
Abstract
Objective:
To identify characteristics associated with an increased risk of cardiovascular events in patients diagnosed with Alzheimer disease (AD) and treated with antidementia medications.
Methods:
Demographics, diagnoses, and medication usage of 30 433 Medicare patients were analyzed using 2006 to 2013 claims data and a combined model of screening, ranking and stepwise logistic regressions to evaluate factors associated with composite outcomes of 6 cardiovascular events.
Results:
Incidence rate of at least 1 cardiovascular event was 25.1%. Fifty-five factors were identified from the 10 381 candidate variables by the combined model with a c-statistic of 67% and an accuracy of 75%. Factors associated with increased risk of cardiovascular events include history of heart rhythm disorders, alteration of consciousness (odds ratio [OR]: 1.25; 95% confidence interval [CI]: 1.14-1.36), and usage of β-blockers (OR: 1.19; 95% CI: 1.13-1.27).
Conclusions:
Clinicians should consider the increased risk of cardiovascular events in patients with AD with heart rhythm disorders and on β-blockers.
Introduction
Alzheimer disease (AD) is a neurodegenerative disease characterized by progressive cognitive impairment and accounts for 69.9% of all dementia cases. 1 The estimated prevalence of AD among Medicare beneficiaries was 10.8% in 2017. 2
Currently, there are 4 pharmacological agents available for delaying the cognitive impairment progression associated with AD, including 3 acetyl cholinesterase inhibitors (AChEIs)—donepezil, rivastigmine, and galantamine, and 1 N-methyl-D-aspartic acid-type glutamate receptor antagonist—memantine. 3,4 Adverse cardiovascular events have been reported in patients treated with all 4 drugs. 5 -12 There is evidence of increased risk of syncope and bradycardia with AChEIs, 5 -9 and several case reports alerted the risk of atrioventricular block, ventricular tachycardia and QT interval prolongation following AChEIs use. 9 -11 For memantine, its association with bradycardia among a few other cardiovascular adverse drug reactions was also reported. 12 Recently, 2 large studies have investigated the incidence of these cardiovascular events but yielded conflicting results on which antidementia agent or drug class is associated with a higher risk of these events. 13,14 To our knowledge, no study has investigated what patient and clinical characteristics are associated with the risk of cardiovascular events among patients with AD on antidementia therapy.
To address this evidence gap, we used 2007 to 2014 Medicare claims and advanced methods to identify risk factors for cardiovascular events among Medicare patients with AD on antidementia therapy.
Methods
Data Source and Study Population
We used 2007 to 2014 claims data from a 5% random sample of Medicare beneficiaries obtained from the Centers for Medicare and Medicaid Services (CMS). Figure 1 represents the selection of the study sample. First, we identified patients who were newly diagnosed with AD between January 1, 2007, and December 31, 2013 (n = 173 917). We used the CMS Chronic Condition Data Warehouse (CCW) definition of AD, 15 which traces back to the first month of Medicare enrollment for each patient since 1999 and indicates the earliest AD diagnosis date. This variable was developed by the CMS based on valid disease classification and procedure codes from Medicare claims 15 and has been used extensively in literature. 14,16 -28 Previous studies demonstrate a 95% specificity using Medicare claims and a 79% sensitivity among continuous enrollees in Medicare fee-or-service using this definition. 29,30 Then, we selected those who filled at least 1 prescription for an antidementia drug (donepezil, rivastigmine, galantamine, or memantine) after the AD diagnosis (n = 73 642). Index date was defined as the day of the first prescription filled for an antidementia medication. We excluded patients with a history of bradycardia, syncope, QT prolongation, ventricular tachycardia, atrioventricular block, and acute myocardial infarction during a 1-year washout period before the index date (n = 17 350) because these conditions are our primary outcomes and we want to ensure that observed outcome events were not a recurrence of previous events. To ensure we have complete claims information for all study participants, we further excluded those with partial Stand-Alone Prescription Drug Plan or Medicare Advantage Prescription Drug coverage during the 12 months before and after the index date (n = 25 859). Our final sample included 30 433 patients, who were followed from index date until the first of the following events: first cardiovascular outcome event, medication discontinuation, death, or December 31, 2014. Discontinuation was defined as having a 60-day gap without antidementia medication. This study was deemed exempt by the institutional review board at the University of Pittsburgh.

Flowchart of sample selection. Using 5% random sample of Medicare part D beneficiaries, we selected patients newly diagnosed with Alzheimer disease between 2007 and 2013 who filled at least 1 prescription for an antidementia medication after diagnosis. After excluding those with a history of bradycardia, syncope, QT prolongation, ventricular tachycardia, atrioventricular or acute myocardial infarction, and those had no continuous enrollment in Stand-Alone Prescription Drug plans, the final sample included 30 433 beneficiaries.
Outcomes
The primary outcome was the incidence of any of the following 6 cardiovascular events that have been documented to be associated with antidementia therapy: bradycardia (International Classification of Diseases-9 [ICD-9] = 427.89), QT prolongation (ICD-9 = 426.82), atrioventricular block (ICD-9 = 426.0), syncope (ICD-9 = 780.2), ventricular tachycardia (ICD-9 = 427.1), and acute myocardial infarction (ICD-9 = 410). 5 -12 Secondary outcomes included the incidence of 3 specific cardiovascular events: bradycardia, acute myocardial infarction, and syncope.
Covariates
To take advantage of the rich patient information in Medicare claims data, we extracted a large number of covariates, including patient demographics, chronic health conditions, ICD-9 diagnosis codes for medical claims in the year before index date and during follow-up, and therapeutic classes of all medications used both in the year before index date and during the follow-up period. The total number of covariates included in analyses was 10 381.
Patient demographics included race (non-Hispanic white as reference group, black, Hispanic, Asian/Pacific Islander, Native, and Other), sex (female as reference group), and age. Histories of 24 chronic disease conditions were included using definitions of the CMS CCW following the same approach in which AD was definied. 15
We extracted all pharmacy and medical (provider) claims for each patient in 2 time periods: in the year before index date and during follow-up (between index date and loss to follow-up). We created indicator variables for the first 4 digits of ICD-9 diagnosis codes. This process yielded 4818 indicator variables for unique first 4 digits of ICD-9 diagnosis codes in the year before index date and 4774 during follow-up. Following a similar approach but using pharmacy claims, we created indicator variables for therapeutic classes of medications used in the year before index date (n = 373) and in the year after index date (n = 384). We aggregated drugs into therapeutic classes using the uniform system classification. 31 Diagnosis codes were aggregated into groups using the first 4 digits and drugs into therapeutic classes because this allowed us to reduce the number of dimensions considerably, while maintaining enough granularity. 32 Finally, we created an indicator variable representing whether the antidementia treatment initiated on index date was AChEIs (as opposed to memantine) to specify antidementia drug class.
Statistical Analyses
We compared baseline patient characteristics between patients experiencing at least 1 cardiovascular event and those who did not. We used 2-sample Student t tests for continuous variables and χ2 tests for categorical variables.
Figure 2 shows the process of the selection of risk factors. First, we screened the 10 381 candidate variables one by one and excluded those with little variation. For continuous variables, we examined the distribution of each variable and excluded those with a coefficient of variance (ratio of sample variance and the sample mean) less than 0.1. For each of the categorical variables, we checked the proportion for each category and excluded those with a maximum proportion in a single category larger than 99%. 16 With the variables remained after screening, we ranked their importance in terms of predicting the occurrence of any cardiovascular event and kept those in the top 5% for further analysis. The importance of a variable was determined by the P value from either of the following tests: a simple logistic regression for a continuous variable or an individual χ2 test for a categorical variable. Finally, we built a stepwise logistic regression with those variables stayed after screening and ranking, given the response being any cardiovascular event. The cutoff probability to enter and to remove was set to 0.05 and 0.01 to further curtail the list of potential variables. Our final list of risk factors was determined based on the variables selected by the stepwise regression.
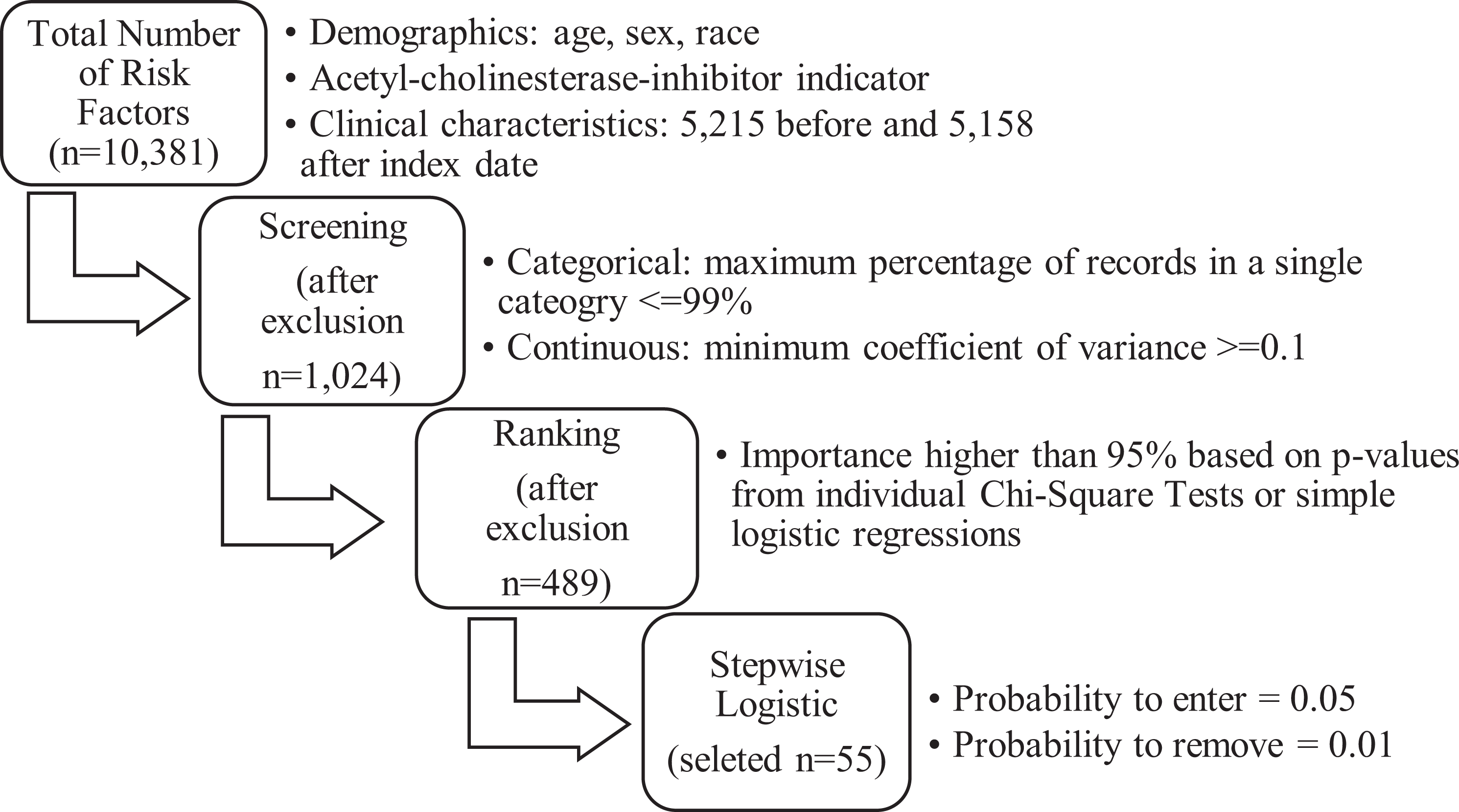
Model building process of feature selection and stepwise logistic regression for primary analysis. The number in each box indicates the number of covariates remained after each step with selection criteria listed as bullet points for the step, for the primary outcome of any cardiovascular event.
We evaluated model performance by comparing predicted values from the stepwise logistic regression with observed outcomes. Analyses for secondary outcomes were conducted following the same methodology. All analyses were performed using IBM SPSS Modeler version 18.1 (IBM Corp, Armonk, New York) and SAS version 9.4 (SAS Institute Inc, Cary, North Carolina).
Results
Patient Characteristics
The mean follow-up time for beneficiaries included in the final sample was 2.6 years (standard deviation [SD]: 2.16). On average, patients initiated antidementia treatment 106.1 days (SD: 249.5) after the first diagnosis of AD. The first prescription filled following diagnosis was an acetylcholinesterase inhibitor for 22 800 (74.9%) beneficiaries and memantine for 7633 (25.1%) beneficiaries.
Table 1 compares baseline characteristics measured on index date between patients who experienced any cardiovascular event and those who did not. There were no significant differences in age across 2 groups. Patients who experienced at least 1 cardiovascular event were more likely to be male, black, have atrial fibrillation, chronic kidney disease, congestive heart failure, and ischemic heart disease, among other chronic conditions.
Baseline Patient Characteristics by Outcome Group.

Abbreviations: CCW, Chronic Conditions Data Warehouse; CMS, Centers for Medicare and Medicaid Services; ICD-9, International Classification of Diseases-9; SD, standard deviation.
a Variables for cardiovascular events were defined using the ICD-9 codes listed in the outcomes section.
b All CCW priority chronic conditions were defined using the CMS Chronic Condition Data Warehouse definitions of these conditions, which track the first diagnosis back to January 1999. 15
Incidence of Cardiovascular Events
Among the 30 433 study participants, 7651 (25.1%) experienced at least 1 cardiovascular event. Syncope was the event with the highest incidence (20.7%), followed by bradycardia (14.5%), acute myocardial infarction (6.4%), ventricular tachycardia (1.6%), and atrioventricular block (1.2%). The incidence rate for QT prolongation (0.3%) was the lowest among all 6 cardiovascular events.
Model Performance
After screening, 1024 of the 10 381 covariates were selected for further ranking. The total number of covariates included in the development of stepwise logistic regression was 489. The final logistic model identified 55 statistically significant covariates associated with the primary outcome of any cardiovascular event. Model performance indicates an area under the curve (AUC) of 67.4% and an accuracy of 74.0% (Supplemental Table 1).
The ranking procedure for analyses of secondary outcomes selected 372 covariates for the outcome of bradycardia, 230 for acute myocardial infarction, and 413 for syncope. Stepwise logistic regressions further identified 39 statistically significant factors for the outcome of bradycardia, 24 for myocardial infarction, and 46 for syncope. General performance was similar across all 3 models with an average AUC of 67.5%, ranging from 66.4% for bradycardia to 68.5% for acute myocardial infarction. Model accuracy was 86.7% for bradycardia, 92.0% for acute myocardial infarction, and 83.7% for syncope.
Risk Factors for Outcomes of Any Cardiovascular Event
Main factors associated with higher risk of any cardiovascular event included a history of atrial fibrillation (odds ratio [OR]: 1.16; 95% confidence interval [CI]: 1.08-1.25), chronic kidney disease (OR: 1.19; 95% CI: 1.12-1.26), depression (OR: 1.13; 95% CI: 1.07-1.19), ischemic heart disease (OR: 1.26; 95% CI: 1.18-1.34), and alteration of consciousness (OR: 1.25; 95% CI: 1.14-1.36) before index date. After the index date, prescription of β-blockers (OR: 1.19; 95% CI: 1.13-1.27), diagnoses of specified cardiac dysrhythmias (OR: 1.45; 95% CI: 1.25-1.67), dizziness and giddiness (OR: 1.29; 95% CI: 1.17-1.42), and unspecified injury of head, face, and neck (OR: 1.19; 95% CI: 1.09-1.30) were also associated with higher risk of any cardiovascular event (Figure 3).

Odds ratios of risk factors for the outcomes of any cardiovascular event. Odds ratios of risk factors with P values < .0001 from the stepwise logistic regression for the primary analysis.
Conversely, history of diagnosed hypertension was associated with lower risk of any cardiovascular event (OR: 0.83; 95% CI: 0.78-0.87). Benzodiazepines (OR: 0.60; 95% CI: 0.54-0.66), ophthalmic anti-infect broad/med spectrum (OR: 0.83; 95% CI: 0.76-0.90), varicella vaccine (OR: 0.67; 95% CI: 0.55-0.82), aminopenicillins (OR: 0.83; 95% CI: 0.76-0.90), cephalosporins (OR: 0.81; 95% CI: 0.75-0.86), and noninjectable morphine and opium (OR: 0.40; 95% CI: 0.35-0.46) prescribed after the antidementia therapy were also associated with lower risk of the outcomes of any cardiovascular event.
Risk Factors for Bradycardia, Acute Myocardial Infarction, and Syncope
Analyses for secondary outcomes consistently identified 6 factors associated with increased risk of bradycardia, syncope, and acute myocardial infarction (Table 2). Specifically, a history of chronic kidney disease was associated with an 11% increased risk of syncope (P = .0071), 14% of bradycardia (P = .0021), and 28% of acute myocardial infarction (P < .0001). Similarly, a history of ischemic heart disease was associated with a 20% increased risk of syncope (P < .0001), 21% for bradycardia (P < .0001), and 84% for acute myocardial infarction (P < .0001). However, cephalosporins, benzodiazepines, and noninjectable morphine and opium prescribed after the initiation of antidementia treatment were all associated with lower risk of 3 secondary outcomes. Among those medications, noninjectable morphine and opium was associated with the lowest risk of all 3 outcomes, with a 41% lower risk of myocardial infarction (P = .0001), 60% for bradycardia (P < .0001), and 63% for syncope (P < .0001).
Odds Ratio Effects of Risk Factors Selected by All 4 Stepwise Logistic Regressions.a

Abbreviation: ICD, International Classification of Diseases.
a The table shows the odds ratio for the association between covariates and outcomes for the covariates that remained in the logistic regression models built for the primary outcome and for the 3 secondary outcomes. Stepwise procedure was used to select predictors, using a P value for entry of .05 and a P value for removal of .01. The table also lists the total number of covariates that were included in the development of each logistic regression model and the number that were selected by the stepwise procedure.
Discussion
In this study, we leveraged the richness of information in Medicare claims data to explore what patient characteristics are associated with the risk of experienced cardiovascular events in patients with AD on antidementia medications while controlling for antidementia drug classes. Through factor screening, ranking, and stepwise logistic regressions, we successfully identified 55 factors associated with the risk of any cardiovascular event among more than 10 000 covariates. This method achieved a 74% accuracy in predicting the incidence of any cardiovascular event. We found that patients with existing cardiovascular diseases and patients on drugs with pronounced cardiovascular effects like β-blockers were at a higher risk of adverse cardiovascular events.
Although previous studies compared the incidence of cardiovascular events across antidementia medications, none of them sought to investigate what characteristics place patients at a higher risk of cardiovascular events while controlling for medication classes. 13,14 The identification of those characteristics in this study helps orientate clinicians to discriminate patients with AD at high risk of suffering cardiovascular events while on antidementia therapy.
Specifically, our study suggests that clinicians should use discretion in the prescribing of antidementia treatment to patients with a history of ischemic heart disease, arrhythmias, depression, alteration of consciousness, or dizziness and giddiness. Clinicians should also be cautious about treating patients with AD already on antidementia medications with β-blockers as our results show that the concomitant use of β-blockers was associated with a 19% increased risk of cardiovascular events (P < .0001). This association is mostly driven by the increased risk of bradycardia since β-blocker use was not associated with increased risk of other secondary outcomes (Supplemental Table 2). This finding is not surprising, as bradycardia was one of the most commonly documented cardiovascular events in our study and is a shared cardiovascular effect of AChEIs and β-blockers. Some degree of bradycardia is inherent to β-blocker therapy, and so monitoring of heart rate is routinely performed after initiating β-blocker treatment. This may increase the likelihood that bradycardia is documented in these patients. In addition, diagnoses of arrhythmias (P < .0001), dizziness (P < .0001), and unspecified injury of head, face, and neck (P < .0001) were associated with an increased risk of cardiovascular events. We hypothesize that these diagnoses are related to the causes and consequences of syncope, the most common cardiovascular event in our study population.
Conversely, patients with a history of hypertension were 18% less likely to experience any cardiovascular event (P < .0001) when treated with antidementia medications, which may be explained by the lower risk of syncope in hypertensive patients. Alternatively, having a formal diagnosis of hypertension could represent high quality care and/or greater engagement with the health-care system. Medications that depress the activity of the central nervous system such as benzodiazepines (P < .0001) and morphine (P < .0001) were associated with a lower risk of cardiovascular events. However, codeine and hydrocodone products were not associated with either the composite primary outcome or the secondary outcomes of bradycardia or acute myocardial infarction. These groups of medications have the same mechanism of action without robust off-site effects, which suggests that the relationship between morphine products and the risk of cardiovascular events may not be causal. Additionally, the lower risk of cardiovascular events associated with the use of injectable anesthetics (P = .0097), cephalosporin (P < .0001), and aminopenicillin antibiotics (P < .0001) and morphine products (P < .0001), all of which are commonly used peri- and postoperatively, could be explained by selection bias since healthier patients who have lower risk of cardiovascular events are more likely to undergo elective surgery than high-risk frail patients. Similarly, we observed that most of the factors associated with cardiovascular risk collected during follow-up time were protective. This could also be a product of bias since patients who interact more with the health-care system may be more likely to have diagnoses recorded and have better cardiovascular outcomes.
Our study has several other limitations. First, as other studies using claims data, we did not have access to detailed clinical information, patient behavioral outcomes or laboratory tests and thus could not evaluate their potential effects on study outcomes. For that reason, it was unclear whether bradycardia episodes were symptomatic. Second, in our analyses, we grouped ICD-9 diagnosis codes using their first 4 digits and drugs into therapeutic classes, which reduced the granularity of our covariates. However, the application of this dimensionality reduction method by aggregation of data was important to increase the prevalence of individual covariates. 17 Third, our analysis only included cardiovascular outcomes and did not explore time mortality or hospitalization outcomes, which could also be impacted by antidementia therapy. Fourth, while we conducted a sophisticated set of analyses to identify covariates associated with the outcome, we conducted logistic regression models in the final step due to the easier interpretability of the results. Nevertheless, our estimates from the final models could have been affected by multicollinearity and overfitting. It is also possible that some of the associations we observed were a product of spurious correlation since the type I error rate increases with the number of covariates being tested. Finally, due to the observational nature of our study, we cannot establish causal relationships between discovered factors and the development of cardiovascular events.
Conclusions
We leveraged the richness of information in Medicare claims data and identified 55 factors associated with the risk of cardiovascular events in patients with AD on antidementia therapy. In particular, a history of heart rhythm disorders and use of β-blockers were strongly associated with higher risk of cardiovascular events among those patients. Our findings provide insights on identifying patients with AD at high risk of having cardiovascular events while on antidementia therapy and help clinicians make better decisions to treat these patients.
Supplemental Material
Supplemental_Materials - Risk Factors for Cardiovascular Events in Patients on Antidementia Medications
Supplemental_Materials for Risk Factors for Cardiovascular Events in Patients on Antidementia Medications by Meiqi He, James M. Stevenson, Yuting Zhang and Inmaculada Hernandez in American Journal of Alzheimer's Disease & Other Dementias
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Hernandez reports scientific advisory board fees from Pfizer outside of the submitted work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Alzheimer’s Association (Grant Number AARGD-17-500234). Dr Hernandez is funded by the National Heart, Lung and Blood Institute (Grant Number K01HL142847). Dr Stevenson is funded by the American Heart Association (Grant Number 17MCPRP33400176).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.