
Abstract
Purpose:
This study aims to examine the factors affecting caregivers’ acceptance of the use of wearable devices by patients with dementia by extending the Unified Theory of Acceptance and Use of Technology (UTAUT) model with 2 additional constructs: resistance to change (RC) and technology anxiety (TA).
Methods:
A structured online questionnaire was developed and distributed to caregivers who have either dealt previously with or were currently taking care of patients with dementia in sub-Saharan Africa. The selection of countries for the study was purely based on the availability of caregivers of patients with dementia and their readiness to take part in the survey. Questionnaire data from 350 respondents were analyzed and the hypothesis tested using partial least squares based on structural equation modeling.
Result:
The results of the extended model show that social influence, effort expectancy, facilitating conditions, and behavioral intention (BI) all had P < .05, thus were statistically significant in explaining the perceived BI and actual use of health-care wearable devices among patients with dementia as reported by caregivers. However, P value for RC and TA was greater than .05, hence were insignificant.
Introduction
Dementia affected about 50 million people globally in 2018, making it the seventh leading cause of death according to the World Health Organization (WHO). This figure is projected to rise to 131.5 million by 2050 (WHO Dementia Fact sheets, 2019) with about 10% of people developing the disorder at some point in their lives and about 9.9 million new cases diagnosed yearly translating into one case every second. 1 In sub-Saharan Africa, an estimated 2.13 million people were living with dementia as of 2015, with numbers projected to nearly double every 20 years, increasing to 3.48 million by 2030 and 7.62 million by 2050. This translates into over 367 000 new cases of dementia in a year in the region. 2
Data From World Population Prospects
The 2017 Revision show that the number of older persons, those aged 60 years and older, is expected to be more than double by 2050 and to be more than triple by 2100, rising from 962 million globally in 2017 to 2.1 billion in 2050 and 3.1 billion in 2100. 3 Globally, population aged 60 years and above is growing faster than all younger age groups. Although the proportion of the population of older people is rather small in sub-Saharan Africa compared to other parts of the world, the number in the region is growing. In 2005, there were 34 million people older than 60 in the region; this number has increased to over 52 million in 2019 (Population Pyramids, 2019), making it the most rapidly growing population of older people compared to those in the developed world. As more people are living longer in sub-Saharan Africa, dementia and other chronic conditions are becoming more common and prevalent in the population as a whole, 4 triggering the need for increase in both the quality and variety of health-care services offered to these patients.
Dementia is overwhelming not only for the people who have it but also for their caregivers and families, impacting their careers, and physical, psychological, and economic well-being. Issues such as lack of awareness and understanding of dementia in most countries, which ultimately result in stigmatization and barriers to diagnosis and care, further exacerbate the burdens for caregivers. Economically, the total costs of dementia in sub-Saharan Africa are estimated to be over US$6.2 billion, accounting for more than the national gross domestic product of 19 of the 49 countries in the region. Almost three-quarters of this are made up of the cost of informal care, predominantly provided by family members. It is expected that, as the population ages over the next several decades, dementia cases and their associated costs will go up dramatically. Aside the economic burden, a 2017 Alzheimer’s Statistics show that nearly one-fourth of dementia caregivers are “sandwich generation” caregivers, who are caring for both someone with the disease and a child or grandchild, with more than 40% of family caregivers reporting that the emotional stress of their role is high or very high. The report further stated that more than 1 in 6 dementia caregivers had to quit work entirely either to become a caregiver in the first place or because their caregiving duties became too burdensome. According to the study, 74% of caregivers of people with Alzheimer disease and other dementias reported that they were “somewhat concerned” to “very concerned” about maintaining their own health since becoming caregivers. 5 The enormous stress of dementia on both caregivers and patients has led to more intensified research by dementia researchers to investigate ways to delay, manage, cure, or prevent the onset and progression of dementia in order to assist caregivers and stakeholder’s effort to slow down or completely prevent the occurrence of a health-care crisis in sub-Saharan Africa, while minimizing the burden on caregivers. Due to the nature of the disease, which consists of wide range of symptoms that are associated with decline in memory and thinking skills, there is a constant need for assistance by these patients from family members and health-care providers, leading mostly to the institutionalization of these patients, and a corresponding increase in cost of institutional care for both policymakers in the health-care industry and caregivers. Although institutionalization may seem to be the best option for managing dementia, the majority of these older adults with dementia prefer to live independently for as long as they possibly can, 6 -8 while receiving the best health care. Several interrelated factors can affect the ability of older adults to live independently: chronic diseases, a diminishing social network, low level of physical activity, and functional and cognitive impairment, which is very common in people with dementia. 9 -12 However, thanks to the advancement in technological innovation particularly in the past decade, most of these challenges can be minimized. Wearable technologies such as sensor-based networks for activity monitoring, fall and wandering detection, smart socks, Clevercare smartwatch, and various e-health applications have since been introduced to help patients live their lives independently. These wearable devices allow patients to continuously monitor physiological parameters and manage their health and well-being on personal basis, and also grant caregivers access to their health data, thereby helping these patients to receive personalized medical care. 13 -15 Though the ultimate impact of health-care wearable devices on consumers as well as on society can be substantial 13,16 especially in reducing the burden of dementia on caregivers, little has been done in terms of research to understand the factors that could influence these caregivers to recommend for acceptance and adoption of health-care wearable devices for their relatives and patients. Thus, this study seeks to examine factors that influence caregivers’ acceptance of the use of wearable devices by patients with dementia using an extended UTAUT 17 as theoretical framework to empirically test and understand those influencing factors in the context of sub-Saharan Africa.
Theoretical Framework, Research Model, and Hypotheses
This study adopts one of the most influential user acceptance and behavior analysis models, the UTAUT, to analyze the factors that influence caregivers’ acceptance of the use of wearable devices by patients with dementia in sub-Saharan African. Theories such as the theory of reasoned action, diffusion of innovation theory, theory of planned behavior (TPB), technology acceptance model (TAM), a combination of technology acceptance model and theory of planned behavior (TAM-TPB), and social cognitive theory have been developed and implored in several research to explain the intention and use of new technologies. However, most of these models are deficient in sufficiently explaining the actual use and behavioral intention (BI) of users. For instance, the TAM model according to Venkatesh et al only provides limited guidance on how to influence usage through design and implementation, which does not necessarily help understand or explain acceptance in ways that guide development beyond the suggestion that system characteristics impact ease of use. 17 Another challenge with the TAM was the inability of the findings to be generalized due to issues relating to the type of respondents, examined systems, or the sample choice. 18 These, among other limitations, necessitated the creation of the UTAUT model.
The UTAUT model is one of the models derived by a comprehensive examination of various models mentioned above aimed at achieving a unified view of user acceptance. 17 The model proposes 4 constructs, 17 namely, performance expectancy (PE), effort expectancy (EE), social influence (SI), and facilitating conditions (FCs), grouping similar earlier constructs. Since its appearance, the UTAUT model has gradually attracted researchers’ attention and has recently been applied to explore users’ acceptance of mobile technologies, 19,20 and incrementally tested and applied to several technologies for both individual and organizational uses, within single and multiple countries. 21 It has also been widely adopted in different areas in the health-care sector, including e-Health, mHealth, and wearable devices. 22 -24 Even though traditional UTAUT provides a very good and detailed model for acceptance and use of technology, its ability to explain user and BI through the introduction of moderating effects of technology anxiety (TA) and resistance to change (RC) in the area of dementia and other cognitive impairment illnesses is unknown, hence the decision to incorporate these new constructs. The reasons for choosing to extend the UTAUT model over all other technology adoption models are its ability to account for 70% of the variance in usage intention, which is considered a measured improvement over any of the adoption models where the maximum was around 40%. Second, by adapting and extending UTAUT to include new constructs and altering existing relationships, this work furthers the generalizability of UTAUT to a different context that is an important step to advance a theory, 25 irrespective of the type of respondents, examined systems, or the sample choice.
Development of Extended UTAUT Model
Using reviews of prior studies of UTAUT in health care, we adopted the 4 most commonly used constructs of the traditional UTAUT model: PE, EE, SI, and FC, in addition to 2 new moderating constructs: TA and RC for this study. The conceptual research model (see Figure 1) developed in this study consists of those 4 antecedents: PE, EE, SI, and FC act as determinants of users’ BI and use behavior (UB). Among those, PE, EE, and SI s are significantly direct determinants of user intention to adopt technology such as health-care wearable devices. Both FCs and BI explain user’s actual UB of technology. 17

Research model.
Performance expectancy
The PE component of the UTAUT model was originally based on the perceived usefulness component of TAM and is defined as “the degree to which an individual believes that using the system will help him or her to attain gains in job performance.”
17
Venkatesh et al found after several empirical comparisons of 8 models that the PE component of each model was the strongest predictor of BI. Sun et al
26
empirically demonstrated that the greater the PE, the more likely mobile health services would be adopted. Performance expectancy is used for analysis in this study due to its robust antecedent of technology acceptance. Hypothesis 1 was posited. Hypothesis 1: Caregivers perceive PE has positive impact on the intension of patient with dementia to use health-care wearable devices.
Effort expectancy
Effort expectancy is defined as “the degree of ease associated with the use of the system.”
17
Effort expectancy was derived from the perceived ease of use (PEOU) component of TAM. It has been identified by Boontarig et al
26
and Sun et al
27
as an important factor directly influencing users’ intention to use mobile health monitoring systems, e-Health services via a smartphone, clinical decision support systems, and mobile health. Hypothesis 2 was formed based on the discussion above. Hypothesis 2: Caregivers perceive EE has positive impact on the intension of patients with dementia to use health-care wearable devices.
Social influence
According to Venkatesh et al, SI is defined as how strongly an end user perceives that others (family, community, and society) believe they should use the new system. Previous studies have shown that the attitudes and behaviors of other individuals in a user’s social and work circles significantly impact that end user’s use of technology.
28
-30
Hypothesis 3 was posited. Hypothesis 3: Caregivers perceive SI has positive impact on the intension of patient with dementia to use health-care wearable devices.
Facilitating condition
Venkatesh et al
17
defined FC as the degree to which an individual believes that an organizational and technical infrastructure exists to support their use of a particular system. The FC comprises of 3 factors: training and support, shared belief in the system, and project communication. Seymour et al
31
used symbolic adoption as the sole dependent variable in determining end-users’ acceptance of enterprise resource planning systems. Research by Boontarig et al
27
suggested that FC positively influences the BI and UB of using smartphones for health services. Based on the above literatures, we posited hypotheses 4 and 5 as follows: Hypothesis 4: Caregivers perceive FC has positive impact on the intension of patient with dementia to use health-care wearable devices. Hypothesis 5: Caregivers perceive FC has positive impact on the actual use of health-care wearable devices for patient with dementia.
Behavioral intention
Extensive research on the relationship between BI and actual UB has shown BI to be a valid predictor of actual UB.
32,33
Empirically, BI has been tested and found out to be able to explain user’s actual UB of technology.
17
Research by Han et al
34
on determining physicians’ BIs regarding the use of mobile technology revealed that actual UB influences the BI of physicians in their quest to use mobile health technology. Hypothesis 6 was posited for BI. Hypothesis 6: Caregivers perceive BI has positive impact on the actual use of health-care wearable devices for patient with dementia.
Constructs for extending UTAUT
Since the introduction of the UTAUT, researchers have sought to extend the original constructs of the model to include variables, such as hedonic motivation, which was used as a key predictor in consumer behavior research by Holbrook and Hirschman; price value; and habit of the user. 23,35 -38 The choice to extend the traditional UTAUT model with TA and RC as moderating constructs stems from the fact that these factors have been found by researchers to influence whether or not an elderly patient uses technology. 39 Due to the cognitive effect of the dementia disease, these factors were chosen to explain the real effect they have on the acceptance and adoption of wearable devices from the perspective of caregivers.
Technology anxiety is a negative emotional response and pertains to the fear of discomfort people experience when they think of using technology.
40
Also, RC has the tendency of reducing the adoption intention of technology.
41
It is also argued that elderly people have a high degree of RC,
22,42
and since dementia is commonly known to be associated with aging, the inclusion of RC will help to test this assertion. The addition of these 2 moderating variables adapted from
22
: TA and RC (see Figure 1) will also enhance the prediction of intention of patient with dementia to use health-care wearable devices from the perspective of caregivers. For purposes of this study, we posited hypotheses 7 and 8 for these 2 moderating variables. Hypothesis 7: Caregivers perceive RC has a negative impact on the intention of patient with dementia to use health-care wearable devices. Hypothesis 8: Caregivers perceive TA has a negative impact on the intention of patient with dementia to use health-care wearable devices.
Materials and Methods
Questionnaire Design and Data Collection
A structured questionnaire was developed in English using eSurvey Creator, an online portal for creating surveys. English was chosen because the research participants (caregivers) were from English-speaking sub-Saharan African countries. The selection of countries for the study was purely based on the availability of caregivers’ and their readiness to take part in the survey. This study relied on caregivers as proxies as opposed to patients with dementia themselves in responding to the survey question due to the peculiar characteristic of the dementia disease, issues of cognitive decline (in thinking, memory, and reasoning), and the inability to perform certain physical functions. A research by Infurna et al 43 aimed at examining the extent to which retrospective proxy reports of well-being mirror participant self-reports revealed that there is moderate agreement between self-reports and proxy reports (r = 0.42). Thus, it is expected that the results of this current study would not deviate significantly if it was to use patients with dementia themselves. Also, the questions posed were closed ended in order to eliminate issues of biases in the responses. The questionnaires were distributed via social media platforms and e-mails of caregivers with an introduction stating clearly the objective of the survey, the eligibility criteria to qualify to be a respondent, and Internet hyperlink to the survey.
The questionnaire was divided into 2 parts, with the first part containing the demographic information. Respondents were asked information about their age, gender, educational qualifications, country of residence, marital status, and the number of years they have dealt with patients with dementia. The second part included questions for the different constructs of the extended UTAUT model presented in the research model using a 5-point Likert scale, ranging from (1) “strongly disagree” to (5) “strongly agree.”
Respondents were made aware that there were no risks anticipated by agreeing to be part of the study. A confidentiality statement was also included prompting respondents that their data will not be connected to their names or other personal information, all personal data they wish to provide will be treated strictly confidential unless they explicitly give the researchers permission to disclose such personal information. Respondents were also made aware that their participation in the study was completely voluntary and that should they at any time decide to withdraw by exiting the questionnaire, any response they had submitted up to that point will be retained.
Contact information of the researchers was also provided, so as to give respondents the opportunity to freely contact should they have further questions regarding the study. Finally, a checkbox capturing a Consent Agreement, “The purpose and nature of this research have been sufficiently explained and I agree to participate in this study. I understand that I am free to withdraw at any time without incurring any penalty,” was included for respondents to tick in agreement to participate in the study.
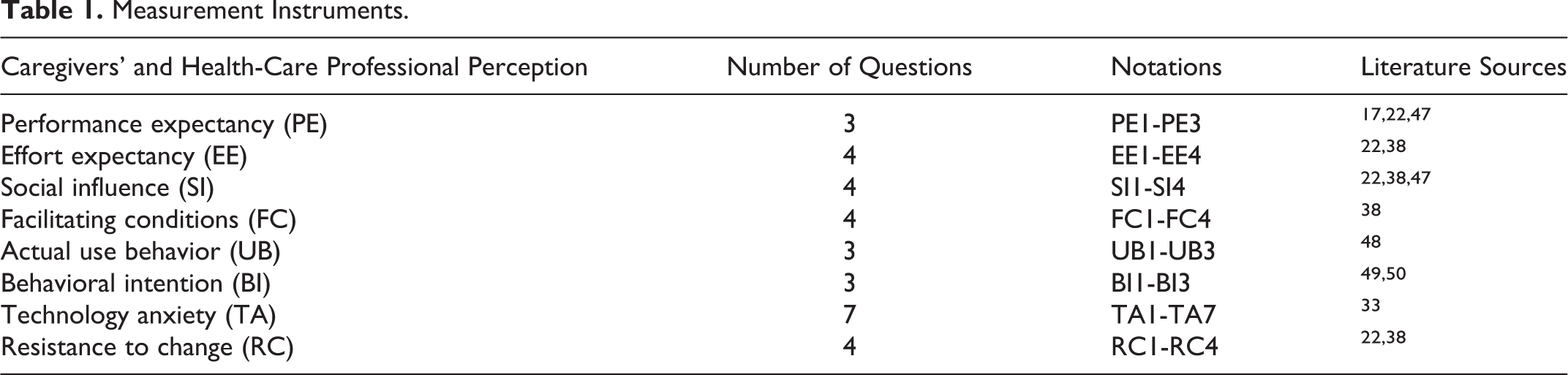
Missing values, outliers, and normality were assessed to ensure the quality of data to be used for further analysis. Of the total 408 responses received, 58 responses were excluded from the study: 28 were excluded due to either substantially incomplete responses or missing values, and 30 for not meeting the criteria for number of years they had worked with patients with dementia. A total of 350 responses were used for further analysis. For statistical analysis such as structural equation modeling (SEM), a sample size of 200 is considered to be fair and 300 as good. 44 -46 Hence, the sample size of 350 meets these requirements and is significant enough to obtain robust results after analysis. Also, the use of the UTAUT model, which allows for generalizability of results, gives sufficient justification of the sample size. Questionnaire composition as were adapted from literature sources are indicated in Table 1.
Measurement Instruments.
Data Analysis
Data from the questionnaire were exported from the online database of eSurvey Creator into Microsoft Excel format for statistical analysis. The data analysis consisted of both exploratory and confirmatory analyses to ensure the validation of the reflective measurement model. 51 The exploratory/descriptive analysis was performed on the data using Statistical Package for the Social Sciences (SPSS) software. This is to ensure the data meet the initial requirement for it to be used for SEM. This process was followed by a confirmatory factor analysis. The partial least squares (PLS) method, a statistical analysis technique based on the SEM, was used to test and validate the proposed model and the relationships between the hypothesized constructs due to its robustness of estimations and statistical power. 52 SmartPLS3 software was used to analyze the data 53 due to its ability to provide results for all types of variables, regardless of whether they have metric, quasi-metric, ordinal, or categorical scales (eg, binary coded). 54
In order to identify the relationships between the constructs in the research model, a structural model was developed. The path coefficient (β) and t statistics were used to test how closely related the dependent and independent variables are. For a relationship between the constructs to be considered to be strong, the path coefficients must be closer to +1. In contrast, path coefficients values closer to 0 are considered to have a weaker relationship while those with very low values closer to 0 are considered to be statistically insignificant. Thus, P value must be smaller than .05 to conclude that the relationship under consideration is significant at a 5% level or less than .01 at 1% significant level. In terms of t statistic value, when an empirical t value is larger than the critical value, which is commonly obtained using critical value for 2-tailed test (1.65 at a significant level of 10% and 1.96 at a significant level of 5%), one can conclude that the coefficient is statically significant at that error probability.
Results
Results obtained by means of PLS algorithm, bootstrapping, and blindfolding from SmartPLS and the descriptive statistics that provided the demographic result of participants obtained using SPSS software are presented below (see Tables 2 to 6).
Age and Years of Experience Distribution.

Other Demographic Distributions.

Measurement Model
The data were assessed for the internal consistency reliability, convergent, and discriminant validity. 55 The various loadings, average variance extracted (AVE), composite reliability, Cronbach α, and t values 55,56 that satisfy the minimum criteria for inclusion used to examine the measurement model are shown in Table 4.
Quality Criteria and Factor Loadings.

Abbreviations: AVE, average variance extracted; HTMT, Heterotrait-Monotrait ratio.
Results of the discriminant validity of all the constructs UB, BI, EE, FC, PE, RC, SI, and TA, which were obtained using the square root of the AVE and cross-loading matrix of 0.814, 0.846, 0.766, 0.682, 0.754, 0.703, 0.754, and 0.64, respectively, are shown in Table 5. According to Hair et al, the square root of the AVE of a construct should be greater than its correlation with other constructs for satisfactory discriminant validity 55 and the diagonal elements must be larger than the entries in corresponding columns and rows to satisfy discriminant validity. 57
Correlation Matrix and Square Root of the AVE.

Abbreviations: AVE, average variance extracted; BI, behavioral intention; EE, effort expectancy; FCs, facilitating conditions; PE, performance expectancy; RC, resistance to change; SI, social influence; TA, technology anxiety; UB, use behavior.
Hypothesis Testing
Table 6 shows the structural model developed to test the relationships between the variables: both dependent and independent variables in the research model by path coefficient (β
Structural Model.a,b

Abbreviations: BI, behavioral intention; EE, effort expectancy; FCs, facilitating conditions; PE, performance expectancy; RC, resistance to change; SI, social influence; TA, technology anxiety; UB, use behavior; UTAUT, Unified Theory of Acceptance and Use of Technology.
a Significant at P < .05.
b PE and BI (t statistics = 1.857, β = .108, P value = .064, P > .05), RC and BI (t statistics = 0.718, β = −.040, P value = .473, P > .05), TA and BI (t statistics = 0.163, β = −.008, P value = .871, P > .05) were insignificant and not supporting hypotheses 1, 7, and 8. However, EE and BI (t statistics = 8.657, β = .444, P value = .000, P < .05), SI and BI (t statistics = 3.314, β = .173, P value = .001, P < .05), BI and UB (t statistics = 9.557, β = .404, P value = .000, P < .05), FC and BI (t statistics = 5.411, β =.284, P value = .000, P < .05), and FC and UB (t statistics = 13.288, β = .515, P value = .000, P < .05) were significant. Thus, hypotheses 2, 3, 4, 5, and 6 were supported.
Discussion
Results for the descriptive statistic of the participants for this study are presented in Tables 2 and 3. There were 213 females constituting a percentage of 60.90 and 137 males constituting a percentage of 39.10. The minimum age of respondents is 20, while the maximum age is 70 with a standard deviation of 12.31 (see Table 2). The percentages of demographic distribution for the educational levels of respondents are 41.70, 53.70, 3.70, and 0.90 for BSc, diploma, certificate, and those with no formal education, respectively.
This study applied an extended UTAUT model comprising of 2 new moderating constructs: TA and RC, and 4 key constructs: PE, EE, SI, and FCs from the traditional UTAUT model, to understand the factors that influence caregivers to recommend for the acceptance and adoption (BI and actual UB) of health-care wearable devices among patients with dementia. The study provided empirical support for the proposed hypotheses in relation to SI), BI, FCs, and EE in explaining health-care wearable adoption and usage among patients with dementia from the perceptive of caregivers. Most of the findings were consistent with the results of previous studies on the application of the traditional UTAUT in examining technology adoption in the health-care sector. For instance, Hoque and Sorwar 22 observed that SI) and BI have significant influence on the adoption and usage of mHealth among elderly patients in Bangladesh, which is consistent with our findings. We found that FCs explained the highest amount of variance. This finding is consistent with previous studies by Melenhorst et al, Alvseike and Brønnick, and Czaja et al, who revealed that FCs such as an individual’s intellectual and cognitive abilities, and perceived cost of learning new technologies, have effect on the adoption of technology. 58 -61
We found that caregivers were willing to recommend the use of these devices to patients; however, factors such as little or no disposable income, lack of technical know-how on the part of patients, and limited access and availability of wearable devices in sub-Saharan Africa were limiting the usage of these devices, hence the hesitation by caregivers to encourage its use by patients with dementia. Additionally, the issue of affordability of these devices in sub-Saharan Africa also deters its recommendation by caregivers as it further puts financial constraints on the already scanty resources available to them. Though most of these caregivers perceived that patients were confident their medical practitioners and caregivers have the requisite knowledge to assist them to use these devices, issues of safety and security such as hacking, confidentiality of patients’ information, and privacy concerns do not make patients with dementia feel safe to use these devices. Contrary to the assertion of Venkatesh et al 17 that, if both PE and EE constructs are present in a model and significant, FC becomes nonsignificant in predicting user’s BI to the adoption and acceptance of technology, we found that if FC and EE constructs are present in a model and significant, then PE becomes nonsignificant in predicting user’s BI to the adoption and acceptance of technology. This may be as a result of some of the unique nuances that exist in sub-Saharan Africa, such as limited availability of wearable devices, lack of technical know-how and the awareness of the importance of technical, monetary, and/or infrastructural resource requirements.
The study also found RC and TA to have a negative influence on BI to use health-care wearable devices as perceived by caregivers of patient with dementia (see Table 6), supporting hypotheses 7 and 8 though their relationships were not significant. These are consistent with previous studies as to the role of RC and TA in technology adoption among the elderly patients. Guo et al 41 revealed that TA can reduce the adoption intention of elderly people by reducing the PEOU. A study by Ryu et al 62 also argued that TA creates major barriers for the elderly patients in adopting innovations. According to the result, PE, which is a core construct of UTAUT and acts as a direct determinant of BI, is not a significant determinant in the BI to use these health-care wearable devices contrary to findings of several previous research. 17,22,61 In determining the relationship between BI and actual UB of health-care wearable devices among patients with dementia from the perspective of caregivers, this study identified a positive relationship between the 2 constructs. Adapting from the literature of Carlsson et al, 63 we assert that the higher the patient with dementia’s BI to adopting health-care wearable device is, the greater their actual UB of such devices.
In order to assess the predictive accuracy and relevance of the model, this study used the R 2 to indicate the variance explained of the endogenous constructs by the exogenous construct. An R 2 range of 0 to 1 is acceptable with higher values indicating higher levels of predictive accuracy and, Q 2 values larger than 0 suggest that the mode has predictive relevance for a certain endogenous construct. According to Hair et al 54,65 and Hensler et al 64 , R 2 values of 0.75, 0.50, or 0.25 represent, respectively, substantial, moderate, and weak predictive abilities of the variable. Also, Chin and Marcoulides 66 articulates the values of 0.67, 0.33, and 0.19 as substantial, moderate, and weak, respectively. Therefore, R 2 values 0.707 and 0.737 for BI and UB, respectively, show the model has substantial predictive accuracy (see Table 6). Also, Q 2 values of 0.544 and 0.534 suggest the model has predictive relevance for the endogenous constructs.
Implications of Study
This study has implication for stakeholders in the health-care sector, especially those in the area of dementia and for researchers in dementia-related fields. It also has implication for manufacturers of health-care wearable devices for patients with dementia, especially in sub-Saharan Africa. Although several researchers have relied on the use of technology acceptance models to access the acceptance of technologies, only few studies have focused on understanding factors that influence the acceptance and adoption of health-care wearable devices among patients with dementia by considering the perspective of caregivers. These studies have either relied on the basic constructs of TAM or UTAUT model in investigating the UB of new technologies. Also, there seems to be a lack of a conceptual approach in technology acceptance modeling since studies usually concentrate on a specific technology or service. 67 -70 Though the moderating constructs RC and TA which this study attempted to use in extending the UTAUT model were not significant, they supported the original hypotheses. Thus, our study will offer researchers important insights into analyzing acceptance behavior of patients with dementia. To the best of our knowledge, this is the first study that seeks to extend the UTAUT model with TA and RC in the UB of health-care wearable devices among patients with dementia from the perspective of their caregivers.
The significant relationship between FC and BI suggests that stakeholders need to invest more into the adoption of these devices by either making them freely available or at a subsidized cost for patients with dementia in order to help reduce the costly option of institutional care for these patients and caregivers. This study also provides a guide for stakeholders to pursue agenda that will eliminate the barriers and build better conditions to facilitate the adoption and use of these health-care wearable devices by patients with dementia in sub-Saharan Africa. Additionally, manufacturers and service providers should organize training aimed at communicating concrete benefits of these devices and also provide sustainable technical support to caregivers, medical professionals, and patients with dementia so as to allay their fears concerning confidentiality and security of their information. Also, these devices should be modeled in such a way that it reduces the anxiety levels of these patients with dementia by through the use of more user-friendly and easy-to-use interfaces, as this has been shown to significantly reduce elders’ anxiety about technology use 71 in developing countries. Finally, the findings could assist stakeholders in other developing countries in their planning processes and introduction of health-care wearable devices among patients with dementia, since the model used for this study allows for findings to be generalized.
Limitations and Future Study
This study is limited due to the use of caregivers of perspective of patient with dementia as proxies in examining the adoption behavior of patients with dementia in using health-care wearable devices in sub-Saharan Africa. Though most of the findings were consistent with the technology adoption behavior of elderly patients, there is the need for a deeper understanding of the UB of health-care wearable devices from the perspective of patients with dementia themselves. Thus, further study should be carried out to extend by soliciting responses directly from patients themselves through semistructured face-to-face interviews. Additional demographic and geographic factors such as the age of the patients with dementia, income levels of the patients with dementia, and the educational level of patients should be included.
Conclusion
The results of this study indicate that SI, FCs, and EE have statistically significant effect on the BI of patient with dementia to use health-care wearable devices from the caregivers’ perspective. Constructs such as PE, RC, and TA were not significantly supported, though they confirmed the hypotheses enumerated for this study. The study has implications for the development of health-care wearable devices for patients with dementia in sub-Saharan Africa. Also, the predictive accuracy of 70.7% shows that the constructs used for this study were substantially able to explain the variance of the endogenous variables compared to other technology adoption models.
Footnotes
Acknowledgments
The authors would like to sincerely thank the editor and anonymous reviewers for their helpful and insightful comments and suggestions that have resulted in a much-improved version of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Nature Science Foundation of China (71774069).