
Abstract
Family caregivers of elders with dementia often face the challenging behaviors of nighttime agitation, sleep disturbances, and urinary incontinence. To date, no study has examined the interrelationships of these behaviors in community-dwelling persons. This single group, descriptive study employs wireless body sensors to objectively collect data on nighttime agitation, sleep, and urinary incontinence in patients with dementia in their homes over a 5- to 7-day period. The aims are to (1) examine the feasibility and acceptability of the use of body sensors in community-dwelling persons with dementia; (2) describe patterns of nocturnal agitation, sleep continuity and duration, and nighttime urinary incontinence; and (3) examine the relationships among nocturnal agitation, sleep continuity and duration, and nighttime urinary incontinence. Data collection is in early stages and is still in progress. Challenges and advantages from preliminary data collection are reported.
Introduction
Nighttime agitation in persons with Alzheimer’s disease and related dementia (ADRD) is highly burdensome and costly for caregivers and for the health care system. Family caregivers report that coping with nighttime agitation and associated sleep disturbances in their care recipients with dementia can be overwhelming and that these disturbances are often a “tipping point” for seeking institutional care for their loved ones. 1 Likewise, findings confirm that the care requirements for urinary incontinence (UI) tax already burdened caregivers. 2,3 The result is that many family caregivers and formal caregivers believe that nighttime agitation, sleep disturbances, and UI are all a normal part of the progression of ADRD. As such, they seek pharmacologic assistance for handling these disruptions or choose to accept the disruptions and do not adequately intervene to prevent the disruptions.
Although there is anecdotal evidence of the relationship among incontinence, sleep disturbance, and agitation, UI is thought to often trigger awakening from sleep with subsequent agitation of persons with ADRD although there is a lack of systematic evidence that these phenomena are related. If confirmed relationships exist among nighttime agitation, sleep disturbances, and UI, interventions such as regularly waking persons to toilet should reduce nighttime agitation, sleep disturbances, and UI in persons with ADRD delaying institutionalization and resulting in substantial savings in the cost of caring for many persons with Alzheimer’s disease (AD) as well as related dementias.
In our previous work, less frequent toileting of persons with cognitive impairment resulted in higher rates of bed-wetting. The greater the degree of cognitive impairment, the greater the rate of bed-wetting. 4 Although not confirmed, we believe that bed-wetting may prompt sleep disturbances and thus increase nighttime agitation in persons with ADRD. To pursue this hypothesis, agitation, sleep, and incontinence data must be collected throughout the night on patients with moderate to severe cognitive impairment. Given that collecting these data in a conventional sleep laboratory is impractical because of cost and the invasiveness for patients with cognitive impairment, we are using a novel method of collecting sleep, agitation, and UI data. Inexpensive sensors are deployed in natural living environments, that is, the patients’ bedrooms, to collect these data. Our team of investigators has expertise in the development and use of passive body sensors to measure agitation and sleep in persons with ADRD.
Theoretical Framework
In persons with dementia, disruptive, agitated behaviors are believed to result from one or more unmet needs—physical, psychological, emotional, or social. 5 These behaviors result from progressive loss of ability to recognize needs and/or express these needs orally. The Need-Driven Dementia-Compromised Behavior framework depicts how the combination of background and proximal factors leads to agitated behavior. For this study, UI was conceptualized as a proximal factor that leads to both agitation and sleep interruption in persons with ADRD. This relationship, however, has not been systematically specified and confirmed, that is, which of incontinence, sleep disturbance, and agitation is triggered by which others or if each triggers the others at different times.
Nighttime Agitation in ADRD
Nocturnal agitation in older adults with ADRD is most frequently treated with antipsychotic and hypnotic medications although these pharmacologic therapies result in little success and have adverse effects on persons’ outcomes and quality of life. 6,7 Thus, need continues to prevail to identify precursors for nocturnal agitation behaviors as a basis for developing effective nonpharmacologic interventions to prevent or reduce these behaviors. These interventions would not only prevent the negative effects of psychoactive drugs on persons with ADRD but would also reduce caregiver burden and the cost of care. If agitation can be prevented or managed without psychoactive drugs for 1 year for this study population, the savings could be highly significant. Based upon the national average of 800 000 new admissions of persons with AD to nursing homes each year at a cost of US$219 per day and a conservative estimate of US$76 per day for 4 hours of nursing assistant care, 8 the savings would be over US$114 million.
We are using audio sensors near the bed to record acoustic signals during the time when the person with dementia is sleeping. Our system records the timings and durations of each period of verbal outbursts or repetitive sentences so that these can be used to find correlations among nighttime agitation, sleep, and UI. In addition, the Wireless Identification and Sensing Platform (WISP) and Technology-Enabled Medical Precision Observation (TEMPO) sensors (described later) will be used to combine with the recorded vocalizations to identify agitation and its timing.
Sleep Disturbances in ADRD
Studies estimate that between 18% and 82% of persons with ADRD experience sleep disturbances and that caregivers report that the sleep disturbances are a major reason for institutionalization of the care recipient. 2,9,10 Manifestations of sleep disturbances in persons with dementia include frequent nighttime awakenings, increases in daytime sleep, day–night sleep pattern reversals, and decreases in slow-wave sleep and rapid eye movement sleep. 11,12 Further, in persons with AD, nighttime agitation was most prevalent in those who were the most cognitively impaired and who were awakened the fewest amount of times for toileting. 12 A combination of data from the TEMPO sensors worn on the wrists and WISP system, a tag under the mattress, is being used to identify sleep onset, duration, and quality.
Urinary Incontinence in ADRD
Rates of UI are higher among persons with dementia (53%) than those without dementia (13%). The prevalence of UI in dementia varies widely, ranging from 11% to 90% with institutionalized persons with dementia having a higher prevalence than those living in the community. 13 In a study by Ouslander and colleagues, 14 incontinence was identified by 36% of 184 caregivers as a problem in their care of older community-dwelling persons with dementia. Incontinent persons with dementia had greater impairment of cognitive function and more frequent behavioral problems than did patients without UI. Follow-up interviews with caregivers of persons placed in a nursing home revealed that UI had played an important role in most caregiver decisions to institutionalize their loved ones. However, UI was rarely the primary reason. The majority of incontinent elderly individuals still residing in the community were being managed by nonspecific techniques such as incontinent aids and toileting schedules. These data emphasize the need to educate community caregivers of persons with dementia in the appropriate management of UI and the need for further research on methods of effectively targeting assessment and treatment strategies to this patient population. 15 The DryBuddy is the wireless sensor used to record timing and frequency of incontinent episodes occurring throughout the night in this study.
State of Technology
The need for development and implementation of technology for the advancement of dementia research cannot be overstated. Studies of agitated behaviors in this population have traditionally relied on interviews with staff and family members and/or direct observation by research personnel. The latter method can be intrusive, inefficient, and quite possibly alter the behavior of interest merely by the presence of the observer. The use of videotaping has been described in dementia research as well 16,17 but also raises concern for patient/caregiver privacy and can result in reams of footage to be reviewed and interpreted. In the area of sleep research, polysomnography (PSG) is routinely used to assess sleep architecture and quality and involves recording of multiple physiologic variables (electroencephalogram, electrocardiogram, electromyogram, and electrooculogram). 18 Although portable PSG systems are available for home use, they require trained personnel for monitoring the equipment, which can be expensive and intrusive. Actigraphy, another widely accepted sleep research method, employs the use of a watch-like device that measures limb movements to determine rest and activity cycles. 19,20 The utility of actigraphy in examining agitated behaviors in dementia has been reported by Nagels et al, 21 but its ability to differentiate normal movement from agitated movement has been questioned. 22 A proposed system based on audio, video, and heart rate sensors proved to be low cost and useful to detect sleep–wake states 23 but again raises privacy concerns. Special mattress pads embedded with sensors to monitor body movement, vibration, position in bed, and physiological variables (body temperature, heart, and respiratory rate) have been developed but require batteries in some cases and may be uncomfortable, thus affecting sleep. 24 The automated wireless “zeo” headband system showed promise in a study of young healthy adults as an easy-to-use and accurate complement to other established technologies for monitoring sleep. 25 However, its use in older adults with cognitive impairment is questionable due to the possible unacceptability of wearing the headband.
Research in the area of elder incontinence is strikingly scarce and lacking in the use of advanced technology. Devices and systems have been proposed to detect incontinence episodes with the aim of improving management in long-term care settings. However, none of these systems to date have been used for research purposes. Siden and colleagues described the use of a disposable wireless diaper unit, the “smart” diaper that transmits a radio signal upon moisture, triggering an alarm that alerts caregivers to incontinence episodes. 26 Wai et al tested a wireless continence management system in 1 institutionalized patient with dementia; detection rate for wetness approximated 50%. 27 Less sophisticated technologies including odor sensors and wetness detecting underwear are in the developmental stages but are not designed for data transmission and clearly are not applicable for use with patients having cognitive impairment. 28
The combination of multimodal instruments, WISP system (bed sensors), TEMPO nodes (watch-like devices), the acoustic sensor (microphone), and the DryBuddy (incontinence detection device) to measure nighttime agitation, sleep characteristics, and UI is novel and provides objective measures of these problematic behaviors in real-life settings (ie, home environments) where over two-thirds of persons with dementia receive care. 29 The impact of the use of this passive system of measures includes the collection of objective data with minimal invasion of the private lives of persons with dementia and their family caregivers. Wireless body sensor networks hold promise as innovative, reliable, and valid means to collect these data.
Preliminary Studies
This project builds upon the 3 studies performed to date by the collaborators on this project. The use of TEMPO, 30 a custom inertial wireless body sensor network (Figures 1 and 2), has been explored to objectively, continuously, and noninvasively measure movement in older persons with dementia over an extended period of time and to make time-domain assessments of physical agitation from these raw movement data. A pilot study was conducted with 6 elderly residents with dementia living in long-term care identified as being at high risk of agitated behaviors. 22 Nine hours of data were collected from each resident using devices applied at 3 sites while behaviors were simultaneously observed and annotated. The TEMPO data were processed using Teager energy analysis, 31 (Kaiser) which measures the mechanical energy of the movement, emphasizing the jerky and repetitive movements that tend to correspond to physical agitation. Construct validity testing revealed that the Teager energy analysis correlated well with agitation and aggression but not with cognitive decline as measured by the Cohen-Mansfield Agitation Inventory, 32 the Aggressive Behavior Scale, and the Mini-Mental State Examination (MMSE), respectively. Wrist, waist, and ankle interreliability values were all statistically significant, ranging from .41 to .84, P < .001 to .05, indicating strong reliability. Convergent validity tests resulted in moderately strong support (consistent with Cohen’s d effect sizes).

Technology-Enabled Medical Precision Observation (TEMPO) device.

Technology-Enabled Medical Precision Observation (TEMPO) in place.
In the Early Targeted Urinary Incontinence Intervention pilot study,
33
a program of early treatment with prompted voiding to improve the urinary control of long-term residents was tested. One component of the study used 24-hour pad tests to specify UI episodes and as a basis for planning the prompted voiding intervention. The pad test was conducted with 34 patients, 14 with a diagnosis of ADRD. Each resident was checked hourly for incontinence in the pad and was toileted. The pad was weighed before and after placement to determine whether there was any urine loss hourly. Of the 14 patients, 10 went 4 to 6½ hours (mean = 4.5) without voiding in the toilet or leaking in the pad. Dryness usually occurred between 12:00
A system to monitor body positions and movements during sleep based on Intel WISPs was built and validated. 24 This system does not require any additional user action outside of the user’s daily routines as the WISP tags are attached to the sides of the bed mattress and accelerometer data are collected by these tags (Figure 3). Using these data, the user’s body position was inferred (lying on the back [supine], abdomen [prone], left or right sides) as well as movements and body positions during sleep. Thus, using the WISP system in conjunction with TEMPO nodes, it is possible to accurately and passively monitor sleep continuity and duration and nocturnal agitation in the study participants (Figure 3).
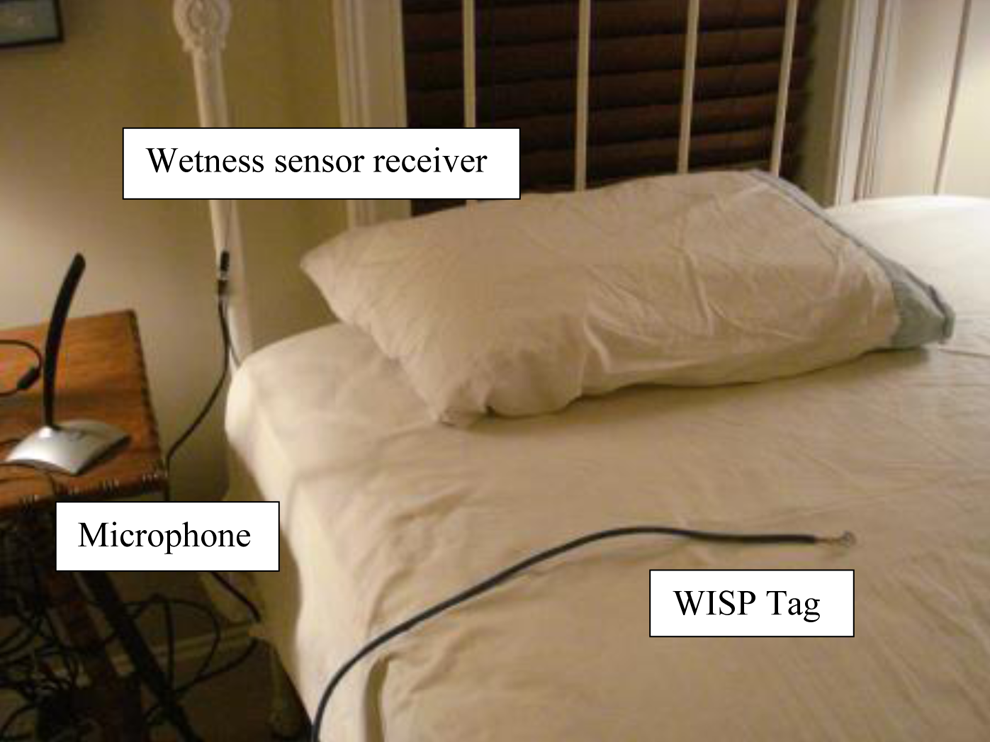
Equipment set up (note: Wireless Identification and Sensing Platform [WISP] tags are placed under sheet).
Approach
Design
A single-group, descriptive design with persons having a diagnosis of dementia (Alzheimer’s, vascular, mixed, or unspecified) and their caregivers (n = 50 for dementia participants; n = 50 for caregivers) was employed. Data collection took place over 5 to 7 week nights in participants’ home environments. As we were using a single-group design, there was no randomization of study participants. Institutional review board approval was obtained from the University of Virginia.
Sample
The study sample of 50 persons with ADRD and their 50 family caregivers is being drawn from eligible persons receiving treatment through the University of Virginia Health System as well as non-University of Virginia sites including Adult Daycare Centers, Alzheimer’s Association support groups and functions, home health care programs, and community-based neurology clinics
Inclusion Criteria
Inclusion criteria for persons with AD and related dementia include (1) male or female with notation if man has enlarged prostate; (2) aged 65 to 95 years; (3) physician documentation of dementia: Alzheimer’s, vascular, mixed, or unspecified type; (4) caregiver confirmation of at least 2 agitation behaviors occurring a minimum of several times per week in person with ADRD as measured by the Cohen-Mansfield Agitation Inventory-Community version; (5) caregiver confirmation of an average of ≥2 occurrences of nocturnal UI per week; (6) all medications stable for at least 6 weeks prior to the study; (7) community dwelling; (8) willingness to defer changes in the following medications until the completion of the study protocol: antidepressants and anxiolytics; psychotropics, sedating, and PRN over-the-counter sleep medications, as these may affect study outcomes; and (9) fluent in English For family caregiver the criteria include: (1) aged 21 years or older; (2) informal, unpaid caregiver who resides with the care recipient; (3) fluent in English; and (4) willingness to defer changes in the following medications for the person with ADRD until the completion of the study protocol: antidepressants, anxiolytics, psychotropics, sedatives, and PRN over-the-counter sleep medications as these may affect study outcomes
Exclusion Criteria
Exclusion criteria for persons with dementia include (1) documented history in medical record of sleep apnea, periodic limb movements in sleep disorder, or restless legs syndrome; (2) presence of acute illness as this could lead to delirium; (3) alcohol abuse or dependence within the past 2 years (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition criteria); and (4) history of significant psychiatric illness (eg, schizophrenia).
Sources of Material
The research data are obtained from survey instruments, poststudy interviews with caregivers, and wireless sensors (TEMPO, WISP, DryBuddy, and audio sensor) collected from 5 to 7 days in participants’ homes. After confirmation of inclusion criteria, baseline information is collected. The demographic form, 3 Modified MMSE for cognitive function, medical history, and Minimum Data Set physical function form are completed 1 time by the caregiver and the person with dementia at the initiation of the study.
Wireless Sensors
To measure agitation and sleep, the TEMPO, a watch-like device is worn at night to detect movement and assess for agitation. The WISP bed sensors are secured below the bedsheet/pad to remain in place throughout the study period to monitor body positions and movement, and a microphone remains in place at the bedside to detect verbal agitation through vocalization. No movement implies sleep and periods of no or minimal movement will be tabulated from the recordings. We apply acoustic processing on the recorded audio to detect verbal agitation, given that some of the most frequent agitation behaviors of persons with dementia are screaming, constant repetition of sentences, and sounding frustrated during these agitated behaviors while asleep. 8 The goal of the acoustic processing on the recorded audio during sleep is to detect screaming, periods of constant repetition of sentences, and frustration in their voices during these periods. We detect screaming based on a threshold-based algorithm. To detect repetition of sentences, we do apply a speech-to-text conversion algorithm on the recorded audio and save all the sentences the person uttered during sleep. Repetitive sentences are found by a matching algorithm. 22
To determine frequency and timing of UI, the DryBuddy (patented by US7808392 B1) a commercially available wetness sensor is used. This is a highly accurate sensor at detecting urine. The incontinence data are transmitted wirelessly through a small (2 in) sensor worn in the provided brief, held in place by a magnetic device so that there is no belt or taping (Figures 4 and 5). Two data receivers that transmit DryBuddy data are placed on both sides of the bed and remain stationary throughout the study period.

DryBuddy device.

Placement of DryBuddy in brief.
A computer for data transmission is setup at the bedside at the initiation of the study. During the study period, the caregiver’s only task related to the wireless sensors is placement of the TEMPOs on the wrists and DryBuddy in the brief; all other equipment remain in place undisturbed (Figure 6).

Equipment set up with patient.
Additional Study Measures
To determine the volume of UI, participant’s worn briefs are weighed prior to use and then stored in dated plastic bags each morning by the caregiver to be weighed at completion of the study to reflect volume of urine lost in the time frame. 34 The pad tests have been shown to be a reliable measure of urine volume lost. Pads can be stored for a number of days in a sealed plastic bag and still accurately reflect the volume lost.
To confirm sleep data collected by body sensors, each morning, caregivers complete a standard sleep diary for the care recipient to record bedtime, awakenings, and arising time. To assess for care recipient’s pain, caregivers complete either the “Pain Thermometer” or “Pain Assessment in Advanced Dementia Scale” each night at bedtime. A measure of pain is taken because of the relationship of pain with both agitation and sleep, allowing us to ascertain whether the relationships are further compounded by pain. At the completion of the 5 to 7 night study period, caregivers undergo a brief interview to measure the feasibility and acceptability of the use of the body sensors.
Challenges and Opportunities
In our subject recruits to date, the technology provides an opportunity for improved data collection because it is wireless and requires minimal effort to operate. Yet the data are collected in real-time collection and it is immediately available to research staff for monitoring. The technology is also noninvasive so it is much less burdensome to the patients. The data collection instruments involve only a bracelet, a pad on the bed, and a small sensor in the brief or pajamas of the patients. None of these things have bothered the patients to date.
However, the technology has also presented challenges. Although simple, it still seems cumbersome to some, caregivers, especially those who are not technologically savvy, thus it presents higher perceived burden. The biggest concern of caregivers is that they do things correctly; once they have tried to use the equipment they seem easier about it. In fact, they report that the nontechnology requirements of the study, like the sleep diary or the pain rating, are more difficult to complete.
It is a challenge to do the trouble shooting for the technology from a distance. However, often by reviewing the data collected, it is possible to discover the nature of the problem and it can often be addressed via phone. An advantage is that if the technology does not work correctly for 1 night, data can be collected easily for 1 more night as long as the participants are willing.
The DryBuddy, the sensor for incontinence, has especially presented challenges some of which were worked out when it was being piloted. Placement of the sensor in the brief is a challenge to be able to pick up the time of the incontinence episode or to detect multiple episodes if the brief is not changed. The addition of a second bedside receiver has helped to overcome this problem. Every patient has had different methods of UI management and a challenge has been to have the DryBuddy work with a minimum of change for the persons with dementia and their caregivers. Bowel incontinence further complicates the accurate detection of urinary episodes (both timing and frequency). Again, when this occurs it is possible to extend the data collection.
Caregivers have expressed the sense of “doing something” and have demonstrated high levels of commitment and adherence. They have expressed how participation in this study provides them affirmation of their caregiving efforts.
In conclusion, although there are both challenges and opportunities to the technology for exploring the relationship of UI, agitation, and sleep in community-dwelling persons with AD and related dementias, the challenges seem possible to overcome and the opportunities outweigh the challenges. We are optimistic that the findings will lead to interventions that will help caregivers sustain their caregiving longer and allow the person with dementia to remain in the community longer at less cost to the health care system.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Funding for this work is provided by NIH, National Institute of Nursing Research, 1R21NR013541.