
Abstract

Introduction
Dementia is a chronic neurodegenerative disease with loss of memory, problem-solving and other cognitive abilities that are severe enough to interfere with daily life of older people. According to Alzheimer’s Disease International, 1 there were about four thousand people living with dementia in Macao and it was expected that the number of people living with dementia would increase rapidly, resulting of increases in life expectancy at birth over the past years. 2 In response to the significant health and social burden incurred by dementia, Macao Special Administrative Region Government had launched Macao Dementia Policy which included a 10-year strategic framework to build dementia friendly community and integrated health and social services in 2016, 3 of which the Macao Dementia Registry (MDR) was a powerful tool for monitoring of clinical care to facilitate population-level surveillance over time. Methods of identifying cases of dementia differentiated between registries but usually included reporting from clinics and hospitals. However, diagnosis occurred in a variety of settings and inclusive of the whole population could be challenging for a dementia registry. Therefore, understanding and studying the cohort with dementia captured within the registry could significantly contribute to the understanding of health service use, medicines, hospitalizations, mortality and other information. 4 The current evaluation had examined (1) the demographic and clinical characteristics of people living with dementia and (2) the comparability of data captured in the MDR dementia registry with selected established international dementia registries. This would allow for better understanding of the characteristics and limitations of this MDR cohort for monitoring the quality of care and outcomes for people living with dementia in Macao.
Cohort Description
Design and Data Sources
The study presented the results of a cross-sectional evaluation of the people with dementia identified by assessment data in the Dementia Medical Center and all the eleven Health Centers between September 21st, 2016 and July 22nd, 2021 in Macao. The entry point to the MDR cohort was in the Dementia Medical Center and all the eleven Health Centers where assessment and a recording of dementia were conducted and a person was identified from dementia medication prescribing records.
Dementia Ascertainment
Dementia was determined through eligibility assessments in the Macao Dementia Medical Center. During assessments, assessors made records of major diseases or disorders along with documented evidence of a diagnosis from doctor, which all had an impact on the person’s need for assistance with activities of daily living and social participation. Assessors could record one or more types of dementia or had the option to classify the dementia as ‘unspecified’ based on the medical record. In addition, medicines prescribed for the treatment of Alzheimer’s disease were not dispensed for any other reason, therefore, any person with who had been dispensed Donepenzil, Galantamine, Rivastigmine or Memantine could be classified as having dementia. 5
Data Set
Comparison of Dataset Available of Macao Dementia Registry Cohort and International Dementia Registries.

aInternational Classification of Diseases, version 10, Australian Modification.
While most dementia registries included the Mini-Mental Status Examination (MMSE), the copyright restrictions had precluded its widespread clinical use. Instead, the Montreal Cognitive Assessment (MoCA) was scheduled to be conducted where cognitive impairment was suspected or known. A Geriatric Depression Scale (GDS-15) was conducted where symptoms of depression and dysthymia were present. Functional dependence was rated across domains, including nutrition, mobility, personal hygiene, toileting, continence, home maintenance and transport, though a validated measure as Barthel Index (BI) used in other registries was also included in the MDR dementia registry.
Cohort Characteristics
Comparison of Demographic Characteristics of Macao Dementia Registry Cohort and International Dementia Registries.
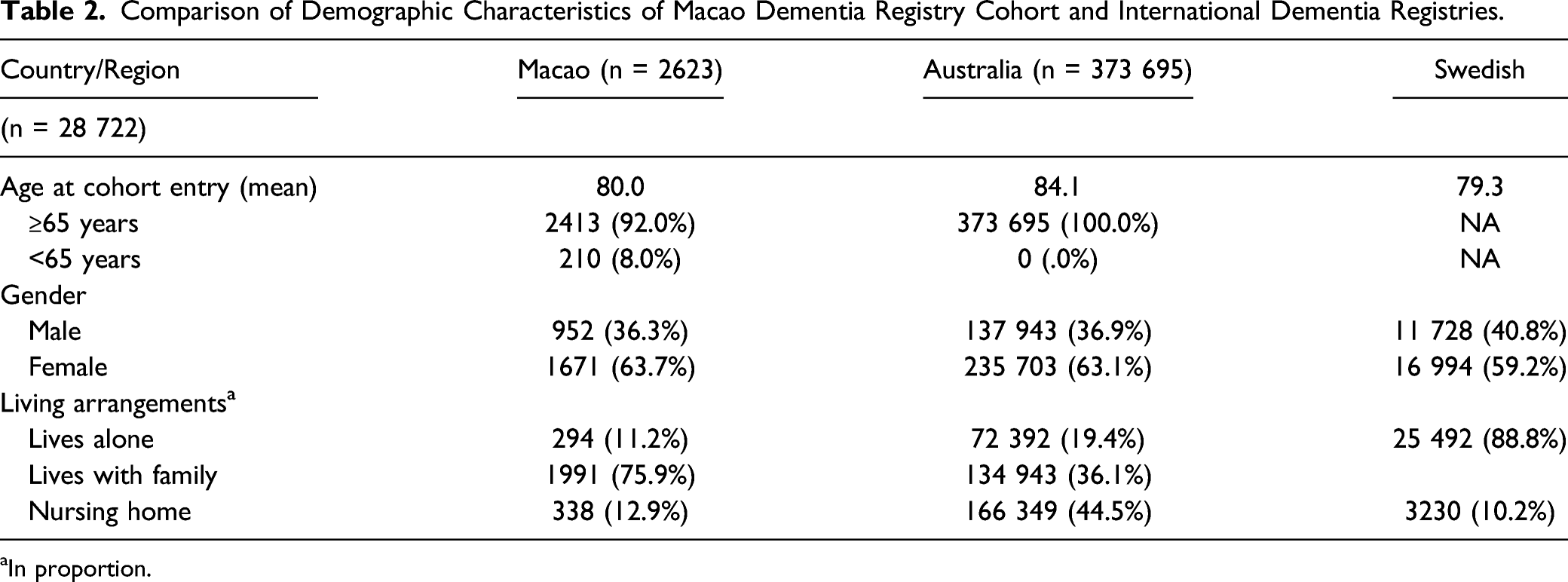
aIn proportion.
Comparison of Clinical Characteristics of Macao Dementia Registry Cohort and International Dementia Registries.

aIn proportion.
Discussion
The only and largest sample and regional coverage provided by the Registry were key strengths of the MDR cohort. The MDR included the only and largest existing population-based sample of people with dementia in Macao and was acting as representative of the population in many ways, including demographic characteristics and clinical diversity. The MDR dementia cohort was, therefore, a powerful resource and could facilitate monitoring of clinical care and determinants of important outcomes including institutionalization and mortality over time. Furthermore, the MDR dementia cohort might inform the policymaking in Macao and future development of the Registry. Following a Chinese traditional culture of emphasis on family values and harmony interpersonal relationship in Macao, there was a greater proportion of persons with dementia who lived with their family members (75.9%), more than a double compared to those in Australia (36.1%). This might underscore the significant need for the strong effort to support the family caregivers in Macao Dementia Policy that was launched in 2016 as the 27th globally and was aligned with WHO Global Action Plan on the Public Health Response to Dementia 2017-2025. 8 Macao Dementia Policy, which included a 10-year strategic framework to establish dementia friendly communities across the region, had been highly praised by Alzheimer’s Disease International in 2018 as a positive model. 3
Despite these benefits, there were some limitations to the MDR dementia cohort. First, the MDR could not capture people with dementia who did not have a diagnosis in medical history. Approximately half of people with dementia in Macao were estimated to receive a diagnosis, 3 and delays in diagnosis were common.9,10 People who received a diagnosis tended to have more severe impairment, have insight into their impairment, and be married. 11 The MDR was not able to capture these individuals who had not been diagnosed and these factors introduced a sampling bias to the Cohort. Second, the data available in the MDR were not collected for research purposes and therefore might have limited internal validity. The accuracy of clinical and demographic data also relied on assessors who might not have been necessarily trained in research data collection or in dementia care. The accuracy of the dementia diagnosis recorded in the MDR was dependent on the skills and resources available to the clinician who made the diagnosis.
Conclusion
There were 2623 people living with dementia in the MDR and the MDR included the only and largest existing population-based sample of people with dementia in Macao and was representative of the population in many ways, including demographic characteristics and clinical diversity. The MDR was, therefore, a powerful resource and could facilitate monitoring of clinical care and determinants of important outcomes including institutionalization and mortality over time. Furthermore, the MDR dementia cohort might inform the policymaking in Macao and future development of the Registry.
Supplemental Material
sj-pdf-1-aja-10.1177_15333175211067124 – Supplemental Material for Cohort Profile: The Dementia Registry in Macao
Supplemental Material, sj-pdf-1-aja-10.1177_15333175211067124 for Cohort Profile: The Dementia Registry in Macao by Sio Mui Wong, Wen Zeng, and Iek Long Lo in American Journal of Alzheimer's Disease & Other Dementias®
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.