
Abstract
Objective
High monocyte to high-density lipoprotein cholesterol ratio (MHR) is known to be a risk factor for cardiovascular (CV) complications. We aimed to evaluate the relationship between MHR and CV outcomes in patients commencing dialysis.
Methods
The medical records of patients who started maintenance dialysis between January 2006 and July 2017 were reviewed. The primary outcomes were all-cause mortality and overall CV mortality and the secondary outcomes were CV event-free survival and the incidence of CV complications.
Results
Five hundred ninety-seven patients were enrolled and allocated to low- or high-MHR groups. All-cause mortality did not differ between the groups during a mean follow-up period of 3.9 years. In addition, overall CV mortality did not differ between the groups. However, CV event-free survival was significantly lower in the high-MHR group than in the low-MHR group (47.5% vs. 59.0%). Multivariate Cox regression analysis showed that high MHR was an independent predictor of CV events (HR 1.886, 95% CI 1.015–3.505).
Conclusion
High MHR at the time of initiation of dialysis may represent a useful predictor of CV complications.
Keywords
Introduction
Cardiovascular (CV) disease is a leading cause of mortality in patients with end-stage kidney disease (ESKD), accounting for nearly 40% of deaths. 1 Therefore, a great deal of research effort is focused on the identification of simple and accurate means of predicting CV complications. Monocytes are an essential component of the immune system, have a specific role in the inflammatory response, and are a key component of the inflammatory process that develops as part of the pathogenesis of atherosclerosis. 2 In contrast, high-density lipoprotein (HDL) cholesterol protects endothelial cells by antagonising the pro-inflammatory and pro‐oxidant effects of monocytes. 3 Therefore, a combination of the monocyte count and the serum HDL-cholesterol concentration, the monocyte to HDL-cholesterol ratio (MHR), is a marker of inflammation and atherosclerosis, and represents a risk factor for CV complications. Therefore, MHR may represent an independent predictor of severe coronary artery disease and future CV events in patients, in the presence or absence of acute coronary syndrome.4–7 Furthermore, MHR is associated with resistant hypertension in patients with chronic kidney disease (CKD). 8 Real-world studies have previously shown associations between mortality, CV outcomes, and MHR in patients with ischemic heart disease, diabetes, and/or CKD.9–12 However, the links between MHR and CV outcomes in patients undergoing dialysis have not been fully investigated. Therefore, in the present study, we evaluated the relationships between the MHR and CV outcomes in patients commencing dialysis.
Materials and Methods
Study population and protocol
Clinical data were collected retrospectively for patients >18 years old who started maintenance haemodialysis (HD) or peritoneal dialysis (PD) between January 2006 and July 2017 at Incheon St. Mary’s Hospital. The participants were followed until they died, underwent kidney transplantation or until 28 February 2019. The study was approved by the Institutional Review Board of the Catholic University of Korea (OC19ISOISI0172). Because this was a retrospective study that used medical records alone, the requirement for informed consent was waived. The reporting of this study conforms to the STROBE statement. 13
A patient with incident ESKD was defined as one that required the initiation of maintenance HD or PD and continued this dialysis for >3 months. The information that was extracted from medical records included the baseline clinical and demographic data (age; sex; body mass index (BMI); presence of diabetes; cause of ESKD; previous CV disease; smoking status; dialysis modality; use of an erythrocyte-stimulating agent; and details of any prescribed medications, including statins, angiotensin II receptor blockers, angiotensin-converting enzyme inhibitors, beta-blockers, calcium channel blockers, calcium-based phosphate-binders, non-calcium-based phosphate-binders, and vitamin D analogues), the total and differential leukocyte count (performed using XN-9000 and XE-9000 analysers; Sysmex Co., Ltd., Kobe, Japan), circulating biochemical parameters (transferrin saturation, ferritin, calcium, phosphorus; Ca × P product, intact parathyroid hormone [iPTH], albumin, high-sensitivity C-reactive protein [hs-CRP], total cholesterol, triglyceride, low-density lipoprotein [LDL] cholesterol and HDL-cholesterol) (measured using a Beckman Coulter analyser; Brea, CA, USA), and echocardiographic parameters determined within 3 months of starting dialysis. Cardiac morphology and function were evaluated using two-dimensional echocardiography (Acuson SC2000; Siemens, Malvern, PA, USA) on a non-dialysis day within 1 month of the initiation of dialysis. The echocardiographic parameters were measured according to the recommendations of the American Society of Echocardiography. The MHR was calculated by dividing the absolute circulating monocyte count by the serum HDL-cholesterol concentration. 14
We included patients who commenced maintenance dialysis during the study period but excluded those (1) for whom an MHR was not available within 3 months of the start of dialysis, (2) who had an acute infection at the time of the MHR measurements, (3) who had hematologic disease or (4) who were followed for <3 months (Figure 1). We allocated the patients to a low-MHR group or a high-MHR group, according to whether their MHR values were lower or higher than the median value of 12.3.

Flow chart describing the study. Five hundred and seventy-seven patients with end-stage kidney disease (ESKD) who were commencing maintenance dialysis were initially enrolled. The patients were allocated to Low-MHR and High-MHR groups, depending on whether their MHR was below or above the median value, respectively.
The primary outcomes were the all-cause mortality and overall CV mortality of the two groups. The secondary outcomes were the CV event-free survival and the development of any CV complication. A “CV event” was defined as coronary heart disease (unstable angina, myocardial infarction or sudden cardiac death), cerebrovascular disease (transient ischemic attack, cerebral infarction or cerebral haemorrhage) and peripheral or pulmonary vascular disease. Figure 1 consists of a flow chart that summarises patient enrolment and the number of CV events that occurred in each of the groups.
To identify independent risk factors for CV events, parameters that demonstrated statistically significant differences between the groups and were known to affect the risk of CV complications developing (MHR, age, presence of diabetes, previous CV disease, smoking status, BMI, hs-CRP, left ventricular [LV] ejection fraction, the ratio of the amplitudes of the E wave [peak early diastolic flow velocity] to the A wave [peak late diastolic flow velocity] [E/A ratio], and the ratio of the peak early transmitral flow velocity [E] to peak early diastolic mitral annular velocity [E′] [E/E′ ratio]) were further evaluated using multivariate Cox regression analysis.
Statistical analysis
Continuous data are expressed as mean ± standard deviation (SD) and categorical data are expressed as number (%). Differences between the two groups were identified using Student’s t-test. Categorical datasets were compared using the chi-square test. Kaplan–Meier curves and log-rank tests were used to compare the survival of participants in each group with respect to all-cause mortality, overall CV mortality and CV event-free survival. Independent risk factors for CV events were identified using multivariate Cox regression analysis, which was performed using variables that showed statistically significant differences between the groups in univariate analysis as covariates. All descriptive and multivariate analyses were conducted using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). The estimated standard error of the coefficient was used to calculate the confidence interval (CI) of the hazard ratio (HR) for each potential risk factor. Statistical significance was accepted when P < 0.05.
Results
Characteristics of the participants
Five hundred ninety-seven patients were recruited, of whom 299 were in the Low-MHR group and 298 were in the High-MHR group. The recruited patients were followed for a mean 3.9 years. The mean age of the participants was 58.6 years (range, 21 to 91 years) and the mean duration of follow up was 3.9 years (range, 0.3 to 12.3 years). Three hundred thirty-five patients were male (56.1%), 347 had diabetes (58.1%) and 129 had a history of CV disease (21.6%). The median MHR was 12.3 (interquartile range, 8.1 to 19.7).
The High-MHR group contained more men, smokers and more participants with diabetes, and the mean BMI of this group was higher than that of the Low-MHR group (Table 1). The haemoglobin concentration, leukocyte count, monocyte count, platelet count, serum hs-CRP and serum triglyceride concentration were significantly higher in the High-MHR group than in the Low-MHR group. In contrast, the intact parathyroid hormone (iPTH), total cholesterol, LDL-cholesterol and HDL-cholesterol concentrations were significantly lower in the High-MHR group than in the Low-MHR group. However, none of the echocardiographic parameters significantly differed between the two groups (Table 2).
Baseline characteristics and laboratory parameters of the participants.

Continuous data are expressed as mean ± standard deviation (SD) and categorical data are expressed as number (%).
Differences between the two groups were identified using Student’s t-test or the chi-square test, as appropriate.
MHR, monocyte count to serum high-density lipoprotein cholesterol concentration ratio; BMI, body mass index; ESKD, end-stage kidney disease; CGN, chronic glomerular nephritis; CV, cardiovascular; HD, haemodialysis; iPTH, intact parathyroid hormone; hs-CRP, high-sensitivity C-reactive protein; LDL, low-density lipoprotein; HDL, high-density lipoprotein; ESA, erythropoiesis-stimulating agent; ARB, angiotensin receptor blocker; ACEi, angiotensin-converting enzyme inhibitor.
Echocardiographic parameters for the study population.
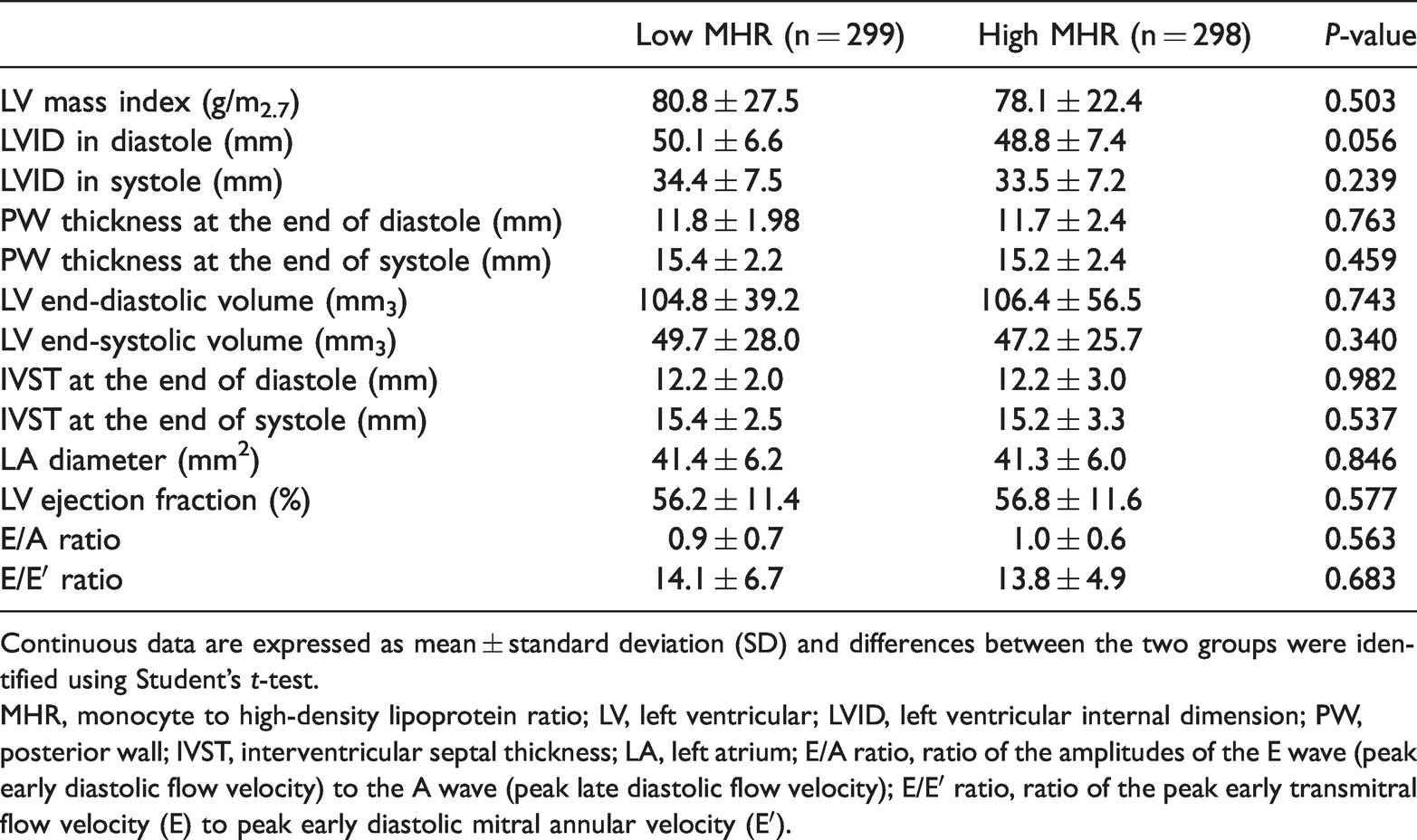
Continuous data are expressed as mean ± standard deviation (SD) and differences between the two groups were identified using Student’s t-test.
MHR, monocyte to high-density lipoprotein ratio; LV, left ventricular; LVID, left ventricular internal dimension; PW, posterior wall; IVST, interventricular septal thickness; LA, left atrium; E/A ratio, ratio of the amplitudes of the E wave (peak early diastolic flow velocity) to the A wave (peak late diastolic flow velocity); E/E′ ratio, ratio of the peak early transmitral flow velocity (E) to peak early diastolic mitral annular velocity (E′).
All-cause mortality and overall CV mortality
One hundred thirty-three participants died during the study. Thirty-three participants died as a result of CV complications (24.8%), of which 15 were in the Low-MHR group (45.5%) and 18 were in the High-MHR group (54.5%). Of these deaths, 14 occurred because of myocardial infarction, two were sudden cardiac deaths, 11 occurred because of cerebral haemorrhage, and six occurred because of cerebral infarction. The remaining 100 deaths were not CV-related (75.2%); 48 of these participants were in the Low-MHR group (48.0%) and 52 were in the High-MHR group (52.0%). The principal causes of non-CV death were infection (n = 52, 52.0%), malignancy (n = 6, 6%) and gastrointestinal bleeding (n = 8, 8%). Neither all-cause mortality nor overall CV mortality differed between the two groups during the study period (Figure 2).

Comparison of all-cause mortality and overall cardiovascular mortality in the Low-MHR and High-MHR groups. (A) All-cause mortality (P = 0.371) and (B) overall cardiovascular mortality (P = 0.615) did not significantly differ between the two groups.
Overall CV event-free survival rate
During the follow-up period, 131 participants experienced a CV event, of whom 54 (41.2%) were in the low-MHR group and 77 (58.8%) were in the high-MHR group. The CV events that occurred were the development of ischemic heart disease (n = 76, 58.0%), sudden cardiac death (n = 3, 2.3%), transient ischemic attack (n = 2, 1.5%), cerebral infarction (n = 22, 16.8%), cerebral haemorrhage (n = 21, 16.0%) and the development of peripheral or pulmonary vascular disease (n = 7, 5.3%). CV event-free survival was significantly lower in the high-MHR group than in the low-MHR group (47.5% vs. 59.0%, P = 0.006; Figure 3).

Comparison of cardiovascular event-free survival in the Low-MHR and High-MHR groups. The cardiovascular event-free survival of the High-MHR group was significantly lower than that of the Low-MHR group (P = 0.017).
Assessment of MHR as a risk factor for adverse cardiovascular outcomes
To identify independent risk factors for CV events, the parameters that showed significant differences between the groups and were thought to be likely to influence the development of CV complications were analysed using Cox regression. These were MHR, age, the presence of diabetes, previous CV disease, smoking status, BMI, hs-CRP concentration, LV ejection fraction, E/A ratio and E/E′ ratio. Univariate Cox regression analysis showed that MHR, age, the presence of diabetes, previous CV disease, hs-CRP and LV ejection fraction were associated with subsequent CV events. The multivariate analysis showed that high MHR was an independent predictor of CV events (HR 1.886, 95% CI 1.015–3.505), as was age (HR 1.031, 95% CI 1.007–1.056) and LV ejection fraction (HR 0.971 95% CI 0.948–0.995), even after adjustment for MHR, age, the presence of diabetes, previous CV disease, smoking status, BMI, hs-CRP concentration, haemoglobin concentration, total cholesterol, triglyceride, LDL-cholesterol, HDL-cholesterol, LV ejection fraction, E/A ratio and E/E′ ratio (Table 3).
Cox regression analysis of potential predictors of cardiovascular events.
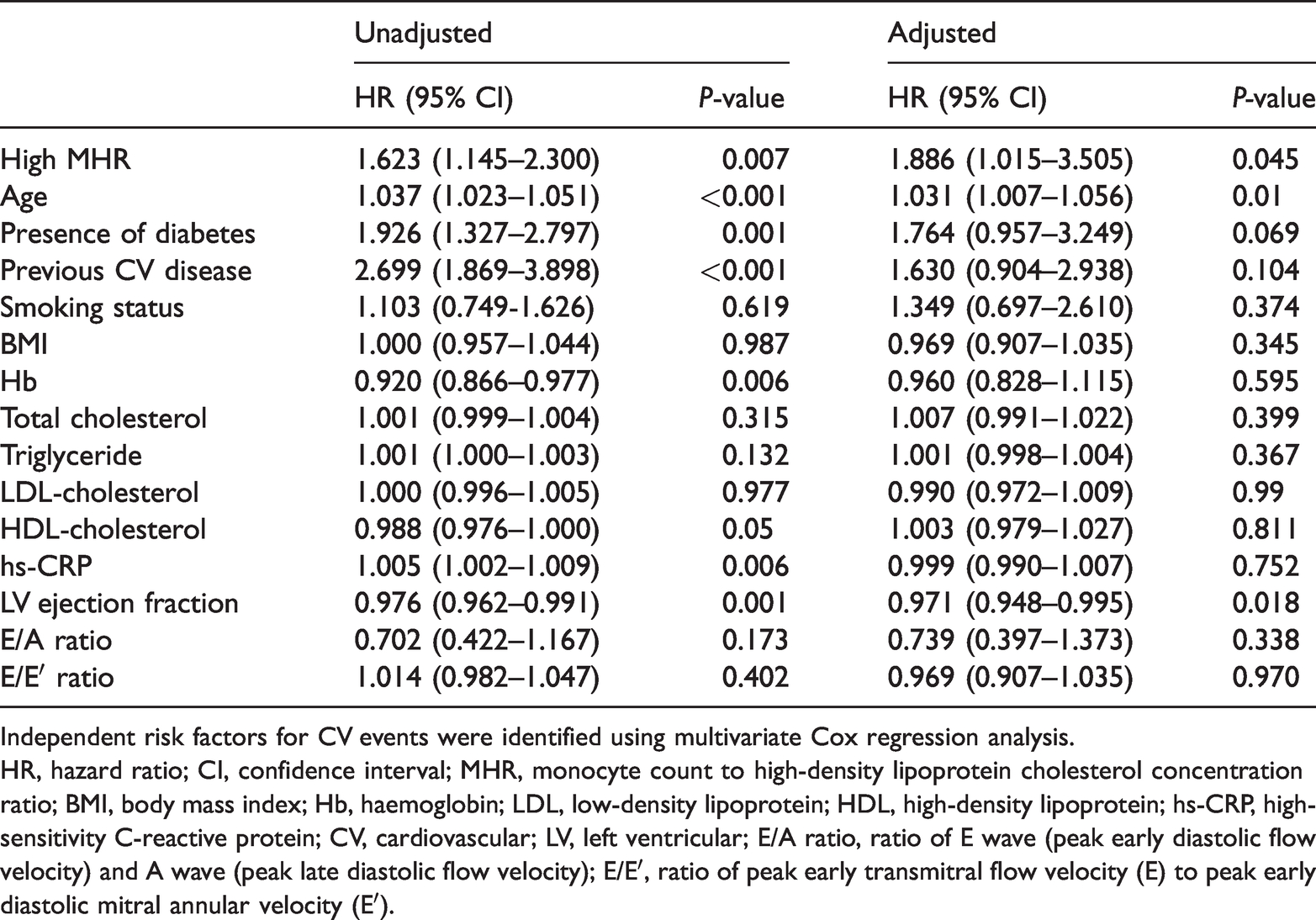
Independent risk factors for CV events were identified using multivariate Cox regression analysis.
HR, hazard ratio; CI, confidence interval; MHR, monocyte count to high-density lipoprotein cholesterol concentration ratio; BMI, body mass index; Hb, haemoglobin; LDL, low-density lipoprotein; HDL, high-density lipoprotein; hs-CRP, high-sensitivity C-reactive protein; CV, cardiovascular; LV, left ventricular; E/A ratio, ratio of E wave (peak early diastolic flow velocity) and A wave (peak late diastolic flow velocity); E/E′, ratio of peak early transmitral flow velocity (E) to peak early diastolic mitral annular velocity (E′).
Discussion
The most important finding of the present study is that MHR may be a useful predictor of CV complications in patients with incident ESKD. CV event-free survival was significantly shorter in the High-MHR group than in the Low-MHR group, and MHR was shown to be an independent predictor of CV complications in patients with ESKD in multivariate Cox regression analysis. Therefore, patients commencing dialysis who have a high MHR should undergo regular monitoring for CV events.
MHR has been shown to be associated with mortality in patients with other diseases10,15 and to be associated with CV events in retrospective studies.16,17 However, neither all-cause mortality nor overall CV mortality differed between the two groups in the present study. These unexpected results may be explained by the numerous patients who were excluded from the study. Many of the 30 patients who were transferred to other institutes within 3 months of commencing dialysis had MHR values below the median. Therefore, the patients who were lost to follow up may explain the lack of significant differences in survival outcomes. Nevertheless, the study has demonstrated the predictive value of MHR for CV complications in patients with ESKD, as shown in previous studies. 18 The present study has also shown that a high MHR is associated with high levels of inflammation-related parameters, including leukocyte count, monocyte count, and hs-CRP, relative to patients with a low MHR. Several previous studies have generated contrasting results regarding the relationship between MHR and lipid profile. A previous study by Canpolat et al. showed that HDL decreased substantially as the MHR increased, whereas the total cholesterol, LDL-cholesterol and triglyceride concentrations did not change significantly. 19 In another study, only triglyceride concentration negatively correlated with MHR. 20 In the present study, the total cholesterol, LDL-cholesterol and HDL-cholesterol concentrations were significantly lower in the High-MHR group, whereas the triglyceride concentration was higher. It may be that although statin use did not significantly differ between the two groups, statins were more likely to be used in the High-MHR group, which might have affected the lipid concentrations. In addition, because the High-MHR group had a higher prevalence of a history of prior CV disease, it is possible that the participants had improved their lifestyles.
Although we found no associations between high MHR and all-cause or CV mortality, high MHR was associated with CV complications (HR 1.886, 95% CI 1.015–3.505, P = 0.045). The present results suggest that MHR may represent a simple and useful method for the prediction of CV complications in dialysis patients. A previous study of 880 dialysis patients from China showed that MHR is an independent risk factor for CV events in patients who are undergoing PD. In this study, 15.8% of the participants experienced a CV event over a 2.2-year period and high MHR was associated with 1.97-fold higher incidence of cardiovascular complication versus participants with low MHR (HR 1.97, 95% CI 1.19–3.28, P = 0.009). 18 Another recent study conducted in China showed that high MHR is an independent risk factor for all-cause and CV mortality in patients undergoing PD, with HRs of 1.43 (95% CI 1.06–1.93, P = 0.019) and 1.54 (95% CI 1.01–2.35, P = 0.046), respectively. 21 However, these studies were conducted only in patients who were undergoing PD, whereas large numbers of patients undergo both HD and PD worldwide,22–24 and patients who were undergoing both types of dialysis were included in the present study. Another consideration is whether a 3.9-year follow-up period is sufficient to obtain significant survival data in patients undergoing dialysis. A previous study of data from the Korean Health Insurance Review and Assessment Service database regarding 30,279 patients who were undergoing dialysis recorded 11,053 (36.5%) CV events during a 1.8-year period and cumulative incidences of CV events of 21.1%, 32.3% and 40.5% over 1, 2 and 3 years, respectively. 25 The incidences of CV events identified in this study were similar to that measured in the previous Korean study. Therefore, the results of the present study imply that MHR may represent a useful means of predicting CV outcomes in patients with ESKD, whether they undergo HD or PD.
Monocytes play an essential role in chronic inflammation and CV disease. Furthermore, they differentiate into macrophages and induce inflammation as part of the progression of atherosclerosis. 2 When the vascular endothelium is injured, monocytes migrate to the subendothelium and mature into macrophages. Macrophages take up LDL-cholesterol, differentiate into foam cells, and release pro-inflammatory, pro-oxidant cytokines. In contrast, HDL-cholesterol protects endothelial cells by antagonising the pro-inflammatory and pro‐oxidant activities of monocytes. 26 Therefore, a high MHR is likely to be associated with atherosclerosis, which predisposes toward CV events. High MHR is associated with high serum hs-CRP concentration and inflammation, which plays a major role in endothelial dysfunction and atherosclerosis, including thrombotic complications.7,19,27 In addition, high MHR has previously been shown to be an independent risk factor for CV complications.5,10,12,27,28 Considering that the most common cause of mortality in patients with ESKD is CV complications, appropriate screening of high-risk groups for CV complications should be the first step in a strategy aimed at reducing patient mortality. To date, a number of potential predictors of CV events have been evaluated, but their widespread clinical use is limited by cost and time factors.29–31 However, monocyte count and HDL-cholesterol concentration are commonly included in the basic laboratory assessment of patients with ESKD, and therefore MHR can be easily calculated by clinicians, without incurring additional cost or time. In the present study, we have shown that MHR is an independent risk factor, along with hs-CRP, which predicts CV complications in patients who are commencing dialysis. Furthermore, in multivariate cox regression, high MHR was found to be more strongly associated with CV complications than hs-CRP, with a higher HR. Therefore, both may be useful predictors of CV complications. The use of such a cost-effective, time-efficient means of predicting CV outcomes may assist with the identification of patients who are at high risk of CV complications and enable regular surveillance. Thus, the results of the present study suggest that MHR is a risk factor for CV events in patients commencing dialysis.
There were some limitations to the present study. First, it was conducted retrospectively. Second, MHR was only calculated at the initiation of dialysis. Third, because an appropriate cut-off value for MHR was not determined, the median value was used. Nonetheless, a high MHR at the initiation of dialysis predicted CV outcomes in patients with ESKD over a 3.9-year period, consistent with the findings of previous studies. Prospective studies should be conducted in the future to confirm the relationships of serial MHR measurements with patient survival and CV outcomes in patients undergoing dialysis, and to calculate an appropriate MHR cut-off value for the purpose of predicting such events. In conclusion, high MHR at the time of initiation of dialysis may represent a useful predictor of CV complications, but this should be confirmed in carefully designed prospective studies.
Footnotes
Author contributions
Conceptualisation: all authors. Data curation: DK, DWK, YHL, SYP, YWS, HS, THB and SJS. Formal analysis: DK, THB, SJS, DWK, YHL, HEY, BSC and BSK; Investigation: DK, SYP, YWS, HS, THB, SJS, HEY and HSP. Methodology and project administration: THB and SJS; Supervision: THB and SJS. Validation: THB, SJS, BSC and BSK. Writing-original draft: DK. Writing-review & editing: DK, THB and SJS.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This study was supported by a grant to the Research Centre from Incheon St. Mary’s Hospital, The Catholic University of Korea.