
Abstract
Background:
The objective of this study was to validate the Turkish version of the Quick Mild Cognitive Impairment (Qmci-TR) screen.
Methods:
In total, 100 patients aged ≥65 years referred to a geriatric outpatient clinic with memory loss were included. The Qmci was compared to the Turkish versions of the standardized Mini-Mental State Examination and the Montreal Cognitive Assessment (MoCA).
Results:
The Qmci-TR had higher accuracy than the MoCA in discriminating subjective memory complaints (SMCs) from cognitive impairment (mild cognitive impairment [MCI] or dementia), of borderline significance after adjusting for age and education (P = .06). The Qmci-TR also had higher accuracy than the MoCA in differentiating MCI from SMC, which became nonsignificant after adjustment (P = .15). A similar pattern was shown for distinguishing MCI from dementia. Test reliability for the Qmci-TR was strong.
Conclusion:
The Qmci-TR is a reliable and useful screening tool for discriminating MCI from SMC and dementia in a Turkish population.
Introduction
With recent improvements in life expectancy, the number of people aged 65 years and older is expected to increase worldwide. 1 With this, the prevalence of cognitive impairment including dementia is also expected to increase. 2,3 Mild cognitive impairment (MCI) is a transitional condition between normal cognitive functioning and dementia. 4 The diagnosis is characterized by subjective and corroborated cognitive deficits associated with objective evidence of impairment at clinical evaluation, decline in cognitive functioning relative to previous abilities without a change in basic daily functioning, with or without subtle difficulties in complex day-to-day activities, and the absence of dementia. 4,5 MCI places patients at an elevated risk of developing dementia, 6 and the progression rate is approximately 10%. 7 -9
It is important to discriminate between patients presenting to busy general and geriatric medicine clinics with subjective memory complaints (SMCs) but normal cognition (those with subjective and nonprogressive memory complaints without objective cognitive deficits or functional decline), 10 MCI, and dementia as the early detection of MCI may be important in providing preventative and interventional approaches to management. 9,11,12 Furthermore, treatment choices differ. 12 -14 Although no gold standard yet exists to screen for MCI in clinical practice, a number of instruments are available to clinicians to differentiate between MCI and SMC. The Montreal Cognitive Assessment (MoCA) is an increasingly popular short cognitive screening instrument used for this purpose. 15 A Turkish version is validated but has shown lower sensitivity and specificity compared to the initial validation in English. 16 Further, the established MoCA cutoff for cognitive impairment (<26) yielded very poor specificity, suggesting that the optimal MoCA-Turkish score may be much lower (≤21). 16,17 Similar results were found when it was used in patients with Parkinson’s disease. 18 Other short screens that take ≤10 minutes such as the AB Cognitive Screen 135, 19 the Mini-Cog, 20 and the Mini-Addenbrooke Cognitive Examination 21 have not yet been validated in Turkish. The Quick Mild Cognitive Impairment (Qmci) screen is a recently developed brief screening instrument and is more accurate in differentiating MCI from normal controls than the Standardized Mini-Mental State Examination (SMMSE). 22,23 It correlates with the Clinical Dementia Rating Scale, the Standardized Alzheimer’s Disease Assessment Scale–cognitive section, and the Lawton-Brody Activities of Daily Living Scale. 24 It is noninferior to the MoCA, with similar accuracy but greater specificity and a shorter administration time of ≤5 minutes. 25,26 It has been externally validated in Dutch, 27 Irish, 25 and Australian populations. 26,28 Given the apparent utility of this new instrument, the aim of this study was to validate the Turkish version of the Qmci (Qmci-TR) in a geriatric outpatient population.
Patients and Procedure
Consecutive patients ≥65 years referred to a university hospital geriatric outpatient clinic with symptoms of memory loss, between December 2014 and June 2015, were included in this study. Participants were excluded if they were under 65, unable to communicate verbally in Turkish, and if they had depression (as defined by clinical evaluation and a Geriatric Depression Scale 29 score using a high cutoff greater or equal to 7). 30
A diagnosis of dementia was based on the original National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) criteria 31 for Alzheimer’s Disease (AD) and other for major neurocognitive disorder on the Diagnostic and Statistical Manual of Mental Disorders -V (DSM-V). 32 Dementia severity was graded using a modified version of the Reisberg Functional Assessment Staging (FAST) scale. 33 In this study, brain imaging was performed to each patient before the diagnosis. Cerebrovascular disease was excluded depending on brain imaging. The patients with the presence of ischemic or hemorrhagic infarct of the brain on imaging were excluded from the study. Patients with Parkinson’s dementia, Lewy body dementia, and frontotemporal dementia (total n = 9) were also excluded as these often present with atypical MCI syndromes. 34 -37 The diagnosis of MCI was consistent with Petersen’s criteria. 38 SMCs were diagnosed for patients presenting with cognitive symptoms but without cognitive deficits on neuropsychological testing or functional decline.
Participants were categorized by a consultant geriatrician into 3 groups (SMC, MCI, or dementia) after history, examination, independent neuropsychological testing by a trained psychologist using categorical fluency, the Trail Making Test, controlled oral word association test and tests of abstract thinking, praxis and the digit span test, and neuroimaging. The Qmci-TR was administered to a total of 100 patients: 32 patients with SMC but normal cognition, 35 with MCI, and 33 with dementia. Trained raters scored the Qmci-TR and SMMSE; the trained psychologist scored the MoCA. Test administration was alternated to avoid learning and fatigue effects and subsequent bias. These results were not used to inform that diagnostic classification.
Demographic characteristics of patients (age, gender, and duration of education) were recorded on their first visit. The study protocol was approved by the clinical research ethics committee of Hacettepe University. The aim and procedure of the study was explained to each patient and informed consent was obtained. Assent was obtained where capacity was felt to be absent.
The Screening Instruments
The Qmci screen comprises of 6 subtests: orientation, registration, clock drawing, delayed recall, verbal fluency, and logical memory. It has the total score of 100 (score range: 0-100, impaired to normal) and takes 3 to 5 minutes to complete. 23 The recommended cutoff for cognitive impairment is <62 of 100. 39 The Turkish translation is presented in Appendix A. The MoCA has 7 subtests: visuospatial/executive, naming, attention, language, abstraction, delayed recall, and orientation. It is scored out of 30 points (score range: 0-30, impaired to normal) and takes approximately 10 minutes to complete. 15 The recommended cutoff for cognitive impairment is <26 of 30, 15 although lower cutoffs have been suggested to improve specificity. 39,40 The standardized 30-point MMSE (score range: 0-30, impaired to normal) was used. 41,42
Translation
A native speaking translator translated the Qmci into Turkish using a forward–backward translation approach. The Turkish version was revised by health-care professionals fluent in Turkish. A professional, native English-speaking translator, without knowledge of the concepts behind the screening tool, completed the back-translation. The back-translation was reviewed by the original developers of the Qmci screen, who approved the final version. The final version of the Qmci-TR screen was tested on a small group of patients with normal cognition before it was used in this study.
Reliability
In order to test interrater reliability, the Qmci-TR screen was administered to 30 patients (with MCI or dementia), sequentially but randomly, on the same day, in different rooms by the 2 trained raters blind to the eventual diagnosis. The same raters scored the Qmci-TR tool a second time on 34 patients (with MCI or dementia) within 2 weeks to establish test–retest reliability. Alternative versions of the Qmci-TR were included to reduce learning effects. 43 Test administration was alternated to avoid learning and fatigue effects and subsequent bias.
Statistical Analysis
SPSS version 22 and Stata version 12.0 were used for statistical analysis. Data were presented as mean (SD) for normally distributed variables and as median (minimum–maximum) for nonparametric continuous variables. Categorical variables were shown as number and frequencies. One-way analysis of variance (ANOVA) was used to compare Qmci-TR and MoCA scores among the 3 groups (SMC, MCI, and dementia). Levene’s test was used to assess the homogeneity of variances for variables calculated for the 3 groups. An overall P value <.05 was considered statistically significant. When overall significance was observed, post hoc testing was performed using Tukey’s test, whereas Dunn’s test was performed to identify differences between groups. In order to test construct validity, Pearson or Spearman correlation coefficients were used to determine the correlation between the Qmci-TR and the other validated tests, if parameters were parametric or nonparametric, respectively. Interrater and test-retest reliabilities were determined using the intraclass correlation coefficient (ICC). The diagnostic accuracy of the instruments was analyzed by measuring the area under the curve (AUC) from receiver operating characteristic (ROC) curve analysis. The optimal cutoff score for each instrument was calculated from the ROC curves using the maximal accuracy approach allowing for calculation of the sensitivity and specificity of both instruments at each of these optimal cutoffs, based solely on this sample. Binary logistic regression was used to adjust ROC curve analysis for the effects of age and education. A psychometric evaluation was also conducted according to age (≤75 or >75 to balance the sample) and education, taking 7 as the cutoff (ie, ≥8 or <8), the mean years of schooling in Turkey. A power calculation, based upon published data for the Qmci and MoCA, indicated that the study would require approximately 350 paired tests to show a significant difference between instruments and their ability to separate MCI from SMC. Thus, due to time and budgetary constraints, this study was designed as a noninferiority study to show the reliability, construct validity, and diagnostic accuracy of the Turkish translation of the instrument.
Results
Demographic Results and General Characteristics of the Study Population
One hundred patients (32 with SMC, 35 with MCI, and 33 with dementia) were included. Sixty-five percent were female. The overall mean age was 75.4 (SD ±6.9) years. The mean age of the participants with SMC, MCI, and dementia was 72.4, 75.7, and 78.1 years, respectively. Patients with dementia were older than those with SMC and MCI (P = .002). The dementia group mostly consisted of patients with mild dementia (25 of 32), graded as stage 4 according to Reisberg FAST scale. The mean time in education for the whole sample was 5.5 years, and there were no statistically significant differences between the 3 groups. Mean MoCA, Qmci-TR, and SMMSE scores were significantly different between all 3 diagnostic groups (P < .001). General characteristics of patients are summarized in Table 1.
General Characteristics of Patients: Total and Those With SMC, MCI, and Dementia.
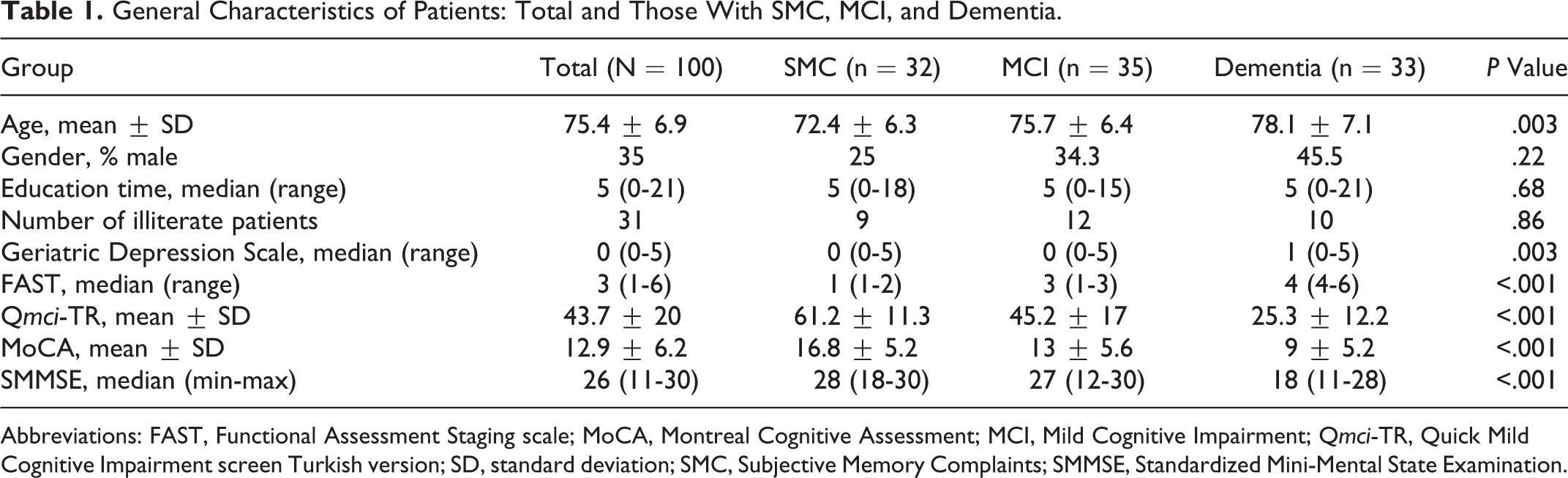
Abbreviations: FAST, Functional Assessment Staging scale; MoCA, Montreal Cognitive Assessment; MCI, Mild Cognitive Impairment; Qmci-TR, Quick Mild Cognitive Impairment screen Turkish version; SD, standard deviation; SMC, Subjective Memory Complaints; SMMSE, Standardized Mini-Mental State Examination.
Results of the Neuropsychological Tests
One-way ANOVA was used to determine the differences in mean MoCA and Qmci-TR scores and found that mean Qmci-TR (F = 54.899, df = 2.0, P < .001) and MoCA (F = 16.556, df = 2.0, P < .001) scores were significantly different among the 3 groups (SMC, MCI, and dementia). The distributions of these scores are presented in box plots in Figure 1.
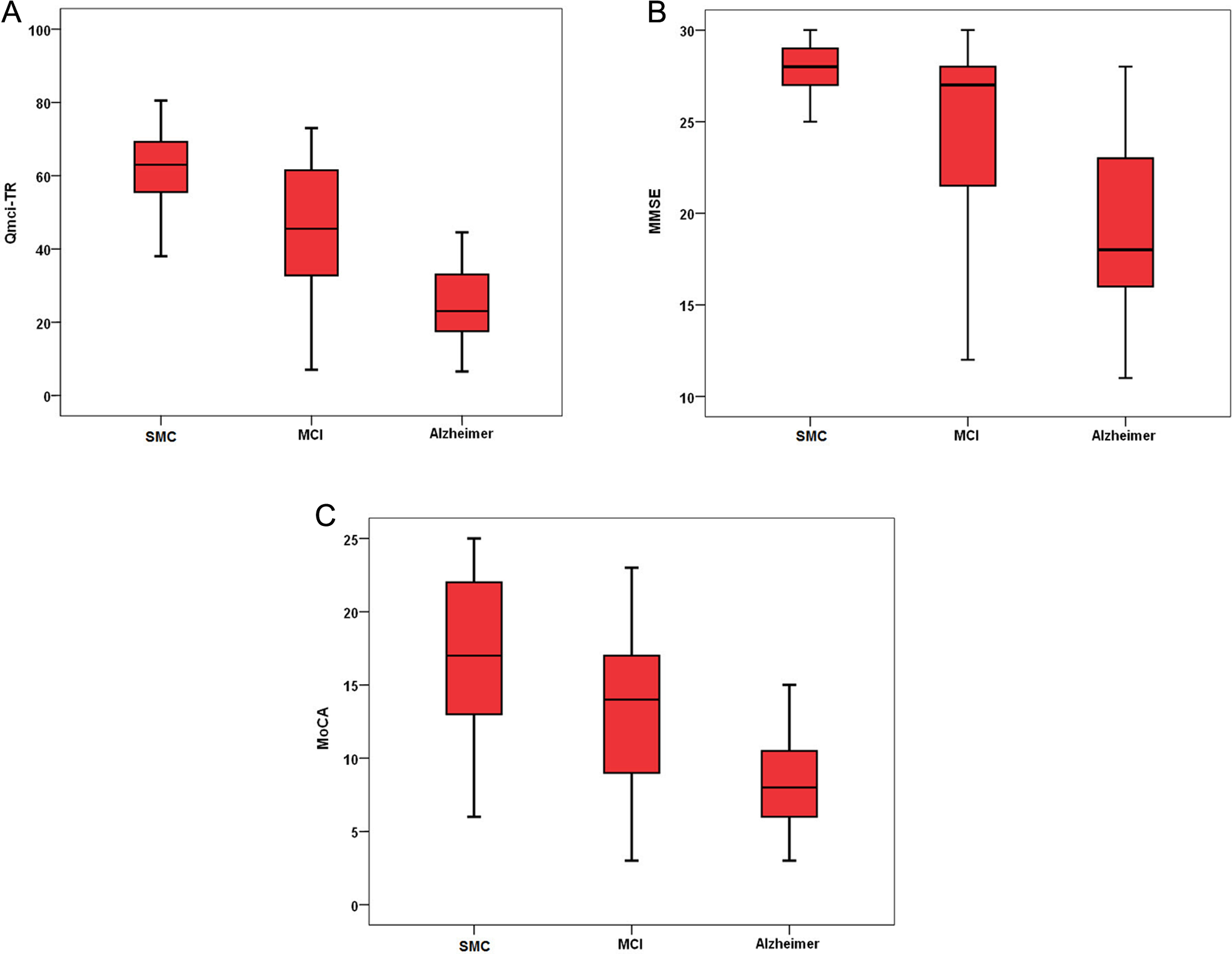
Box plot distributions demonstrating the mean ± standard deviation scores of the (A) Quick Mild Cognitive Impairment screen–Turkish version (Qmci-TR; score range 0-100); (B) Montreal Cognitive Assessment (MoCA; score range 0-30); (C) Standardized Mini-Mental State Examination (SMMSE; score range: 0-30) for patients with subjective memory complaints (SMC), mild cognitive impairment (MCI), and dementia.
Reliability
The interrater reliability of the Qmci-TR was strong for the total sample (ICC = 0.90, 95% confidence interval [CI]: 0.80-0.95) and for the MCI and dementia groups (ICC = 0.91, 95% CI: 0.62-0.98, P = .001 and 0.84, 95% CI: 0.62 to 0.94, P < .001, respectively). Test–retest reliability was also strong for the total sample (ICC = 0.92, 95% CI: 0.85 to 0.96) and for the MCI group (ICC = 0.83, 95% CI: 0.62-0.98, P = .001). Test–retest reliability was moderate for patients with dementia (ICC = 0.67, 95% CI: 0.09-0.88, P = .016).
Construct Validity
Construct validity was assessed by correlating the Qmci-TR with the MoCA. Significant and positive strong correlations were found with the MoCA (r = .77, P < .001). The Qmci-TR had a statistically significantly greater accuracy than the MoCA in discriminating SMC from MCI (AUC = 0.80, 95% CI: 0.69-0.91 compared to 0.69, 95% CI: 0.56-0.82; P = .05). After adjustment for age and education, this difference became nonsignificant (P = .15). In distinguishing MCI from dementia, the Qmci-TR was more accurate than the MoCA (AUC = 0.83, 95% CI: 0.73-0.93 compared to 0.71, 95% CI: 0.58-0.84, P = 0.009), albeit this again became nonsignificant after adjusting for the effects of age and education (P = .29). The Qmci-TR (AUC = 0.89, 95% CI: 0.82-0.95) was again more accurate than the MoCA in differentiating cognitive impairment (MCI and dementia; AUC = 0.77, 95% CI: 0.67-0.87, P = .006), which retained borderline significance after adjusting for age and education (P = .06; see Table 2). The ROC curves are presented in Figure 2.
Area Under the Curve Values of Qmci-TR and MoCA Including Adjusted Values for the Effects of Age and Education in Differentiating SMC From MCI From Dementia.
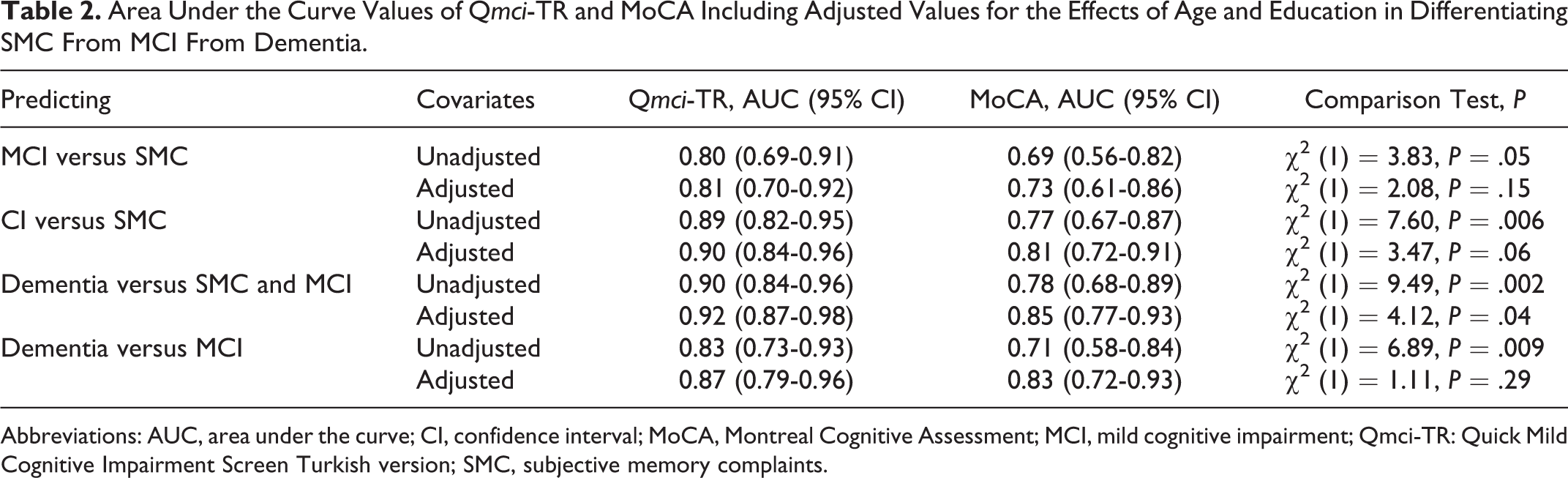
Abbreviations: AUC, area under the curve; CI, confidence interval; MoCA, Montreal Cognitive Assessment; MCI, mild cognitive impairment; Qmci-TR: Quick Mild Cognitive Impairment Screen Turkish version; SMC, subjective memory complaints.
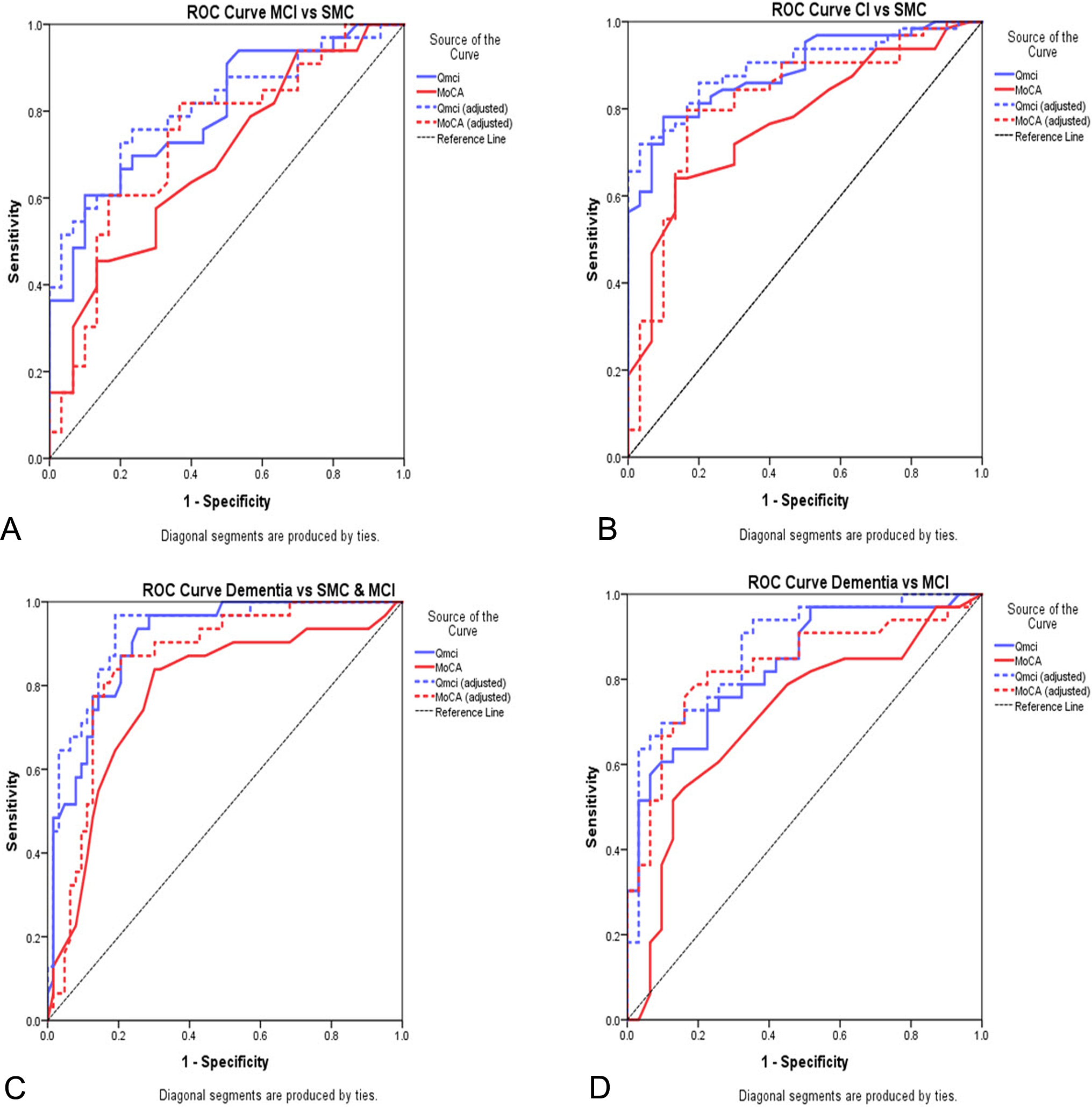
Receiver operating characteristics curves demonstrating the accuracy of Quick Mild Cognitive Impairment screen–Turkish version (Qmci-TR) and Montreal Cognitive Assessment (MoCA) including adjusted values for the effects of age and education in differentiating (A) subjective memory complaints (SMC) from mild cognitive impairment (MCI) from dementia; (B) cognitive impairment (MCI and dementia) from normal cognition but SMC; (C) dementia from everything else, and (D) MCI from dementia.
The Qmci-TR was also compared with the SMMSE, as this is widely used in Turkey, although not specific for MCI. A significant, positive strong correlation was found with the SMMSE (r = .80, P < .001), and as expected, the Qmci-TR was more accurate than the SMMSE in discriminating SMC from MCI (AUC of Qmci-TR = 0.80 vs SMMSE = 0.71, 95% CI: 0.54-0.78, respectively, P = .019). In distinguishing MCI from dementia, the Qmci-TR was as accurate as SMMSE with an AUC score of 0.83 compared to AUC of 0.81 (95% CI: 0.70-0.90), P = .56.
Cutoff Scores
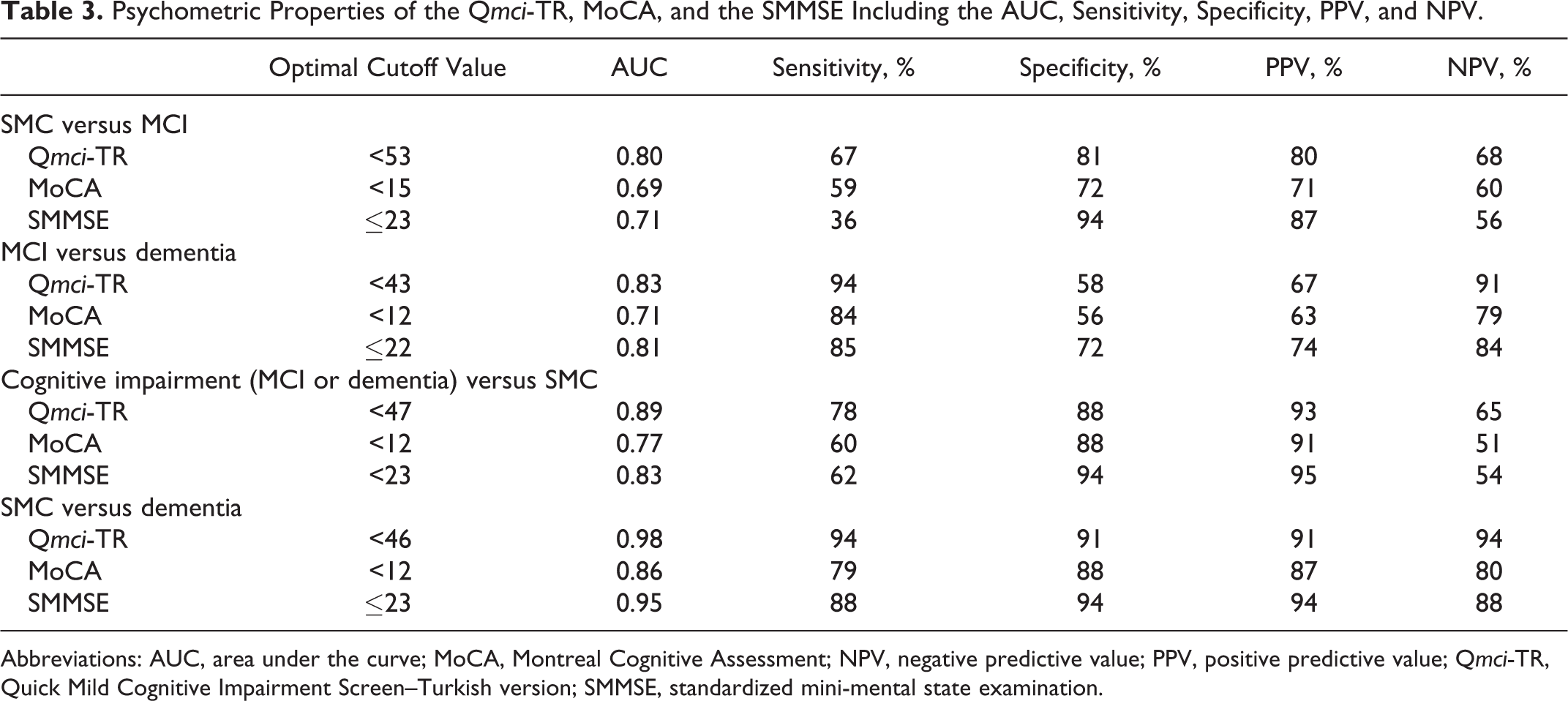
At its optimal cutoff, for differentiating MCI from SMC (<53), calculated using the maximal accuracy approach, the Qmci-TR had a sensitivity of 67% and a specificity of 81%. The MoCA had a sensitivity of 59% with a specificity of 72% at its optimal cutoff (<15). The Qmci-TR was also more sensitive and specific at identifying cognitive impairment (MCI or dementia) with a sensitivity of 78% and specificity of 88% at its optimal cutoff score (<48). The MoCA had lower sensitivity at 60% (cutoff score of <13). The complete list of AUC scores, sensitivity, specificity, positive and negative predictive values of the Qmci-TR, and MoCA in discriminating MCI from SMC and dementia is presented in Table 3.
Psychometric Properties of the Qmci-TR, MoCA, and the SMMSE Including the AUC, Sensitivity, Specificity, PPV, and NPV.
Abbreviations: AUC, area under the curve; MoCA, Montreal Cognitive Assessment; NPV, negative predictive value; PPV, positive predictive value; Qmci-TR, Quick Mild Cognitive Impairment Screen–Turkish version; SMMSE, standardized mini-mental state examination.
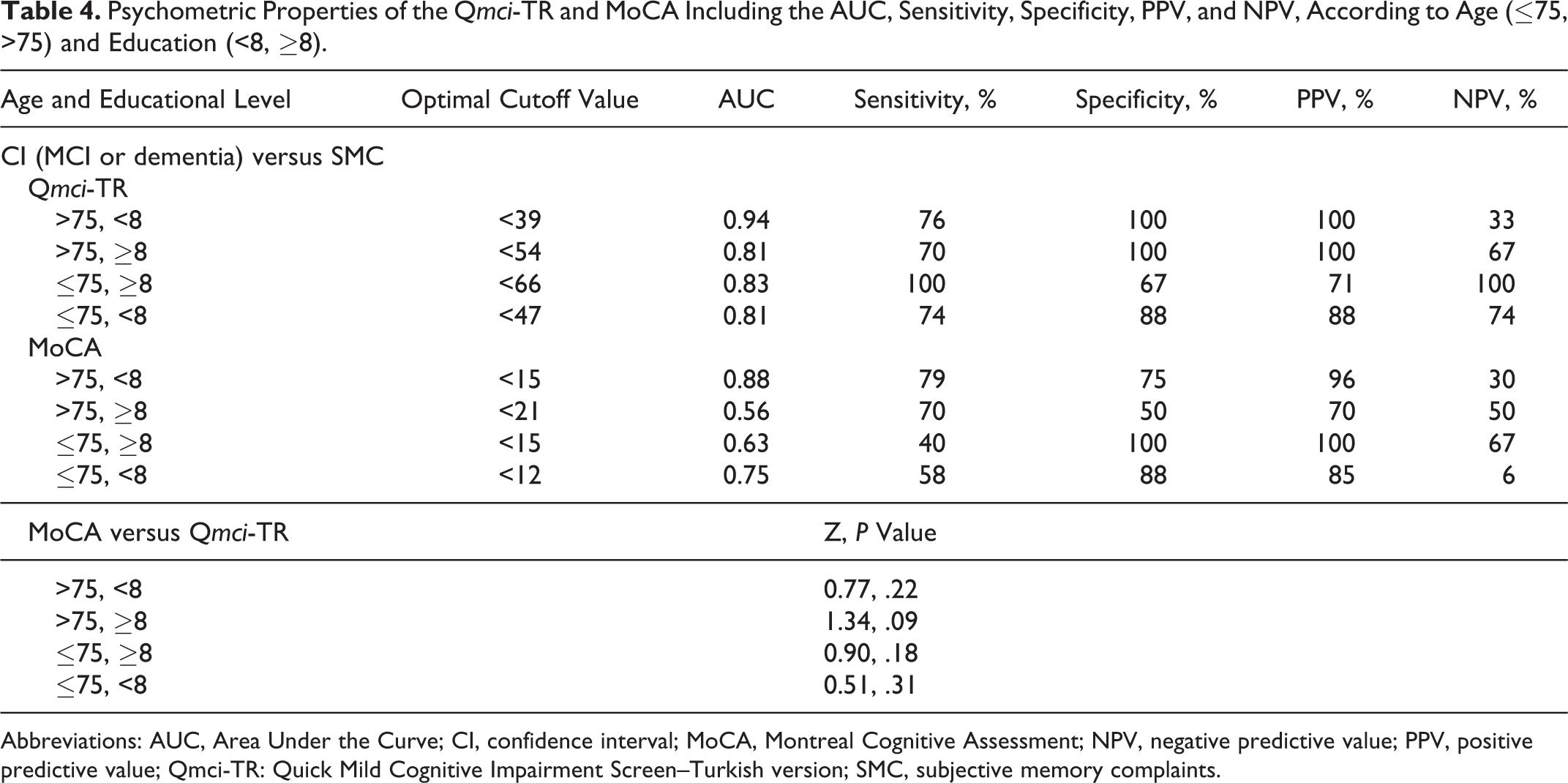
Comparing the psychometric properties of the Qmci-TR and the MoCA according to age and education levels showed that there were no statistically significant differences in accuracy between the 2 instruments (see Table 4). The Qmci-TR was most sensitive for detecting cognitive impairment (differentiating MCI and dementia from SMC) in younger patients (≤75 years) with more education (≥8 years) at a cutoff of <66 with a sensitivity of 100% and specificity of 67%, whereas the MoCA was most sensitive for older patients (>75 years) with less education (<8 years), at a cutoff of <15 with a sensitivity of 79% and specificity of 75%. The Qmci-TR, however, had higher accuracy in identifying cognitive impairment (AUC of 0.94) in older patients with less education than the MoCA (AUC of 0.88), although this was not a significant difference (P = .22). The Qmci-TR produced an AUC > 0.80 irrespective of age or education.
Psychometric Properties of the Qmci-TR and MoCA Including the AUC, Sensitivity, Specificity, PPV, and NPV, According to Age (≤75, >75) and Education (<8, ≥8).
Abbreviations: AUC, Area Under the Curve; CI, confidence interval; MoCA, Montreal Cognitive Assessment; NPV, negative predictive value; PPV, positive predictive value; Qmci-TR: Quick Mild Cognitive Impairment Screen–Turkish version; SMC, subjective memory complaints.
Post Hoc Analysis
Post hoc testing with the Tukey and Levene tests showed that Qmci-TR scores were significantly different from each other in all 3 diagnostic groups: SMC (M = 61.23, SD = 11.33), MCI (M = 45.21, SD = 16.99), and dementia (M = 25.35, SD = 12.24).
Discussion
This study presents the results of the validation of the Turkish version of the Qmci and shows that this rapid cognitive screen for MCI and early dementia seems to be a reliable and valid instrument, and it may be able to differentiate MCI from patients with SMC but normal cognition or dementia in a Turkish geriatric outpatient population.
The Qmci-TR represents the second translation and external validation of the instrument, after its recent validation in Dutch, 27 and adds to the growing evidence supporting its use with patients in busy clinical practice. Although the study is underpowered to show superiority, the results suggest that the Qmci-TR is at least noninferior at discriminating SMC from cognitive impairment (MCI or dementia), compared with the more commonly used MoCA. Given its brevity (median administration time of less than 5 minutes), 23,25 the Qmci may be preferable, particularly where time is limited.
The optimal cutoff scores for the Turkish translations of both the Qmci and MoCA were markedly lower than those previously published in English, which is explained by the lower levels of education and high levels of illiteracy in this older population attending a geriatric clinic as well as the low numbers available for analysis. In this sense, these cutoff scores should not be used in clinical practice. For example, in this study, the optimal cutoff for the Qmci-TR for cognitive impairment was ≤47, which produced a sensitivity of 78% and specificity of 88%, and is much lower than that previously found for similar geriatric memory clinic samples (<62). 25 Likewise, the MoCA’s optimal cutoff for cognitive impairment was <13, which had a sensitivity of only 60% and specificity of 88%. Again, this is much lower than the recommended MoCA cutoff of <26 15 or more recent external validations showing that a lower cutoff may be optimal. 40,44
The relatively low level of accuracy of the MoCA could be explained by the low levels of education in patients in this study, which may have resulted in exaggerated floor effects with both instruments but particularly with the MoCA. The Turkish version of the MoCA has lower sensitivity and specificity for distinguishing MCI in patients with less time in formal education, and MoCA subtests, trail making, and phenomenic fluency in particular require minimal levels of literacy approximating to 5 years of education. 17 This has also been shown for other translations of the MoCA. 45 According to the Turkish Statistical Institue, in 2014, the rate of being uneducated in Turkey is 43.3% in those >65 years. 46 In this study, 31% of all patients (9 patients presenting with SMC, 12 with MCI, and 10 with dementia) were illiterate. There were, however, no significant differences between years in education between diagnostic groups, and differences in accuracy between the 2 instruments became nonsignificant after adjusting for the effects of education. Using different cutoffs for different levels of education is therefore necessary to increase the utility of the Turkish MoCA. 17 On the other hand, the Qmci, which depends less heavily on subtests that require more education, may be more useful in these patients.
The recent validation of the MoCA-Basic 47 in patients with low levels of education highlights the need to adjust all short cognitive screens for illiteracy. Further research is now required to translate and compare the MoCA-Basic with the MoCA, develop and validate a version of the Qmci suitable for those with illiteracy, and compare both adapted versions, while establishing usable cutoff scores.
However, irrespective of the level of age or education, the Qmci-TR had good to excellent accuracy (AUC > 0.80), albeit sensitivity and specificity values varied, likely reflecting the small numbers available for analysis. In the current study, the majority of patients with dementia were classified as mild, stage 4 according to FAST scale. This suggests that the Qmci-TR retains its diagnostic validity in distinguishing MCI from the early stages of dementia, a major diagnostic challenge in clinical practice. This study showed good interrater and test–retest reliabilities, which were found for both MCI and dementia. These findings are consistent with the results of the initial validation. 23
This study has several limitations. Patients diagnosed with SMC but normal cognition were diagnosed using clinical criteria rather than those suggested by consensus panels such as those recently published by the working group of the Subjective Cognitive Decline Initiative. 10 That said, no guidelines have been widely accepted as a gold standard. These patients were significantly younger than those with MCI or dementia, potentially creating bias. However, correcting the ROC curve analysis for the effects of potential confounders confirmed that differences in the AUC scores were likely attributable to the effects of age and education. This relates to the inherent challenges of a cross-sectional study design, which does not allow for adequate matching between groups. Further study should collect age- and education-matched normal controls to further demonstrate the diagnostic accuracy of the instrument and allow comparison with the results of previous validation studies. However, the use of patients presenting with SMC but found to have normal cognition after neuropsychological testing is more reflective of real-life clinical practice, and this makes the study more robust than including large numbers of volunteer controls; the challenge in clinical practice is to differentiate SMC from MCI and dementia, particularly given that treatment options differ between these patients.
The sample size included was small and did not power the study to detect significant differences in accuracy between patients presenting with MCI and SMC, limiting the comparison to a noninferior study. Patients with active depression and less prevalent dementia subtypes were excluded. Active depression was excluded as these patients may have slower reaction times and processing speeds. 48 Lewy body, Parkinson’s disease, and frontotemporal dementia usually present with exaggerated functional deficits often confounding the diagnosis of MCI. Excluding these may have caused spectrum bias, limiting the external generalizability of the study. This said, few patients presented with these subtypes reflecting that patients with these dementia or MCI subtypes infrequently present to geriatric medicine clinics. Finally, the cutoff scores generated by this unrepresentative sample of patients with high levels of illiteracy are not generalizable and should not be used.
In conclusion, the Qmci-TR is a brief and reliable cognitive screen for detecting MCI in a Turkish population. It demonstrates adequate construct validity against the MoCA. Although further research with a suitably powered study and in other settings with younger adults such as neurology, psychiatry, and general practice clinics is now required, this study adds to the evidence that the Qmci and its Turkish translation (Qmci-TR) is useful as a cognitive screen in busy clinical practice, particularly given its short administration time. Further study is also required to calculate usable and representative cutoffs for the Qmci-TR.
Footnotes
Appendix A
Qmci-TR
1. Yönelim
2. Kelime Kayıt Etme Başlamak için şunu söyleyin:
Skor __________ / 5 Alternatif kelime grupları şunları içerir:
3. Saat Çizme
4. Gecikmiş Geri Çağırma Başlamak için şunu söyleyin:

köpek
yağmur
Tereyağı
sevgi
kapı
5. Sözel Akıcılık
6. Mantıksal Bellek “Size kısa bir hikaye okuyacağım. Okumayı bitirdikten sonra bana hikayenin anlatabildiğiniz kadar çok kısmını anlatmanızı istiyorum. Tamam mı?” [hasta kabul ettiğini belirttikten sonra her kelime bölümünü yaklaşık 1 saniyede olmak üzere paragrafı okumaya başlayın] “Kırmızı…tilki…sürülmüş.…….…üzerinde oluşmaktaydı.” Skor __________ / 30
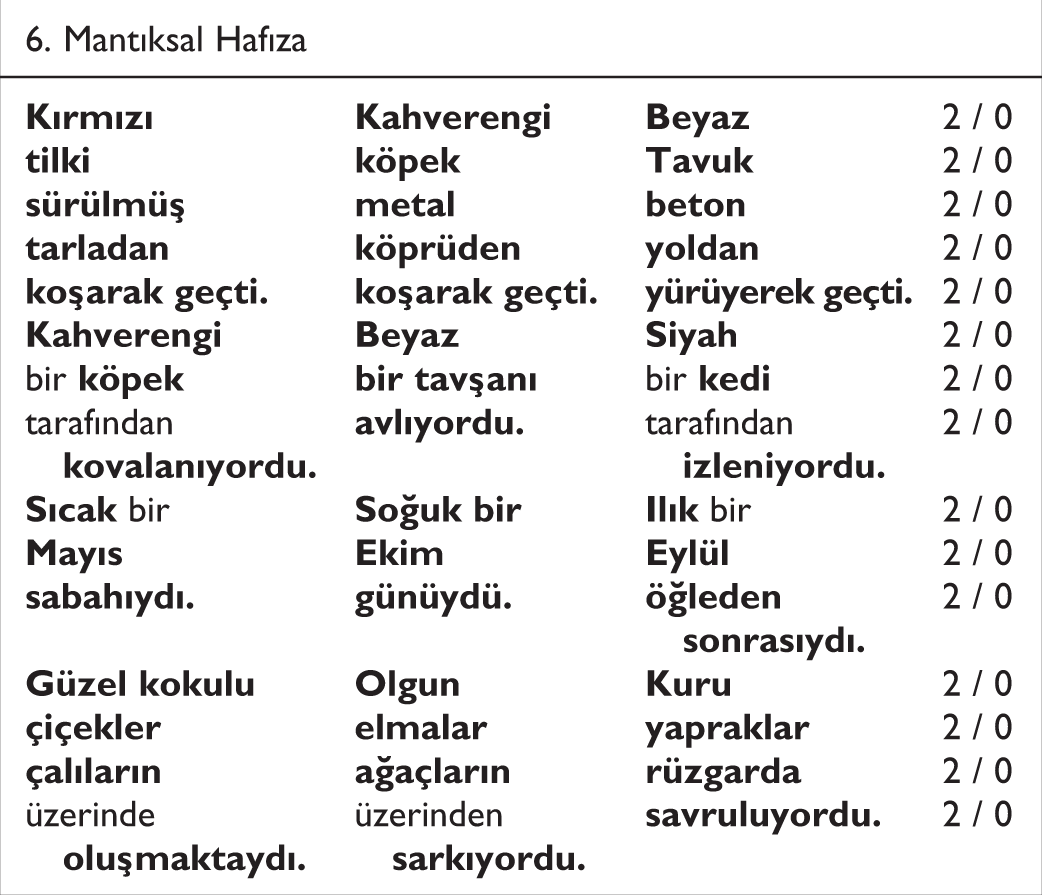
6. Mantıksal Hafıza
2 / 0
2 / 0
2 / 0
2 / 0
2 / 0
2 / 0
bir
bir
2 / 0
tarafından
tarafından
2 / 0
2 / 0
2 / 0
2 / 0
2 / 0
2 / 0
2 / 0
üzerinde
üzerinden
2 / 0

____________________
/ 100
Appendix B
1. Yönelim ✎ Puanlama Doğru cevap için 2 puan, yanlış cevaplar için 1 puan, hiç cevap yok veya kavramsal olarak ilişkisiz cevap için 0 puan (aşağıdaki detaylara bakınız). ⌚ Her cevap için en fazla 10 saniye.
Başlamak için şöyle söyleyin:
Skor __________ / 10
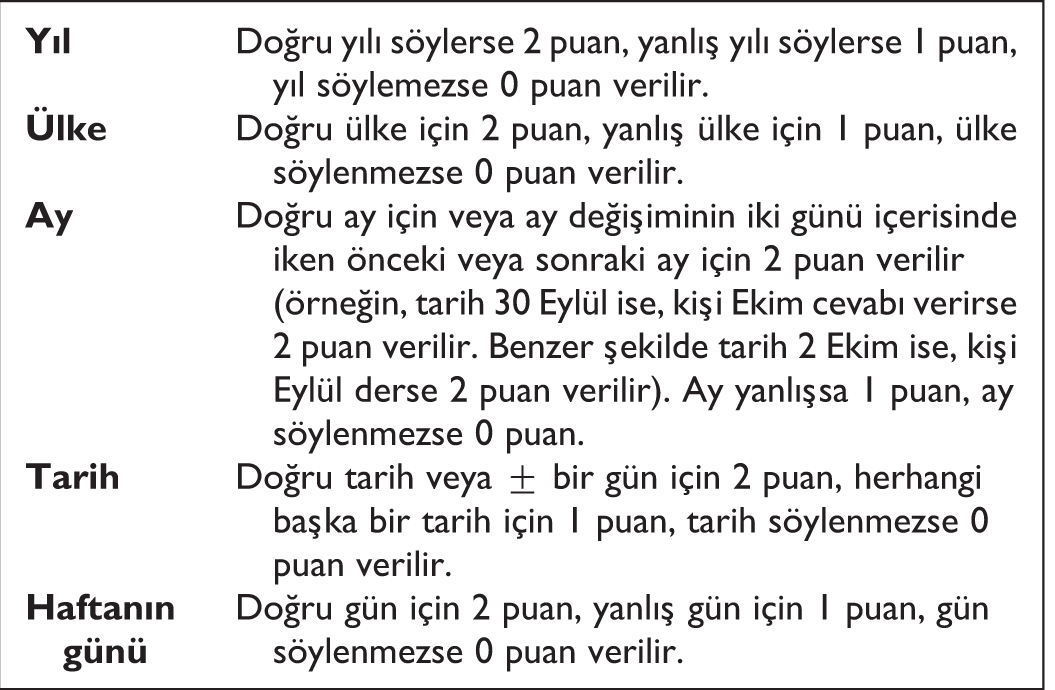
Doğru yılı söylerse 2 puan, yanlış yılı söylerse 1 puan, yıl söylemezse 0 puan verilir.
Doğru ülke için 2 puan, yanlış ülke için 1 puan, ülke söylenmezse 0 puan verilir.
Doğru ay için veya ay değişiminin iki günü içerisinde iken önceki veya sonraki ay için 2 puan verilir (örneğin, tarih 30 Eylül ise, kişi Ekim cevabı verirse 2 puan verilir. Benzer şekilde tarih 2 Ekim ise, kişi Eylül derse 2 puan verilir). Ay yanlışsa 1 puan, ay söylenmezse 0 puan.
Doğru tarih veya ± bir gün için 2 puan, herhangi başka bir tarih için 1 puan, tarih söylenmezse 0 puan verilir.
Doğru gün için 2 puan, yanlış gün için 1 puan, gün söylenmezse 0 puan verilir.
__________
__________
__________
__________
__________
2. Kelime Kayıt Etme Uygulama ve Puanlama Kılavuzu ✎
İlk okuma ardından hatırlanan her kelime için 1 puan verin. Kişi beşini birden hatırlarsa beş maddeyi bir seferde tekrarlayın ve saat çizme testine geçin. Kişi beşini birden hatırlayamazsa 5 maddeyi tekrarlayın ve hastanın tekrarlamasını isteyin. Bunu kişi doğru bir şekilde 5 maddeyi birden hatırlayana kadar ya da en fazla 3 deneme olacak şekilde tekrarlayın. İkinci ve üçüncü denemeler için puan vermeyin. Bu denemeler kişinin gecikmiş hatırlama testine hazırlanması için öğrenmesine yardım etmek içindir. ⌚ Kelimeleri çok dikkatlice saniyede bir tane olacak şekilde söyleyin. Hatırlama için 10 saniye zaman tanıyın. Başlamak için şöyle söyleyin:
Bitince şöyle söyleyin: Alternatif kelime grupları şunları içerir:

Köpek
yağmur
Tereyağı
sevgi
Kapı

3. Saat Çizme
Uygulama ve Puanlama Kılavuzu
✎
Transparan puanlama şablonunu hastanın tamamlanmış saatinin dairesinin üzerine koyun. “12” yi hizalamak için şablon dairesini döndürün. 1, 2, 4, 5, 7, 8, 10 ve 11 doğru kadranlardaysa her birine 1’er puan verin. 12, 3, 6 ve 9 kadran çizgilerine değiyorsa her birine 1’er puan verin. Tekrarlayan her sayı için veya 12’nin üzerinde her sayı için 1 puan çıkarın. (Hasta “12” yazmadıysa şablonu 3, 6, veya 9 ile hizalayın.)
Saatin kollarının yerleşimini uçlarına ve merkez noktasına göre puanlayın. Kesikli çizgiler arasındaki her kol için 1’er puan verin. Merkez noktasında birleşen kollar için 1 puan verin. ⌚
Başlamak için:
Hastaya üzerinde önceden çizilmiş daire olan kağıdı ve kalemi verin. Şöyle söyleyin:
Her evrede hatırlatma yapabilirsiniz…“sayıları yerleştirin.…saati on biri on geçiyor olacak şekilde yapın”.
4. Gecikmiş Geri Çağırma
5. Sözel Akıcılık
✎
En fazla 40 kelimeye kadar doğru hatırlanan her kelime için ½’ şer puan verin. Son skoru yukarıya yuvarlayın. Farklı soneklere sahip kelimeleri iki kere puanlamayın (örn. balık/balıklar, fare/fareler gibi). Aynı grubun farklı türlerini kabul edin (örn. karga, bülbül, serçe, ördek gibi.).
Alternatif formlarında meyve ve sebzeler, şehirler ve kasabalar sorulabilir. ⌚
60 saniye. Hastanın söylediği her kelimeyi yazın. (Daha hızlı hastalar için bir çeşit “kısayol” geliştirmeniz gerekebilir. Örneğin, her kelimenin ilk 3 harfini yazıp sonradan tamamlamak gibi.)
Başlamak için şöyle söyleyin: “Bir dakika içinde sayabildiğiniz kadar çok hayvan ismi sayın. Hazır mısınız? Başlayın.”
6. Mantıksal Bellek
✎ Puanlama
Harfi harfine hatırlanmış her doğru kelime için 2’şer puan verin. 2 puan için her bölümdeki koyu belirtilmiş her kelimenin hatırlanması gerekir. Aksi takdirde 0 puan verin. Hatırlama herhangi bir sırayla olabilir. ⌚
Başlamak için şöyle söyleyin:
“Size kısa bir hikaye okuyacağım. Okumayı bitirdikten sonra bana hikayenin anlatabildiğiniz kadar çok kısmını anlatmanızı istiyorum. Tamam mı?” [hasta kabul ettiğini belirttikten sonra her kelime bölümünü yaklaşık 1 saniyede olmak üzere paragrafı okumaya başlayın] “Kırmızı…tilki…sürülmüş.…….…üzerinde oluşmaktaydı.”
Transparan puanlama şablonunu hastanın tamamlanmış saatinin dairesinin üzerine şablonun “12”si hastanın “12”sinin üzerine gelecek şekilde koyun. Şablonu sayı ve kolların puanlarının en yüksek olacağı şekilde ayarlayın. Toplam skor 15’dir. Skor sayfasına skorları aşağıdaki gibi kaydedin.
12, 3, 6 ve 9 için ilgili çizgilere değiyorsa her birine bir (1) puan verin, değmiyorsa sıfır (0) puan verin ve sayı ihmal edilmişse sıfır (0) puan verin. 1, 2, 4, 5, 7, 8, 10 ve 11 için doğru kadrandaki her sayı için bir (1) puan verin, sayı kadranın dışındaysa sıfır (0) puan verin ve sayı ihmal edilmişse sıfır (0) puan verin. Tekrar eden her sayı için veya 12’nin üzerindeki her sayı için bir puan çıkarın.
Kolun bütününün yerleştirilmesine puan verin. Kollar aralık içerisine çizildiyse her kol için bir (1) puan verin; kollar hazırlanmış çizgilerin dışında çizildiyse veya çizilmediyse sıfır (0) puan verin. Kollar merkez noktasında birleşiyorsa bir (1) puan verin.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.