
Abstract
The aim of this study is to investigate the impact of optimal antihypertensive medication on cognitive function. In this 6-month clinical trial, 248 adults were randomly selected by a registry of hypertensive-treated patients (based on a National Hypertension Treatment Program), followed health centers located in Rafsanjan County, Southeast, Iran. Blood pressure was measured 3 times in each appointment pre- and posttreatment. Mini-Mental State Examination was used for cognitive performance evaluation. Paired t test and multiple regression model showed significant correlation between “the differences of systolic and diastolic blood pressure levels” and “cognitive performance in treated patients more than 40 years old.” Cognitive performance was not significantly different in patients less than 40 years old post antihypertensive treatment. Cognitive performance scores demonstrated significant increase in responders more than 40 years old post antihypertensive treatment. Antihypertensive treatment in responders with age equal or more than 40 years improves the level of cognitive performance significantly.
Introduction
Most of the previous investigations have demonstrated the inverse association between high blood pressure and cognitive performance (CP). 1,2 It is also evident that patients with a chronic disorder such as type II diabetes mellitus having hypertension present greater cognitive decline compared to normotensive diabetic patients. 3
In several clinical trials, antihypertensive treatment with a target of resting systolic blood pressure (SBP) more than 160 mm Hg has decreased the incidence of subsequent dementia in elderly participants with previous normal cognitive function. 4 -7 Conversely, other studies have failed to reveal significant effect of optimal antihypertensive treatment on progression of cognitive impairement. 8,9
The relation between blood pressure and dementia is complicated. Verghese et al demonstrated that low diastolic blood pressure (DBP) is associated with higher risk of dementia in elderly individuals older than age 75, supporting a clear relation between cognitive impairment and age. 6
Forette and colleagues revealed that blood pressure–lowering therapy can protect against dementia in older patients with systolic hypertension. However, Knecht et al reported that relation between SBP and cognitive function has not been fully elucidated. 1 Finally, Di Nucci et al showed the lack of relationship between hypertension and CP in community elderly residents. 10 Controversies and challenges regarding hypertension and cognitive function interaction highlight the need for further well-designed studies.
It is well known that the relation between high blood pressure and CP without age assessment would be misleading, due to the clear effect of age on dementia progression. Interestingly, Elias et al showed that young adults are as susceptible to blood pressure–related longitudinal decline in CP as elderly people. 2 Cognitive performance has also been correlated with other factors such as education. 1 Therefore, the impact of these individual factors should be well defined so as to establish the correlation between hypertension and CP.
More evidence is required to establish the benefit of antihypertensive treatment on cognition performance as Knecht and colleagues stated in their study “how much cognitive benefit could be gained from antihypertensive medication?” 1 In the present clinical trial, we attempted to assess the effect of both optimal systolic and DBP treatment on cognition performance in different age groups.
Methods
This clinical trial conducted to investigate the impact of antihypertensive treatment on CP. The research protocol has been approved by our university ethics committee.
Study Population and Sample
Hypertensive residents of 9 rural and urban health centers located in Rafsanjan County, in southeast, Iran, that were registered on National Hypertension Treatment Program constitute the population of this study. According to the national health program for hypertension control, all people at risk of hypertension should be reviewed in the respective health centers. For a 6-month period, hypertension was confirmed in 492 people of the registered population, whereas 248 people, representing approximately 50% of hypertensive patients, were consented and allocated to the study. Forty-three people of 248 finally did not attend their appointments and were replaced by other hypertensive individuals. Hypertensive participants with one or more comorbidities were excluded.
Measures
Hypertension quality measurements stemmed from a single clinic appointment can potentially misclassify a large proportion of patients. 11 According to the recommendations of the 1988 Joint National Committee, the acquirement of true baseline blood pressure readings may require consecutive measurements in 3 or more separate occasions. In this study, 3 serial BP measurements were performed in each clinical appointment pre - and posttreatment initiation. 12
A specific case report form was used to record demographic and clinical information after obtaining participants’ written consent form by trained expert physicians. Mini-Mental State Examination (MMSE) was used for the assessment of CP of the allocated individuals by trained general practitioners. Cognitive performance was assessed in 2 occasions; initially—when hypertension diagnosis was established and 3 months post antihypertensive treatment initiation when normal blood pressure levels were succeeded.
To minimize the different types of errors, a standard protocol was followed enhancing the accuracy of BP measurements and further the treatment effectiveness. Therefore, all potential sources of errors were accurately controlled, for example, the patient, the observer, and the equipment. 13
Patients were requested to avoid coffee, tea, chocolate and coke consumption, smoking, exposure to cold temperatures, and strenuous physical exertion 30 minutes before the respective blood pressure measurements. They were also advised to wear clothes with loose sleeves, rest 5 minutes in a quiet, comfortable place and report any additional doses of the prescribed or other medication.
Vision and audition of health professionals were previously tested while they were also trained appropriately to follow the recommended techniques for accurate blood pressure measurements (eg, support the patient’s arm, supply a chair with back support, use an appropriately sized blood pressure cuff, check the blood pressure by palpation before auscultation, allow 1 to 2 minutes between readings, and etc). Mercury sphygmomanometers were used, and all necessary precautions about these equipment were regarded.
Hypertension Treatment Protocol
Hypertensive responders in our study were treated according to the widely used strategies. 14,15 Cardioinhibitory drugs including β-blockers were mainly used. Atenolol as a β-blocker with a dose of 100 mL/d along with a diuretic drug, for example, triamterene (25-50 per/d) for a duration of 3 to 6 months was used. All responders were followed up for the duration of the treatment. Respondents, who received further medication or/and changed their lifestyle to control their hypertension, in the treatment duration, were excluded.
Data Analysis
Data were analyzed using SPSS (version 21). Mean pressure levels were calculated by the 3 consecutive measurements obtained for both SBP and DBP in 2 separate appointments of before and after the treatment. A mean difference was also derived from the respective mean of pre- and posttreatment both SBP and DBP readings.
Responders, in the analysis, were divided into the 2 groups based on the reduction in SBP and DBP levels. Treatment success is defined the efficacy of treatment to decrease the levels of SBP and DBP (positive difference). In the following tables, “success” means that the difference between the level of blood pressure before and after the treatment is more than 0 (eg, mean blood pressure level before the treatment − mean blood pressure level after the treatment > 0). “Failure” means the difference between the blood pressure levels before and after the treatment is ≤0 (mean blood pressure level before the treatment − mean blood pressure level after the treatment ≤ 0).
Given the effect of age on the CP and blood pressure, 16 this variable effect was controlled trough data analysis where appropriate. The CP level for each respondent was obtained from adding the individual scores of MMSE and it was further calculated for the 2 occasions before and after the treatment. The difference between the pre- and posttreatment score of MMSE was also calculated. Paired t test was used to compare the mean scores of MMSE as well as the mean scores of SBP and DBP before and after the treatment. Pearson correlation coefficient was also calculated to reveal the correlation between both SBP and DBP with MMSE scores.
In the last section of the analysis, multiple regression model was applied to evaluate the correlation between “the differences of SBP and DBP levels” and “CP mean differences scores” before and after the treatment, when the effects of age and education were controlled in the model.
Results
From a population sample of 492 hypertensive people, data were collected from 248 people who were willing to help with the survey. Mean age of this group was 60.9 ± 11.9 years (min = 28, max = 84 years). Demographic characteristics of responders based on the gender are presented in Table 1. Notably, 77% (n = 192) of responders were women. More than 48.8% (n = 117) of patients responding to antihypertensive therapy were equal or older than 60 years. About three-quarters of responders were employed (n = 184), and the majority (88.5%, n = 216) demonstrated an educational level of primary school or lower. Only 6.5% registered as smokers, 5.4% were living alone and approximately 95% (n = 177) of responders with available height and weight measurements had a BMI over 20 (n = 170).
Demographic Characteristics of Respondents in the 2 Groups of Men and Women.
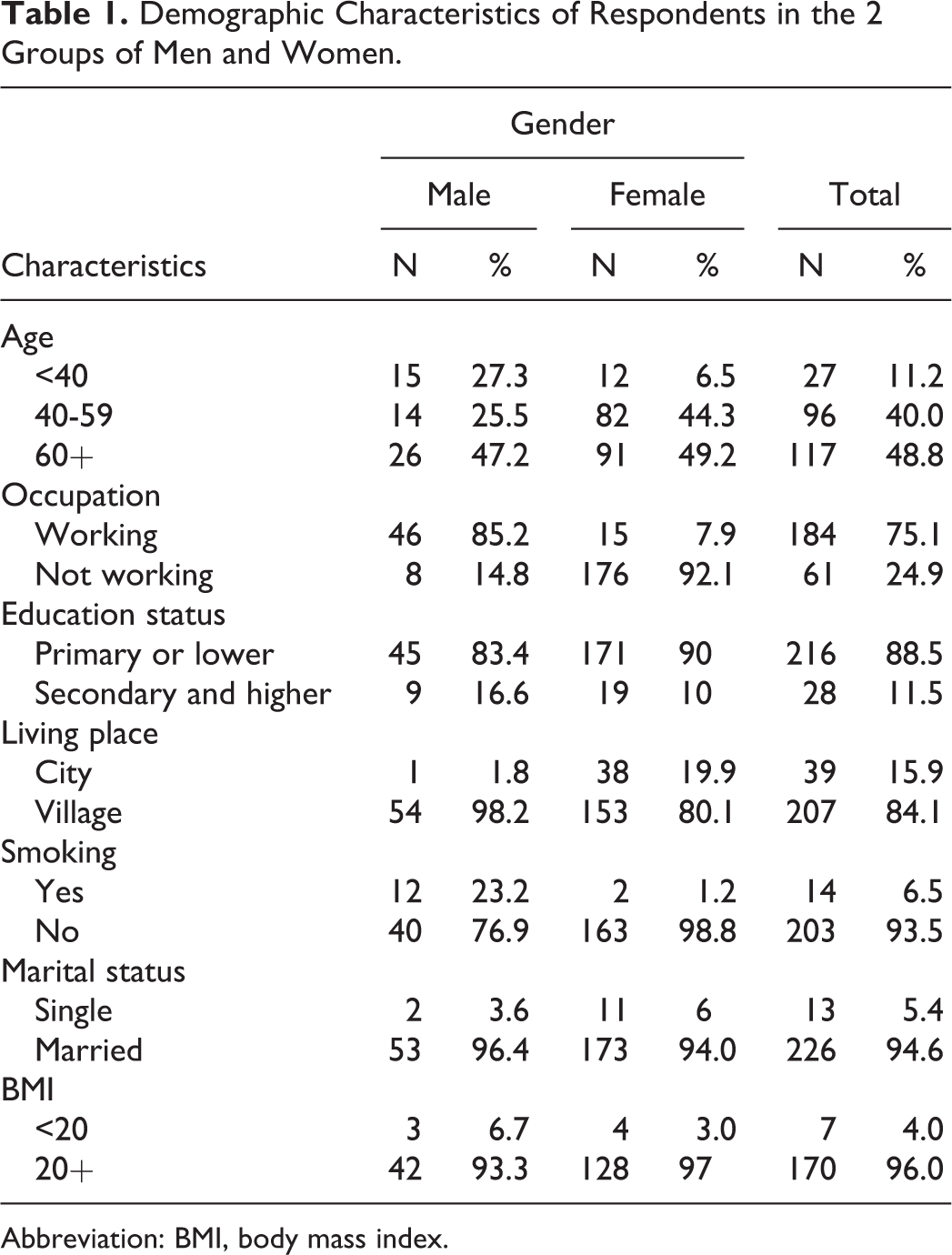
Abbreviation: BMI, body mass index.
According to the results of this study, 58% (n = 134) of responders reported a family history of hypertension, whereas 31.1% (n = 71), 28.7% (n = 64), and 40.9% (n = 94) presented a positive family history for coronary artery disease, stroke, and diabetes, respectively.
Among all responders (n = 248), mean levels of SBP and DBP before the treatment were 163.6 ± 10.9 (min = 115, max = 196.7) and 95.1 ± 9.7 (min = 66.7, max = 115), respectively. Mean levels were reduced in responders to antihypertensive therapy to 133.4 ± 10.9 (SBP, min = 106.7, max = 175) and 79.9 ± 5.7 (DBP, min = 63.3, max = 100), respectively. We divided responders into the 2 groups based on the success in hypertension treatment program: (1) responders whose hypertension was successfully treated (based on SBP and DBP) named success group, (2) responders whose hypertension was not successfully treated (based on SBP and DBP) named failure group.
Table 2 shows the mean levels of SBP and DBP among responders before and after the treatment in the 2 groups of success and failure. The results of paired t test showed significant differences in both SBP and DBP mean levels, further demonstrating a positive significant difference in SBP and/or DBP after the treatment (success or positive difference means; blood pressure [SBP and/or DBP] before the treatment − blood pressure [SBP and/or DBP] after the treatment > 0).
Mean Levels of SBP and DBP Among Respondents Before and After the Treatment Based on the Results of the Treatment.
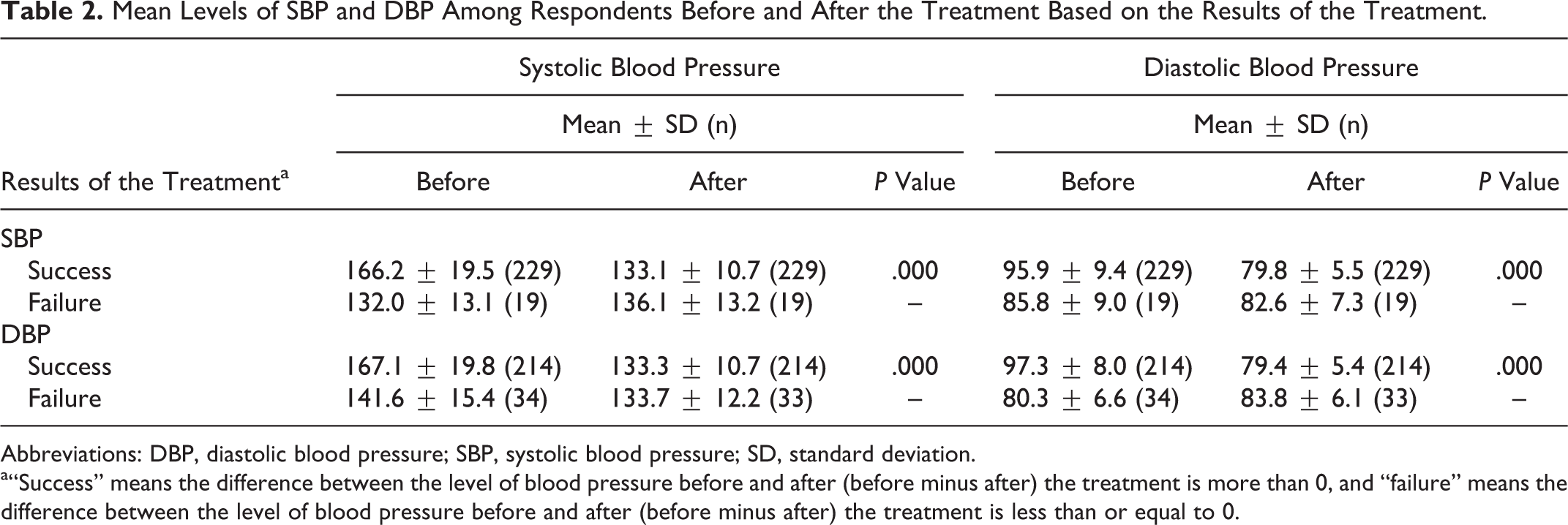
Abbreviations: DBP, diastolic blood pressure; SBP, systolic blood pressure; SD, standard deviation.
a“Success” means the difference between the level of blood pressure before and after (before minus after) the treatment is more than 0, and “failure” means the difference between the level of blood pressure before and after (before minus after) the treatment is less than or equal to 0.
Table 3 presents the mean scores of CP among responders based on the results of hypertension treatment. As it is presented in Table 3, the mean CP scores before and after the treatment of hypertension among respondents with SBP difference more than 0 were 28.1 ± 2.9 and 28.9 ± 2.7, respectively. Paired t test results showed that the mean CP score of responders was significantly higher before compared to posttreatment initiation (t = 4.2, df = 228; P = .000). Whereas, this difference in respondents with a mean SBP difference less than or equal to 0 was not significant.
Mean Scores of Cognitive Performance Among Respondents Before and After Treatment Based on the Results of Hypertension Treatment.
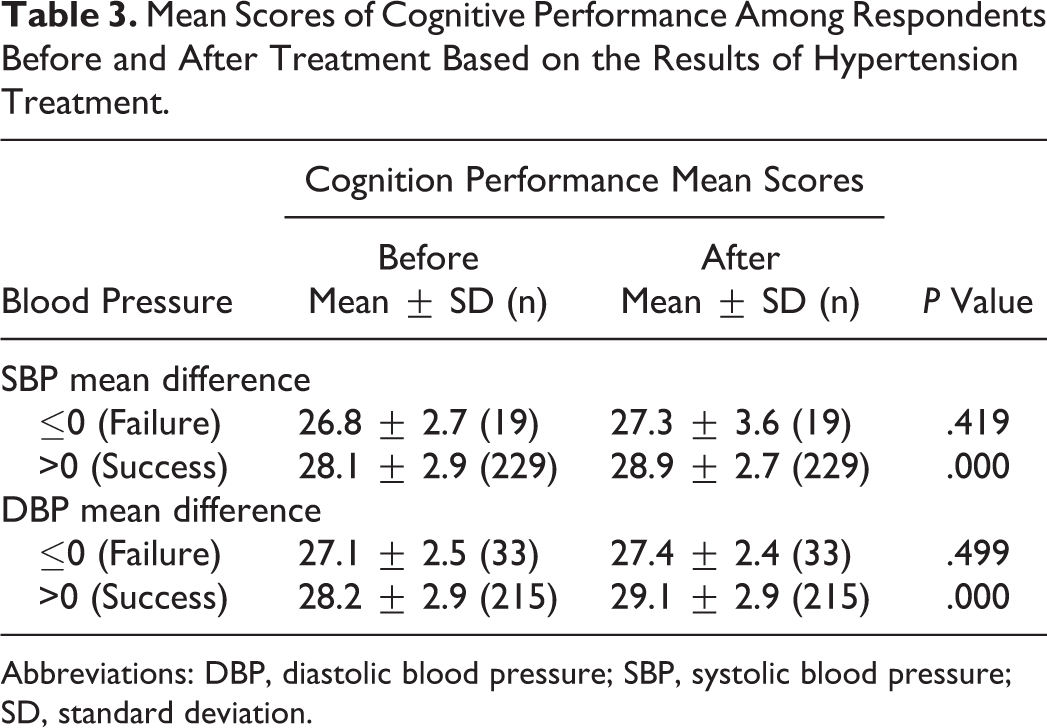
Abbreviations: DBP, diastolic blood pressure; SBP, systolic blood pressure; SD, standard deviation.
The pre- and posttreatment CP mean scores were also compared between the responders with DBP mean difference >0 and DBP mean difference ≤0. Cognitive performance mean score was significantly increased posttreatment in patients with mean DBP difference >0 (t = 4.2, df = 214; P = .000).
Due to well-known effect of age on CP scores of responders, responders were further divided into the following 3 age groups: <40 years, 40-60, and >60 years old. Table 4 contains information about the average scores of CP among responders with SBP mean difference >0 and DBP mean difference >0, before and after the treatment based on responders’ age.
Mean Scores of CP Among Respondents With SBP Mean Difference and/or DBP Mean Difference More Than Zero in Different Age Groups.
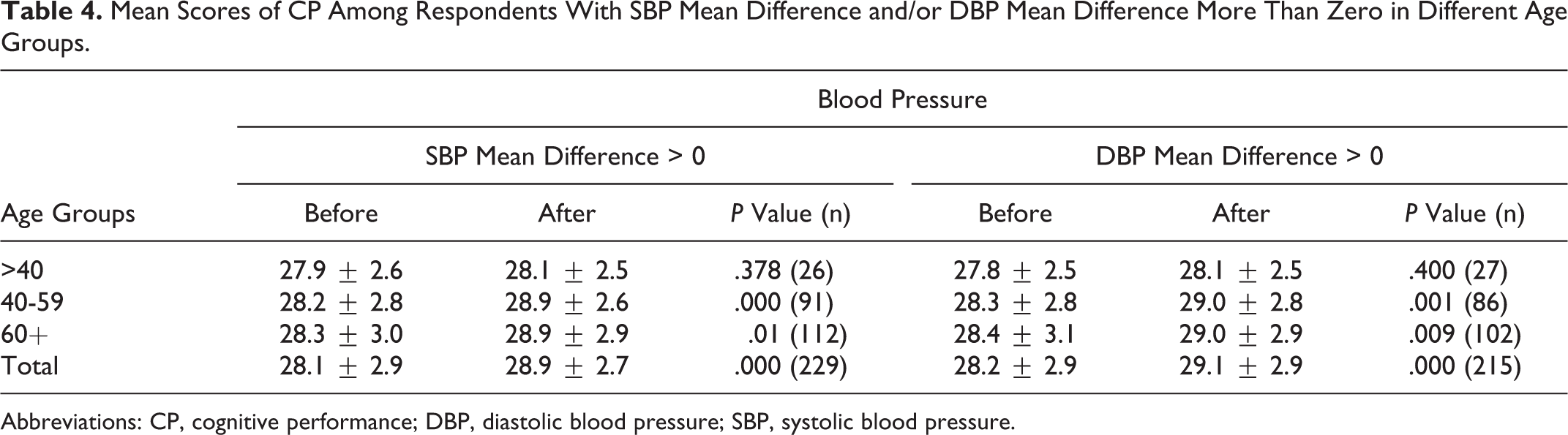
Abbreviations: CP, cognitive performance; DBP, diastolic blood pressure; SBP, systolic blood pressure.
Mean scores of CP in responders less than 40 years old before (27.9 ± 2.6 and 27.8 ± 2.5 in responders with mean SBP and DBP difference >0, respectively) and after antihypertensive treatment were not significantly different (28.1 ± 2.5 in both groups of respondents with SBP and DBP mean difference > 0, respectively; Table 4).
Whereas, the mean scores of CP among respondents in the other 2 age groups (40-59 and 60+ years old) following antihypertensive treatment were significantly increased in responders with SBP and DBP difference >0 (Table 4).
The results of multiple regression analysis revealed significant correlation between CP scores and both SBP (ρ = 0.357; P < .000) and DBP (ρ = 0.309; P < .000) mean differences.
Multiple regression model equations were also derived from the correlation between CP as well as SBP and DBP scores of mean differences (Figure 1).
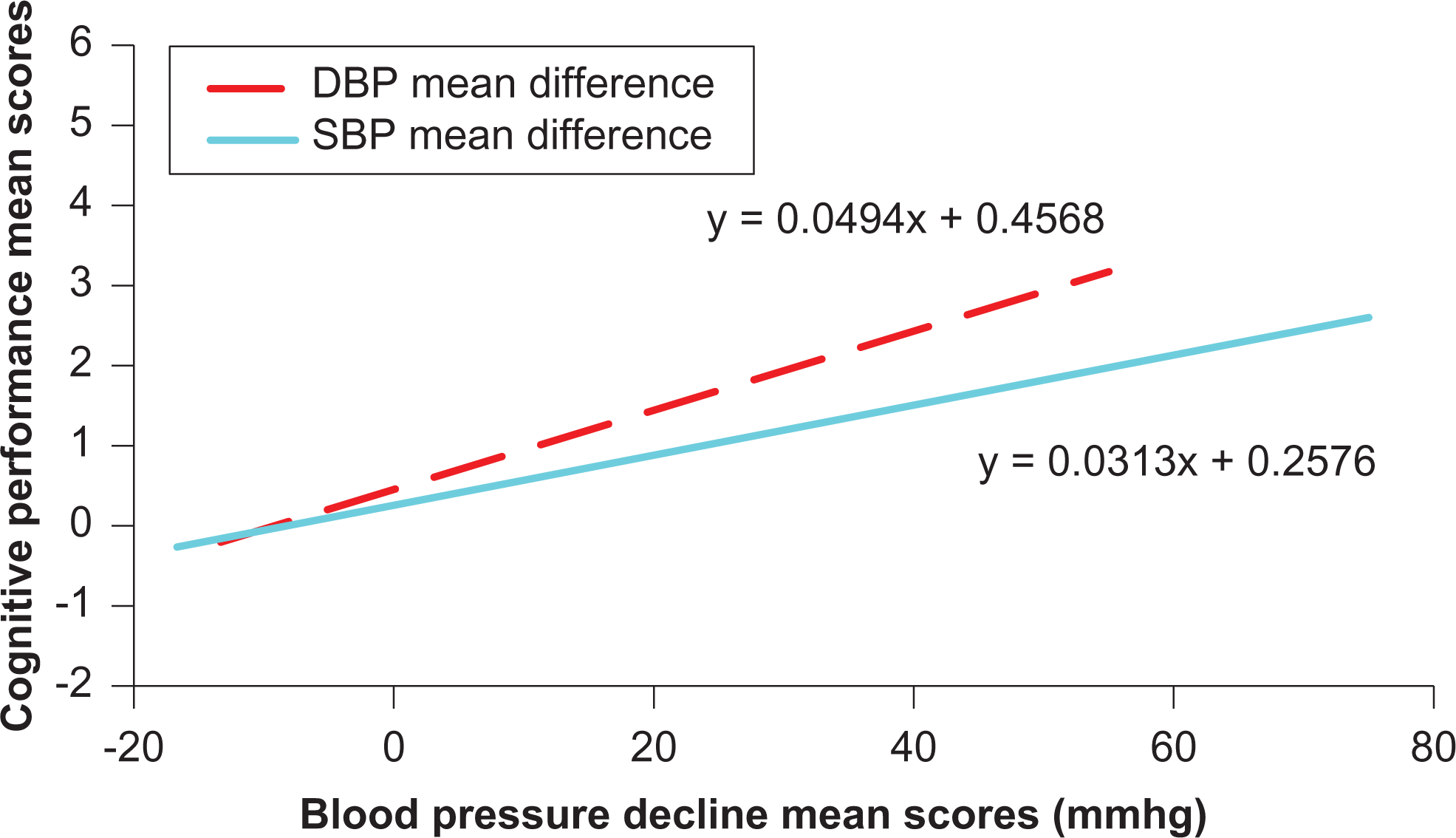
Multiple linear regression between mean scores of cognitive performance differences and both systolic blood pressure (SBP) and diastolic blood pressure (DBP) mean differences among respondents.
Discussion
In the present study, we evaluated the CP of hypertensive participants’ pre and post antihypertensive treatment initiation. All treated patients in our study were under the National Hypertension Treatment Program. Interestingly, several hypertensive patients did not comply with the treatment protocol properly. Poor adherence to medical regimens could be the main reason as it was proposed by Jacobs and colleagues. 17 Since the aim of the study was to assess the effect of hypertension on cognitive function decline, responders were divided into 2 groups based on treatment effectiveness on SBP and/or DBP reduction. The level of cognitive function was evaluated pre- and post the treatment initiation in patients succeeded a SBP and/or DBP decrease. These results were compared with the respective CP changes in patients that were demonstrated no reduction in their BP (SBP and/or DBP). Statistical comparison confirmed significant effect of the treatment protocol on reduction in both SBP and DBP, among a big proportion of responders in our study (for SBP; 229 of 248 and for DBP; 214 of 247).
The level of CP in responders to antihypertensive therapy was improved significantly. Whereas, nonresponders to antihypertensive therapy did not reveal any improvement in their cognitive function levels. These results confirm the findings of Franceschi and colleagues that initially reported the effect of hypertension on CP. 18 Knecht and colleagues revealed a linear negative correlation between SBP and cognition. 1 In our study, we attempted to assess how much cognitive benefit could be gained from antihypertensive medication started in mid- rather than late life. Our results demonstrated that responders to antihypertensive treatment belonged to age groups of 40 to 59 and ≥60 years present significant CP improvement after treatment initiation. On the contrary, responders to antihypertensive therapy less than 40 age did not reveal any significant improvement in their CP confirming the statement of Elias and colleagues 2 that elderly patients could present greater BP-related cognitive decline than younger adults.
Our results are also in concordance with the results of Harrington and colleagues that showed that older participants with hypertension may have impaired cognition in a broad range. 19 However, the abovementioned study concluded that antihypertensive treatment might not necessarily reduce cognitive decline, fact that is against with our results.
It has been demonstrated that hypertensive participants are approximately 10% slower in psychomotor tests compared with normotensive participants. 19 In our study, in a reverse approach, we showed that the treatment of hypertension in older responders can result in a greater influence on their CP comparing to younger responders.
Our results demonstrated a significant reduction in both SBP and DBP in about 92% and 87% of responders to antihypertensive therapy resulting in significant CP improvement, respectively. Whereas, CP revealed no difference in nonresponders to antihypertensive therapy. Forette and colleagues concluded that antihypertensive therapy with calcium channel blocker nitrendipine in elderly reduces dementia incidence by 50%. 20 Fact that further supports the impact of treating hypertension on the CP, proven in both our study and Tzourio and colleagues’ trial. 21 The design of our study is consistent with other studies in the hypertension field, 1,19 suggesting the CP evaluation in antihypertensive-treated individuals.
Based on the regression model equations obtained from our data, it is possible to predict the degree of CP improvement in relation to SBP or DBP reduction. For instance, based on this model, it is evident that a decrease in SBP equal to 20 mm Hg would be accompanied by CP improvement corresponding to 0.8836 on the respective MMSE scores. The community-based clinical trial design, the wide age range, serial blood pressure measurements (3 times with 1 hour interval on the day of examination), and standard approach increase the study’s power. Since in this study, each responder was acting as control to himself before and after the treatment, further minimizing the effect of any confounders.
There were some limitations in our research including the probability of having a learning effect of using MMSE for more than one occasion. Although, it might happen when using all measures for more than once, our trained experts (General Practitioners) were asked to use the flexibility of the MMSE items to minimize learning effect.
More clinical studies should be performed to support further our results and to reveal the pathophysiological mechanisms of antihypertensive therapy on inhibition of cognitive dysfunction. Based on the results of our study, dementia might be prevented in mid and later age-treated patients by establishing regular hypertension control and early treatment in community. Further attempts should be made in community level to prevent and to control high blood pressure, in particular, among high-risk groups.
Perspectives
The present community-based study revealed linear correlations between decreasing both “SBP and DBP” and improving “cognition performance.” However, when responders were classified based on their age, our findings illustrate that hypertensive-treated patients less than 40 years old would not demonstrate a statistically significant improvement in CP, compared to responders >40 years old, in whom antihypertensive treatment correlated with significant CP improvement. This process might show that controlling hypertension could be helpful to postpone dementia among older people. It is mentioned that cognitive dysfunction due to hypertension can be accounted for the subsequent cognitive dysfunction 22,23 that could be partly improved post high blood pressure treatment in older age. Therefore, additional molecular studies are needed to establish the effect of hypertension treatment on the inhibition of cognitive dysfunction.
Footnotes
Authors’ Note
All the authors imply that the work described has not been published previously and they also, imply that if it accepted, it will not be published elsewhere in the same form, in English or in any other language.
Acknowledgments
The authors thank all respondents who accepted to help with this work. The authors also appreciate the valuable help we have received from general practitioners in recruiting responders and data collection process.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Rafsanjan University of Medical Sciences, Social Determinants of Health Research Centre, financially.