
Abstract
Highlights
1. MCI patients had a significant higher reduction of auditory P50 gating than controls. 2. MCI patients might have impaired the ability of inhibiting the repeated stimulus, when compared to the non-MCI controls. 3. P50 gating measure might improve the accuracy of the diagnosis of MCI in clinical practice.
Introduction
Mild cognitive impairment (MCI) is a clinical syndrome thought to represent the transition from normal function to dementia. 1 Mild Cognitive Impairment patients have a high risk of converting to Alzheimer’s disease (AD). 2 The earlier discern MCI, the more beneficial obtain from cognitive interventions, 3 especially in low-income and middle-income countries (LMIC) where around two-thirds of population with dementia live. 4 Considering the heterogeneity of MCI, 1 it needs more reliable biomarkers or measures that support the clinical diagnosis. Auditory event-related potentials (ERPs), as a kind of electroencephalography (EEG) technology, have been widely used in the study of cognitive impairment. These studies mainly focuses on the changes of neural activity in different parts of the brain between aging, MCI, and dementia. 4 The auditory ERPs components, like P300 and N200, might help distinguish between health aging and MCI in clinical practice. 5 Auditory P50 is one component of ERPs that appear at the approximate latency of 50 milliseconds after the auditory stimulus, 6 and it refers to the ability of repetitive auditory stimulus inhibition of the central nervous system, 7 whereas the inhibition of repetitive stimulus seems to be preserved with aging, 8 P50 gating shows an increase of amplitude in both patients with MCI and AD, which has been suggested as a neurophysiological biomarker of early stages of AD. 9
As far as we know, there are only two studies direct comparison alterations of auditory P50 gating between MCI patients and controls that found reduction of P50 amplitude.2,10 According to recent finding focused on P50 gating in aging and AD, 9 we hypothesized that MCI patients had a more reduction in P50 gating when compared with those health controls. We aimed to determine the impact of P50 gating among MCI patients that diagnosed mainly based on the clinical interview by using the Clinical Dementia Rating (CDR). 11 These findings will further support the diagnosis of MCI patients and may help in implementing P50 gating measure among those have cognitive impairment in clinical practice.
Methods
The study design and data were part of our program funded by Shenzhen Science and Technology Innovation Commission from 2014 to 2017 (program number: JCYJ20140415092628046). We had obtained the approval of the Ethics Committee of Shenzhen Mental Health Center before the program started (ethics number: [2014] Lun Shen No. [03]).
Participants
We had conducted face-to-face cognitive interview of 350 participants in the Memory Clinic of Shenzhen Mental Health Center between April 01, 2015 and September 30, 2015, and 121 participants were defined as MCI cases. The prevalent of MCI cases in our study is about 35%. Twenty MCI patients and 17 healthy elderly controls finished the auditory P50 gating measure. All participants provided informed consent before the clinical interview, neuropsychological test, and P50 gating measure. This study was conducted in accordance with the approved protocols and the Declaration of Helsinki.
The inclusion and exclusion criteria of MCI patients12,13: (1) age ≥60 y old; (2) the patient just complained memory impairment at least 6 month; (3) the uniformly trained geriatric psychiatrist conducted face-to-face cognitive interview using the CDR, with a score of .5 points 11 ; (4) Exclude any type of dementia or any chronic physical conditions or mental disorders that might cause brain dysfunction, including head trauma, schizophrenia, and depression. The age of control participants was also no less than 60 years old, but complaining no memory impairment and the CDR interview scored 0 points. The control participants were not diagnosed any chronic physical conditions or mental disorders as the MCI patients.
Measurements
All eligible participants completed a structured questionnaires including demographic information, Geriatric Depression Scale (GDS), Activity of Daily Life (ADL), MINI-Metal State Examination (MMSE), and Montreal Cognitive Assessment (MoCA). Demographic information, such as age, gender, education, marital and living status, income, and chronic physical conditions (hypertension, diabetes) were collected.
GDS: GDS includes 13 items with a total score of 30 points. The higher the scores are, the severer the depressive symptoms are. 14 The Chinese version of GDS has satisfactory reliability and validity among the elderly in urban communities in China. 15
ADL: ADL contains 14 items, including 6 items of physical self-care and 8 items of instrumental activities of daily living. The total score ranges from 16 to 64 points. The higher the scores are, the worse the function of daily living is. 16 The scale has been showed that it can be used for the auxiliary diagnosis of cognitive dysfunction in China. 17
MMSE: MMSE includes 11 items, which are evaluated according to the Likert scale from 0 to 3 points. The total score is 30 points. The higher the scores are, the better the cognitive function is. 18 The scale has been proved that it was suitable for widespread clinical practice in China. 19
MoCA: MoCA contains 11 items with a total score of 30 points. The higher the scores are, the better the cognitive function is. Compared with the MMSE, MoCA is more sensitive to screen the MCI patients. 20 The Chinese version of the scale has been proved its reliability and validity on the elderly population in China. 21
Auditory P50 Gating Measure
Recording Procedures
A 32-channel EEG system (Germany Brain Products BrainAmp MR amplifier) was using for auditory evoked potential recording with Ag/AgCl electrodes positioned according to the 10 to 20 international system. 22 During the recording sessions, the participants were seated upright in a shielded quiet room while the instruction and auditory stimuli were delivered via head set headphone. Each participant was told to relax, keep eye open, and looked at a fixation picture at about .5 m distance via the computer screen in order to prevent drowsiness. P50 gating were obtained from Fz, Cz and Pz positions referred to linked left ear lobes, blinks, and vertical ocular movements (Electro-oculogram) were monitored via two electrodes placed above and below the right eye. Data were recorded in alternating currency (AC) using a band-pass filter .05 to 200 Hz, and a sampling rate of 1000 Hz. Electrode impedance was kept below 5 KΩ.
Testing Paradigms
Pairs of pure tone clicks were delivered to participants according to Recording Procedures. The clicks (duration 4 millisecond, inter-stimulus interval 500 m/s) were presented at 80 dB above the average of human hearing threshold. The inter-pairs interval was of 10 s which was used to avoid habituation. All recording took about 1.5 s as an epoch between 100 milliseconds before the first click and 400 m/s after the second click.
Data Processing
When data are analyzed offline, electrical signals were digitally filtered using a 10 to 50 Hz band-pass filter to avoid the N100 effect on P50. 23 Each electrical signal was visually controlled and remaining artifacts (mostly eye movements) were manually removed by two independent experienced technician blinded to diagnosis of participants. P50 was defined as the second most positive peak occurring in latency between 40 and 70 m/s after each click onset. 6 P50 amplitude was measured from the preceding negativity (Nb). When Pa overlapped P50 so that Nb was not clearly identifiable, P50 amplitude was measured relative to the prestimulus baseline. 24 One hundred epochs that have been removed artifacts were recorded to calculate individual averages for each participant. Auditory P50 gating was indexed as the second stimulus (S2)/the first stimulus (S1) ratio.
Statistical Analysis
IBM SPSS version 22.0 for Windows was used for all statistical tests. Proportions (%) was used to presented categorical variables, and mean ± standard deviation (x ± s) was used to present continuous variables. Independent-samples T test, Chi-square tests were performed to assess the demographic information and neuropsychological test results in two groups. One-way analysis of variance (ANOVA) was used to compare the P50 average amplitude and gating at Fz, Cz, and Pz sites between two groups, respectively. The repeated measured ANOVA was used to compare the changes of P50 average amplitude and gating at different sites between two groups. The Spearman’s correlation coefficient was used to analyze the correlation between P50 gating and neuropsychological tests. A Receiver operating characteristic curve (ROC) analysis was conducted to distinguish MCI and control group of auditory P50 gating. A value of two-tailed P < .05 was considered statistically significant.
Results
Demographic Information and Neuropsychological Tests
Demographic information and neuropsychological test results in Mild Cognitive Impairment patients and controls.
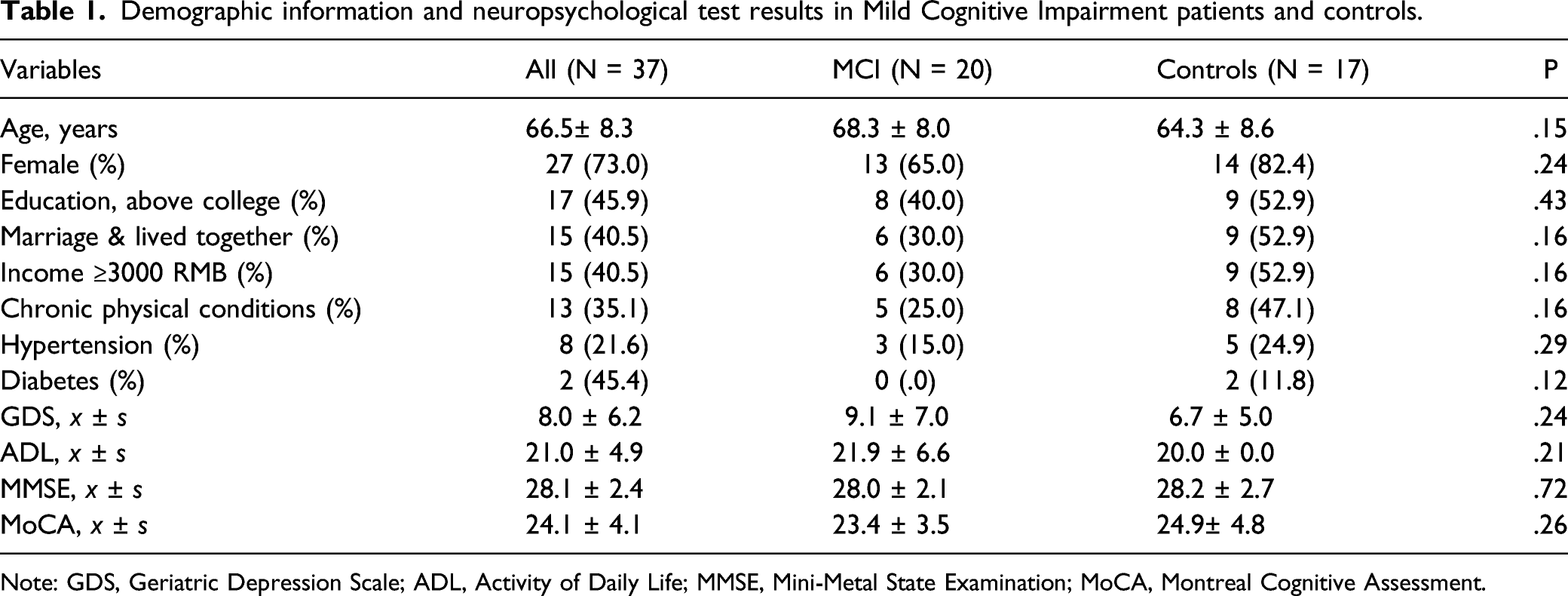
Note: GDS, Geriatric Depression Scale; ADL, Activity of Daily Life; MMSE, Mini-Metal State Examination; MoCA, Montreal Cognitive Assessment.
P50 Average Amplitude and Gating Compared at Different Sites
Figure 1A show that the P50 average amplitude at Pz site in MCI patients was significantly higher when compared to controls (2.62 ± 1.20 vs 1.70 ± .74, P = .01), and there were no statistically significant differences of P50 average amplitude at Fz and Cz sites between MCI patients and controls respectively. Figure 1B showed that P50 gating reduction at Fz site in MCI patients was significantly higher than controls (1.21 ± .68 vs .66 ± .37, P = .00), but no significant higher at Cz and Pz sites than controls, respectively. Compared P50 average amplitude: (A) and gating: (B) at Fz, Cz, and Pz sites between Mild Cognitive Impairment patients and controls respectively.
P50 average amplitude and gating repeated measured at different sites
P50 Average Amplitude and Gating Repeated Measured at Fz, Cz, and Pz Sites Between MCI Patients and Controls

Note: MCI, Mild Cognitive Impairment, *: P ≤ .05.
Correlation Between the P50 Gating Measure and Neuropsychological Tests in MCI Group
Correlation between the P50 gating measure and neuropsychological tests in MCI groups (n = 37).

Note: MCI, Mild Cognitive Impairment; GDS Geriatric Depression Scale; ADL, Activity of Daily Life; MMSE, MINI-Metal State Examination; MoCA, Montreal Cognitive Assessment, * P ≤ .05, **P ≤ .01.
The best cut off point of auditory P50 gating measure that distinguishes MCI and control group
A ROC analysis was conducted to distinguish MCI and control group of auditory P50 gating S2/S1 at Fz site. According to the results of Coordinates of the Curve and the formula Youden’s index = Sensitivity + Specificity – 1, Zero point five was the maximum value of Youden’s index that was defined as the best cut off point to distinguish MCI and control of auditory P50 gating S2/S1 at Fz site. The corresponding sensitivity and specificity are .5 and 1.0.
Discussion
In this case-controlled study with a moderate sample size, we have proved our hypothesis that MCI patients had a significant higher reduction of P50 gating than their age-sex matched controls. There were no significant association between neuropsychological tests and auditory P50 gating measure in MCI group. Zero point five was the best cut off point to distinguish MCI and control of auditory P50 gating S2/S1 at Fz site.
We also found that the P50 average amplitude at Pz site in MCI patients was significant higher when compared to controls. Our findings provided additional measures that support diagnosis of MCI patients beyond conventional methods using to identify cognitive declines, like clinical interview and neuropsychological tests. This may popularize P50 gating measure among those have cognitive impairment in clinical practice.
Our study found that P50 gating and average amplitude in MCI patients was significantly higher than those in controls. To some extent, our findings were in consistent with previous studies focused AD-dependent alterations of auditory P50 gating. 9 These previous studies mainly used across-sectional designed and the participants were mostly patients with AD type dementia. Golob et al conducted two studies that directly compared between MCI patients and elder controls. One used the “paired click” paradigm auditory stimulation found that P50 amplitude and latency were significantly increased in MCI patients with a cross-sectional design. 10 Although the study did not report the P50 gating index as S2/S1, the P50 amplitude of S2 in MCI patients was significantly higher than those in controls. It equally suggested that MCI patients had weaken ability to filter out repeated or redundant stimulus. The other used the “steady-state” paradigm auditory stimulation found that the P50 amplitude increased in MCI as a function of MCI diagnostic subgroup (stable vs amnestic MCI) with a longitudinal design. 2 The study reported the P50 average amplitude across all trials as the index auditory P50 gating, and the findings also suggested that P50 gating reduction in MCI patients might be considered as a sensitive neurophysiological biomarker of prodromal AD. Compared to the similar two studies, our study used a paired click paradigm, and then reported both the P50 gating index as S2/S1 ratio and the P50 average amplitude in one paired click. On the other hand, we also found that .5 was the best cut off point to distinguish MCI and control of auditory P50 gating S2/S1 at Fz site. The corresponding sensitivity and specificity are .5 and 1.0. That means when the P50 gating S2/S1 at Fz site is less than .5, it could exclude the possibility of MCI based on our findings. The significance of the above findings is that the auditory P50 gating is useful to identity the negative cases but poor for positive MCI cases (50%). That might be physiological aging impacts the regulation functions of brain inhibitory modulation of auditory P50 gating. 25 In the auditory P50 gating positive cases, physiological aging might play a major role in the limited capacities of filtering out the same auditory stimulus, which resulted in poor identify for positive MCI cases. In summary, our study findings indicated that MCI patients might have impaired the ability of inhibiting the repeated stimulus by reporting P50 gating index as S2/S1 ratio.
Although the mechanisms underlying auditory P50 gating changes in cognitive impairment are still unclear, there might be involved several brain neurotransmitters or receptors changes. First, while AD might involve a substantial loss of choline neurotransmitters in different brain regions, 26 the studies in AD patients indicated that P50 gating inhibition might be a cholinergic-modulated process. 6 Second, it has been proved that nicotinic acetylcholine receptors (nAChRs), which impacted the release of some neurotransmitters linked to sensory processing,27,28 were decreased in patients with AD. 29 Third, the nAChRs has been showed to have significant influences for inhibition of a human analogy of the auditory P50 gating in animal auditory gating studies. 30 However, more direct evidence focusing on the link between specific neurotransmitters or receptors and P50 gating in cognitive impairment patients still needed to clear the underlying associations.
The strengths of the current study include a moderate sample size and well-matched controls for comparison. However, several limitations should be noted. Our study used clinical interview by using Clinical Dementia Rating (CDR) for the inclusion criteria of MCI patients that lack of other assessments. A cross-section design in our case-controlled study restricted inspection the causal relationships of auditory P50 gating and cognitive impairment. To some extent, our study replicated previous study design and methods, but our findings proved that the reduction of P50 gating in MCI patients by reporting both average amplitude and S2/S1 ratio. Future study should consider using objective assessments to establish MCI patients’ diagnosis and conduct follow-up P50 gating measure.
In conclusion, MCI patients had a significant higher reduction of auditory P50 gating than controls, and .5 was the best cut off point to distinguish MCI and control of auditory P50 gating S2/S1 at Fz site. The results of our study indicated that MCI patients might have impaired the ability of inhibiting the repeated stimulus, when compared to the non-MCI controls. Our findings suggests that P50 gating measure might improve the accuracy of the diagnosis of MCI, and this may help implementing P50 gating measure among those have cognitive impairment in clinical practice.
Footnotes
Acknowledgments
The author would like to thank Dr Xu Jie in Shenzhen Mental Health Center for providing auditory P50 gating measure. This assistance was supported by the Electroencephalogram Institute of Shenzhen Mental Health Center. All authors listed have approved the final version of the manuscript and take full responsibility for the manuscript.
Author Contributions
Manuscript writing: Weidong Song; Analysis and interpretation of data: Donghui Wu; Data collection: Xiaohui Hu, Guohua Xie; Quality Control: Yang Wang.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: This study was supported by Shenzhen Science and Technology Innovation Commission from 2014 to 2017. The program number is JCYJ20140415092628046.