohort study of inpatients who were hospitalized at the Respiratory Department of Zhejiang Provincial Hospital of Traditional Chinese Medicine from 1 January 2015 to 31 December 2017. This study was approved by the ethics committee of The First Affiliated Hospital of Zhejiang Chinese Medical University [2019-KL-082-01]. This study met the condition for exemption from informed consent.
All patients met the Western medicine diagnostic criteria for AECOPD1,7 and the criteria for TCM syndrome differentiation of phlegm-heat obstruction of the lungs.17,18 The inclusion criteria were as follows: 1) >18 years old; and 2) diagnosis of AECOPD with TCM syndrome differentiation of phlegm-heat obstruction of the lung. The exclusion criteria were as follows: 1) patients receiving oral TCM treatment 3 days after admission; 2) patients with a duration of oral TCM treatment for <5 days; 3) tuberculosis; 4) patients who self-discharged against medical advice; and 5) patients with incomplete data.
The diagnostic criteria for AECOPD referred to the Global Initiative for Chronic Obstructive Lung Disease (2019) 1 and the Expert Consensus on Management of Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD) in China (updated in 2017) issued by the Experts Group for Diagnosis and Treatment of Acute Exacerbations of Chronic Obstructive Pulmonary Disease (AECOPD).19,20 COPD was confirmed by comprehensive analyses, such as clinical manifestations, a history of risk factors, and pulmonary function tests. Clinical manifestations of COPD included chronic and progressively aggravated dyspnea, cough, and expectoration, which frequently occurred in the cold seasons of autumn and winter. Furthermore, there was a history of smoking or exposure to occupational or environmentally harmful substances. Pulmonary function tests confirmed persistent airway obstruction (forced expiratory volume in 1-s/forced vital capacity <70% after inhalation of bronchodilators). After excluding other diseases, COPD was confirmed.
The diagnosis of AECOPD mainly depended on the patient’s clinical manifestations. These were characterized by acute exacerbations of respiratory symptoms that exceeded the normal range of variation, leading to the requirement for additional treatments, and after excluding other specific diseases that could explain sudden changes in these symptoms.1,7 The main manifestations of AECOPD included exacerbation of shortness of breath, which was often accompanied by wheezing, chest tightness, aggravated cough, an increased amount of phlegm, changes in color and/or viscosity of phlegm, and fever.
The TCM diagnostic criteria for phlegm-heat obstruction of the lung referred to the TCM Terminology for Clinical Diagnosis and Treatment, 21 the Guidelines for TCM Diagnosis and Treatment of Chronic Obstructive Pulmonary Disease (2011 edition), 15 and Internal Medicine of Traditional Chinese Medicine (9th edition). 22 The symptoms for this condition included cough, wheezing and rough breathing, chest tightness, dysphoria, sudden eyeball protrusion, excessive phlegm, yellow or white phlegm, difficulty in coughing, fever, slight aversion to cold, less sweating, thirst and favor of a cold drink, scanty dark urine, dry stool, red tongue, yellow or yellow greasy coating of the tongue, and a rapid or slippery pulse. The diagnostic criteria for phlegm-heat obstruction of the lung were as follows: 1) cough or wheezing and dyspnea; 2) excessive phlegm, yellow or white phlegm, and difficulty in coughing; 3) fever or thirst and favor of a cold drink; 4) dry stool; and 5) red tongue, yellow or yellow greasy coating, and a rapid or slippery pulse. Phlegm-heat obstruction of the lung was diagnosed in the presence of items 1 and 2, plus any two items among 3, 4, and 5.
Therapeutic methods
The control group included patients who received treatment for AECOPD according to the Global Initiative for Chronic Obstructive Lung Disease (2019) 1 and the Expert Consensus on Management of Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD) in China (updated in 2017).
The treatment group included patients who received routine treatment, as in the control group, but patients also received oral TCM treatment of clearing heat and resolving phlegm for >5 days and within 3 days after admission. TCM of clearing heat and resolving phlegm was self-prepared by the hospital. Each patient took the decoction of TCM orally twice a day, with 200 mL each time. The main component of this medicine was a white mulberry root-bark decoction (10–15 g of white mulberry root-bark, 9–12 g of processed Pinellia rhizome, 9–12 g of Perilla, 10–12 g of apricot kernel, 10–12 g of thunberg fritillary bulb, 10–12 g of gardenia, and 9–12 g of Scutellaria root). Ephedra and Platycodon root were added for patients with chest tightness and labored breathing caused by the stagnation of lung qi. Snakegourd root and reed rhizome were added for patients in whom body fluids were consumed by phlegm-heat. Adenophora root, dwarf lilyturf tuber, and figwort root were added for those with excessive heat damaging the yin. Peach kernel, safflower, and Sichuan lovage root were added for patients with blood stasis. Rhubarb root and rhizome and magnolia bark were added for those with constipation.
Observational indicators
The general data included sex, age, body mass index, smoking history, past medical history, course of the disease, and medications during hospitalization. Efficacy evaluation indicators included changes in the white blood cell count (WBC), the percentage of neutrophils, C-reactive protein (CRP) levels before and after treatment, duration of defervescence, and hospital stay. Observational indicators of safety included changes in levels of hemoglobin, platelets, serum creatinine, blood urea nitrogen (BUN), alanine aminotransferase (ALT), aspartate aminotransferase (AST), and total bilirubin (TBIL) before treatment and at discharge. Laboratory indicators were obtained from peripheral venous blood under the fasting state in the morning. Blood was collected on the day of admission or the next day, after 5 to 7 days of treatment, and within 3 days after discharge.
Statistical analysis
Data processing was performed using SPSS 22.0 (IBM Corp., Armonk, NY, USA). Continuous data were tested for a normal distribution using the Kolmogorov–Smirnov test. Continuous data with a normal distribution are presented as mean ± standard deviation and were compared with the Student’s t-test. Data with a non-normal distribution are presented as median (interquartile range) and were compared with non-parametric tests. Categorical data are presented numbers and percentages and were analyzed with the chi-square test.
PSM was implemented using SPSS 22.0. Receiving oral TCM treatment of clearing heat and resolving phlegm was used as the dependent variable, and the independent variables included sex, age, course of the disease, the presence or absence of fever, the presence or absence of lung cancer, bronchiectasis, bronchial asthma, interstitial lung disease, pulmonary embolism, cor pulmonale, and pneumonia, WBC and platelet counts, the percentage of neutrophils, levels of hemoglobin, CRP, creatinine, BUN, ALT, AST, and TBIL before treatment, and the use of glucocorticoids, antibiotics, expectorants, and theophylline. The nearest matching method and a ratio of 1:1 were used for matching, using a caliper value of 0.03. P values <0.05 were considered statistically significant.
Results
Clinical characteristics between the two groups before and after PSM
A total of 488 patients were included and assigned to the TCM group (n = 88) and control group (n = 400). Before matching (Table 1), there were significant differences in age, presence/absence of fever, rates of type II respiratory failure and pulmonary embolism, BUN levels at admission, and glucocorticoid use between the two groups (all P < 0.05).
Comparison of clinical characteristics between the two groups before and after matching.

PSM, propensity score matching; TCM, traditional Chinese medicine; M, median; P25, P75, 25th and 75th percentiles; BMI, body mass index; WBC, white blood cell; NEUT, neutrophils; CRP, C-reactive protein; HGB, hemoglobin; PLT, platelet; CREA, serum creatinine; BUN, blood urea nitrogen; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TBIL, total bilirubin.
A total of 164 patients (82 pairs) were successfully matched. After matching (Table 1), there were no significant differences in the clinical characteristics between the two groups.
Evaluation of therapeutic effect
After 5 to 7 days of treatment, there was no significant difference in the WBC count compared with before treatment in the two groups between the two groups. The percentage of neutrophils was significantly lower after 5 to 7 days of treatment compared with before treatment in the control group (P = 0.045) and in the TCM group (P < 0.001) Additionally, CRP levels were significantly lower after 5 to 7 days of treatment compared with before treatment in the control group (P < 0.001) and in the TCM group (P < 0.001). There was no significant difference in the WBC between the two groups. The percentage of neutrophils and CRP levels were significantly lower in the TCM group than in the control group after treatment (P = 0.013, P = 0.044, respectively) (Table 2).
Comparison of therapeutic effects before and after 5 to 7 days of treatment.
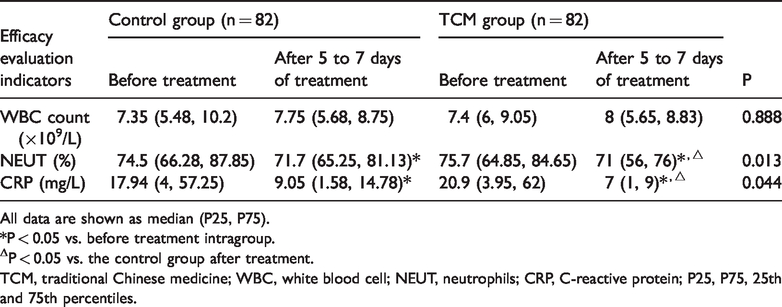
All data are shown as median (P25, P75).
*P < 0.05 vs. before treatment intragroup.
ΔP < 0.05 vs. the control group after treatment.
TCM, traditional Chinese medicine; WBC, white blood cell; NEUT, neutrophils; CRP, C-reactive protein; P25, P75, 25th and 75th percentiles.
Comparison of hospital stay and duration of defervescence in febrile patients
There was no significant difference in hospital stay between the two groups (Table 3). The duration of defervescence was significantly shorter in the TCM group than in the control group (P = 0.044) (Table 3). Because fever caused by pneumonia was different from that caused by AECOPD alone, we performed analysis again after removing patients with pneumonia. The difference in the duration of defervescence was still significant (P = 0.035) (Table 3).
Comparison of the hospitalization stay between the groups.

Data are shown as median (P25, P75).
TCM, traditional Chinese medicine; P25, P75, 25th and 75th percentiles.
Safety indicators
There were no significant differences in levels of hemoglobin, platelets, creatinine, BUN, ALT, AST, and TBIL between before and after treatment in both groups (Table 4).
Comparison of safety indicators before treatment and at discharge.

Data are shown as median (P25, P75).
TCM, traditional Chinese medicine; HGB, hemoglobin; PLT, platelet; CREA, serum creatinine; BUN, blood urea nitrogen; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TBIL, total bilirubin; P25, P75, 25th and 75th percentiles.
Discussion
Because most studies of TCM for AECOPD are randomized trials in highly selected patients,12–16 the present real-world study aimed to evaluate the clinical efficacy of clearing heat and resolving phlegm for AECOPD with the syndrome of phlegm-heat obstruction of the lung. Our findings suggest that therapy for clearing heat and resolving phlegm may effectively control the inflammatory reaction of AECOPD in patients with the syndrome of phlegm-heat obstruction of the lung, especially for those with fever. The safety indicators showed no abnormalities.
The findings of RCTs are recognized as the highest level of evidence. However, RCTs are characterized by application of strict inclusion and exclusion criteria, randomization, blinding, control, and standardized treatments to minimize the effects of confounding factors and to evaluate the therapeutic efficacy of interventions.23–25 This makes RCTs an “ideal” state that cannot reflect the real world, leading to extrapolation in application of the results. Real-world research is usually based on a large sample. According to the patient’s actual conditions and personal willingness, therapeutic methods are selected in a non-random manner. Additionally, long-term evaluation is performed in this research, and it focuses on significant treatment outcomes for further evaluation of external validity and safety of interventions.23–25 Real-world research is closer to medical reality.
Presently, many clinical studies are available regarding clearing heat and resolving phlegm for the treatment of AECOPD with the syndrome of phlegm-heat obstruction of the lung. These studies’ results suggest that clearing heat and resolving phlegm can relieve symptoms, control inflammatory reactions, improve lung function, and improve clinical efficacy.12–16 Most of the evidence from these findings has come from RCTs, and patients >80 years of age, and those with bronchiectasis, bronchial asthma, lung cancer, and other diseases were generally excluded. In clinical practice, middle-aged and older patients are predominant among the COPD population; those aged >80 years are not a minority, and many are accompanied by other respiratory diseases. These patients are often excluded from RCTs, which makes evaluation of TCM treatment of clearing heat and resolving phlegm in the above-mentioned patients difficult. Therefore, for a more realistic medical condition, this study was designed as observational real-world research without strict inclusion and exclusion criteria. Of the 164 eligible patients, those aged over 80 years accounted for 38% of the study population. Patients accompanied by lung cancer, bronchial asthma, bronchiectasis, and interstitial lung disease also accounted for a certain proportion (0.8%–53.3% depending upon the comorbidity).
Our study showed that, after 5 to 7 days of treatment, the decrease in neutrophils and CRP levels in the TCM group was more pronounced, and the duration of defervescence was shorter than that in the control group. These findings indicated that clearing heat and resolving phlegm might play a role in controlling inflammatory reactions. White mulberry root-bark decoction was obtained from the Complete Works of Zhang Jing-Yue, and is effective in clearing lung heat, dissolving phlegm, directing qi downward, and relieving labored breathing, and is often used to treat phlegm-heat respiratory diseases. 26 In the formula, white mulberry root-bark clears and drains heat in the lungs, and drains pulmonary edema, and it has effects of clearing lung heat and relieving difficulty in breathing. Processed Pinellia can dry dampness and dissolve phlegm. 27 Perilla is effective in directing qi downward and dissolving phlegm. 27 Apricot kernel has purifying and descending effects, and can also diffuse lung qi and relieve coughing and difficulty in breathing. 27 Thunberg fritillary bulb clears heat and dissolves phlegm, and descends and drains lung qi. 27 Gardenia and Scutellaria root are effective in clearing and draining lung fire. 27 The combination of these Chinese medicinal herbs can clear phlegm-heat and direct lung qi downward, thereby effectively treating related symptoms. Previous studies have investigated the mechanism of clearing heat and resolving phlegm, mainly including controlling inflammatory reactions by inhibition of inflammation-related cytokines and adhesion molecules, improving airway mucus hypersecretion, and enhancing transporting capacity of antibiotics in lung tissues.17,27–29 Clearing heat and resolving phlegm might control inflammatory reactions and improve clinical efficacy through the above-mentioned mechanisms. With regard to safety indicators, in our study, there were no significant differences in levels of hemoglobin, platelets, creatinine, BUN, ALT, AST, and TBIL at discharge between the two groups. This finding suggested that oral TCM treatment of clearing heat and resolving phlegm did not have an effect on the hematopoietic system and liver and renal function, with good safety compared with Western medicine.
The present study has some limitations. The patients were from a single center and were treated by the same team of physicians, which could have introduced some bias. PSM has the advantage of controlling for confounders between two groups, but at the sacrifice of excluding some patients. 30 As a retrospective study, the data were limited to those available from the medical charts. Moreover, the sample size was not large enough. In the future, relevant clinical studies should be designed, and observational indicators, such as symptoms, blood gas analysis, and lung function, could be included to evaluate the effect of clearing heat and resolving phlegm on pulmonary ventilatory function.
In conclusion, this real-world retrospective study with PSM shows that the therapy of clearing heat and resolving phlegm might effectively control the inflammatory reaction of AECOPD in patients with the syndrome of phlegm-heat obstruction of the lung, especially for those with fever. Additionally, safety indicators show no abnormalities with this therapy. Nevertheless, more large-scale and prospective studies are required to provide a higher quality of evidence.