
Abstract
Objective
To investigate the independent and synergistic associations between abdominal obesity, chewing difficulty and cognitive impairment in a community-dwelling older adults sample in China.
Methods
Cognitive function was measured by the 5 min- Montreal Cognitive Assessment (5 min-MoCA) and abdominal obesity was measured by A Body Shape Index (ABSI) in 572 participants recruited from local communities. Chewing difficulty was assessed via a self-report questionnaire. Linear regression and general logistic regression were performed to investigate the association of chewing difficulty and abdominal obesity with cognition.
Results
Chewing difficulty score [β (95% CI) = −.30 (−.49, −.11)] and ABSI [β (95%CI) = −.30 (−.55, −.05)] were independently associated with worse performance on the 5 min-MoCA. Whilst ABSI was not associated with cognitive impairment, the co-existence of chewing difficulty and abdominal obesity [OR (95% CI) = 2.22 (1.18, 4.17)] was found associated with the presence of cognitive impairment.
Conclusion
Chewing difficulty and abdominal obesity were independently associated with cognition. Abdominal obesity and chewing may have an additive effect on cognitive function.
Significance Statement
1. Although indicators such as nutrition are thought to promote cognitive function, statistical indicators reject the hypothesis that there may be a common mechanism between mastication difficulties and abdominal obesity to arise cognitive impairment. 2. In the meantime, our study applies A Body Shape Index as an indicator measuring abdominal fat, exploring the potential application of this recent tool. In the long term, our study helps to review the existing research on chewing difficulty, abdominal obesity and cognitive function and provide insights for further studies, that is we could dive into a meticulous examination into preexist independent association and try to match them.
Introduction
Dementia is a neurodegenerative disease associated with accelerated aging. Once developed, dementia patients require lifelong care and have a high risk of a series of adverse prognoses like hospitalization, disability, or even death, bringing a tremendous burden on families and society.
The older population goes through physical aging naturally, and exploring potentially important signs in the body’s aging process to predict dementia risk is gaining increasing attention. Chewing difficulty is one of the vital problems that could impose long-term changes on cognition and the physical body, 1 but its relationship with cognition remains vague. Some studies reported that chewing dysfunction is associated with cognition decline in the older population,2–4 a 2-years follow-up study demonstrates that the older adults whose masticatory function is improved have better cognitive performance, 5 whereas others show opposing evidence. 6 Memory and decision-making difficulties have been reported to be associated with subjective discomfort in older adults, 7 which may in turn have an impact on their dietary preferences. 8 Moreover, elderly individuals with poorer subjective masticatory function not only exhibited decreased cognitive performance. 9 but also showed a greated likelihood for subjective cognitive complaints in the long-term. 10
Discussions around the interplay mechanism of chewing difficulty and cognition are scarce of explicit explanation. Nutrition intake is one of the potentially interactive factors. Some articles suggest that chewing ability may influence nutrition intake since the constitution of diet is altered, which could ultimately contribute to obesity, especially in the abdominal area of the body.11,12 Meanwhile, people with obesity shows variation in their chewing behavior, including eating rate, biting size etc. 13 A study uncovers that individuals who have excess weight are observed with notable changes in masticatory behavior and chewing ability, 14 indicating the effect could be mutual. Further, recent findings suggest that abdominal obesity demonstrates a higher risk for dementia than general obesity, namely despite normal or abnormal body mass, the older adults with abdominal obesity are more likely to develop into dementia.15–17 Traditionally, BMI serves as the most common indicator in reflecting body mass. To examine abdominal obesity more accurately, our study introduces the A Body Shape Index (ABSI). ABSI is an indicator integrating height, weight, and waist circumference, which possesses a higher ability to remedy the shortcomings of traditional anthropometric indicators on reflecting abdominal obesity. 18
Previous research has highlighted the independent association of chewing ability, abdominal obesity and worse cognition among older adults, respectively. However, till present, few research has investigated the relationship between chewing ability and abdominal obesity, as well as how their relationship affect cognition among older adults.
Therefore, the present study examined the independent and interactive associations between abdominal obesity, chewing ability and cognition. We hypothesized that 1) severer chewing difficulty and worse ABSI were independently associated with worse cognition; 2) when respectively controlling for ABSI and chewing difficulty, their association with cognition disappeared accordingly.
Methods
Study Population
Participants were recruited from 2 local communities in Hangzhou, Zhejiang. Inclusion criteria were: 1) Age ≥50 years; 2) Dementia-free; 3) No major diseases; 4) Capable to complete medical investigation. Exclusion criteria were: 1) Patients with malignant diseases (cancer, etc.); 2) Demented patients; 3) Severe visual or verbal impairment. A total of 572 participants entered the final analysis (Figure 1). Flowchart for the research.
This study was approved by Medical Ethics Committee in Zhejiang University School of Public Health (ZGL202101-1) and written informed consent was obtained from all participants or their legally acceptable representatives.
Cognitive Function Assessment and Diagnosis
The 5 min- Montreal Cognitive Assessment (5 min-MoCA) and Clinical Dementia Rating (CDR) were performed to measure participant’s cognitive function. The 5min-MoCA (total score 12) is designed based on memory, verbal fluency and orientation, and has been validated that it can be widely used in a large-scale community screening of the older adults population. 19 The cutoff for cognitive impairment of 5 min-MoCA was measured by CDR, the golden criteria for dementia diagnosis and whose application in China has been validated. 20 The cutoff for cognitive impairment of 5 min-MoCA was ≤7, with a sensitivity of .87 and specificity of .82. All cognitive function measurements were conducted by trained researchers in the preferred language/dialects of the participants.
Abdominal Obesity Assessment
Physical measurements was conducted to assess height(m), weight(kg) and waist circumference (WC, m),
21
rounded to .01 m, .1 kg, and .01 m, respectively. Height was measured with participants bear feet, standing straight with back against the wall. Weight was measured with participants took off heavy clothes and carrying no heavy object. Waist circumference was measured at the level of the midpoint between the lower rib margin and the iliac crest.
21
All measurements were administrated by uniformly trained health workers. BMI and A body shape index (ABSI) were calculated by following functions
22
:
Abdominal obesity was defined using ABSI. A receiver operator characteristic curve was conducted to determine the cutoff of ABSI and estimate the corresponding sensitivity and specificity, taking WC as golden criteria. The Chinese criterion of abdominal obesity was defined as WC ≥.9 m in male and ≥.85 m in female. 23 The cutoff for abdominal obesity defined by ABSI was ≥.085, with an area under the curve = .74, and a Youden index of .57.
Chewing Difficulty Assessment
Self-reported chewing difficulty was measured through the chewing difficulty questionnaire with following questions: 1) ‘Do you have any kind of chewing difficulty?’. If the answer is ‘Yes’, then participants would be asked for two more questions: 2) ‘Do you eat less food than before because of chewing difficulties?’; 3) ‘Do you change the texture or type of food because of chewing difficulties?’. Each question counts for one point and the total chewing difficulty score was added up into four levels (0, 1, 2, 3). Every ‘Yes’ answer would add one point to the total score and higher score represents more serious chewing difficulty. Participants who had ‘Yes’ answer to the first question ‘Do you have any kind of chewing difficulty?’ were defined as having chewing difficulty.
Covariates
Participants’ age, sex, highest educational level, past smoking history, past drinking history, and cardiovascular disease history were collected through a questionnaire and administrated by trained health workers.
Statistical Analysis
For descriptive analysis, continuous variables were represented as mean ± standard deviation and categorized variables were represented as the number of cases (%). Comparisons between the normal cognition group and cognitive impairment group were made using analysis of variance for continuous variables following normal distribution, using rank sum test for continuous variables following skewed distribution, or using chi-square test for categorical variables.
To estimate the associations among abdominal obesity, chewing difficulty, and cognitive function, ABSI, chewing difficulty score, and 5min-MoCA score were measured continuously. A multiple linear regression model was performed, adjusting for participant’s age, sex, highest educational level, smoke history, drink history, cerebrovascular diseases history and heart disease history, with effect size demonstrated as β-values (95% CI).
To estimate the interactive effect between abdominal obesity and chewing difficulty, abdominal obesity and chewing difficulty were further adjusted in the linear models respectively. As model used in estimating the association of abdominal obesity with cognitive function was further adjusted for chewing difficulty, and model used in estimating the association of chewing difficulty with cognitive function was further adjusted for abdominal obesity. Additionally, the association of abdominal obesity with cognitive impairment was further estimated after stratified by chewing difficulty. The interactive effect is considered existing when the effect size after adjustment or stratification differs from the effect size before adjustment or stratification. Moreover, a chi-square model was performed to examine the association between chewing difficulty and abdominal obesity, with P < .05 considered as existing inter-group difference.
To estimate the risks of cognitive impairment from abdominal obesity and chewing difficulty, a general logistic model was performed, adjusting for participant’s age, sex, highest educational level, past smoking history, past drinking history, cerebrovascular diseases history and heart disease history, risks were demonstrated using OR (95% CI). All analyses were performed using SAS 9.4, with a significant level at P < .05.
Results
Demographic Characteristics of Participants
Demographics of the Study Population in Abdominal Obesity Analysis According to Cognitive Function.

Abbreviations: SD, standard deviation; WC, waist circumference; ABSI, A body shape index; 5min-MoCA, 5 minutes Montreal cognitive assessment; ANOVA, analysis of variance.
Note: Inter-group comparisons were made by one-way ANOVA for continuous variables following normal distribution, rank sum test for continuous variables following skewed distribution, and chi-square test for categorical variables.
Associations Among Abdominal Obesity, Chewing Difficulty and Cognitive Function
Interactive Relationships Among Chewing Difficulty, Abdominal Obesity and 5 min-MoCA Score, and Correlation of Chewing Difficulty With 5 min-MoCA Score According to Abdominal Obesity.
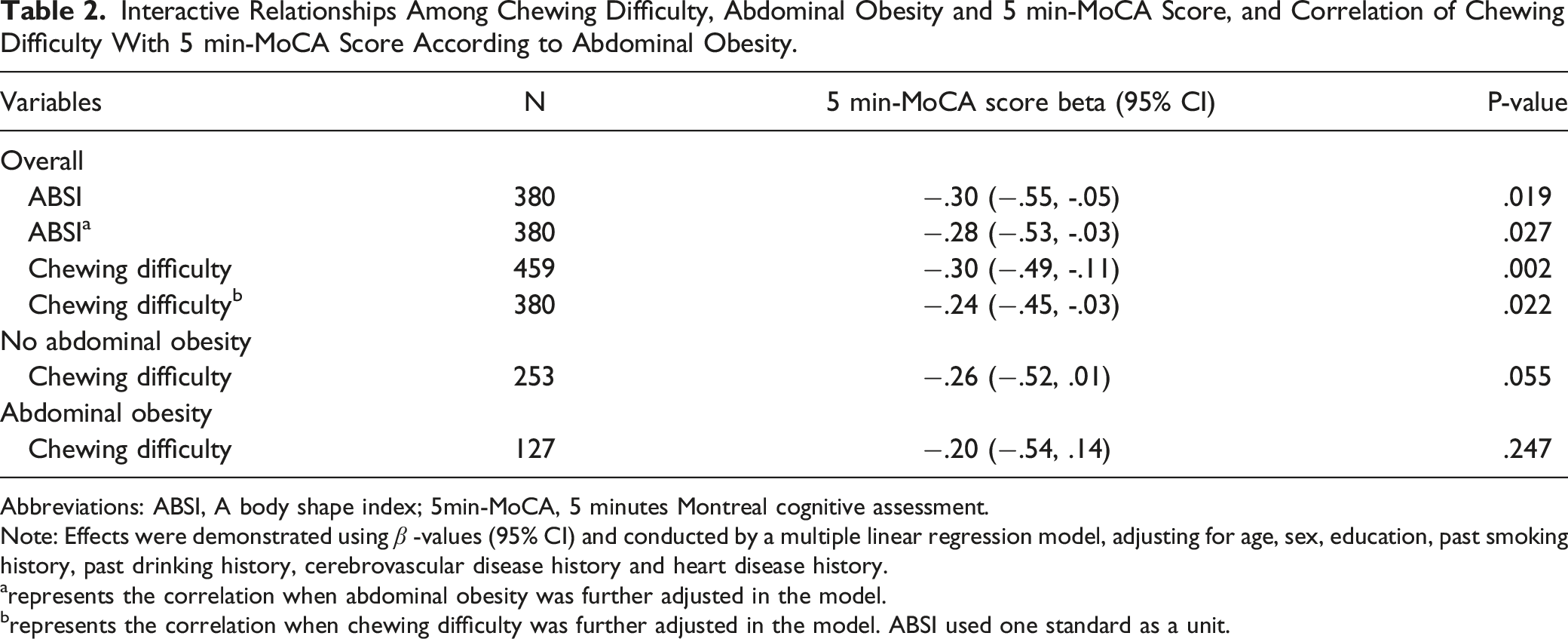
Abbreviations: ABSI, A body shape index; 5min-MoCA, 5 minutes Montreal cognitive assessment.
Note: Effects were demonstrated using
arepresents the correlation when abdominal obesity was further adjusted in the model.
brepresents the correlation when chewing difficulty was further adjusted in the model. ABSI used one standard as a unit.
Association Between Co-Existence of Abdominal Obesity and Chewing Difficulty, and Risk of Cognitive Impairment
Risks of Abdominal Obesity Chewing Difficulty, and Possessing Both on Cognitive Impairment, and Risk of Chewing Difficulty on Cognitive Impairment According to Abdominal Obesity.

Note: Risks were demonstrated using OR (95% CI) and conducted by a general logistic regression model, taking ‘normal cognition’ group as reference, adjusting for age, sex, education, past smoking history, past drinking history, cerebrovascular disease history and heart disease history.
arepresents the correlation when chewing difficulty was further adjusted in the model.
brepresents the correlation when abdominal obesity was further adjusted in the model.
Discussion
This study examined the association of cognitive function with chewing ability and abdominal obesity, and discovered that chewing difficulty, as well as abdominal obesity, was associated with cognitive impairment. On top of that, no synergistic effect was found between chewing difficulty and abdominal obesity.
In our study, the prevalence of cognitive impairment was 30.2% and was higher than some of the reported prevalence in Western countries (20.3%). 24 This inconsistency was also found in previous studies, indicating that east Asia, especially developing countries, has the highest cognitive impairment prevalence worldwide region.25,26 The discrepancy may derive from a lower education level and more lifestyle risk factors of the population in the corresponding regions. 25
The prevalence in our study sample vs the national prevalence of cognitive impairment in Chinese older adults was 30.2% vs 21.8%. 25 Nonetheless, previous studies were conducted in the Chinese population aged 60 and above, 25 while our study sample had a median age of 72 years old. Older age is an accepted risk factor for cognitive impairment and may contribute to the increased prevalence in our study. 27 When compared with studies with a study sample of similar age, our prevalence was within the range of the precedents (27.8%-33.6%).4,28,29
Our results principally revealed independent negative associations in chewing difficulty and ABSI with cognition, but not in abdominal obesity. The older adults with chewing difficulty had a lower 5 min-MoCA score and were prone to have cognitive impairment, corroborating the finding in previous studies.2–4 Some studies regarded chewing ability and abdominal fat as independent risk factors for cognitive function.11–13,24,25 Even though much evidence has supported the association between cognitive function and chewing ability, there is still a lack of explicit explanation about the interplay mechanism of chewing difficulty, abdominal fat and cognition.
Changes in cognitive function could be attributed to chewing ability in two aspects, diverging into direct or indirect effect which is induced by chewing dysfunction. Directly, chewing difficulty could account for hippocampus dysfunction and the Hypothalamic-Pituitary-Adrenal (HPA) axis hyperactivity, leading to cognition impairment. The effect could lie in specific domains of cognition, such as spatial learning and memory deficits. Also, sustained chewing difficulty is served as a chronic stress exposure, causing damage to hippocampal neurogenesis. 30 In addition to the HPA axis, chewing increases basal blood flow to cognitive areas of the brain such as the prefrontal cortex, sensory and insular cortex, striatum, thalamus, cerebellum and hippocampus through sensory and motor nerves, maintaining normal brain function. 31 Due to oral disease, the balance of gut microbe might be interrupted, which is also considered to be associated with cognitive function. 30
Nutrition intake is also a contributive factor to cognition. 32 Based on previous evidence, studies are interested in the association between dietary changes caused by chewing difficulty and cognitive function. A study in Japanese older adults groups has revealed dietary hardness is related to cognitive performance. It discovers significance between nutrient intake and cognition, but fails to reveal individual nutrient contributed to better cognitive performance independently. 12 Furthermore, a treatment designed for older adults subjects with mild cognitive impairment has proved that oral folic acid and vitamin B12 could improve cognitive performance and inflammation levels, which are scanty in group with chewing difficulty. 33 Besides malnutrition, food insecurity also exerted negative influence on cognition. 34
In a nutshell, the masticatory function could, directly and indirectly, be related to cognitive level, which can indirectly reflect the mediating effect through nutritional status and activities of daily living. 35 Nutrition-induced comorbidities also could be a risk factor for cognitive function. 30 Obesity and cognition could cause a change in subjective behavior such as seeking a dentist’s help and sustaining oral health, resulting in deteriorated chewing difficulty.36,37 Self-assessed method in chewing ability was proved to be reliable in other country. 38 Nevertheless, the subjective and objective method of chewing difficulty still needs to be meticulously reviewed. 39 Therefore, more studies excluding confounding factors are required to explore the association between cognition, chewing ability and abdominal obesity.
As for the correlation between abdominal obesity and cognition, ABSI was negatively correlated with cognitive function in our study, whereas no association between abdominal obesity and cognitive impairment was found. This result differs from some precedents finding that abdominal obesity is a risk factor of cognitive impairment,15–17 but there still exist many studies denied such association. 40 The paradox involves several physiological mechanisms. Abdominal obesity reflects visceral fat, which can contribute to insulin resistance, lifted blood insulin level, and further damage cognition. 41 Nonetheless, elevated testosterone or estrogen levels provide merits in improving cognition. For instance, estrogen can degrade inflammation level on cerebral microvasculature and blood-brain barrier cells; and exert protection on mitochondria from oxidative phosphorylation and ATP decline. 42 Therefore, the general role that abdominal obesity plays in cognition changing remains vague. Furthermore, more precise instruments like computed tomography scan or magnetic resonance imaging could have a better assess to abdominal fat, 43 which also should be take into account in the future study. Previous studies assumed that decline of BMI in older adults group bode the incurrence of dementia, 44 however, no solid evidence reveal the role of abdominal fat in weight loss process.
Several studies have noticed the relationship between chewing ability and abdominal fat. Oral health, number of functional teeth, and self-reported chewing difficulty are regarded as risk factors for general and central obesity.36,45 Our study found that although the crude chi-square test revealed an association between chewing difficulty and abdominal obesity, no interactive effect was found. Faster Eating rate and the larger amount of chewing are considered attributions to obesity, 13 other studies have yielded different result. 46 More importantly, There may be the same mechanisms underlying different cognitive risk factors, and by studying their interactions, we may be able to gain a deeper understanding of their mechanisms, which is what our study seeks to reveal.
The limitation of this study lied in the following aspects. This study was a cross-sectional study and therefore was unable to infer a causal relationship between chewing, cognition and abdominal obesity. There is the possibility that cognitive impairment may cause decreased nutrition intake and bad chewing ability, due to memory decline and lack of self-care ability. 15 Additionally, self-assessment of chewing difficulties may not fully reflect the true condition. It has been suggested that older adults with cognitive impairment may overestimate their masticatory function, which may also have an impact on the validity of the self-assessment. 47 Furthermore, the criteria for difficulty chewing are not exclusive. Objective factors, subjective perceptions, and eating habits can all affect chewing condition, which could exert an influence on nutrient intake and body shape. Last but not the least, the sample size included in this study was small, and that the prevalence of CI was higher than previous Western-based studies, which may have limited the generalizability of the study results.
In conclusion, our study validated the association between chewing difficulty and cognitive impairment, but failed to duplicate the association between abdominal obesity and cognitive impairment. Besides, we did not detect an interactive effect between chewing difficulty and abdominal obesity, the effect of chewing difficulty and abdominal obesity on cognition may be independent. To further explore the mechanism and passage that chewing difficulty take in affecting cognition, more longitudinal studies, and studies that take subjective measurement on chewing ability are wanting.
Conclusion
After controlling for abdominal obesity, the initially demonstrated significant association between chewing difficulty and cognitive impairment was gone, indicating there is no synergistic effect. In addition, abdominal obesity and chewing may have an additive effect on cognitive function. Longitudinal studies and objective measurements on chewing ability are warrant to explore the association among chewing difficulty, abdominal obesity and cognition among older adults.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: In the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National nature science fund (Project ID: 72274170), Zhejiang University and Fundamental Research Funds for the Central Universities and Fundamental Research Funds for the Central Universities.