
Abstract
Background:
The present study aimed at investigating loneliness and burden experienced by family members caring for relatives diagnosed with Alzheimer disease.
Methods:
Participants were 40 caregivers of inpatients with Alzheimer disease. Correlation and multiple regression analyses were conducted to investigate whether caregivers’ loneliness (uni- and multidimensional) and burden are associated with and predicted by (1) specific caregiver characteristics and/or (2) patients’ dementia severity and neuropsychiatric symptoms.
Results:
Loneliness was significantly correlated with caregivers’ sex, age, and living circumstances, while burden was significantly correlated with caregivers’ education solely. Regression analyses revealed that caregivers’ sex and living circumstances contributed significantly to variance explanation of loneliness (but not burden), while the additional consideration of patient variables did not improve model fit.
Conclusions:
Loneliness reported by caregivers of relatives diagnosed with dementia is significantly modulated by caregiver (but not patient) characteristics. Notably, both uni- and multidimensional loneliness scales seem to be sensitive diagnostic tools.
Introduction
Loneliness is a multidimensional phenomenon that may seriously hamper individuals’ well-being. Loneliness has been defined as an unpleasant experience that arises when an individual’s social relationships are qualitatively or quantitatively deficient over a prolonged period of time. 1 Loneliness can be differentiated into 2 primary dimensions, namely emotional and social loneliness. 2 Although the term emotional loneliness refers to the absence of others with whom the individual is emotionally attached to, the term social loneliness describes the perceived lack of an acceptable social network. Notably, chronic loneliness (defined as subjective feelings of loneliness over a period of at least 4 years) was observed to be positively correlated with physician visits and thus, to an increase in health-care costs. 3 Hence, the lack of social relationships and experiences of chronic loneliness reported by caregivers should be considered a significant public health issue.
Dementia is a clinical condition characterized by an acquired decline in mental ability that is sufficiently severe to interfere with patient’s independence. 4 The incidence of dementia significantly increases with increasing living expectations (reported incidence rates reaching 1.6% in 65-69 year-olds, 15.7% in 80-84 year-olds, and 41.1% in individuals aged >90; Alzheimer Europe 2009). Beyond exhibiting cognitive impairments, patients diagnosed with dementia frequently present behavioral symptoms such as depression, irritability, aggression, sleep disturbances, and so on. 5 According to a large longitudinal study, up to 97% of participating patients with dementia required psychiatric treatment at least once during disease progression. 6 Furthermore, behavioral symptoms associated with dementia are likely to place a heavy psychoemotional burden on caregivers and, in case of chronic strain, should be considered a health risk for caregivers. 7,8
Dementia and Loneliness
Interestingly, caregiver characteristics seem to explain a higher proportion of the variance in caregivers’ loneliness than patient characteristics. 9 In particular, poorer physical health, lower education, and lower perceived self-efficacy were found to be predictive of loneliness in caregivers of patients with Parkinson disease. Furthermore, the finding that caregivers attending caregiver support groups reported less loneliness than those not attending support groups 9 fits well with previously mentioned mediating effects of social support on loneliness. 10
Study Rationale
We sought to investigate subjective feelings of loneliness and burden in family caregivers of patients diagnosed with Alzheimer disease. Contrary to previous studies, we used both uni- and multidimensional loneliness scales. Moreover, we aimed to assess whether in our study group loneliness and burden were associated with specific caregiver (ie, age, sex, education, living circumstances) and/or patient characteristics (ie, severity of dementia and neuropsychiatric symptoms). Previous results were inconsistent so far and due to methodological differences are difficult to compare with each other directly. Finally, we examined whether specific caregiver and/or patient characteristics predict caregivers’ loneliness and burden.
Working Hypotheses
First, family caregivers of patients diagnosed with advanced dementia should report subjective feelings of loneliness and burden. Second, caregiver and patient characteristics alike might be associated with caregivers’ loneliness and burden. And third, caregiver and patient characteristics alike should be predictive of caregivers’ loneliness and burden.
Methods
Participants
Study participants were family caregivers of patients having Alzheimer disease (major neurocognitive disorder according to Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition [DSM-V] 4 ). All participants were recruited between January 2015 and April 2017 from a gerontopsychiatric inpatient ward specializing in the treatment of elderly patients having moderate to severe dementia.
Patients were required to have been diagnosed with Alzheimer disease. 4 All patients underwent clinical routine psychiatric examination and presented with significant cognitive decline that interfered with independence but was not due to delirium or other mental disorders (thus justifying the DSM-V 4 diagnosis of a major neurocognitive disorder due to Alzheimer disease). All patients were rated as having moderate or severe dementia based on the Clinical Dementia Rating 11 and presented either with affected basic activities of daily living (eg, self-care such as feeding, dressing, bathing, etc) or were already fully dependent.
Caregivers were not paid for caregiving and were included in case they (1) were related to the care recipient and (2) had been caregiving for at least 6 months (average time of direct care was 30 hours per week). Caregivers were excluded when they (1) were having a mental illness or other chronic disease rendering their caregiving role impossible, (2) had severe sensory/motor impairments hampering compliance, and (3) did not have German as their first language.
Of a total of 183 eligible patients, 143 patients (and their caregivers) had to be excluded because (1) patients were discharged before data collection could be finished (n = 98), (2) caregivers refused participation (n = 7), (3) caregivers failed to return questionnaires or to sign the written informed consent (n = 32), (4) patients did not have any relatives or close caregivers (n = 2), and (5) patients deceased during hospital stay (n = 4). Thus, the final sample consisted of 40 caregivers of inpatients diagnosed with major neurocognitive disorder due to Alzheimer disease (DSM-V 4 ; Table 1).
Caregiver and Patient Characteristics.
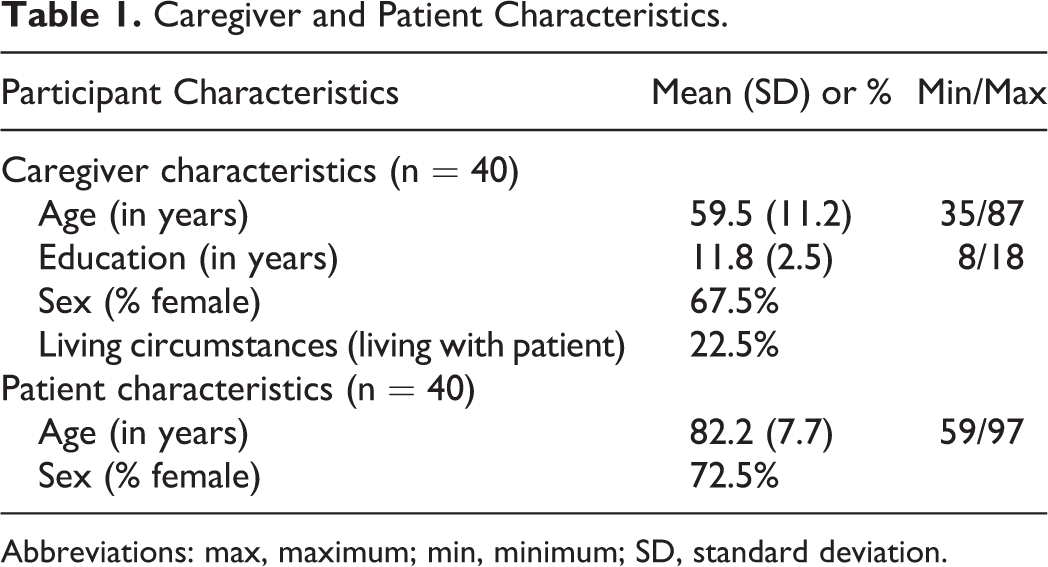
Abbreviations: max, maximum; min, minimum; SD, standard deviation.
Tests and Questionnaires Employed
Subjective feelings of loneliness were assessed with the unidimensional UCLA Loneliness Scale (revised version) 12 and the multidimensional loneliness questionnaire (MEF). 13
The adapted German version of the revised UCLA Loneliness Scale 14 is a 20-item questionnaire designed to measure loneliness unidimensionally on a 5-point Likert scale. According to the authors of the original English version of the revised UCLA Loneliness Scale, 12 the questionnaire ought to measure satisfaction or dissatisfaction (10 items each) with social relationships interpreted in terms of loneliness as an unidimensional construct. For reasons of better comparability and interpretability, we retained the 4-point Likert scale (ranging from 1 to 4) of the revised version of Russell et al. 12 Hence, the total score ranged from 20 to 80, higher scores reflecting stronger feelings of loneliness. Notably, for the UCLA Loneliness Scale, no specific cutoff scores are reported. Reliability (ie, internal consistency) of the adapted German version 14 has been reported to be satisfactory, with Cronbach α ranging from .89 to .96.
The German version of the Multidimensional Loneliness Questionnaire MEF 13 is a 37-item scale that measures loneliness on 3 subscales: social loneliness (n = 15), emotional loneliness (n = 12), and inability to stay alone (n = 10). Items are scored on a 5-point Likert scale (ranging from 1 to 5). Thus, the total score ranged from 37 to 185, with higher scores indicating stronger feelings of loneliness. Empirically validated cutoff scores are lacking for the MEF. Reliability of the MEF has been reported to be satisfactory with Cronbach α ranging from .85 to .89. 13
Caregivers’ subjective feelings of burden were assessed by utilizing the German version of the Zarit Burden Inventory (ZBI) 15 (original version: Zarit et al 16 ). The ZBI consists of 22 items related to patient’s behavioral or functional impairments and/or the care situation. Items were answered on a 5-point Likert scale (ranging from 0 to 4). Thus, the total score ranged from 0 to 88, with higher scores indicating higher feelings of burden. Cutoff scores have been suggested by Zarit and coworkers 16 (ie, scores below 20 reflect little to no burden, scores from 21 to 40 mild to moderate burden, scores from 41 to 60 moderate to severe burden, scores ≥61 severe burden). However, according to the authors, these cutoff scores should be regarded as guidelines only. Reliability of the ZBI has been reported to be satisfactory (Cronbach α .91).
Caregiver Characteristics
Caregivers were asked to report sociodemographic data such as age, sex, years of education, living circumstances (living with the patient or not), and the duration of caregiving.
Neuropsychological Patient Characteristics
Patients were asked to complete a cognitive screening test (Mini-Mental State Examination, 2nd Revision/MMSE-2) 17 that assessed orientation, attention, memory, visuoconstructional skills as well as rudimentary reading comprehension, and writing. The total score was 30 with higher scores indicating better performance (scores <27 indicating cognitive decline).
Furthermore, caregivers were asked to estimate the presence and severity of noncognitive behavioral symptoms presented by their relatives diagnosed with dementia (Neuropsychiatric Inventory/NPI). 5 The NPI assesses 12 behavioral symptoms (ie, paranoid delusions, hallucinations, agitation/aggression, dysphoria, anxiety, euphoria, apathy, disinhibition, irritability/lability, aberrant motor activity, night-time behavioral disturbances, appetite, and eating abnormalities). Caregivers had to estimate symptom frequency and subjective burden. For each symptom, scores were calculated by multiplying frequency and burden. The maximum score per symptom was 12 (ie, maximum 4 regarding frequency × maximum 3 regarding subjective burden). Thus, the total score ranged from 0 to 144, with higher scores reflecting the presence of more neuropsychiatric symptoms.
Analyses
In a first step, descriptive and exploratory statistics were conducted (eg, to test for data’s distribution characteristics). Second, correlation analyses were performed to investigate the association between caregivers’ loneliness and burden on the one side and patients’ severity of dementia and neuropsychiatric symptoms on the other side. As sex has been identified to be a modulating variable for loneliness previously, 18 we performed partial correlations using sex as a covariate. Third, regression analyses were conducted to identify caregiver and/or patient variables predicting caregivers’ loneliness and burden. In particular, we performed hierarchical regression analyses subjecting caregiver characteristics (caregivers’ age, sex, and education as well as living with or without the patient) into the model in a first block of predictors and neuropsychological patient characteristics (MMSE-2 and NPI) in a second block. Relevant predictors in each block were identified using the stepwise procedure. Missing values were infrequent and randomly distributed and thus imputed by the respective scale mean over all caregivers/patients.
In order to facilitate data interpretation (ie, considering the potential tendency to yield underpowered results due to small sample sizes), power estimates were reported whenever necessary. As we aimed at strict power testing, we adhered to Ferguson’s 19 recommendations of power estimate interpretations that are more conservative than those reported by Cohen. 20 Thus, nonsignificant results were discussed only when effect sizes indicated the recommended minimum effect size representing a “practically” relevant effect according to Ferguson 19 : effects may be considered practically relevant when Cohen d >.4 (corresponding to r and standardized b of >.2).
Ethical Approval
The present study was conducted in compliance with the Declaration of Helsinki and was approved by the local ethical committee of Innsbruck Medical University. Written informed consent has been obtained from all participants.
Results
Descriptive Analyses
Table 2 provides the descriptive statistics of caregiver’s subjective feelings of loneliness and burden (UCLA, MEF, ZBI). Although males reported higher levels of loneliness (as indexed by the UCLA and the MEF alike), females perceived higher subjective feelings of burden (as indexed by the ZBI). In further data analyses, these variables were considered to be dependent variables. Likewise, patients’ scores indexing severity of dementia (MMSE-2) and neuropsychiatric symptoms (NPI) are presented in Table 2. Because 2 dependent variables (ie, UCLA and MEF) were not normally distributed, these variables were logarithmically transformed prior to further analyses.
Descriptive Data of Dependent Variables (ie, Caregiver’s Subjective Feelings of Loneliness and Burden; Namely UCLA, MEF, and ZBI, respectively) as Well as Patient’s Test Scores Indexing Dementia Severity (MMSE-2) and Severity of Neuropsychiatric Symptoms (NPI).
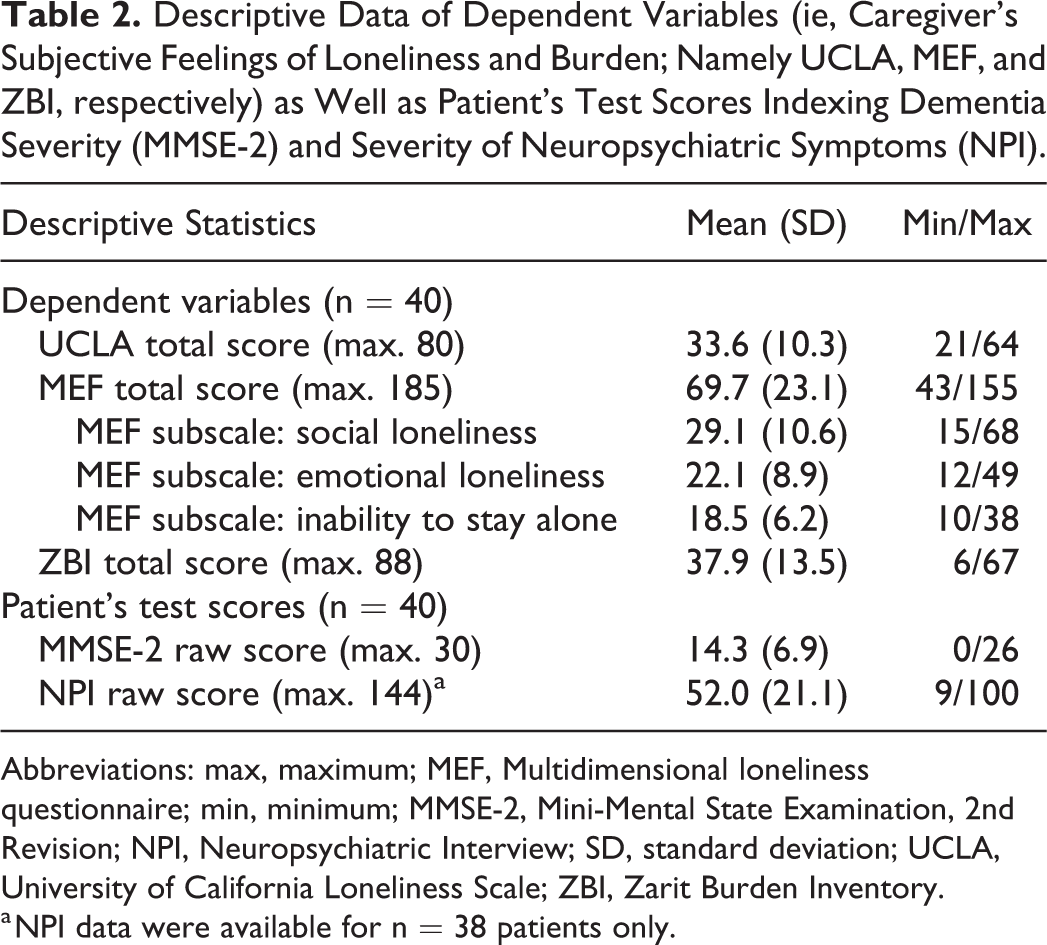
Abbreviations: max, maximum; MEF, Multidimensional loneliness questionnaire; min, minimum; MMSE-2, Mini-Mental State Examination, 2nd Revision; NPI, Neuropsychiatric Interview; SD, standard deviation; UCLA, University of California Loneliness Scale; ZBI, Zarit Burden Inventory.
a NPI data were available for n = 38 patients only.
Correlational Analyses
As depicted in Table 3, Spearman correlation analyses disclosed that loneliness was significantly correlated with caregivers’ sex (UCLA: P = .009; MEF total score: P = .001), age (UCLA: P = .040; MEF total score: P = .046), and living circumstances (living with the patient or not; UCLA: P = .025). In particular, higher levels of loneliness were reported by male caregivers and by caregivers living together with the patient diagnosed with dementia. Moreover, positive correlation coefficients regarding age indicate that relative to younger caregivers older ones reported higher levels of loneliness.
Correlations Between Caregivers’ Subjective Feelings of Loneliness and Burden on the One Side and Caregiver Characteristics on the Other Side.
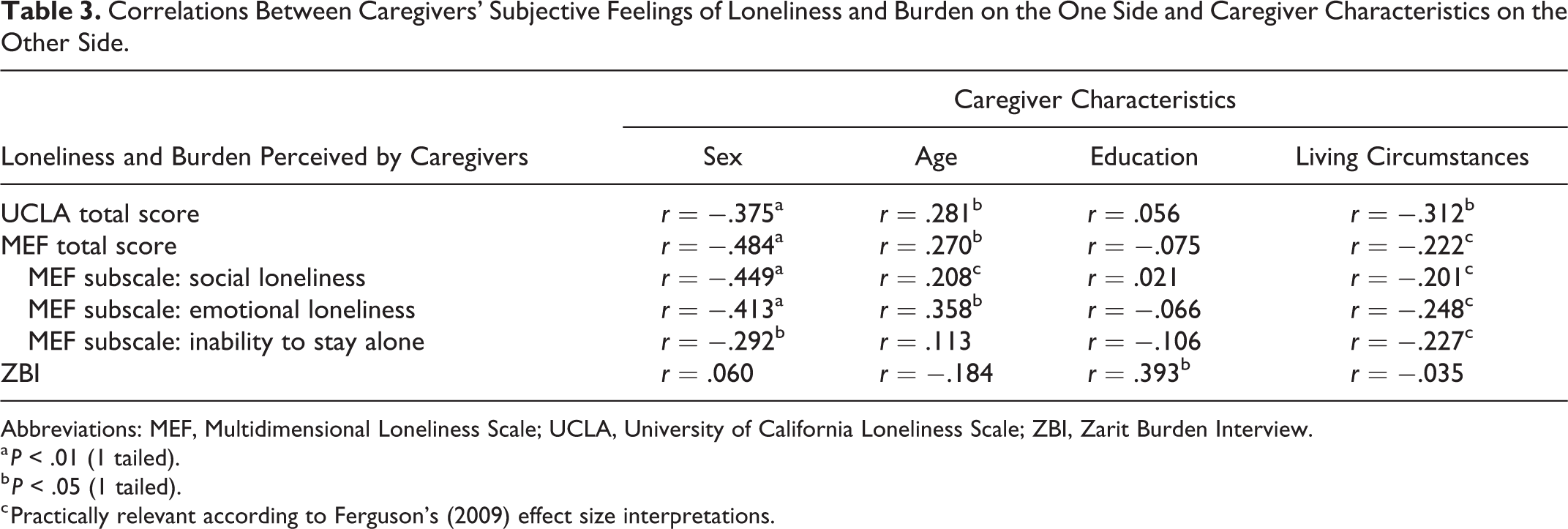
Abbreviations: MEF, Multidimensional Loneliness Scale; UCLA, University of California Loneliness Scale; ZBI, Zarit Burden Interview.
a P < .01 (1 tailed).
b P < .05 (1 tailed).
c Practically relevant according to Ferguson’s (2009) effect size interpretations.
Notably, all 3 MEF subscales were significantly correlated with caregivers’ sex (“social loneliness” P = .002; “emotional loneliness” P = .004; “inability to stay alone” P = .034), while caregivers’ age was significantly correlated with “emotional loneliness” (P = .012). Moreover, the correlation between age and “social loneliness” was practically relevant according to Ferguson 19 (Table 3). Similarly, correlations between caregivers’ living circumstances and all MEF scales were practically relevant according to Ferguson (ie, all correlation coefficients being >.2).
Finally, caregivers’ burden (indexed by the ZBI) was significantly and positively correlated with caregivers’ education solely (P = .013; higher burden being reported by caregivers with higher education).
As shown in Table 4, partial correlations (adjusting for sex) between caregivers’ loneliness and burden and patients’ test scores did not become significant. However, the correlation between dementia severity (indexed by MMSE-2) and caregivers’ loneliness (indexed by MEF total score) was practically relevant according to Ferguson 19 (P = .114; see also the correlation between MMSE-2 and MEF subscale “social loneliness”: P = .101). The latter correlations were positive thus indicating that higher MMSE-2 scores (reflecting less severe dementia) were associated with higher levels of loneliness.
Partial Correlations (Adjusting for Sex) Between Caregivers’ Subjective Feelings of Loneliness and Burden on the One Side (UCLA, MEF, ZBI) and Patients’ Test Scores Indexing Severity of Dementia (MMSE-2) and Neuropsychiatric Symptoms (NPI) on the Other Side.
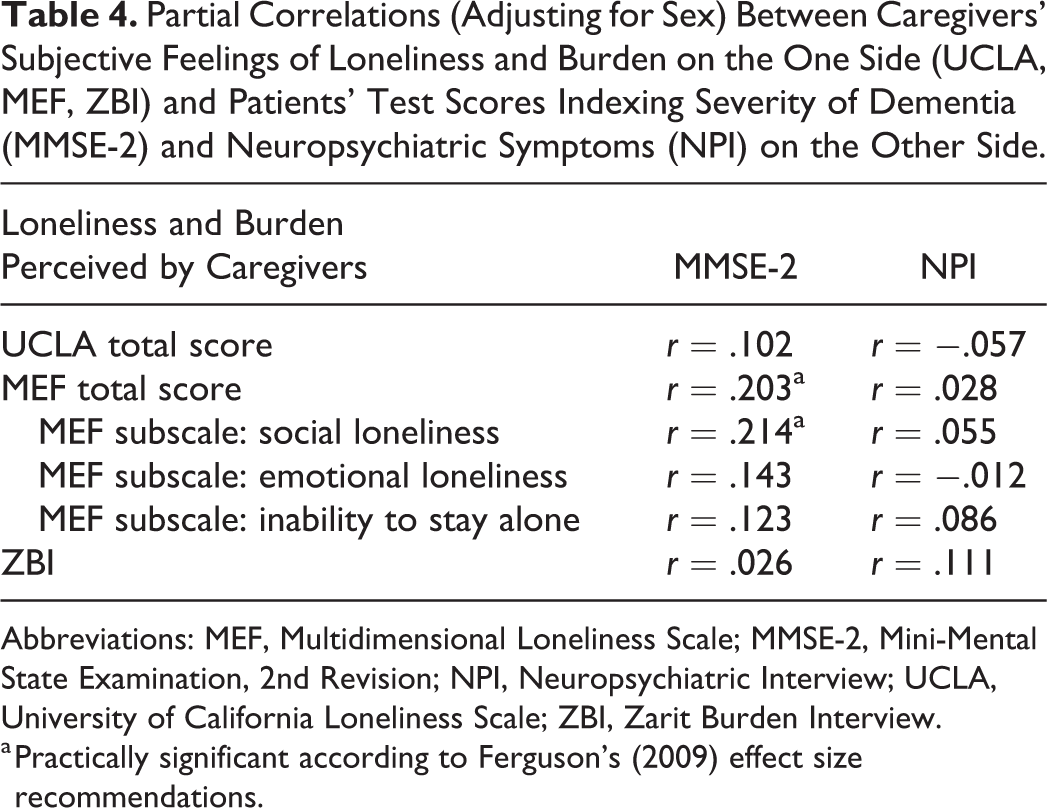
Abbreviations: MEF, Multidimensional Loneliness Scale; MMSE-2, Mini-Mental State Examination, 2nd Revision; NPI, Neuropsychiatric Interview; UCLA, University of California Loneliness Scale; ZBI, Zarit Burden Interview.
a Practically significant according to Ferguson’s (2009) effect size recommendations.
Regression Analyses
The final model of the regression analysis with caregivers’ loneliness indexed by the unidimensional UCLA Loneliness Scale revealed significant influences of caregivers’ sex and living circumstances (R = .55, adjusted R 2 = .26, F (2,37) = 7.89, P = .001, see Table 5). Inspection of β weights indicated that males reported higher loneliness as compared to females. Additionally, caregivers living with the patient reported higher loneliness. Neuropsychological patient characteristics were not observed to significantly predict caregiver loneliness as reflected by the UCLA. No other predictor was clinically relevant following the suggestions of Ferguson. 19
Regression Results.a
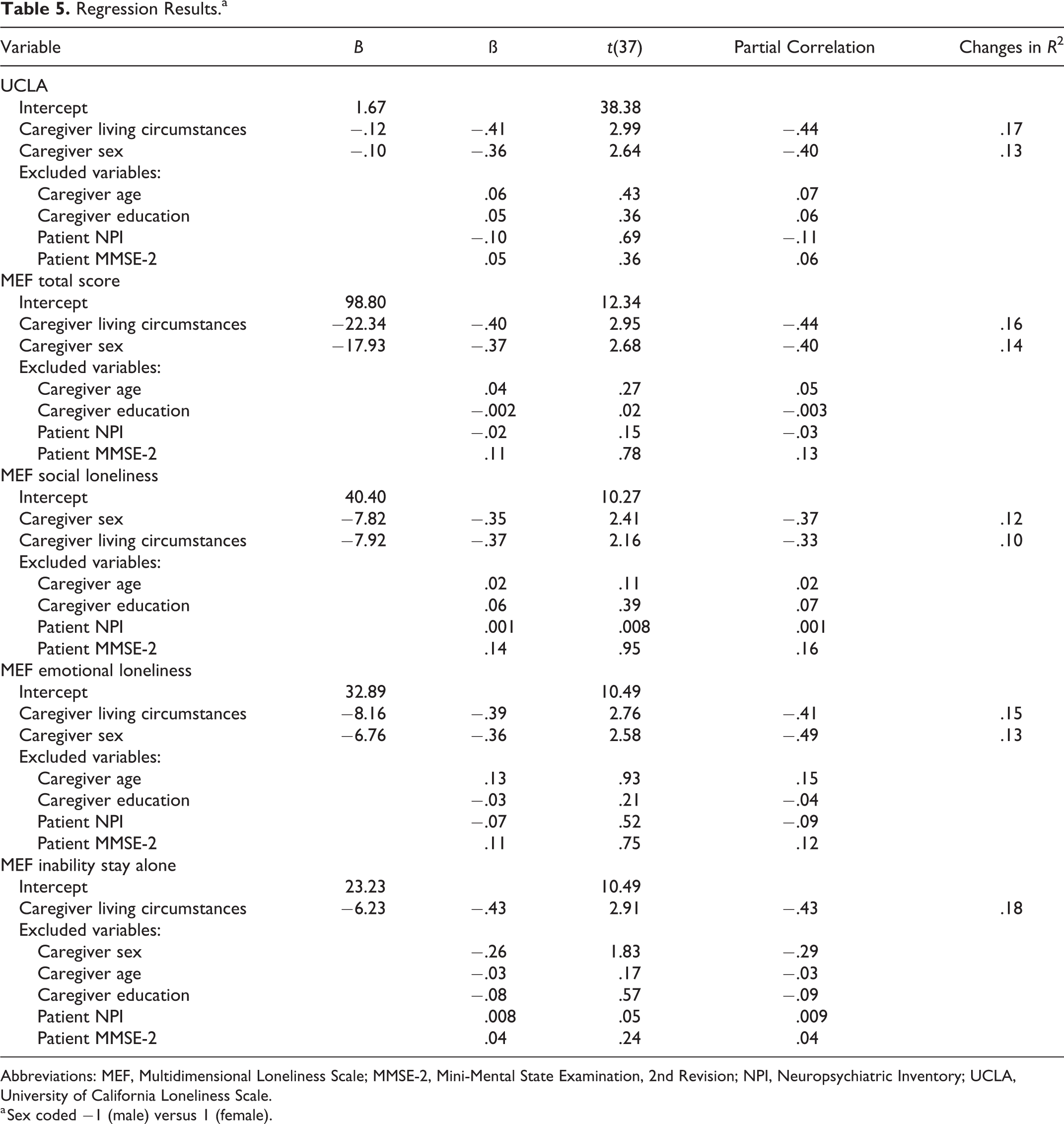
Abbreviations: MEF, Multidimensional Loneliness Scale; MMSE-2, Mini-Mental State Examination, 2nd Revision; NPI, Neuropsychiatric Inventory; UCLA, University of California Loneliness Scale.
a Sex coded −1 (male) versus 1 (female).
Results for the MEF total score largely confirmed above results for the UCLA. The final model considered sex and living with the patient as significant predictors of caregivers’ loneliness (R = .55, adjusted R 2 = .26, F (2,37) = 7.86, P = .001, see Table 5). Again, β weights suggested that males had higher ratings of caregivers’ loneliness than females and that experienced loneliness was higher when caregivers lived with the patient. No neuropsychological patient characteristic significantly predicted caregiver loneliness as indicated by the MEF total score, and no further predictor was clinically relevant as suggested by Ferguson. 19
Closer inspection of the MEF subscales again identified sex and living circumstances as the only significant predictors for the score on the subscale social loneliness (R = .47, adjusted R 2 = .18, F (2,37) = 5.17, P = .011): males reported higher social loneliness than females and living with the patient was associated with higher reported social loneliness (see Table 5). Neuropsychological patient characteristics had no significant influence on caregivers’ social loneliness. No other predictor was clinically relevant as suggested by Ferguson. 19
For emotional loneliness, living with the patient and sex were again the only significant predictors considered in the final regression model (R = .53, adjusted R 2 = .24, F (2,37) = 7.01, P = .003, see Table 5). Again, males reported higher emotional loneliness than females and living with the patient was associated with higher emotional loneliness. No other neuropsychological patient characteristics had a significant influence on caregivers’ emotional loneliness nor was there a clinically relevant influence of any variable according to Ferguson. 19
For the subscale inability to stay alone, living with the patient was the only significant predictor considered in the final regression model (R = .43, adjusted R 2 = .16, F (2,38) = 8.44, P = .006, see Table 5). Living with the patient was associated with higher inability to stay alone. Additionally, sex had a clinically relevant influence (b = −.26) following the suggestions of Ferguson 19 with males reporting higher inability to stay alone than females. No neuropsychological patient characteristic had a significant influence.
Finally, with respect to caregivers’ burden (as indexed by the ZBI) neither caregiver nor patient characteristics contributed significantly to variance explanation.
Discussion
The main aims of the present study were to investigate subjective feelings of loneliness and burden in family caregivers of patients with Alzheimer disease (major neurocognitive disorder, DSM-V 4 ). Loneliness was indexed by the German versions of the UCLA Loneliness Scale 14 (that measures loneliness unidimensionally, focusing on social aspects of loneliness) and the multidimensional loneliness questionnaire MEF, 13 while burden was measured using the ZBI. 15 Furthermore, we sought to examine whether specific caregiver and/or patient variables predicted subjective feelings of loneliness and burden.
Consistent with our first working hypothesis, our findings disclosed that family caregivers of patients with advanced Alzheimer dementia experienced feelings of loneliness and burden. However, the reported levels of loneliness varied substantially across our study participants, ranging from 21 to 64 (of a maximum of 88; unidimensional UCLA) and from 43 to 155 (maximum 185; multidimensional MEF) indexing low to moderate levels of loneliness. However, in the absence of empirically derived cutoff scores, this interpretation needs to be taken with care. In our study sample, male caregivers reported higher levels of loneliness than female caregivers (as reflected by both the UCLA and the MEF; Table 2). The latter finding thus corroborated the results of a recent meta-analysis disclosing that the negative impact of caregiving was stronger among men. 21
Likewise, with respect to caregivers’ subjective feelings of burden (indexed by the ZBI), our findings disclosed rather large variation (ie, raw scores ranging from 6 to 67, maximum 88) and thus, indicated no too severe burden. Nonetheless, contrary to caregivers’ feelings of loneliness, that were more pronounced among men, in our study population female caregivers reported higher subjective levels of burden than their male counterparts (for similar findings, see the study by Etters et al and Morgan et al 22,23 ). At first glance, the differential impact of sex on loneliness and burden might be rather surprising. However, considering that in our society, women are still more likely to be actively involved in direct caring, their higher perceived levels of burden become more readily understandable.
Furthermore, our findings are only partly in line with our second working hypothesis suggesting that both caregiver and patient variables should be correlated with caregivers’ perceived loneliness and burden. As depicted in Table 3, caregivers’ reported loneliness was significantly and positively correlated with caregivers’ sex, age, and living circumstances, but not to caregivers’ education (higher levels of loneliness being reported by older male caregivers who live together with their relative diagnosed with dementia). Notably, these significant effects of sex, age, and living circumstances emerged across both the uni- and multidimensional loneliness scale (ie, UCLA and MEF, respectively). In contrast, caregivers’ burden was significantly correlated with education only (caregivers with higher education reporting higher levels of burden). Our results are partly consistent with those reported by Pinquart and Sörensen 21 who reported that among dementia caregivers older age and male sex were associated with higher levels of subjective feelings of loneliness. However, these latter findings are not unequivocal as other studies disclosed that female caregivers of patients with Alzheimer disease reported higher scores of loneliness than male caregivers. 18
Regarding the assumed modulating effect of patient variables (ie, severity of dementia and neuropsychiatric symptoms) on caregivers’ loneliness and burden, the conducted partial correlations (controlling for caregivers’ sex) did not reach significance level. Nonetheless, the association between dementia severity (indexed by the MMSE-2) and loneliness (indexed by the MEF total score) was practically relevant according to Ferguson 19 (Table 4). Closer inspection of the data revealed that the association between the MMSE-2 and the MEF was mainly due to the MEF subscale “social loneliness” (and less so regarding the subscales “emotional loneliness” and “inability to stay alone”). Interestingly, the latter correlations were positive, thus indicating that higher MMSE-2 scores reflecting less severe dementia were associated with higher loneliness scores. The latter finding was counterintuitive as one might have expected that caregivers’ loneliness may increase with disease progression (ie, dementia severity). Although speculative so far, we suggest that caregivers’ loneliness might be strongest in the first stages of the disease, while with increasing disease progression caregivers’ may get somehow used to their state of chronic social isolation that come along with prolonged and devotional caregiving. Alternatively, it may be plausible to assume that with disease progression (ie, frequently associated with deterioration of patients’ general condition), caregivers were more likely to accept external support ranging from services for outpatients to placement in a nursing home. These provisions are likely to provide caregivers with some spare time, allowing them to take up previously neglected social relations again, which, in turn may alleviate subjective feelings of loneliness. Another possible explanation for our somewhat surprising findings might be that caregivers of patients in advanced disease stages may have been caught up with caregiving, which might have masked any potential feelings of loneliness.
A somewhat different picture emerged regarding another patient variable, namely severity of neuropsychiatric symptoms (measured by the NPI) that were not significantly correlated with caregivers’ loneliness or burden (likewise, these correlations were not practically relevant according to Ferguson 19 ). The latter finding was contrary to expectation and not consistent with previous results disclosing that caregiver burden was significantly associated with severity of neuropsychiatric symptoms in patients with Alzheimer disease. 23,24
Overall, our results corroborated previous findings disclosing that family caregivers of patients diagnosed with dementia should be regarded at risk for developing loneliness. 18,25 Furthermore, upon considering that loneliness has been reported to be a major risk factor for incident dementia (ie, comparable to other well-established risk factors such as late-life depression, physical inactivity, and low education 26 ), family caregivers may develop dementia themselves.
Finally, and partially inconsistent with our third working hypotheses (stating that both caregiver and patient characteristics should predict caregivers’ loneliness and burden), our regression results disclosed that caregiver—but not patient—characteristics contributed significantly to explained variance of caregivers’ loneliness (see Table 5). In particular, male sex and living with the patient (but neither caregivers age nor education) were found to predict caregivers’ loneliness (indexed by both the UCLA and the MEF). Regarding the MEF, our results revealed the subscales “social loneliness” and “emotional loneliness” (but not the subscale “inability to stay alone”) as modulating factors of caregivers’ loneliness. With regard to caregivers’ burden (ZBI), regression results revealed that neither caregiver nor patient variables were found predictive. Hence, our results partly corroborated those reported by McRae et al 9 who found that caregiver characteristics were better predictors explaining variance of caregivers’ loneliness (ie, 46%, while patient characteristics only contributed 12% to variance explanation). Notably, because our findings were similar across the 2 loneliness scales utilized in the present study, we suggest that both the unidimensional UCLA and the multidimensional MEF might be sensitive clinical tools to detect loneliness experienced by family caregivers of patients with advanced dementia.
Overall, our results suggest that family caregivers have an enhanced risk to develop persistent psychological strain that may manifest as subjective feelings of loneliness and burden. Moreover, prolonged or chronic feelings of loneliness and burden in (often elderly) family caregivers frequently cause secondary health problems that may require medical treatment. Thus, family caregivers are likely to present as secondary patients. 8 Future endeavors in health-care politics should be targeted at providing diagnostics and treatment to caregiver–patient dyads instead of to patients solely.
Unique features of our study were (1) the combined investigation of loneliness and burden in family caregivers of patients diagnosed with major neurocognitive disorder due to Alzheimer disease (DSM-V 4 ) and (2) the utilization and comparison of uni- and multidimensional loneliness scales. Although both the unidimensional 20-item UCLA Loneliness Scale 14 and the 37-item multidimensional MEF 13 were found to tap loneliness in family caregivers of patients with dementia, the MEF provided a more differentiated picture of caregivers perceived loneliness.
Finally, our findings suggest that caregivers’ loneliness could be examined effectively during an inpatient stay of their relatives diagnosed with dementia. In this context, accumulating evidence suggests that individuals reporting prolonged loneliness have a substantial risk to develop dementia. 25 -27 Thus, beyond having an easing effect on the affected individuals, the identification and prevention of loneliness among caregivers might significantly decrease health-care utilization and hence, health-care costs. 3
Limitations and Strengths
A limitation of the present study is the rather small sample size (n = 40). As such, our results should be regarded preliminary. A further potential limitation is that we were not able to examine caregivers’ depression (as a potential modulating factor of subjective feelings of loneliness). However, it has to be noted that our results are largely exploratory in nature. In particular, we did not aim at testing causal mechanisms of predicting caregivers’ loneliness and burden.
Strengths of the present study are the carefully selected patient group. To the best of our knowledge, we are among the first to assess loneliness and burden in family caregivers of patients having Alzheimer dementia in advanced stages. Furthermore, our study is unique as we utilized both uni- and multidimensional loneliness scales. Interestingly, our findings disclosed that both the multidimensional MEF and the unidimensional (and more economical) UCLA scales seem to be sensitive to caregivers’ subjective feelings of loneliness. Nevertheless, future research is needed to substantiate the suitability of the 2 scales in specific (caregiver) populations.
Footnotes
Acknowledgments
The authors would like to thank all participating patients and their caregivers.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.