
Abstract
Little is known about multiple medicines and initial therapy among people with dementia. To examine the effect of multiple medicines on the initiation of anti-dementia therapy in patients diagnosed with cognitive impairment (CI), a retrospective study with 2742 CI patients was conducted based on the outpatients’ medical records. The dementias receiving 1–2 drugs were more likely to be prescribed with anti-dementia (one drug: OR = 1.877; two drugs: OR = 1.770) and psychotropic (one drug: OR = 1.980) treatment, whereas had lower chances of receiving psychotropic medication with the combinations of more than three drugs (Alzheimer’s disease: OR = .365; vascular dementia: OR = .940; frontotemporal lobe degeneration: OR = .957; and dementia with Lewy bodies/Parkinson’s disease dementia: OR = .952). Multiple medicines can affect anti-dementia therapy initiation in dementia patients and should be paid extreme caution.
Keywords
Significance Statement
1. Half of the participants with cognitive impairment (52.3%) received initial prescriptions at their first visit. 2. Combined treatment could affect initiation of anti-dementia and psychotropic therapy in dementia patients.
Introduction
Dementia is a chronic, progressive disease characterized by the gradual loss of cognitive function. 1 With the aging of the global population, dementia has become a global public health problem. With this increase in the aged population, the number of people living with dementia has also increased, especially in low- and middle-income countries. 2 According to the 2013 Alzheimer’s Disease International report, approximately 47 million people would suffer from dementia in 2015 3 ; by 2030, the number of people living with dementia is expected to reach estimated 75.6 million and the prevalence of dementia will be triple by 2050. 4 Dementia has extremely high disability and mortality rates and has become an important killer that seriously threatens the quality of life and health of the elderly.5‐7 It is crucial to get right therapy for dementia patients as much as possible, no matter drug and non-drug treatments.
Drug interventions play an important role in anti-dementia treatment, and they mainly include anti-dementia and psychoactive drugs.8,9 Anti-dementia drugs include cholinesterase inhibitors (ChEI) (such as donepezil, rivastigmine, and galantamine) to treat mild to moderate dementia. Often, dementia is accompanied by behavioral and psychological symptoms of dementia (BPSD). Atypical neuroleptics drugs, selective serotonin reuptake inhibitors, benzodiazepines, and non-benzodiazepines have become first-line drugs to treat behavioral symptoms of dementia. However, with the use of atypical neuroleptics, the risk of death increases. Since most cognitive impairment (CI) patients are the elders, it is likely that most of them get comorbidities 10 and receive several different drugs. Thus, multiple medicines are very common in dementias, and drug interactions potentially affect the health of patients and pesticide effect of anti-dementia drugs. Study showed a negative association between multiple medicines and anti-dementia therapy initiation in general practices in Germany. 11 However, there still is lack of evidence focused on the association between multiple medicines and the initiation of anti-dementia treatment in China.
Meanwhile, more and more dementias choose to live in primary medical units or nursing homes to receive professional care and treatment, which provides challenges for doctors working there. Due to the un-cooperation, sensitivity to drugs, or severe disability, especially in patients with BPSD, extra attention should be paid to medication. Therefore, this retrospective study aimed to examine the influence of multiple medicines on the initiation of anti-dementia therapy in patients diagnosed with CI in China and share treatment experience to primary clinicians.
Materials and Methods
Participants and Data Collection
Retrospective data were collected from the Memory Clinic of Tianjin Huanhu Hospital from January 2011 to October 2018. Patients included those who presented to the memory clinic with complaints about decline in memory, or those whose memory problems were noticed by friends or relatives who came to the clinic accompanied. The demographic data and medical histories (such as comorbidities and habits of smoking and drinking) of all patients were recorded, as well as the drugs used within the 3 months prior to first dementia diagnosis. Nearly all of the patients completed Chinese Mini-Mental State Examination (C-MMSE), the Montreal Cognitive Assessment (MoCA), 12 the Clock-drawing Test, 13 the activities of daily living (ADL), 14 and the Neuropsychiatric Inventory (NPI). 15 The C-MMSE and MoCA both range from 30 (best) to zero (worst). The Clinical Dementia Rating 16 was conducted to establish the severity of dementia. If drugs were prescribed, these were recorded, with the focus on anti-dementia agents, psychoactive drugs, as well as treatments for previously diagnosed conditions. The study was approved by the Committee for Medical Research Ethics at Tianjin Huanhu Hospital and the Tianjin Health Bureau.
Diagnostic Criteria
Alzheimer’s disease (AD) and vascular dementia (VD) were diagnosed according to the criteria detailed by the National Institute of Neurological and Communicative Disorders and Stroke (NINCDS) and the Alzheimer’s Disease and Related Disorders Association (ADRDA) (1984) 17 and the Diagnostic and Statistical Manual of Mental Disorders (DSM–IV). 18 Frontotemporal lobe degeneration (FTLD) 19 and dementia with Lewy bodies/Parkinson’s disease dementia (DLB/PDD) were diagnosed according to the criteria proposed by McKeith in 1996 20 and Murat in 2007. 21 Based on the International Working Group on mild cognitive impairment (MCI) diagnosis, 22 we developed the following operational criteria for MCI: (i) cognitive decline was complained by the patient or caregiver or was found by an experienced clinician; (ii) objective evidence of cognitive decline in one or more functional fields was confirmed on neuropsychological estimation; (iii) complex instrumental daily abilities could be slightly impaired, but basic ADL was relatively normal; (iv) the patient’s symptoms did not meet the NINCDS-ADRDA (1984) diagnostic criteria for dementia.
Data Analyses
Descriptive statistics were used to analyze the demographic data, types of CI, cognitive profiles, and drug prescriptions. Logistic regression analyses were conducted to study the impact of the number of different drugs on the reception of anti-dementia therapy. All data were analyzed using the Statistical Package for the Social Sciences version 22.0 (SPSS 22.0, IBM, Armonk, NY, USA). P-values < .05 were considered statistically significant.
Results
Demographic and Clinical Characteristics
Demographic and clinical characteristics of participants.
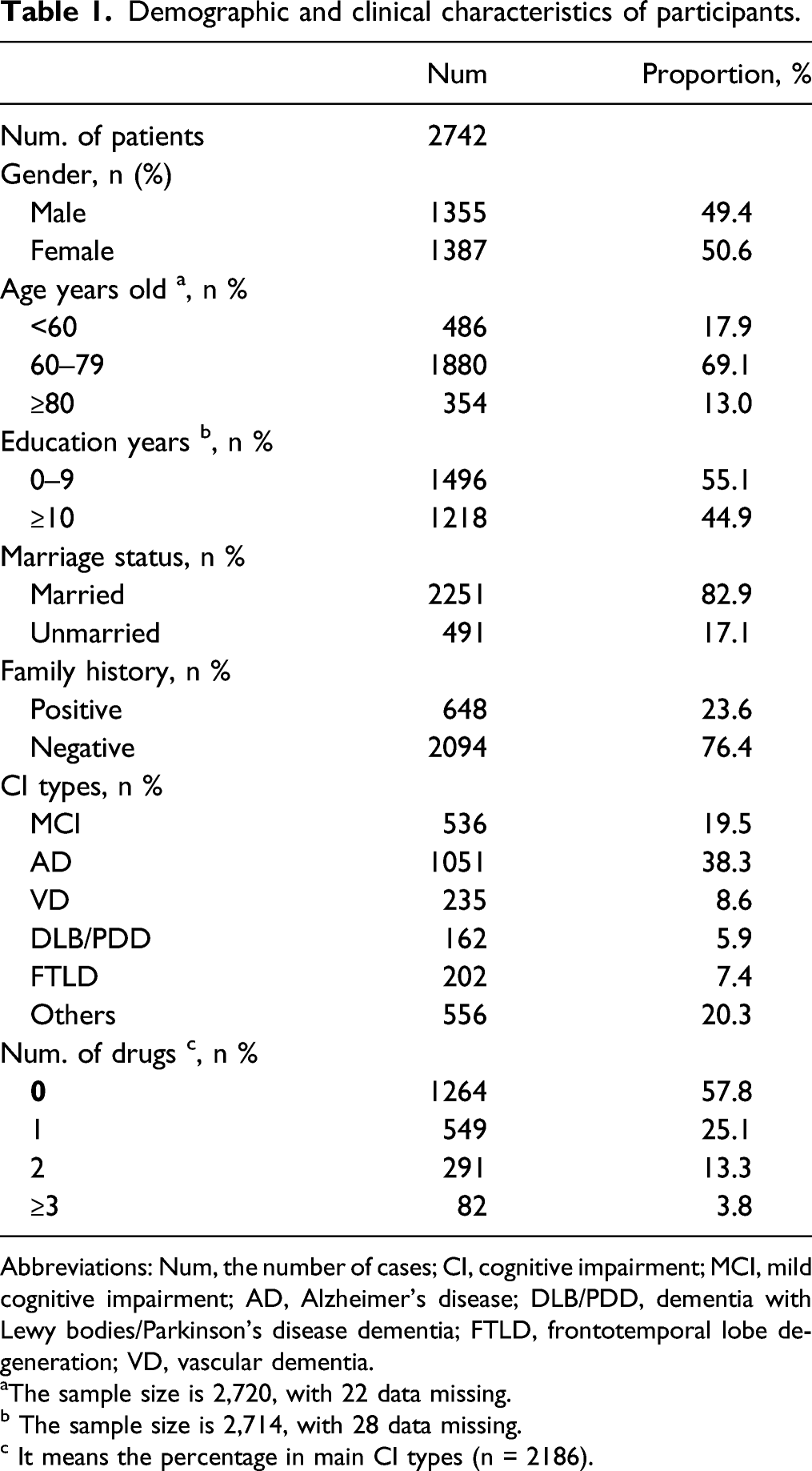
Abbreviations: Num, the number of cases; CI, cognitive impairment; MCI, mild cognitive impairment; AD, Alzheimer’s disease; DLB/PDD, dementia with Lewy bodies/Parkinson’s disease dementia; FTLD, frontotemporal lobe degeneration; VD, vascular dementia.
aThe sample size is 2,720, with 22 data missing.
b The sample size is 2,714, with 28 data missing.
c It means the percentage in main CI types (n = 2186).
Cognitive profiles of general dementia patients.

Abbreviations: SD, standard deviation; C-MMSE, Chinese Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; ADL, Activities of Daily Living; NPI, Neuropsychiatric Inventory; CDR, Clinical Dementia Rating.
Mean NPI scores severity × frequency; range 0-12 and percentage of patients with symptoms.

Initial drug prescriptions in main types of CI patients.
Initial drug prescriptions for patients with CI.

Abbreviations: CI, cognitive impairment; MCI, mild cognitive impairment; AD, Alzheimer’s dementia; FTLD, frontotemporal lobe dementia; DLB, Lewy bodies dementia; PDD, Parkinson’s disease dementia; VD, vascular dementia.
aOthers including anti-Parkinson drugs/neuroleptics drugs/vitamins and folic acid and other drugs of underlying condition.
bThe total number of patients receiving anti-dementia drugs.
cThe total number of patients in each category.
Association between the initiation of anti-dementia therapy and pre-defined variables
Association between anti-dementia/neuroleptics therapy initiation and combination treatment.

Abbreviations: ORs, odds ratios; CI, confidence interval; AD, Alzheimer’s dementia; VD, vascular dementia; FTLD, frontotemporal lobe dementia; DLB, Lewy bodies dementia; PDD, Parkinson’s disease dementia; MCI, mild cognitive impairment.
aGroups were classified by the number of drugs (except for anti-dementia or neuroleptics medication) taken before the patients’ initial visit.
bProportions of samples receiving anti-dementia medication at initial therapy.
cProportions of samples receiving psychotropic medication at initial therapy.
Discussion
To our knowledge, there were few studies to examine multiple medicines and initial therapies among people with dementia. About a half of CI patients received multiple medicines in our study. Additionally, it was showed that patients with one drug were more likely to receive anti-dementia and neuroleptic treatment. Multiple medicines were associated with a similar decrease in the odds of initiating neuroleptic treatment in most types of dementia.
Globally, the symptomatic medication used to against dementia increased from 2008 to 2018 along with the rising prevalence of dementia, which may indicate a growing demand of pharmacological treatment for the management of dementia. 23 Combination treatment, the concurrent use of two or more medications by an individual, 24 was widespread in the older population and more in people with dementia. 25 In recent years, there has been a growing interest in the relationship between dementia, combination treatment, and initial medication. It has been found to be associated with several negative health outcomes, including dementia. A recent German study showed a negative association between combination treatment and anti-dementia therapy initiation in general practices. In a study included 822 participants with CI showed that combination treatment increased the risk of mortality towards the end of an individual’s life. 26 Meanwhile, a study with 4668 dementia patients showed that combination treatment was significantly associated with emergency department visit, hospitalization, unplanned hospital admission, and death within two years. 27 Leelakanok suggested that the increase in the categorical threshold from 5 or more, to 10 or more, led to an increase in the risk of dementia from 30% to 52%, showing a dose-dependent relationship between the threshold value of combination treatment and dementia. 28 Patients receiving six or more drugs were significantly less likely to be prescribed with anti-dementia treatment when compared to those without any drug (6–9 drugs: OR = .75; ≥10 drugs: OR = .58).(11) These findings were corroborated by Lai 29 and Park et al. 30 based on large population.
We found that half of the patients in our study had one or more drugs prescribed at their first clinic visits, which was the samewith that in India 31 and Thailand. 32 Anti-dementia drugs are mostly prescribed with ChEI (donepezil, rivastigmine, and galantamine), which can improve the bioavailability by slowing down the degradation of neurotransmitter acetylcholine. There is also the application of N-methyl-D-aspartic acid (NMDA) receptor antagonist (memantine) in the treatment of severe dementia and BPSD by reducing the excitotoxicity mechanism of glutamate receptor. A few anti-amyloid agents (aducanumab, gantenerumab, BAN2401, and ALZ-801) have shown meaningful efficacy in clinical trials. 33 Aducanumab is recently approved by the US Food and Drug Administration (FDA) for the treatment of AD, with once-a-month intravenous injection. 34 Several studies have shown that the combination was significantly better than either medication alone and provided synergistic benefits in dementia treatment.35–37 The donepezil–memantine combination is the only FDA–approved drugs for the treatment of AD, while the galantamine–memantine combination is considered having significantly better efficacy for cognitive functions than the donepezil–memantine combination in AD.37–39 Galantamine–memantine combination is typically prescribed for the treatment of AD and significantly effective for cognition 40 by decreasing lactate concentration, 41 or improving brain makers including brain-derived neurotrophic factor, kynurenic acid, N-acetylaspartate, NMDA, and so on via α7nACh and NMDA receptors. 42 What is more, galantamine–memantine combination could improve cognition and regulate positive and negative symptoms in neuropsychiatric disorders.35,40,43 Although this combination is off-label used in clinical practice, more RCTs are needed to support this combination. Perhaps in the future, the galantamine–memantine–aducanumab combination will be useful to treat AD and other complex diseases.
When patients suffer from BPSD, they should be prescribed with psychoactive drugs only if specifically required or other treatments have failed. Among psychotropic medications, antidepressants/anxiolytics were the most common drugs used, followed by neuroleptics. Many patients with BPSD will not need psychotropic medications and can be managed successfully with nonpharmacologic techniques. Because some patients with dementia are highly sensitive to the effects (especially adverse effects) of psychotropic medications, short-term mortality increased by 2 to 3 times with their use. 44 In this retrospective study, we found that Chinese CI patients had less combined drugs, most of whom had less than 3 drugs. We also showed that CI patients, not all types, with 1–2 drugs were more likely to receive anti-dementia treatment compared to those without drug. It may be related to the number of comorbidities, which increase the risk of dementia. In contrast, it showed a roughly negative trend for drugs and psychotropic medications for dementias. Patients (with MCI, AD, or FTLD) who took 1–2 drugs were more likely to receive anti-dementia treatment, no matter in women or men. For AD patients used one drug were more likely to receive neuroleptic therapy (obvious significance). Overall, the choice of neuroleptic medication was less, and more cautious should be paid when took more than three drugs, but not significantly different. We give patients intervention of anti-dementia after being diagnosed with dementia as soon as possible while less psychotropic medication in experience.
We used real-world data from clinic where diagnoses were recorded, allowing for no recall bias. The limitations still exist. The results of this retrospective study are from single memory clinic and the small samples should be mentioned firstly. Meanwhile, we are unable to use galantamine at patients’ initial prescription because of hospital constraints, thereby the proportion of anti-dementia drugs reported here cannot fully represent the medication situation of various types of dementia, and further research and analysis are still needed. Moreover, lack of data regarding the potential existence of other chronic conditions, which were important factors in the anti-dementia therapy. Finally, when no anti-dementia drug was prescribed, we had no analysis about the number of drugs.
Treatment outcomes for older dementia patients, especially with multiple medical comorbidities, are not like those observed for younger populations. Anti-dementia and neuroleptic medication can be useful for treating CI in older patients but once these patients have responded to combination treatment, it is not clear how long older patients should continue taking these medications, while the underlying comorbidity treatment should be the primary at any point. Older patients with dementia tend to have combination treatment, complicating anti-dementia treatment not only because the potential for drug–drug interactions but also the addition of another drug increases the complexity of pharmacy management.
Conclusions
Overall, there was a positive association between combination treatment (<3 drugs) and anti-dementia therapy initiation in dementia patients. Anti-dementia should be early treatment and neuroleptic medication should be extremely cautioned. Our study indicates the need for integrated response from general health professionals and multidisciplinary dementia specialists, to improve drug therapy in people with dementia.
Footnotes
Acknowledgments
The authors would like to thank Jing Li (Tianjin Huanhu Hospital, Tianjin, China) for her efforts on data collection and input.
Conflict of Interests Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
The Ethics Committee of the Tianjin Huanhu Hospital gave approval to conduct this study (2011-1).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation [grant number 82171182], Science and Technology Project of Tianjin Municipal Health and Health Committee [grant number ZC20121 and KJ20048].